Embed Size (px)
Citation preview
Lanthanum CarbonateA Review of its Use in Lowering Serum Phosphate inPatients with End-Stage Renal Disease
Monique P. Curran and Dean M. Robinson
Adis, a Wolters Kluwer Business, Auckland, New Zealand
Various sections of the manuscript reviewed by:M. Emmett, Department of Internal Medicine, Baylor University Medical Center, Dallas, Texas, USA;D.J. Goldsmith, Renal Unit, Guy’s Hospital and St Thomas’ Hospital, London, UK; A.J. Hutchison,Manchester Royal Infirmary, Manchester, UK; K.J. Martin, Department of Internal Medicine, Saint LouisUniversity, St Louis, Missouri, USA; R. Mehrotra, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, California, USA; G.A. Siami, Department of Medicine, Division ofNephrology, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Data Selection
Sources: Medical literature published in any language since 1980 on ‘lanthanum carbonate’, identified using MEDLINE and EMBASE,supplemented by AdisBase (a proprietary database). Additional references were identified from the reference lists of published articles.Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.
Search strategy: MEDLINE, EMBASE and AdisBase (a proprietary database) search terms were ‘lanthanum carbonate’ and‘hyperphosphataemia’. Searches were last updated 15 October 2009.
Selection: Studies in patients with end-stage renal disease who received lanthanum carbonate. Inclusion of studies was based mainly onthe methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred.Relevant pharmacodynamic and pharmacokinetic data are also included.
Index terms: Lanthanum carbonate, end-stage renal disease, hyperphosphataemia, pharmacodynamics, pharmacokinetics, therapeuticuse, tolerability.
Contents
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23301. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23312. Pharmacodynamic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23323. Pharmacokinetic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23334. Therapeutic Efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2335
4.1 Short-Term Therapy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23354.1.1 Comparisons with Placebo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23354.1.2 Comparison with Calcium Carbonate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23374.1.3 Comparison with Sevelamer Hydrochloride . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2338
4.2 Long-Term Therapy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23394.2.1 Comparative Trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23394.2.2 Extension Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2340
5. Tolerability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23416. Dosage and Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23437. Place of Lanthanum Carbonate in the Management of Serum Phosphate Levels in Patients with
End-Stage Renal Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2343
ADIS DRUG EVALUATIONDrugs 2009; 69 (16): 2329-2349
0012-6667/09/0016-2329/$55.55/0
ª 2009 Adis Data Information BV. All rights reserved.

SummaryAbstract Orally administered lanthanum carbonate (Fosrenol�) dissociates in the acid
environment of the upper gastrointestinal tract to release the cation lanthanum,
which then binds dietary phosphate.
Lanthanum carbonate was effective in reducing levels of serum phosphate and
serum calcium ·phosphate product and then maintaining these levels within
target ranges for up to 6 years in adult patients with end-stage renal disease
(ESRD) on haemodialysis or peritoneal dialysis. The reduction in serum phos-
phate levels with lanthanum carbonate was generally similar to that with calcium
carbonate or sevelamer hydrochloride. This agent was generally well tolerated,
with the most frequently reported adverse events being gastrointestinal in nature
and occurring at a similar rate to that with calcium carbonate. However, lan-
thanum carbonate was associated with fewer episodes of hypercalcaemia than
calcium carbonate. Overall, lanthanum carbonate is a valuable option for the
reduction of serum phosphate levels in patients with ESRD on haemodialysis or
peritoneal dialysis.
PharmacologicalProperties
Lanthanum carbonate dissociates in the acid environment of the upper gastro-
intestinal tract to release the trivalent cation lanthanum, which binds with high
affinity to dietary phosphate in the stomach and upper small intestine, forming
insoluble lanthanum phosphate.
Lanthanum carbonate reduces daily phosphate absorption. In patients with
chronic kidney disease with residual kidney function, the decrease in uri-
nary phosphate excretion (»300mg/day) achieved with lanthanum carbonate
£3000mg/day was estimated to be equivalent to about one-third of the daily
phosphate absorption.
Lanthanum carbonate was not associated with detrimental effects on bone-cell
activity, according to paired-bone biopsy studies of up to 2 years duration in
patients with ESRD. With lanthanum carbonate versus comparator phosphate
binder therapy, the percentage of patients with improved bone turnover after
1 year, but not 2 years, was significantly higher, and the percentage of patients
with reduced bone volume was significantly lower after 2 years.
Lanthanum does not appear to cross the blood-brain barrier, according to data
from animal studies. In patients with ESRD undergoing haemodialysis, there was
no significant difference between lanthanum carbonate and alternative phosphate
binder therapy in the decline in cognitive function that occurred over a 2-year
period.
Systemic absorption of lanthanum carbonate is minimal (absolute bioavail-
ability <0.002%). In patients with ESRD administered lanthanum carbonate
3000mg/day for 10 days, the mean maximum plasma concentration of lanthanum
was 1.0 ng/mL. Plasma concentrations of lanthanum did not increase with long-
term (up to 6 years) administration of lanthanum carbonate. Bone biopsies taken
from patients with ESRD who were treated with lanthanum carbonate for up to
4.5 years indicated an increase in bone lanthanum concentrations over the treat-
ment phase (maximum concentration in any individual patient »10 mg/g wet
weight bone). After treatment cessation, lanthanum loss from bone was estimated
to be »13% per year. In long-term animal studies, lanthanum concentrations
increased over time in several tissues, including the liver; however, there was no
2330 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

evidence of adverse effects of this agent on the liver in clinical studies in which
patients with ESRD received up to 6 years of lanthanum carbonate treatment.
Lanthanum is not metabolized and is not a substrate of cytochrome P450 en-
zymes. The mean elimination half-life was 52 hours in patients with ESRD.
Lanthanum carbonate is mainly excreted via the biliary route.
Therapeutic Efficacy In short-term, randomized, double-blind, multicentre trials in patients with
ESRD on stable maintenance haemodialysis or peritoneal dialysis, lanthanum
carbonate £3000mg/day was effective in reducing serum phosphate and cal-
cium ·phosphate product levels and then maintaining these levels at target, while
an increase in both these measures occurred with placebo. In a short-term,
randomized, double-blind, multicentre trial in Japanese patients with ESRD
in which phosphate binder dosages were titrated to achieve target serum phos-
phate levels, lanthanum carbonate 750–2250mg/day was noninferior to calcium
carbonate 1500–4500mg/day in reducing serum phosphate levels. In another
short-term, fixed-dosage, randomized, open-label, crossover trial, lanthanum
carbonate 2250–3000mg/day was not significantly different to sevelamer hydro-
chloride 4800–6400mg/day in reducing serum phosphate levels in patients
with ESRD on stable maintenance dialysis, according to an analysis of the intent-
to-treat population (primary analysis). If the completer population of this
study was analysed, then lanthanum carbonate was more effective than sevelamer
hydrochloride.
In randomized, open-label trials in adult patients with ESRD receiving main-
tenance haemodialysis, lanthanum carbonate 375–3000mg/day was as effective incontrolling serum levels of phosphate and calcium · phosphate product as con-
ventional phosphate binders in a 24-month study and as calcium carbonate in 6-
and 12-month studies. Extension studies demonstrated that control of serum
phosphate and serum calcium · phosphate product levels was maintained for up
to 6 years with lanthanum carbonate.
Tolerability Lanthanum carbonate was generally well tolerated in short- and long-term clin-
ical studies, with the most common adverse events being gastrointestinal (e.g.
nausea, vomiting, diarrhoea, abdominal pain and constipation) and occurring
with a similar incidence to that with other phosphate binders (including sevelamer
hydrochloride and calcium-based binders). These adverse events were minimized
by taking lanthanum carbonate with food, and generally abated over time with
continued administration. The incidence of treatment-related adverse events did
not increase with increased exposure to lanthanum carbonate, with no new or
unexpected adverse events being reported in an extension study in which patients
with ESRD received up to 6 years of treatment with this agent. Lanthanum
carbonate was associated with fewer episodes of hypercalcaemia than calcium
carbonate. With up to 6 years of lanthanum carbonate treatment, the incidence of
fractures was low (4.3%).
1. Introduction
Hyperphosphataemia is a common complicationin patients with end-stage renal disease (ESRD).Progressive hyperphosphataemia affects most pa-
tients with ESRD on haemodialysis and its compli-cations include hyperparathyroidism, metabolicbone disease, soft tissue and vascular calcification,and other metabolic derangements.[1,2] Moreover,inadequate phosphate control inESRD is associated
Lanthanum Carbonate: A Review 2331
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

with increased hospitalization and prematuredeath, reduced quality of life and increased costof care.[1,3-5] Increased levels of serum phosphateas low as 6.1mg/dL have been associated with anincreased risk of all-cause mortality, while levelsof serum phosphate as low as 5.1mg/dL havebeen associated with an increased risk of cardio-vascular mortality.[5] Throughout this article,serum phosphate levels are reported in mg/dL; toconvert to mmol/L, values should be multipliedby 0.3229.
Dietary restriction of phosphate and dialysisare able to reduce serum phosphate levels; how-ever, most patients will require additional treat-ment with phosphate binders to lower serumphosphate levels to within the target range of3.5–5.5mg/dL that is recommended by the 2003Kidney Disease Outcomes Quality Initiative(KDOQI) guidelines.[6] Oral phosphate binders,which prevent dietary phosphate absorption,have been used extensively in patients with ESRDundergoing haemodialysis or peritoneal dialysis.However, because calcium is absorbed from thegastrointestinal system, the commonly usedphosphate binders calcium acetate and calciumcarbonate may contribute significantly to cal-cium loading and hypercalcaemia in patients withESRD.[7]
Lanthanum carbonate (Fosrenol�) is an alu-minium- and calcium-free phosphate binder thatis indicated for the reduction of serum phosphatein patients with ESRD.[8,9] This article provides abrief overview of the pharmacology of lantha-num carbonate and focuses on the clinical effi-cacy and tolerability of this drug in reducingserum phosphate levels in patients with ESRD.
2. Pharmacodynamic Properties
Lanthanum is a naturally occurring rare earthelement. Lanthanum carbonate dissociates in theacid environment of the upper gastrointestinaltract to release the trivalent cation lantha-num.[8,10] These ions bind with high affinity todietary phosphate that is released from the foodduring digestion.[8,11] In in vitro studies, lantha-num binds »97% of the available phosphate at thephysiologically relevant pH range of 3–5, when
lanthanum is present in a 2-fold molar excess tophosphate.[8,10] The binding affinity of lantha-num carbonate for phosphate was not altered bythe presence of bile salts, according to an in vitrostudy.[11] In the presence of bile salts (30mmol/L),there was no displacement of phosphate fromthe lanthanum-phosphate complex, whereas thesevelamer-phosphate complex released 50% ofthe phosphate.[11] Lanthanum phosphate has alow aqueous solubility, is not absorbed via thegastrointestinal tract and is excreted in the faeces(see section 3).[8,12]
Lanthanum carbonate reduces daily phos-phate absorption. In a study in 121 patients withchronic kidney disease (CKD) with residual kid-ney function (stage 3 and 4),[13] a decrease in ur-inary phosphate excretion (»300mg/day; p = 0.04vs baseline) was achieved after 8 weeks of treat-ment with lanthanum carbonate £3000mg/day.Since the amount of phosphate excreted in theurine is proportional to the amount of phosphateabsorbed in the intestine, and given a dailyphosphate intake of 1200mg (representing anintestinal absorption of »900mg), this decrease inurinary phosphate was estimated to be equivalentto a decrease of about one-third of the dailyphosphate absorption.[13]
Administration of lanthanum carbonate resultedin significantly reduced levels of serum phosphateand calcium · phosphate product in the serum ofpatients with ESRD, according to data fromclinical studies. These studies are discussed insection 4. The effects of lanthanum carbonate onserum calcium and parathyroid hormone (PTH)levels are also discussed in section 4.
Lanthanum concentrations in bone increasedover time, according to bone biopsy studies inwhich patients received up to 4.5 years of treat-ment (section 3). However, lanthanum carbonatewas not associated with any detrimental effect onbone activity, according to paired-bone biopsystudies of up to 2 years in duration.[14-17]
In a randomized, open-label study in whichpaired biopsies were available from 63 patients withESRD, the total number of patients with bone ab-normalities (such as adynamic bone, osteomalaciaor hyperparathyroidism) was reduced from 36% atbaseline to 18% after 1 year of lanthanum carbonate
2332 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

£3000mg/day treatment, but increased from 43% atbaseline to 53% after 1 year of calcium carbonate£9000mg/day treatment (see section 4 for effectsof lanthanum carbonate on serum phosphate le-vels in this trial).[14] In particular, 26% of calciumcarbonate recipients, but only one lanthanumcarbonate recipient (4%), developed adynamicbone disease. In a separate analysis of this study,assessment of activation frequency changes (ameasure of overall bone-cell activity) indicatedthat 41% of patients treated with lanthanumcarbonate moved towards normal (observed va-lues at follow-up were closer to expected valuesthan those at baseline) compared with 23% inthe calcium carbonate group, although thebetween-group difference was not statisticallysignificant.[16]
In another randomized, open-label study inpatients with ESRD, in which paired biopsieswere available from 65 patients at 1 year and56 patients at 2 years, control of serum phosphatelevels with lanthanum carbonate was associatedwith an upward trend in the levels of osteocalcinand bone-specific alkaline phosphatase, while thelevels of these parameters remained constant inpatients treated with comparator phosphatebinders; however, at study endpoint, the between-group difference was not significant.[17] The per-centage of patients with improved bone turnover(changes in activation frequency and bone for-mation rate compared with normal values) after1 year, but not 2 years, was significantly higher(p < 0.05) with lanthanum carbonate than withcomparator phosphate binders. After 2 years oftreatment, the percentage of patients with re-duced bone volume was significantly lower withlanthanum carbonate than with comparatorphosphate binder treatment (15.6% vs 37.5%;p< 0.05).[17] In an extension study involving93 patients with ESRD treated with lanthanumcarbonate (see section 4 for further study designdetails), in which 22 patients entered a sixth yearof treatment, bone-specific alkaline phosphataseand osteocalcin levels generally remained con-stant throughout the study.[18]
Assessment of changes in cognitive function in360 patients with ESRD undergoing haemo-dialysis indicated that there was no significant
difference in the decline in cognitive functionthat occurred over a 2-year period betweenpatients randomized to lanthanum carbonateand those randomized to alternative phosphatebinders.[19]
3. Pharmacokinetic Properties
Lanthanum carbonate acts locally in the lu-men of the stomach and upper small intestinewhere the binding between lanthanum and diet-ary phosphate forms insoluble lanthanum phos-phate, which is then passed out unabsorbed in thefaeces (section 2). Thus, the efficacy of lanthanumcarbonate is not dependent on plasma con-centrations of lanthanum. Nevertheless, it is im-portant to understand the disposition of the drugso that its clinical tolerability can be assessed.[20]
Lanthanum carbonate is minimally absorbedfollowing oral administration of single or multi-ple doses of lanthanum carbonate (absolutebioavailability <0.002%).[8,9,20,21]
In patients with ESRDwho were administeredlanthanum carbonate 1000mg three times dailyfor 10 days, the mean maximum plasma con-centration (Cmax) of lanthanum was 1.0 ng/mLand the mean lanthanum area under the plasmaconcentration-time curve (AUC) from time zeroto the time of the last measurable concentrationwas 31.10 ng�h/mL.[9,20] The timing of adminis-tration (with or 30 minutes after a meal) of lan-thanum carbonate had no differential effect onthe Cmax or AUC of lanthanum.[8,20]
Long-term studies in which patients receivedlanthanum carbonate for up to 6 years haveindicated no increase in plasma lanthanum con-centrations over this time period.[18,22] In a long-term, open-label, phase III study in 1359 patientswith ESRD, plasma lanthanum concentrationschanged from below the lower limit of quantifi-cation at baseline to a mean value of 0.5 ng/mLat week 7, and remained at this concentrationfor the rest of the 52-week study in recipients oflanthanum carbonate (titrated to obtain targetphosphate levels; see section 4 for further studydesign details).[22] Similarly, in an extension studyin 93 patients with ESRD (22 of whom entered asixth year of lanthanum carbonate therapy; see
Lanthanum Carbonate: A Review 2333
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

section 4 for further study design details), medianplasma lanthanum concentrations which werezero at baseline, increased to 0.3 ng/mL (range0.0–4.2 ng/mL) after 6 months of treatment andremained within the range of 0.0–13.9 ng/mLover the total study duration of up to 6 years; thelatter value being due to a single outlying value ina single patient.[18]
In vitro studies indicated that lanthanum bindsextensively to plasma proteins including humanserum albumin, a1-acid glycoprotein and trans-ferrin (>99%).[8] In long-term animal studies,lanthanum concentrations increased over timein several tissues, including the gastrointestinaltract, bone and liver, and were several orders ofmagnitude higher than those in the plasma.[8,9,20]
The increased concentration of lanthanum in theliver in animal studies is consistent with thehepatic route of elimination of lanthanum car-bonate. However, in clinical studies in which pa-tients received up to 6 years of treatment withlanthanum carbonate,[23] there was no evidencethat this agent had adverse effects on the liver (seesection 5).
Lanthanum does not appear to cross theblood-brain barrier, according to data from ani-mal studies.[8,20,24]
Bone biopsies (iliac crest) taken from patientswith ESRD who were treated with lanthanumcarbonate for up to 4.5 years indicated an in-crease in bone lanthanum concentrations overthe treatment period, although lanthanum con-centrations remained low.[14-17,25] The highestbone lanthanum concentration reported in anyindividual patient was »10 mg/g wet weight bone(data estimated from a graph), according topooled data from patients treated with lantha-num carbonate for up to 4.5 years (105 intent-to-treat [ITT] biopsies).[25] Data from patientsenrolled in an open-label trial (22 paired biopsiesavailable) indicated mean bone lanthanum con-centrations of 0.08 mg/g wet weight bone at base-line, which increased after 2 years to 1.68 mg/g wetweight bone.[17] Bone biopsies of patients ad-ministered lanthanum carbonate at dosages up to3000mg/day over a 2-year period (212 biopsies)indicated that lanthanum bone disposition in-creased at a yearly mean rate of 0.96 mg/g wet
weight bone.[25] A model of the kinetics of lan-thanum in human bone predicted a 7-fold in-crease in total bone lanthanum after 10 years oftreatment (to reach 6.6 mg/g wet weight bone).[25]
After treatment cessation, the fractional loss oflanthanum from bone was estimated to be »13%per year (p < 0.001). The low amounts of lantha-num in bone do not appear to adversely affectbone-cell activity (see section 2).
Lanthanum is not metabolized and is neither asubstrate nor an inhibitor of cytochrome P450enzymes.[20] Lanthanum carbonate is mainly ex-creted via the biliary route, with only 0.00003%excreted via the renal route in healthy subjects(renal clearance rate of 1.36mL/min, represent-ing <2% of the total plasma clearance).[21] Themean elimination half-life of lanthanum in pa-tients with ESRD who were administered lan-thanum carbonate 3000mg/day for 10 days was52.3 hours.[20]
The pharmacokinetics of lanthanum carbo-nate in patients with both chronic renal failureand hepatic impairment have not been studied.However, in phase III studies in patients withchronic renal failure with coexisting hepatic dis-orders, there was no evidence of increased plasmaexposure to lanthanum or worsening hepaticfunction after treatment with lanthanum carbo-nate for up to 2 years.[20]
In healthy volunteers, coadministration oflanthanum carbonate with a single dose of me-toprolol 100mg, digoxin 0.5mg or warfarin10mg had no clinically relevant effect on thepharmacokinetic parameters of these drugs.[8,9,20]
The pharmacokinetic parameters of lanthanumcarbonate were not affected by coadministrationwith citrate-containing compounds.[8] However,coadministration of lanthanum carbonate andciprofloxacin decreased the mean ciprofloxacinAUC from time zero to infinity and Cmax by ap-proximately 50%.[26]
Lanthanum carbonate may increase gastric pH,so the manufacturer’s prescribing information re-commends that compounds that are known to inter-act with antacids should not be takenwithin 2 hoursof lanthanum carbonate administration.[8,9] How-ever, in simulated gastric fluid, precipitation betweenlanthanum and warfarin, digoxin, furosemide,
2334 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)
phenytoin, metoprolol or enalapril did not occur,suggesting a low potential for lanthanum carbo-nate to affect the absorption of these drugs.[8,9,20]
A single, chewable 1000mg tablet of lantha-num carbonate (optimized formulation) demon-strated bioequivalent pharmacokinetic parameters(Cmax and AUC from 0 to 48 hours) to four250mg tablets of lanthanum carbonate in a3-day, randomized, open-label, crossover studyin 52 healthy volunteers (data available from anabstract).[27]
4. Therapeutic Efficacy
The therapeutic efficacy of lanthanum carbo-nate in reducing serum phosphate levels in patientswith ESRD has been investigated in short-term(£6 weeks; section 4.1)[28-34] and in longer-term(£24 months; section 4.2)[14,22,35] trials. Efficacydata are also available from open-label exten-sions[18,36,37] (up to a total of 6 years of treatment)of some of these trials[14,22,28,32,35] (section 4.2).
This section will focus on trials in which pa-tients were treated with lanthanum carbonate£3750mg/day. In most trials, lanthanum carbo-nate was administered orally at a dosage of225–3000mg/day as chewable tablets dividedevenly between mealtimes. Patients were gen-erally permitted to continue with previous vita-min D supplementation.
Patients enrolled in these studies had ESRD,were on stable maintenance haemodialysis (threetimes per week with a consistent type of dialysisequipment/fluids/time on dialysis)[14,22,28-35] orcontinuous ambulatory peritoneal dialysis,[14,30,32]
were aged ‡18 years and required treatmentfor hyperphosphataemia (serum phosphatelevel >5.6mg/dL,[28-31,33,35] >5.9mg/dL[22,32] or‡6.0mg/dL[34] or not stated[14] after a washoutphase of 1–3 weeks).
Exclusion criteria included severe hyperpar-athyroidism (PTH levels of >500 to >1000pg/mL),severe hypercalcaemia (serum calcium >11mg/dL),uncontrolled concurrent illness and abnor-mal laboratory values (excluding markers ofESRD).[14,22,28-33,35]
The mean patient age ranged from 53–60 yearsand the duration on dialysis ranged from
0.2–33.3 years.[14,22,28-35] One trial was conductedin Chinese patients[31] and two others includedJapanese patients.[29,33]
Primary endpoints included the reduction inpredialysis serum phosphate levels (from the endof the washout phase[28,29,33-35]), the predialysisserum phosphate levels at the end of the main-tenance phase,[31,32] and/or the percentage ofpatients with controlled serum phosphate le-vels[30,32] or the presence/absence of hypercalcae-mia at study endpoint.[33] The effect of phosphatecontrol on renal bone disease (see section 2) wasthe primary endpoint in one long-term study,[14]
and tolerability, rather than efficacy, was theprimary endpoint in another long-term study;[22]
nevertheless, because control of phosphate wasalso assessed in these studies, they have been in-cluded in this section. Other endpoints includedserum calcium, calcium ·phosphate product andPTH levels.[14,22,28-33,35]
4.1 Short-Term Therapy
Two dose-ranging, randomized, double-blind,placebo-controlled, multicentre trials (section4.1.1 and table I),[28,29] three randomized, double-blind, placebo-controlled, multicentre maintenancestudies (section 4.1.1 and table II),[30-32] a ran-domized, dose-titration, double-blind, compara-tor-controlled, multicentre, noniferiority trial(section 4.1.2 and table III)[33] and a randomized,fixed-dosage, open-label, comparator-controlled,multicentre trial (section 4.1.3)[34] have in-vestigated the short-term (£6 weeks) efficacy oflanthanum carbonate in reducing serum phos-phate levels in patients with ESRD.
4.1.1 Comparisons with Placebo
In the two dose-ranging, placebo-controlledtrials, 145[28] and 156[29] patients with a serumphosphate level of ‡5.6mg/dL at the end of thewashout phase were randomized to lanthanumcarbonate (see table I for dosages) or placebo.The total duration of double-blind treatment was6 weeks, with 144[28] and 142[29] patients includedin the ITT efficacy population (patients who hada baseline measurement and at least one post-baseline measurement of serum phosphate).
Lanthanum Carbonate: A Review 2335
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)
In the placebo-controlled, maintenance trials,after a washout phase, patients (n = 59,[30] 73[31]and 126[32]) with serum phosphate levels of>5.6mg/dL[30,31] or >5.9mg/dL[32] entered an open-label, dose-titration phase of 4[30,31] or 6[32] weeks.During this phase, lanthanum carbonate was ti-trated to achieve a target serum phosphate levelof £5.6[30,31] or £5.9[32] mg/dL. Patients (n = 36,[30]61[31] and 94[32]) achieving these target serumphosphate levels were eligible to enter the 4-week,double-blind, maintenance phase of the trial,during which they were randomized to receiveplacebo or to continue with lanthanum carbonateat the dosage required to achieve target levels ofserum phosphate. The ITT population consistedof 36,[30] 61[31] and 93[32] patients. The number ofpatients completing the randomized, maintenancephase of the trials was 34,[30] 42[31] and 82.[32]
Outcomes
Short-term trials in patients with ESRD de-monstrated that lanthanum carbonate was sig-nificantly more effective than placebo in reducing
serum phosphate levels and then maintainingthese levels at target.[28-32]
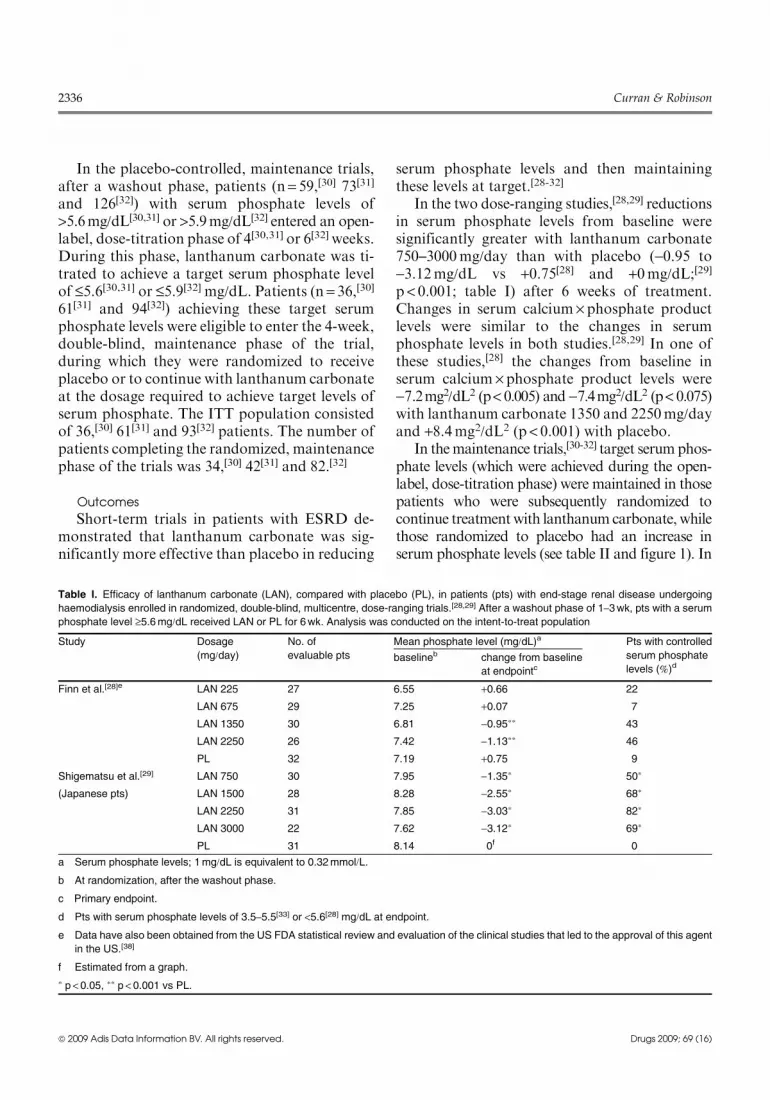
In the two dose-ranging studies,[28,29] reductionsin serum phosphate levels from baseline weresignificantly greater with lanthanum carbonate750–3000mg/day than with placebo (-0.95 to-3.12mg/dL vs +0.75[28] and +0mg/dL;[29]p < 0.001; table I) after 6 weeks of treatment.Changes in serum calcium · phosphate productlevels were similar to the changes in serumphosphate levels in both studies.[28,29] In one ofthese studies,[28] the changes from baseline inserum calcium ·phosphate product levels were-7.2mg2/dL2 (p< 0.005) and -7.4mg2/dL2 (p< 0.075)with lanthanum carbonate 1350 and 2250mg/dayand +8.4mg2/dL2 (p < 0.001) with placebo.
In themaintenance trials,[30-32] target serumphos-phate levels (which were achieved during the open-label, dose-titration phase) were maintained in thosepatients who were subsequently randomized tocontinue treatmentwith lanthanumcarbonate, whilethose randomized to placebo had an increase inserum phosphate levels (see table II and figure 1). In
Table I. Efficacy of lanthanum carbonate (LAN), compared with placebo (PL), in patients (pts) with end-stage renal disease undergoing
haemodialysis enrolled in randomized, double-blind, multicentre, dose-ranging trials.[28,29] After a washout phase of 1–3wk, pts with a serum
phosphate level ‡5.6mg/dL received LAN or PL for 6wk. Analysis was conducted on the intent-to-treat population
Study Dosage
(mg/day)No. of
evaluable pts
Mean phosphate level (mg/dL)a Pts with controlled
serum phosphate
levels (%)dbaselineb change from baseline
at endpointc
Finn et al.[28]e LAN 225 27 6.55 +0.66 22
LAN 675 29 7.25 +0.07 7
LAN 1350 30 6.81 -0.95** 43
LAN 2250 26 7.42 -1.13** 46
PL 32 7.19 +0.75 9
Shigematsu et al.[29] LAN 750 30 7.95 -1.35* 50*
(Japanese pts) LAN 1500 28 8.28 -2.55* 68*
LAN 2250 31 7.85 -3.03* 82*
LAN 3000 22 7.62 -3.12* 69*
PL 31 8.14 0f 0
a Serum phosphate levels; 1mg/dL is equivalent to 0.32mmol/L.
b At randomization, after the washout phase.
c Primary endpoint.
d Pts with serum phosphate levels of 3.5–5.5[33] or <5.6[28] mg/dL at endpoint.
e Data have also been obtained from the US FDA statistical review and evaluation of the clinical studies that led to the approval of this agent
in the US.[38]
f Estimated from a graph.
* p <0.05, ** p <0.001 vs PL.
2336 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

these trials, the differences in serum phosphatelevels between the lanthanum carbonate andplacebo groups at study endpoint were 1.45,[30]
2.1[31] and 1.9[32] mg/dL (all p < 0.001). Sig-nificantly more patients treated with lanthanumcarbonate (65%,[30] 60%[31] and 59%[32]) achievedserum phosphate level control than patientstreated with placebo (21%,[30] 10%[31] and 23%;[32]
see table II for p-values).Lanthanum carbonate was also effective in
controlling serum calcium ·phosphate productlevels in the two treatment maintenance trials thatreported this parameter.[31,32] In the phase IIItrial,[32] serum calcium· phosphate product levelswere significantly lower at treatment end withlanthanum carbonate 375–3000mg/day than withplacebo (between-group difference of -14.22mg2/dL2; p< 0.0001). There was a significant increasein serum calcium ·phosphate product levels attreatment end compared with the end of the dose-titration phase in placebo, but not in lanthanumcarbonate, recipients (p< 0.0001).
Levels of PTH increased during the washoutphase, but decreased during the lanthanum car-bonate dose-titration phase in the treatment
maintenance studies.[30-32] PTH levels remainedwithin those recommended in KDOQI guidelines(150–300 ng/L) throughout the studies in bothtreatment groups. In the phase III trial, PTH le-vels were significantly lower in the lanthanumcarbonate group than the placebo group (209 vs292 ng/L; p< 0.01) at treatment end.[32]
4.1.2 Comparison with Calcium Carbonate
After a 2-week, washout phase, 259 Japanesepatients with a serum phosphate level of ‡5.6 and<11mg/dLwere randomized to 8 weeks of double-blind treatment with lanthanum carbonate orcalcium carbonate (table III).[33] Lanthanum car-bonate was initiated at 750mg/day and calciumcarbonate was initiated at 1500mg/day and thenthe dosage of both phosphate binders was up-titrated every 2 weeks to achieve a target serumphosphate level of 3.5–5.5mg/day; 258 evaluablepatients were included in the ITT efficacy analysis.
Outcomes
Lanthanum carbonatewas noninferior to calciumcarbonate in reducing serum phosphate levels inJapanese patients with ESRD (table II).[33] The least
Table II. Efficacy of lanthanum carbonate (LAN) compared with placebo (PL) in patients (pts) with end-stage renal disease requiring treat-
ment for hyperphosphataemia enrolled in short-term, placebo-controlled, multicentre trials.[30-32] After a washout phase of 1–3wk, pts with a
serum phosphate level >5.6[30,31] or >5.9[32] mg/dL underwent an open-label, dose-titration phase of 4[30,31] or 6[32] wk. Pts with a serum
phosphate level of £5.6[30,31] or £5.9[32] mg/dL were eligible to enter the 4-wk, randomized, double-blind, placebo-controlled, maintenance
phase of the trial
Study Dosage (mg/day) Pt no. at start
of double-blind
phase
Mean phosphate level (mg/dL)a Pts with controlled
serum phosphate
levels at endpoint (%)cend of washout baselineb endpointb change from
baseline at
endpoint
Al-Baaj et al.[30]d LAN 250–2250 17 7.0 5.2 4.84*** 65*e
PL 19 7.0 5.2 6.29 21e
Chiang et al.[31] LAN 375–3000 30 7.7 5.7 5.1***e 60***
(Chinese pts) PL 31 7.7 5.7 7.2e 10
Joy et al.[32] LAN 375–3000 49 7.69 5.49 5.94***e +0.45*** 59**e
PL 44 7.39 5.62 7.85e +2.23 23e
a Serum phosphate levels; 1mg/dL is equivalent to 0.32mmol/L.
b Baseline indicates the end of the open-label, titration phase; endpoint indicates the end of the double-blind, placebo-controlled,
maintenance phase.
c Pts with serum phosphate levels £5.6[30,31] or £5.9[32] mg/dL.
d Data have also been obtained from a report of the open-label, titration phase of this study[39] and the US FDA statistical review and
evaluation of the clinical studies that led to the approval of this agent in the US.[38]
e Primary endpoint.
* p <0.05, ** p <0.01, *** p <0.001 vs PL.
Lanthanum Carbonate: A Review 2337
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

squares mean between-group difference in the re-duction of serum phosphate levels was 0.24mg/dL(95% CI -0.09, +0.57); the upper limit of the 95%CI was lower than the predefined noninferioritymargin of 1.0mg/dL and so noninferiority of lan-thanum carbonate to calcium carbonate was es-tablished. During the double-blind phase, serumcalcium levels gradually increased in the calciumcarbonate group, but remained constant in thelanthanum carbonate group. Interestingly, the in-cidence of hypercalcaemia was significantly lowerwith lanthanum carbonate treatment than withcalcium carbonate therapy. However, the calcium·phosphate product was not significantly differentbetween the two groups at the end of the study(74.44 vs 74.69mg2/dL2).[33]
4.1.3 Comparison with Sevelamer Hydrochloride
A randomized, open-label, crossover, multicentrestudy compared the efficacy of fixed dosages oflanthanum carbonate and sevelamer hydro-chloride in 182 patients with ESRD (CKD stage5) undergoing haemodialysis.[34] Patients with aserum phosphate level ‡6.0mg/dL and a serumcalcium level ‡8.4mg/dL after a washout period of2–3 weeks were randomized to lanthanum carbo-nate 2250–3000mg/day or sevelamer hydrochlo-
ride 4800–6400mg/day for 4 weeks (see table IVfor further study design details). Patients thenunderwent a second washout period of 2 weeks and
Table III. Efficacy of lanthanum carbonate (LAN) compared with calcium carbonate (CaC) in Japanese patients (pts) with end-stage renal
disease requiring treatment for hyperphosphataemia.[33] After a washout phase of 2wk, pts with a predialysis serum phosphate level of ‡5.6and <11.0mg/dL enrolled in this multicentre, noninferiority trial entered the 8-wk, randomized, double-blind phase of the study, during which
LAN was initiated at a dosage of 750mg/day and CaC was initiated at a dosage of 1500mg/day; phosphate binder dosages were then titrated
every 2wk to achieve target serum phosphate levels of 3.5–5.5mg/dL
Dosage
(mg/day)No. of
evaluable pts
Mean phosphate level (mg/dL)a Pts with serum
phosphate levels
controlledd (%)
Pts with
hypercalcaemia (%)c,e,fbaselineb least-squares mean
change from baseline
at endpointc
LAN 750–2250 126 8.35 -2.58g 75 5.7*
CaC 1500–4500 132 8.38 -2.82 82 30
a Serum phosphate levels; 1mg/dL is equivalent to 0.32mmol/L.
b After a washout period of 2wk.
c Co-primary endpoint.
d Pts with serum phosphate levels of 3.5–5.5mg/dL.
e Pts with serum calcium >10.4mg/dL.
f Serum calcium levels; 1mg/dL is equivalent to 0.249mmol/L.
g The difference in the least squares mean reduction of serum phosphate levels between LAN and CaC was 0.24mg/dL (95% CI -0.09,+0.57); the upper limit of the 95% CI was lower than the predefined noninferiority margin of 1.0mg/dL and so noninferiority of LAN to CaC
was established.
* p <0.001 vs CaC.
0
1
2
3
4
5
6
7
8
9
0−3 to −1 2 4 6 8 10Time (wk)
Ser
um p
hosp
hate
leve
ls (
mg/
dL)
Washoutphase
Dose-titrationphase
Randomized,maintenance phase
*
Visit1
LAN (n = 49)PL (n = 44)
Fig. 1. Serum phosphate levels in patients (pts) with end-stage re-nal disease treated with lanthanum carbonate (LAN) or placebo (PL)in a randomized, double-blind, multicentre, phase III trial.[32] After aninitial assessment (visit 1), pts underwent a washout phase of1–3wk. Pts with a serum phosphate level >5.9mg/dL then enteredan open-label, dose-titration phase of 6wk during which LAN(375–3000mg/day) was titrated to achieve serum phosphate control(£5.9mg/dL). Pts were then randomized to receive double-blindtreatment with LAN or PL during a 4-wk, maintenance phase. Theintent-to-treat population was analyzed. * p <0.0001 vs LAN.
2338 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

switched to the alternative phosphate binder for4 weeks. An open-label design was chosen for thisstudy as the differences in formulation (chewablevs non-chewable) in the two phosphate binderswould have meant that blinding of treatmentwould have necessitated double-dummy tabletsand consequently an unmanageable tablet bur-den. The ITT population (patients who had re-ceived at least one does of study medication andhad at least one valid post-dose serum phosphatemeasurement) consisted of 174 patients.
Outcomes
Lanthanum carbonate was at least as effectiveas sevelamer hydrochloride in reducing serumphosphate levels from baseline, but did so with alower tablet burden (three vs eight daily tablets inthe last 3 weeks of treatment). At the end of treat-ment (week 4/10), serum phosphate levels werereduced by 1.7mg/dL with lanthanum carbonateversus 1.4mg/dL with sevelamer hydrochloride,according to the last-observation-carried-forwardanalysis of the ITT population (primary end-point; table IV); there was no significant between-group difference. However, when the completerpopulation (see table IV for definition) was
analyzed, serum phosphate levels were reducedto a greater extent with lanthanum carbonatethan with sevelamer hydrochloride (table IV;difference of least squares mean -0.50mg/dL;p = 0.007).[34]
There were slight increases in serum calciumlevels with lanthanum carbonate (mean increaseof 0.1mg/dL) compared with a mean decrease of0.1mg/dLwith sevelamer hydrochloride (p= 0.025),but these changes were not considered to beclinically significant.[34]
4.2 Long-Term Therapy
4.2.1 Comparative Trials
The efficacy of lanthanum carbonate has beencompared with that of conventional phosphatebinders in randomized, open-label, multicentre trials(table V).[14,22,35] After completing a 1- to 3-weekwashout phase, patients (n= 98,[14] 800[35] and1359[22]) with a serum phosphate level, where stated,of >5.58mg/dL[35] or ‡5.9[22] mg/dL were random-ized to lanthanum carbonate or a conventionalphosphate binder (calcium carbonate[14,35] or vari-ous others[22]). Phosphate binders were then titratedto achieve target serumphosphate levels (£5.58[35] or
Table IV. Efficacy of lanthanum carbonate (LAN) compared with sevelamer hydrochloride (SEV) in patients (pts) with end-stage renal
disease requiring haemodialysis.[34] After a washout phase of 2–3wk, pts with a predialysis serum phosphate level of ‡6.0mg/dL and a serum
calcium level of ‡8.4mg/mL enrolled in this open-label, cross-over, multicentre trial were randomized to LAN or SEV. LAN was initiated at a
dosage of 2250mg/day and SEV was initiated at a dosage of 4800mg/day. After 1 wk of treatment, LAN was increased to a dosage of
3000mg/day (one 1000mg chewable tablet three times per day) and SEV was increased to a dosage of 6400mg/day (eight 800mg tablets per
day). Following 4wk of treatment, pts underwent a second washout period of 2wk and switched to the alternative phosphate binder for 4wk
Dosage (mg/day) No. of pts in ITT
analysis
[completersa]
Mean serum phosphate level (mg/dL)b
for ITT population [completersa]
Mean serum calcium level (mg/dL)c
baseline change from baseline
at treatment endd,ebaseline change from baseline at
treatment endd
LAN 2250–3000 90 [59] 7.5 [7.4] -1.7f [1.75**g] 9.2 +0.1*
SEV 4800–6400 84 [60] 7.3 [7.3] -1.4f [1.25g] 9.2 -0.1a Pts who completed 4wk of treatment with both phosphate binders and had a valid serum phosphorus measurement at wk 4 of each
treatment period.
b Serum phosphate levels; 1mg/dL is equivalent to 0.32mmol/L.
c Serum calcium levels; 1mg/dL is equivalent to 0.249mmol/L.
d Wk 4/10.
e Last observation carried forward.
f Primary endpoint.
g Data estimated from a graph.
ITT = intent-to-treat; * p= 0.025, ** p= 0.007 vs SEV.
Lanthanum Carbonate: A Review 2339
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

£5.9[22] mg/dL where stated) over a 5-,[35] 6-[22] or8-week[14] open-label phase. Patients then con-tinued on their optimal phosphate binder dosageduring a maintenance phase for a total treatmentduration of 6,[35] 12[14] or 24[22] months.
Lanthanum carbonate reduced and then main-tained serum phosphate levels to below target inpatients with ESRD, according to data from 6- to24-month, open-label, comparative trials (tableV).[14,22,35] At endpoint, the number of patients withserum phosphate levels at target was similar withlanthanum carbonate or the comparator phosphatebinder(s) in the 6-[35] and 24-month[22] trials (tableV).
The changes in serum calcium·phosphate prod-uct levels tended to reflect the changes in serumphosphate levels. In the 6-month trial,[35] the reduc-tions from baseline in serum calcium·phosphateproduct levels were greater with lanthanum carbon-ate than with calcium carbonate at week 17 (-22.28vs -16.71mg2/dL2; p= 0.009), but not at week 25(-19.68 vs 15.69mg2/dL2). In the 24-month
study,[22] the serum calcium and the serum cal-cium·phosphate product level decreased duringthe titration phase and then remained relativelyconstant during the maintenance phase in recipientsof lanthanum carbonate and in recipients of com-parator phosphate binders.
In patients randomized to lanthanum carbonate,median PTH levels attained those recommended bythe KDOQI[40] (150–300pg/mL) during the dose-titration phase and then remained within this rangefor the rest of the 6[35] or 24[22] months of these trials.However, in patients randomized to comparatorphosphate binders (calcium carbonate[35] or variousothers[22]), serum PTH levels were below the re-commended values at the end of the titration phaseand throughout the treatment phase in both trials.
4.2.2 Extension Studies
Several open-label extensions[18,36,37] of previoustrials have been conducted. In particular, this sec-tion will focus on an open-label, 2-year extension
Table V. Efficacy of lanthanum carbonate (LAN) compared with phosphate binders (various [VAR] or calcium carbonate [CaC]) in reducing
serum phosphate levels in patients (pts) with end-stage renal disease in long-term, open-label, multicentre trials. Pts underwent a washout
phase of 1–3wk to achieve a pre-dialysis serum phosphate level, where stated, of >5.58,[35] or >5.9[22] mg/dL.[14] Pts were then randomized to
LAN or comparative phosphate binder (VAR[22] or CaC[14,35]). After a 5-,[35] 6-[22] or 8-wk[14], dose-titration phase to achieve, where stated, a
target serum phosphate level of £5.58[35] or £5.9[22] mg/dL, pts entered a maintenance-treatment phase. Analyses are based on the intent-to-
treat population
Study Dosage
(mg/day)Duration of
open-label
maintenance
phase (mo)
No. of
evaluable
pts
Mean phosphate level (mg/dL)a Phosphate-
controlled pts at
end of titration
[end of study] (%)b
end of washout
phase
baseline of
maintenance
phase
end of
maintenance
phase
D’Haese et al.[14]c LAN £3750 12 49 NS 5.5 5.7 NS
CaC £9000 49 NS 5.9 5.3 NS
Finn et al.[22]d LAN 750–3000 24 682 8.0e 6.5e 6.2e 43e [46]
VARf 677 8.0e 5.8e 6.1e 57e [49]
Hutchison et al.[35] LAN 375–3000 6 510g 8.28 5.79 5.58e 57.8 [65.8]
CaC 1500–9000 257g 8.34 5.15 5.58e 70.3* [63.9]
a Serum phosphate: 1mg/dL is equivalent to 0.32mmol/L.
b Pts with serum phosphate levels of £5.58[35] or £5.9[22] mg/dL (£1.8 or £1.9mmol/L) at end of the maintenance phase.
c Tolerability, not efficacy, was the primary endpoint in this study; data relating to this trial have also been obtained from Freemont et al.[16]
d Data have also been obtained from the US FDA statistical review and evaluation of the clinical studies that lead to the approval of this agent
in the US.[38]
e Estimated from a graph.
f Calcium acetate (43%), calcium carbonate (36%), sevelamer (16%), other (4%), not reported (2%); the dosage of the active comparator was
based on current prescribing information or that commonly utilized.
g Pts randomized to treatment who received at least one dose of study medication and for whom evaluable data are available.
NS = not stated; * p= 0.002 vs LAN.
2340 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

(involving 93 patients)[18] of four previous studies(with up to 4 years of total treatment),[14,22,35,36]
which enabled the assessment of up to 6 years oflanthanum carbonate treatment. In this extensionstudy, the dosage of lanthanum carbonate was2250 or 3000mg/day in 65.5% of the patients,with 22 patients entering a sixth year of treatment.During the 2-year period, 16 patients withdrewfrom the study after receiving a kidney transplantand five patients died.[18]
These open-label extension trials demonstratedthat lanthanum carbonate was effective in main-taining long-term control of serum phosphatelevels.[18,36,37] In the extension trial in which pa-tients received up to 6 years of lanthanum carbo-nate, serum phosphate levels (which were 7.8mg/dL at baseline) were reduced to 5.50mg/dL at6months and then remained at this level through-out the follow-up period (mean 5.74mg/dL at3 years, mean 5.23mg/dL at 5 years and were4.5–6.5mg/dL at 6 years).[18] This control wasachieved with a maintenance dosage of lantha-num carbonate of either 2250 or 3000mg/day,which is equivalent to one 750 or 1000mg tabletwith each meal (a total of three tablets perday).[18]
Control of serum calcium · phosphate productlevels was also maintained with long-term lan-thanum carbonate therapy.[18,36,37] Mean cal-cium · phosphate product levels were reducedin lanthanum carbonate recipients from70.2mg2/dL2 at baseline to 50.4mg2/dL2 after6 months of therapy and then remained at thislevel after 3, 5 and 6 years of therapy (53.75, 50.05and »55.0mg2/dL2, respectively) in the extensionstudy with the longest follow-up time.[18] SerumPTH levels remained stable and within KDOQItarget levels throughout the 6-year extensionstudy with lanthanum carbonate treatment.[18]
5. Tolerability
The tolerability of oral lanthanum carbonatehas been evaluated in patients with ESRD onmaintenance haemodialysis or peritoneal dialysisenrolled in randomized, short-term (£6 weeks[28-33])and long-term (up to 24 months)[14,22,35] trials, aswell as open-label extension studies,[18,36,37] with
up to a total of 6 years of follow-up (see section 4for study design details). Lanthanum carbonatewas generally administered at a dosage of£3000mg/day.
Lanthanum carbonate was generally well tol-erated in short- and long-term clinical stu-dies,[14,22,28-33,35] with the most common adverseevents reported being gastrointestinal. These ad-verse events were generally mild or moderate inseverity, were minimized by taking lanthanumcarbonate with food, and generally abated overtime with continued administration of thisagent.[9]
According to a combined analysis of short-term, double-blind, placebo-controlled studies(reported in the manufacturer’s prescribing in-formation[8]) in which patients with ESRD wererandomized to lanthanum carbonate (n = 180) orplacebo (n = 95) for 4–6 weeks, the most commonadverse events that were reported more fre-quently (>5% between-group difference) withlanthanum carbonate than placebo includedgastrointestinal adverse events (nausea, vomitingand abdominal pain), as well as dialysis graftocclusion (see figure 2). Similarly, in the long-term 6-[35] and 24-month,[22] randomized, open-label clinical trials, the most commonly reportedadverse events with lanthanum carbonate orcomparator phosphate binders (including calciumcarbonate, calcium acetate and sevelamer hydro-chloride) were gastrointestinal (nausea, vomiting,diarrhoea, abdominal pain and constipation;figure 2).[8] The incidence of gastrointestinaladverse events was similar in both treatmentgroups. Other common treatment-related ad-verse events associated with either lanthanumcarbonate or comparator phosphate binders in-cluded dialysis graft complications, headache,dialysis graft occlusion, hypotension, rhinitis,bronchitis and hypercalcaemia (figure 2).[8,22,35]
The incidence of treatment-related adverseevents did not increase with increasing exposure tolanthanum carbonate, with no new or unexpectedadverse events being reported in an extension studyin which 93 patients with ESRDwere treated for upto 6 years with lanthanum carbonate. The overallincidence of treatment-related adverse events was26% and, as in the comparator-controlled studies,
Lanthanum Carbonate: A Review 2341
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

most adverse events were gastrointestinal in na-ture.[18] Overall, lanthanum carbonate-relatedgastrointestinal adverse events occurred in15% of US patients and 27% of European pa-tients enrolled in the extension trial, with nogastrointestinal adverse events being reportedafter 3 years of lanthanum carbonate exposure
in the US patients or after 4 years in Europeanpatients.[18]
The incidence of hypercalcaemia reportedwith lanthanum carbonate in clinical trials waslow (<6%).[8,22,35] The percentage of patients withhypercalcaemia was 4% with lanthanum carbo-nate versus 8% with comparator phosphate bin-ders in the 24-month, open-label trial[8,22] and0.4% with lanthanum carbonate versus 20.2%with calcium carbonate in the 6-month trial[8,35]
(figure 2; p-values not stated). In the open-labelextension study in which patients received lan-thanum carbonate for up to 6 years, serum cal-cium levels remained stable over time and theincidence of hypercalcaemia was 5%.[35] In arandomized, double-blind trial in 258 Japanesepatients with ESRD (section 4.1.1), the incidenceof hypercalcaemia (serum calcium >10.4mg/dL)was significantly lower with lanthanum carbo-nate than with calcium carbonate therapy (5.7%vs 30.0%; p < 0.0001).[33]
Lanthanum carbonate was not associated withadverse effects on haematological laboratoryparameters, including serum haemoglobin, hae-matocrit or mean cell volume after up to 6 yearsof treatment.[18]
Lanthanum carbonate (for up to 6 years) wasnot associated with adverse effects on the liver inpatients with chronic liver disease receiving hae-modialysis, according to an analysis[23] of phase IIIstudies[14,22,35,36] and the extensions of these stu-dies. Changes in transaminase, bilirubin andalkaline phosphatase levels were minimal withlong-term treatment (up to 6 years) and were si-milar to those in the short-term comparativestudies.[23] In a 24-month, open-label study,[22]
liver and biliary system events (WHO preferredterm) were reported in 4.1% of lanthanum carbo-nate recipients and 6.9% of recipients of the com-parator phosphate binder.[23] With lanthanumcarbonate versus comparator phosphate bindertreatment, the most common liver and biliary sys-tem events (adjusted for treatment exposure inthe alternative therapy group) were hepatic func-tion abnormalities (0.9% vs 1.3%), cholelithiasis(0.7% vs 1.4%) and increased g-glutamyl trans-ferase levels (0.7% vs 1.0%).[23] In the 93 patients
0
0
5
2
4
6
8
10
40
35
30
25
20
15
10
12
a
b
Nausea Vomiting Dialysis graftocclusion
Abdominalpain
Per
cent
age
of p
tsP
erce
ntag
e of
pts
LAN (n = 180)PL (n = 95)
Trial A: LAN (n = 682)Trial A: VAR (n = 676)Trial B: LAN (n = 533)Trial B: CaC (n = 267)
Nause
a
Vomitin
g
Dialys
is gr
aft c
ompli
catio
n
Diarrh
oea
Heada
che
Dialys
is gr
aft o
cclus
ion
Abdom
inal p
ain
Hypot
ensio
n
Consti
patio
n
Bronc
hitis
Rhinitis
Hyper
calca
emia
Fig. 2. Tolerability profile of lanthanum carbonate (LAN) in patients(pts) with end-stage renal disease (ESRD). (a) Short-term trials.Percentage of pts with ESRD with treatment-emergent adverseevents reported more commonly (between-group difference >5%)with LAN than placebo (PL) in randomized, double-blind trials withtreatment durations of 4–6wk.[8] (b) Long-term trials. Percentage ofpts with treatment-related adverse events reported (‡5% in eithergroup) in a 24-mo, randomized, open-label, comparator-controlledtrial (trial A)[22] after treatment with LAN or various comparatorphosphate binder (VAR), and in a 6-month, randomized, open-labelcomparator-controlled trial[35] (trial B) after treatment with LAN orcalcium carbonate (CaC). In trial A, data have been adjusted forthe mean exposure differences between treatment groups. All datawere reported in the manufacturer’s prescribing information.[8]
2342 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

who enrolled in a final 2-year, open-label, exten-sion study (with up to 6 years follow-up), therewere no clinically relevant changes in transami-nase levels, with mean ALT and AST levels being17.3 and 17.2U/L at baseline, and 20.4 and17.9U/L at 5 years; the range of ALT and ASTvalues in the five patients who remained in thestudy after 6 years was within that observed ear-lier in the study.[23]
With up to 6 years of lanthanum carbonatetreatment, the incidence of fractures and bone-related musculoskeletal adverse events was low(4.3%).[18] The effect of lanthanum carbonate onthe number of patients with biopsy-assessed boneabnormalities is discussed in section 2.
According to a combined analysis of both the6- and 24-month, open-label, comparator-controlledtrials in which a total of 1215 patients with ESRDwere treated with lanthanum carbonate and 943patients were treated with comparator phosphatebinders, 14% of recipients of lanthanum carbo-nate withdrew due to adverse events (most gas-trointestinal).[8] In the extension study in whichpatients received up to 6 years of lanthanumcarbonate treatment, none of the 12 adverseevents that led to withdrawal (19.7% of patients)were considered to be treatment-related.[18]
The incidence and type of serious adverseevents reported in the 6-[35] and 24-month[22]
trials were those typical for patients with ESRDundergoing haemodialysis. None of the seriousadverse events in the 6-month study were con-sidered to be related to lanthanum carbonatetreatment.[35] In the 24-month study,[22] threeserious adverse events were considered to belikely to be related to treatment with lanthanumcarbonate (pancreatitis, gastrointestinal bleedand constipation). In an extension study (seesection 4.2.2) with up to 6 years of treatment,[18]
there was one serious treatment-related adverseevent (worsening gastritis in a patients with aprevious history of gastritis, abdominal wall ab-scess and peritonitis).
6. Dosage and Administration
Lanthanum carbonate is indicated to reduceserum phosphate levels in patients with ESRD in
the US,[8,41] Europe[9,41] and various other coun-tries including Japan.[42]
Lanthanum carbonate should be taken orallywith or immediately after food, with the totaldaily dose divided between meals.[8,9] Patientsshould adhere to recommended diets in order tocontrol phosphate and fluid intake.[9] Lantha-num carbonate is available as a chewable tablet,which should be chewed completely before swal-lowing; intact tablets should not be swallowed.However, tablets may be crushed in order to as-sist in chewing.
The initial total daily dose of lanthanumcarbonate recommended in the US is 1500mg.[8]
The dose of lanthanum carbonate should betitrated every 2–3 weeks until an acceptableserum phosphate level is reached.[8,9] Serumphosphate levels should be monitored duringdose-titration and regularly thereafter.[8] Mostpatients required a lanthanum carbonate dosageof 1500–3000mg/day to reduce plasma phos-phate levels to less than 6.0mg/dL.[8] Lanthanumcarbonate is available as 500, 750 and 1000mgtablets.[8,9]
Lanthanum carbonate should be used withcaution in patients with active peptic ulcer, ul-cerative colitis, Crohn’s disease or bowel ob-struction as these patients were excluded from theclinical trials described in section 4.
Local prescribing information should be con-sulted for approved label information, includingdosage information (e.g. in special patient popula-tions), contraindications and precautions for use.
7. Place of Lanthanum Carbonate in theManagement of Serum Phosphate Levelsin Patients with End-Stage Renal Disease
Phosphorus is a common element found in thebody, where most of it binds with oxygen to formphosphate.[43,44] CKD impairs the ability of thekidneys to maintain the balance between phos-phate input and output and, as renal functiondeteriorates, progressive hyperphosphataemia(plasma phosphate >4.5mg/dL) develops. Eleva-tions in levels of serum phosphate generallyoccurs when the glomerular filtration rate is<30mL/min/1.73m2.[6]
Lanthanum Carbonate: A Review 2343
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

Hyperphosphataemia can lead to secondaryhyperparathyroidism, renal osteodystrophy, andvascular and soft tissue calcification.[43] Althoughstudies have not been conducted to demonstratethe direct benefits of lowering serum phosphateon patient-level clinical outcomes (e.g. hospitali-zation, bone fracture, cardiovascular events andmortality), epidemiological studies have shown apositive association between increased serumphosphorus levels and the relative risk of mor-tality, independent of CKD stage.[4,5,45-48] TheDialysis Outcomes and Practice Patterns Study,for example, indicated a relationship betweenelevations in serum phosphate and the relativerisk of mortality that was consistent across all12 countries analyzed.[5] It is generally acceptedand biologically plausible that elevated serumphosphorus levels should be lowered in patientswith CKD stages 3–5D in an effort to controlcomplications.[45]
The US,[6] Canada,[49,50] the UK[51] andAustralia[52] have published guidelines for phos-phate levels for patients with CKD stage 5, withsome variation existing between the various guide-lines. These guidelines also recommend serumlevels for calcium, calcium · serum product andPTH in these patients. In the US (for example),the KDOQI lines recommend that serum levels ofphosphate should be maintained between 3.5 and5.5mg/dL.[6] The new Kidney Disease ImprovingGlobal Outcomes (KDIGO) clinical practiceguidelines suggest that in patients with CKDstage 3–5, serum phosphate levels should bemaintained within the normal range.[45] In thosewith stage 5D CKD, the KDIGO guidelinessuggest lowering elevated levels of serum phos-phate towards the normal range.[45] Theseguidelines also suggests maintaining serum cal-cium in the normal range in patients with CKDstages 3–5D.
Several strategies have been used to controlserum phosphate levels, including dietary con-trol, dialysis and the use of drugs that bind diet-ary phosphate and prevent its absorptionthrough the gastrointestinal tract. Althoughdietary restriction is one option for limiting theintake of phosphate, it is often impractical inmany patients, especially those who eat pre-
prepared supermarket meals.[53] Moreover, therisks associated with controlling serum phos-phate by restricting dietary protein intake mayoutweigh the benefits and may lead to greatermortality.[54] Conventional, 4-hour haemodia-lysis three times per week removes up to 900mgof phosphate each treatment, but does not gen-erally maintain phosphate levels within the re-commended targets.[7] Peritoneal dialysis is littlebetter in this respect. Slow nocturnal haemodia-lysis or daily haemodialysis are also means ofcontrolling phosphate levels that are gaining in-creased attention.[55-57]
Most patients on haemodialysis require phos-phate binder therapy to control serum phosphatelevels.[7] Ideally, phosphate binders should have ahigh binding affinity (regardless of the pH) forphosphate, have a low solubility, have low ab-sorption (preferably none) from the gastro-intestinal tract, be nontoxic and well tolerated,have a low pill burden, be palatable and be costeffective.[58] The use of phosphate-binding agentsin patients with CKD stages 3–5 and 5D is sug-gested by the new KDIGO guidelines.[45] Thecomparative features of the various phosphatebinders are shown in table VI.
Aluminium hydroxide and aluminium carbo-nate have been used as effective phosphate bin-ders since the 1970s.[7] They dissolve rapidly andbind phosphate at any pH; however, they havebeen associated with bone toxicity, cognitivedisturbances and anaemia.[59,60] Their use in thelong-term treatment of hyperphosphataemia isnot common. Calcium salts (e.g. calcium carbo-nate, calcium acetate) bind dietary phosphate lesseffectively than aluminium, but are commonlyused phosphate binders. However, since calciumcan be absorbed into the gastrointestinal system,these agents have been associated with hyper-calcaemia, especially with prolonged or high-doseuse or when administeredwith vitaminD analogues(which facilitate the absorption of calcium).[61,62]
Moreover, to achieve satisfactory phosphatecontrol, the dosages of these agents often exceedthe limits of daily calcium intake levels set by theKDOQI guidelines.[63] These guidelines recom-mend that a patient’s total intake of calcium fromdiet and drug treatment should not exceed
2344 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

2000mg/day.[40] Magnesium-based phosphatebinders have been used as an alternative tocalcium-based phosphate binders.[64,65] Becausemagnesium must be used at relatively high con-centrations and is absorbed in the intestine,adverse effects such as hypermagnesaemia anddiarrhoea are common. Studies investigatingtheir efficacy and tolerability in the long termhave not been conducted.
Sevelamer hydrochloride was the first metal-free, non-calcium phosphate binder to be ap-proved in the US and Europe for the treatment ofhyperphosphataemia in patients with ESRD onhaemodialysis or peritoneal dialysis.[66] Sevela-mer carbonate has subsequently been approvedin the US and has efficacy equivalent to that of
sevelamer hydrochloride.[67] Sevelamer is a syn-thetic ion-exchange resin that binds phosphate inexchange for chloride or carbonate ions, is re-sistant to digestive degradation and is not ab-sorbed by the intestinal tract. This process is mosteffective in the higher pH of the small intestine. Ithas been effective in lowering serum phosphatelevels in both short- and long-term studies.[67,68]
Orally administered lanthanum carbonatedissociates in the acid environment of the uppergastrointestinal tract to release cationic lantha-num, which binds dietary phosphate (section 2),is minimally absorbed (section 3) and is indicatedto reduce serum phosphate levels in patients withESRD in the US,[8,41] Europe[9,41] and variousother countries, including Japan.[42]
Table VI. Comparison of properties of phosphate-binding agents[7,58,66]
Phosphate binder Mechanism of action Advantages Disadvantages
Aluminium salts Dissociates in the GI tract;
aluminium then binds to phosphates
and forms an insoluble precipitate
High binding affinity
Low cost
Efficacy not pH dependent
Bone toxicity
Cognitive disturbances
Anaemia
Calcium acetate Dissociates in the GI tract; calcium
then binds with phosphates and
forms an insoluble precipitate
Aluminium free
Moderate binding affinity
Soluble in both an acid and basic
environment
Moderate pill burden
Lower cost vs lanthanum carbonate
or sevelamer
Lower calcium load than calcium
carbonate
Binding influenced by pH
Large tablets
Hypercalcaemia
GI adverse effects
Possible vascular calcification
Calcium carbonate Dissociates in the GI tract; calcium
then binds with phosphates and
forms an insoluble precipitate
Aluminium free
Moderate binding affinity
Moderate pill burden
Low cost
Solubility is influenced by pH
Binding influenced by pH
Unpalatable
Hypercalcaemia
GI adverse effects
Possible vascular calcification
Lanthanum carbonate Dissociates in the GI tract;
lanthanum then binds with
phosphates and forms an insoluble
precipitate
Aluminium free
Calcium free
High binding affinity
Low pill burden
Chewable tablet
Some GI absorption
GI adverse effects
Expensive
Magnesium salts Dissociates in the GI tract;
magnesium then binds with
phosphates and forms an insoluble
precipitate
Aluminium free
Calcium free
Low cost
Efficacy and tolerability not
assessed long term
Sevelamer Anion exchange resin that binds
phosphate in exchange for chloride
or carbonate ions (depending on the
formulation)
Aluminium free
Calcium free
Moderate efficacy
No GI tract absorption
Reduces total and LDL cholesterol
Expensive
Efficacy influenced by pH
High pill burden
GI adverse effects
Binds fat soluble vitamins
GI= gastrointestinal; LDL = low-density lipoprotein.
Lanthanum Carbonate: A Review 2345
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

In both short- and long-term studies, as wellas extensions of these studies (involving up to6 years of treatment), lanthanum carbonate waseffective in initially reducing serum phosphateand serum calcium ·phosphate product levelsand then maintaining these levels within targetranges for up to 6 years (section 4). Lanthanumcarbonate was noninferior to calcium carbonatein a short-term trial[33] and demonstrated similarefficacy to calcium carbonate in trials of longerduration[14,35] (section 4). In a short-term, cross-over study, lanthanum carbonate was not sig-nificantly different to sevelamer hydrochloride inreducing serum phosphate levels, according to ananalysis of the ITT population (primary analy-sis), but did so with a lower tablet burden (section4).[34] In an analysis of the completer population,lanthanum carbonate was more effective thansevelamer hydrochloride.[34] In a 24-monthtrial,[22] lanthanum carbonate reduced serumphosphate levels to a similar extent to variousphosphate binders, with no significant between-group difference in the number of patientsachieving serum phosphate targets (£5.9mg/dL)at study endpoint (46% vs 49%). However, thereis still a need for long-term, well designed studiesthat specifically compare the efficacy of lantha-num carbonate with sevelamer or calcium acet-ate, using KDOQI or KDIGO target levels. Inpatients with ESRD who were treated with lan-thanum carbonate, levels of serum PTH tendedto increase during initial treatment and thengenerally remained stable and within KDOQItarget levels in studies discussed in section 4. Todate, there are no data regarding the impact oflanthanum carbonate on vascular calcification ormortality.
Lanthanum carbonate was generally well tol-erated, with the most frequently reported adverseevents being gastrointestinal in nature and oc-curring at a similar rate to that with comparatorphosphate binders (including calcium carbonate;section 5). These adverse events were generallymild or moderate in severity, were minimized bytaking lanthanum carbonate with food, andgenerally abated over time with continued ad-ministration of this agent (section 5). However,compared with calcium carbonate, lanthanum
carbonate was associated with a lower incidenceof hypercalcaemia (section 5). A common re-sponse to the inadequate control of phosphatelevels in patients treated with calcium-basedphosphate binders is to increase the dosage,risking the development of hypercalcaemia.Lanthanum carbonate may be a suitable alter-native in patients who are inadequately con-trolled on calcium-based phosphate binders or inpatients with pre-existing hypercalcaemia. Withup to 6 years of lanthanum carbonate treatment,the incidence of fractures (4.3%) was low.
Lanthanum concentrations increased overtime in the liver in long-term animal studies,consistent with its hepatic route of elimination(section 3). However, in clinical studies in whichpatients received up to 6 years of treatment withlanthanum carbonate, there was no evidence thatthis agent had adverse effects on the liver (seesection 5).
Plasma concentrations of lanthanum re-mained stable after up to 6 years of treatment(section 3) in patients with ESRD. In contrast,bone biopsies from patients with ESRD indicatedthat lanthanum continued to be deposited intobone after 4.5 years of lanthanum carbonatetreatment (highest level in any patient of »10 mg/gwet weight bone), with lanthanum concentrationsnot reaching steady state at that point (section 3).However, lanthanum carbonate was not asso-ciated with detrimental effects on bone activity,according to bone-biopsy studies in patients withESRD who received up to 2 years of lanthanumcarbonate therapy (section 2). Moreover, paired-bone biopsy studies also indicated that lantha-num carbonate improved bone turnover after1 year of treatment and improved bone volumeafter 2 years of treatment (section 2). There wasno increase in the incidence of fractures or bone-related musculoskeletal adverse events (section 5)and generally no changes in bone-specific alkalinephosphatase or osteocalcin levels in an extensionstudy in which patients received up to 6 years oflanthanum carbonate treatment (section 2).
Nonadherence to dietary phosphate binders isprevalent in patients with ESRD,[69,70] especially ifthese patients are subject to complex treatment regi-menswith large daily tablet burdens.[71] A systematic
2346 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

review of clinical studies in which patients wereadministered phosphate binder therapy indicatedadherence rates of 22% to 74% (mean 51%), withthe variation being attributable to definition andmethods of assessment of nonadherence.[69] Achart review of patients taking phosphate bindersnoted that noncompliant patients, compared withcompliant patients, had a higher pill burden (9.3vs 8.3 pills/day), but actually took fewer pills (4.2vs 7.6 pills/day).[70] One possible explanation forthis is that failure to reach targets (often as a resultof poor compliance) may lead to increased do-sages requiring higher pill burdens, which leadto further reductions in compliance. Thus, a phos-phate binder with a lower pill burden may poten-tially increase compliance and allowmore patientsto achieve target serum phosphate levels.[12]
An optimized formulation of lanthanum car-bonate was developed to allow the administrationof smaller sized and higher dose (750 and 1000mg)tablets than the original formulation. In short-term studies,[72,73] and a longer extension study[18]
in which patients received up to 6 years of treat-ment, the optimized formulation of lanthanumcarbonate allowed the majority of patients whoachieve target phosphate levels to do so with threetablets per day. Pharmacokinetic parameters ofthis optimized formulation were bioequivalent tothose of the original formulation in healthy vo-lunteers (section 3). Other phosphate binders, suchas calcium acetate and sevelamer hydrochloride,require higher daily tablet counts to achieve targetserum phosphate levels. Moreover, according todata from one of these studies, the majority ofpatients and physicians expressed a preference forthe new formulation of lanthanum carbonate.[73]
Whether these factors ultimately translate intoimproved adherence with lanthanum carbonatecompared with other phosphate binders has yet tobe clearly established.
In conclusion, lanthanum carbonate was effec-tive in reducing levels of serum phosphate andserum calcium ·phosphate product and thenmaintaining these levels within target ranges foras long as 6 years in adult patients with ESRD onhaemodialysis or peritoneal dialysis. The reductionin serum phosphate levels was generally similarwith lanthanum carbonate to that with calcium
carbonate or sevelamer hydrochloride. Thisagent was generally well tolerated, with the mostfrequently reported adverse events being gastro-intestinal in nature and occurring at a similar rateto that with calcium carbonate. However, lan-thanum carbonate was associated with fewerepisodes of hypercalcaemia than calcium carbo-nate. Up to 2 years of treatment with lanthanumcarbonate was not associated with detrimentaleffects on bone-cell activity. Overall, lanthanumcarbonate is a valuable option for the reductionof serum phosphate levels in patients with ESRDon haemodialysis or peritoneal dialysis.
Disclosure
The preparation of this review was not supported by anyexternal funding. During the peer review process, the manu-facturer of the agent under review was offered an opportunityto comment on this article. Changes resulting from commentsreceived were made on the basis of scientific and editorialmerit.
References1. Burke SK. Phosphate is a uremic toxin. J Ren Nut 2008 Jan;
18 (1): 27-32
2. Albaaj F, Hutchison A. Hyperphosphataemia in renal fail-ure: causes, consequences and current management. Drugs2003; 63 (6): 577-96
3. Block GA, Hulbert-Shearon TE, Levin NW, et al. Associa-tion of serum phosphorus and calcium · phosphate pro-duct with mortality risk in chronic hemodialysis patients: anational study. Am J Kidney Dis 1998 Apr; 31 (4): 607-17
4. Block GA, Klassen PS, Lazarus JM, et al. Mineral meta-bolism, mortality and morbidity in maintenance hemodia-lysis. J Am Soc Nephrol 2004 Aug; 15 (4): 2208-18
5. Tentori F, Blayney MJ, Albert JM, et al. Mortality risk fordialysis patients with different levels of serum calcium, phos-phorus, andPTH: theDialysisOutcomes andPractice PatternsStudy (DOPPS). Am J Kidney Dis 2008 Sep; 52 (3): 519-30
6. National Kidney Foundation. K/DOQI clinical practiceguidelines for bonemetabolism and disease in chronic kidneydisease. Am J Kidney Dis 2003 Oct; 42 (4 Suppl. 3): S1-201
7. Ashfaq A, GitmanM, Singhal PC, et al. Emerging strategiesfor lowering serum phosphorous in patients with end-stagerenal disease. Expert Opin Pharmacother 2006; 7 (14):1897-905
8. ShireUS Inc. Fosrenol� (lanthanumcarbonate):USprescribinginformation [online]. Available from URL: http://www.fosrenol.com/PDFs/PrescribingInfo.pdf [Accessed 2009 May 10]
9. Shire Pharmaceuticals Limited. Fosrenol� 250mg, 500mg,750mg and 1000mg chewable tablets: summary of pro-duct characteristics [online]. Available from URL: http://emc.medicines.org.uk/document.aspx?documentid=19617[Accessed 2009 May 1]
Lanthanum Carbonate: A Review 2347
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)
10. Swainston Harrison T, Scott LJ. Lanthanum carbonate.Drugs 2004; 64 (9): 985-96
11. Autissier V, Damment SJ, Henderson RA. Relative in vitroefficacy of the phosphate binders lanthanum carbonateand sevelamer hydrochloride. J Pharm Sci 2007 Oct; 96(10): 2818-27
12. Sprague SM. A comparative review of the efficacy and safetyof established phosphate binders: calcium, sevelamer, andlanthanum carbonate. Curr Med Res Opin 2007 Dec; 23(12): 3167-75
13. Sprague SM, Abboud H, Qiu P, et al. Lanthanum carbonatereduces phosphorus burden in patients with CKD stages 3and 4: a randomized trial. Clin J Am SocNephrol 2009 Jan;4 (1): 175-85
14. D’Haese PC, Spasovski GB, Sikole A, et al. A multicenterstudy on the effects of lanthanum carbonate (Fosrenol�)and calcium carbonate on renal bone disease in dialysispatients. Kidney Int 2003 Jun; 63 Suppl. 85: S73-8
15. Spasovski GB, Sikole A, Gelev S, et al. Evolution of boneand plasma concentration of lanthanum in dialysis patientsbefore, during 1 year of treatment with lanthanum carbo-nate and after 2 years of follow-up. Nephrol Dial Trans-plant 2006 Aug; 21 (8): 2217-24
16. Freemont AJ, Hoyland JA, Denton J, on behalf of theLanthanum Carbonate SPD 405-303 Study Group. Theeffects of lanthanum carbonate and calcium carbonate onbone abnormalities in patients with end-stage renal disease.Clin Nephrol 2005 Dec; 64 (6): 428-37
17. Malluche HH, Siami GA, Swanepoel C, et al. Improvements inrenal osteodystrophy in patients treated with lanthanum car-bonate for two years. Clin Nephrol 2008 Oct; 70 (4): 284-95
18. Hutchison AJ, Barnett ME, Krause R, et al. Long-termefficacy and safety profile of lanthanum carbonate: resultsfor up to 6 years of treatment. Nephron Clin Pract 2008;110 (1): c15-23
19. Altmann P, Barnett ME, FinnWF, et al. Cognitive function instage 5 chronic kidney disease patients on hemodialysis: noadverse effects of lanthanum carbonate compared with stan-dard phosphate-binder therapy. Kidney Int 2007; 71 (3): 252-9
20. Damment SJP, Pennick M. Clinical pharmacokinetics of thephosphate binder lanthanum carbonate. Clin Pharmaco-kinet 2008; 47 (9): 553-63
21. Pennick M, Dennis K, Damment SJ. Absolute bioavail-ability and disposition of lanthanum in healthy humansubjects administered lanthanum carbonate. J Clin Phar-macol 2006 Jul; 46 (7): 738-46
22. Finn WF, on behalf of the SPD 405-307 Lanthanum StudyGroup. Lanthanum carbonate versus standard therapy forthe treatment of hyperphosphatemia: safety and efficacy inchronic maintenance hemodialysis patients. Clin Nephrol2006 Mar; 65 (3): 191-202
23. Hutchison AJ, Barnett ME, Krause R, et al. Lanthanumcarbonate treatment, for up to 6 years, is not associatedwith adverse effects on the liver in patients with chronickidney disease stage 5 receiving hemodialysis. Clin Nephrol2009 Mar; 71 (3): 286-95
24. Damment SJ, Cox AG, Secker R. Dietary administration inrodent studies distorts the tissue deposition profile of lan-thanum carbonate; brain deposition is a contaminationartefact? Toxicol Lett 2009 Aug 10; 188 (3): 223-9
25. Bronner F, Slepchenko BM, Pennick M, et al. A model of thekinetics of lanthanum in human bone, using data collectedduring the clinical development of the phosphate binder lan-thanum carbonate. Clin Pharmacokinet 2008; 47 (8): 543-52
26. How PP, Fischer JH, Arruda JA, et al. Effects of lanthanumcarbonate on the absorption and oral bioavailability of ci-profloxacin. Clin J AmSocNephrol 2007Nov; 2 (6): 1235-40
27. Dammet S, Pennick M, Dennis K. A new 1000-mg formula-tion of lanthanum carbonate effectively reduces urinaryphosphorus excretion in healthy volunteers [abstract no.F-PO982]. J Am Soc Nephrol 2005; 16: 550A
28. Finn WF, Joy MS, Hladik G. Efficacy and safety of lan-thanum carbonate for reduction of serum phosphorus inpatients with chronic renal failure receiving hemodialysis.Clin Nephrol 2004 Sep; 62 (3): 193-201
29. Shigematsu T, and the LanthanumCarbonateResearchGroup.Lanthanum carbonate effectively controls serum phosphatewithout affecting serum calcium levels in patients undergoinghemodialysis. Ther Apher Dial 2008 Feb; 12 (1): 55-61
30. Al-Baaj F, Speake M, Hutchison AJ. Control of serumphosphate by oral lanthanum carbonate in patients un-dergoing haemodialysis and continuous ambulatory peri-toneal dialysis in a short-term, placebo-controlled study.Nephrol Dial Transplant 2005 Apr; 20 (4): 775-82
31. Chiang SS, Chen JB, Yang WC. Lanthanum carbonate(Fosrenol�) efficacy and tolerability in the treatment ofhyperphosphatemic patients with end-stage renal disease.Clin Nephrol 2005 Jun; 63 (6): 461-70
32. Joy MS, Finn WF, on behalf of the LAM-302 Study Group.Randomized, double-blind, placebo-controlled, dose-titration,phase III study assessing the efficacy and tolerability of lantha-num carbonate: a new phosphate binder for the treatment ofhyperphosphatemia. Am J Kidney Dis 2003 Jul; 42 (1): 96-107
33. Shigematsu T, and the Lanthanum Carbonate Group. Multi-center prospective randomized, double-blind comparativestudy between lanthanum carbonate and calcium carbonateas phosphate binders in Japanese hemodialysis patients withhyperphosphatemia. Clin Nephrol 2008 Nov; 70 (5): 404-10
34. Sprague SM, Ross EA, Nath SD, et al. Lanthanum carbo-nate vs. sevelamer hydrochloride for the reduction of serumphosphorus in hemodialysis patients: a crossover study.Clin Nephrol 2009 Oct; 72 (4): 252-8
35. Hutchison AJ, Maes B, Vanwalleghem J, et al. Efficacy, toler-ability, and safety of lanthanum carbonate in hyperphos-phatemia: a 6-month, randomized, comparative trial versuscalcium carbonate. Nephron Clin Pract 2005; 100 (1): c8-19
36. Finn WF, Joy MS, on behalf of the LAM-308 Study Group.A long-term, open-label extension study on the safety oftreatment with lanthanum carbonate, a new phosphatebinder, in patients receiving hemodialysis. Curr Med ResOpin 2005 May; 21 (5): 657-64
37. Hutchison AJ, Maes B, Vanwalleghem J, et al. Long-term ef-ficacy and tolerability of lanthanum carbonate: results from a3-year study. Nephron Clin Pract 2006; 102 (2): c61-71
38. US Department of Health and Human Services – Food andDrug Administration. Statistical review and evaluation:clinical studies. Available from URL: http://www.fda.gov/cder/foi/nda/2004/21-468_Fosrenol_StatrClinStudy.pdf[Accessed 2009 Apr 1]
39. Hutchison AJ, SpeakeM, Al-Baaj F. Reducing high phosphatelevels in patients with chronic renal failure undergoing dialysis:a 4-week, dose-finding, open-label study with lanthanumcarbonate. Nephrol Dial Transplant 2004 Jul; 19 (7): 1902-6
40. Eknoyan G, Levin A, Levin NW, et al. Bone metabolismand disease in chronic kidney disease. Am J Kidney Dis2003; 42 (4 Suppl. 3): 1-201
41. Hutchison AJ. Oral phosphate binders. Kidney Int 2009May; 75 (9): 906-14
2348 Curran & Robinson
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)

42. Shire Plc. Shire announces launch of FOSRENOL� inJapan: management of hyperphosphataemia in end-stagerenal disease patients [media release]. Available fromURL:http://www.medicalnewstoday.com/articles/142033.php[Accessed 2009 Mar 12]
43. Hruska KA, Mathew S, Lund R, et al. Hyperphosphatemiaof chronic kidney disease. Kidney Int 2008; 74 (2): 148-57
44. Ritz E. The clinical management of hyperphosphatemia.J Nephrol 2005; 18 (3): 221-8
45. Moe SM, Drueke TB, Block GA, et al. KDIGO clinicalpractice guidelines for the prevention, diagnosis, evalua-tion, and treatment of Chronic Kidney Disease-Mineraland Bone Disorder (CKD-MBD). Kidney Int Suppl 2009Aug; (113): S1-130
46. Kanbay M, Goldsmith D, Akcay Al, et al. Phosphate – thesilent stealthy cardiorenal culprit in all stages of chronickidney disease: a systematic review. Blood Purif 2009; 27:220-30
47. Kestenbaum B, Sampson JN, Rudser KD, et al. Serum phos-phate levels and mortality risk among people with chronickidney disease. J Am Soc Nephrol 2005 Feb; 16 (2): 520-8
48. Voormolen N, Noordzij M, Grootendorst DC, et al. Highplasma phosphate as a risk factor for decline in renalfunction and mortality in pre-dialysis patients. NephrolDial Transplant 2007 Oct; 22 (10): 2909-16
49. Jindal K, Chan CT, Deziel C, et al. Hemodialysis clinicalpractice guidelines for the Canadian Society of Ne-phrology. J Am Soc Nephrol 2006; 17 (3 Suppl. 1): S1-27
50. Levin A, Hemmelgarn B, Culleton B, et al. Guidelines forthe management of chronic kidney disease. CMAJ 2008Nov 18; 179 (11): 1154-62
51. Joint Speciality Committee on Renal Medicine of the RoyalCollege of Physicians and the Renal Association. Chro-nic kidney disease in adults: UK guidelines for identifica-tion, management and referral [online]. Available fromURL: http://www.renal.org/CKDguide/full/UKCKDfull.pdf[Accessed 2009 Apr 22]
52. Elder G, Faull R, Branley P, et al. Management of bonedisease, calcium, phosphate and parathyroid hormone.Nephrology 2006; 11 Suppl.: S230-61
53. Mohammed IA, Hutchison AJ. Phosphate binding therapyin dialysis patients: focus on lanthanum carbonate. TherClin Risk Manag 2008 Oct; 4 (5): 887-93
54. Shinaberger CS, Greenland S, Kopple JD, et al. Is control-ling phosphorus by decreasing dietary protein intake ben-eficial or harmful in persons with chronic kidney disease?Am J Clin Nutr 2008 Dec; 88 (6): 1511-8
55. Pauly RP. Nocturnal home hemodialysis and short dailyhemodialysis compared with kidney transplantation:emerging data in a new era. Adv Chronic Kidney Dis 2009May; 16 (3): 169-72
56. Mucsi I, Hercz G, Uldall R, et al. Control of serum phosphatewithout any phosphate binders in patients treated with noc-turnal hemodialysis. Kidney Int 1998; 53 (5): 1399-401
57. Buoncristiani U. Fifteen years of clinical experience withdaily haemodialysis. Nephrol Dial Transplant 1998; 13Suppl. 6: 148-51
58. Mohammed I, Hutchison AJ. Oral phosphate binders forthe management of serum phosphate levels in dialysis pa-tients. J Ren Care 2009 Mar; 35 Suppl. 1: 65-70
59. Wills MR, Savory J. Aluminium poisoning: dialysis enceph-alopathy, osteomalacia and anaemia. Lancet 1983 Jul 2;II (8340): 29-34
60. Gonzalez-Revalderia J, Casares M, de Paula M, et al. Bio-chemical and haematological changes in low-level aluminiumintoxication. Clin Chem Lab Med 2000 Mar; 38 (3): 221-5
61. Schaefer K, Umlauf E, von Herrath D. Reduced risk of hy-percalcemia for hemodialysis patients by administeringcalcitriol at night. Am JKidneyDis 1992May; 19 (5): 460-4
62. Goodman WG. Vascular calcification in chronic renal fail-ure. Lancet 2001 Oct; 358 (9288): 1115-6
63. Locatelli F, Cannata-Andia JB, Drueke TB, et al. Manage-ment of disturbances of calcium and phosphate metabo-lism in chronic renal insufficiency, with emphasis on thecontrol of hyperphosphataemia. Nephrol Dial Transplant2002 May; 17 (5): 723-31
64. O’Donovan R, Baldwin D, Hammer M, et al. Substitutionof aluminium salts by magnesium salts in control of dialysishyperphosphataemia. Lancet 1986 Apr; I (8486): 880-2
65. Spiegel DM. The role of magnesium binders in chronickidney disease. Semin Dial 2007; 20 (4): 333-6
66. Goldsmith DR, Scott LJ, Cvetkovic RS, et al. Sevelamerhydrochloride: a review of its use for hyperphosphataemiain patients with end-stage renal disease on haemodialysis.Drugs 2008; 68 (1): 85-104
67. Delmez J, Block G, Robertson J, et al. A randomized, double-blind, crossover design study of sevelamer hydrochlorideand sevelamer carbonate in patients on hemodialysis. ClinNephrol 2007 Dec; 68 (6): 386-91
68. Chertow G, Dillon M, Burke S, et al. A randomized trialof sevelamer hydrochloride (Renagel) with and withoutsupplemental calcium: strategies for the control of hyper-phosphataemia and hyperparathyroidism in hemodialysispatients. Clin Nephrol 1999 Jan; 51 (1): 18-26
69. Karamanidou C, Clatworthy J, Weinman J, et al. A sys-tematic review of the prevalence and determinants of non-adherence to phosphate binding medication in patientswith end-stage renal disease. BMCNephrol 2008 Jan 31; 9 (2)
70. Tomasello S, Dhupar S, Sherman R. Phosphate binders,K/DOQI guidelines, and compliance: the unfortunate rea-lity. Dialysis Transplant 2004; 33: 236-42
71. US Renal Data System. Medication use among dialysis pa-tients in the Dialysis and Morbidity and Mortality Study.Am J Kidney Dis 1998; 32 (2 Suppl. 1): S60-8
72. Hutchison AJ, Laville M, SPD405-313 Lanthanum StudyGroup. Switching to lanthanum carbonate monotherapyprovides effective phosphate control with a low tabletburden. Nephrol Dial Transplant 2008 Nov; 23 (11):3677-84
73. Mehrotra R, Martin KJ, Fishbane S, et al. Higher strengthlanthanum carbonate provides serum phosphorus controlwith a low tablet burden and is preferred by patients andphysicians: a multicenter study. Clin J Am Soc Nephrol2008 Sep; 3 (5): 1437-45
Correspondence: Monique P. Curran, Adis, a WoltersKluwer Business, 41 Centorian Drive, Private Bag 65901,Mairangi Bay, North Shore 0754, Auckland, New Zealand.E-mail: [email protected]
Lanthanum Carbonate: A Review 2349
ª 2009 Adis Data Information BV. All rights reserved. Drugs 2009; 69 (16)





























