Embed Size (px)
Citation preview

D R C O L M H E N RYN AT I O N A L C L I N I C A L A DV I S O R A N D G R O U P L E A D
A C U T E H O S P I TA L S H S E
Clinical Directors and Integrated Care




Clinical Directors in Ireland – 2008-2014• Hospital-based and Mental Health
• 55 hospital-based• 18 Mental health directorates• Roles evolved based on local requirements and
politics
• Aligned to institutions primarily, with Group Lead CDs appointed 2015
• Limited regional governance approach until advent of Hospital Groups
• No link to Community Healthcare Organisations
• No link to Primary Care
Escher, Waterfall, 1961

Challenges: old and new
1. Health inequality
2. Changing role of hospitals in Ireland
3. Changing role of hospitals internationally
4. Demographics: the push to integrated care

Challenges: old and new
1. Health inequality
2. Changing role of hospitals in Ireland
3. Changing role of hospitals internationally
4. Demographics: the push to integrated care
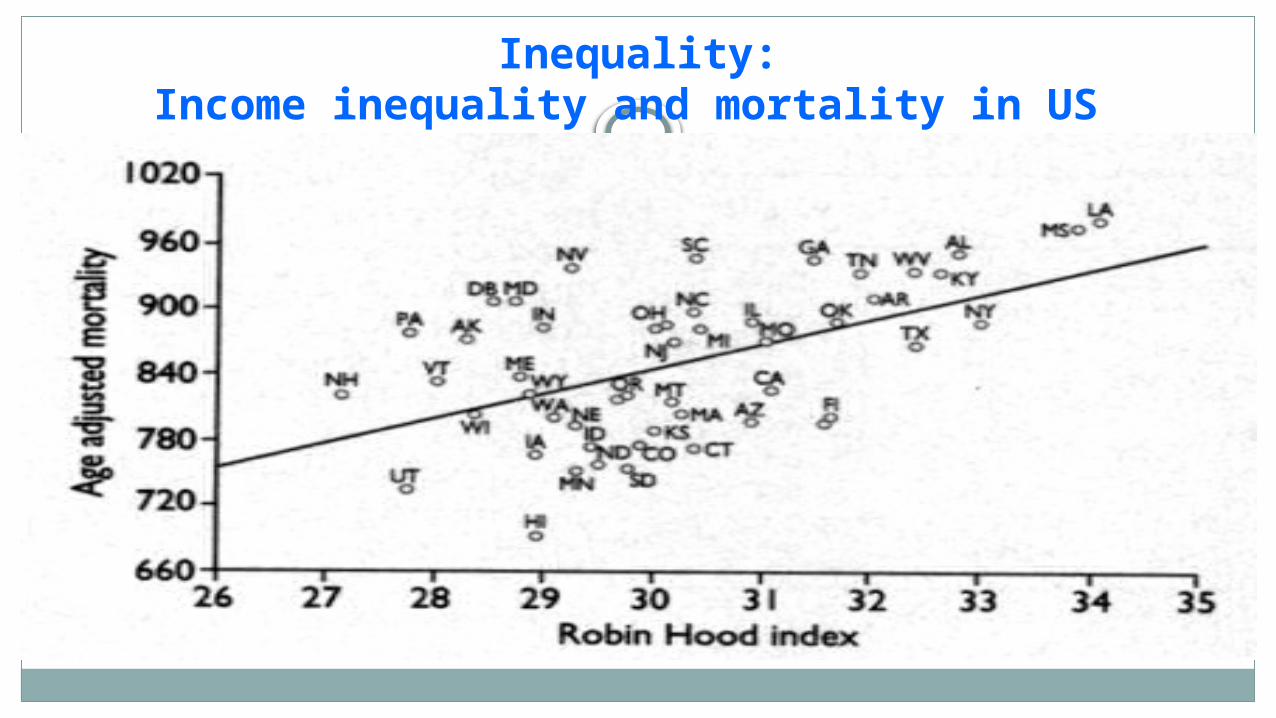
Inequality:Income inequality and mortality in US


Annual directly standardised death rate for working age males by Socio-Economic Group during 1989-1998 in
the Republic of Ireland for all causes of death
241.5325.4 347.2
761.3
545.7
312.5
0100200300400500600700800
Seg A Seg B Seg C Seg D Unknown Farmers
Socio - Economic Group
RA
TE
PE
R 1
00
,00
0
Key to Socio-economic Group CodingSeg A: Higher professionals, lower professionals Seg B: Employers and managers, salaried employees Seg C: Non-manual wage earners, other non-manual wage earners, skilled manual workersSeg D: Semi-skilled manual workers, unskilled manual workers, farm labourersFarmers: Farmers, farmer's relatives and farm managersUnknown: Unknown

Challenges: old and new
1. Health inequality
2. Changing role of hospitals in Ireland
3. Changing role of hospitals internationally
4. Demographics: the push to integrated care

Reconfiguration, Year 0: 1933
“Too many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine. The central specialised hospitals must be made available for all, and the poor must get the use of them free. The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully planned……the government cannot stand idly by and see millions of money poured into a system obviously unorganised and insufficient. To do this would be to stereotype all the existing deficits for generations to come…’
Dr FC Ward, Parliamentary Secretary
[Junior Minister for Health] to the Minister for Local Government and Public Health; Second (Committee) Stage, Public Hospitals Bill, Dáil Debate 28thApril 1933
Sir John Lavery, London Hospital, c 1918

1. Hospitals Commission 1936
2. Fitzgerald Report 1968
3. Hanley Report 2003
4. Higgins Report, Smaller Hospital Framework 2013
Reconfiguration: the long road
Escher, Waterfall, 1961
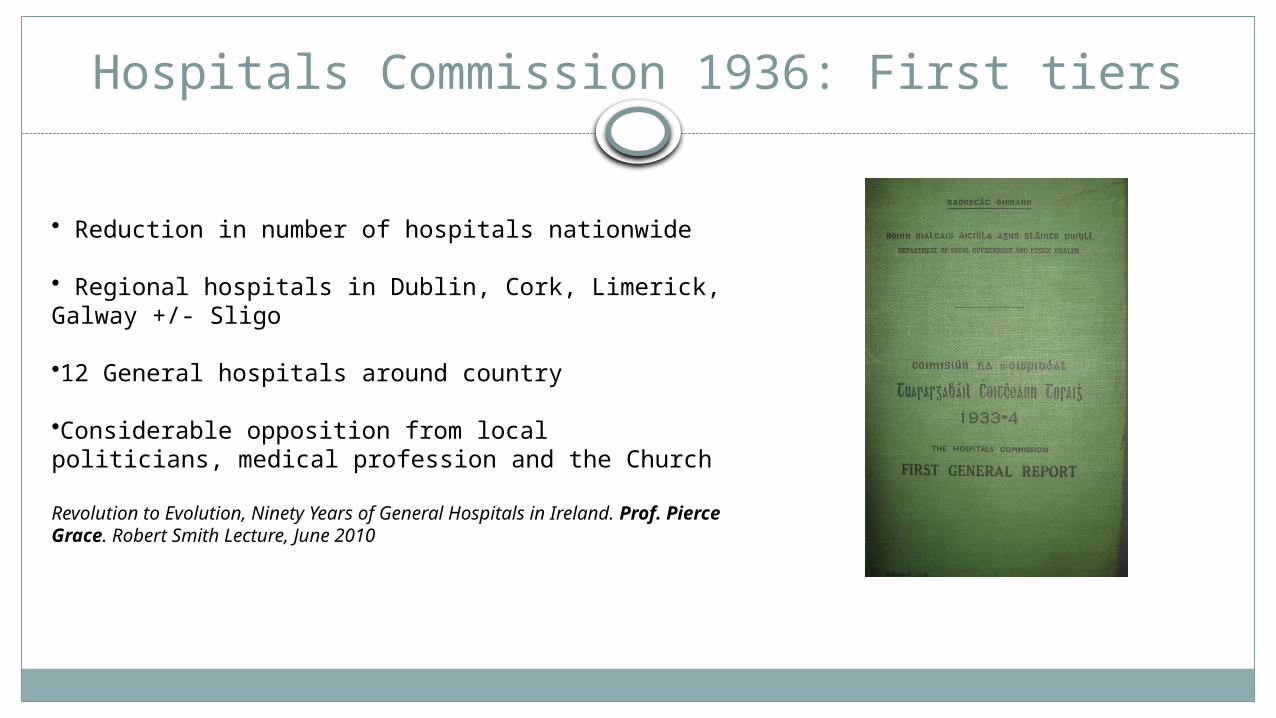
• Reduction in number of hospitals nationwide
• Regional hospitals in Dublin, Cork, Limerick, Galway +/- Sligo
•12 General hospitals around country
•Considerable opposition from local politicians, medical profession and the Church
Revolution to Evolution, Ninety Years of General Hospitals in Ireland. Prof. Pierce Grace. Robert Smith Lecture, June 2010
Hospitals Commission 1936: First tiers

National Taskforce on Medical Staffing, 2003
Reforming the organisation of hospital services
“There is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience, high volumes of activity and access to appropriate diagnostic and treatment facilities”
Hospital in Arles, Van Gogh, 1889
Dr Gachet, Vincent Van Gogh, 1890

Hospital Groups 2013
7 hospital groups
Separate governance and management structures
Linked to academic centres
Limitations - link with CHOs? - Links with primary care? - funding = hospital-based activity
Challenges: old and new
1. Health inequality
2. Changing role of hospitals in Ireland
3. Changing role of hospitals internationally
4. Demographics: the push to integrated care

3. How hospitals are changing internationally
The analogous situation in health care is that whereas doctors and hospitals focus on producing health care, what people really want is health. Health care is just a means to that end — and an increasingly expensive one. If we could get better health some other way, just as we can now produce images without film and transport people and freight without railroads, then maybe we wouldn't have to rely so much on health care…….
In the future, successful doctors, hospitals, and health systems will shift their activities from delivering health services within their walls toward a broader range of approaches that deliver health. Although we're seeing the earliest steps in this shift toward accountability for health, we currently lack both good tools for moving forward in any substantial way and more established pathways for redirecting financing toward those outcomes.5 What do we need to move from a product-oriented industry to a customer-oriented one?
What Business Are We In? The Emergence of Health as the Business of Health CareDavid A. Asch, M.D., M.B.A., and Kevin G. Volpp, M.D., Ph.D.N Engl J Med 2012; 367:888-889September 6, 2012DOI: 10.1056/NEJMp1206862

Kings Fund Integrated Care 2015
‘………moving from an organisational focus to a system-wide perspective’
‘………..working more closely with local partners, including primary care, social care and community services’
‘……….developing integrated service models that span organisational boundaries’
‘….. developing job roles that span acute and community settings’
‘…using tangible service changes and early wins to demonstrate to staff the benefits of integrated models of care for patients.acute hospitals
Changing funding models

Integrated care: how hospitals might look
- Option 1 – Hospitals as islands
- Fortress mentality in face of mounting financial and demographic pressures
- Option 2 – Hospitals as part of integrated care system
- - Working with partners to provide co-ordinated care to patients with greatest need through vertical and horizontal integration
- Option 3 – Hospitals in population health systems
- Going beyond integrated care for patients and addressing health needs of population
• Integrated health caredelivery system
• 9.1 million members• 16,000+ physicians• 48,000+ nurses • 174,000+ employees • Serving 8 states and the
District of Columbia • 37 hospitals
Scope includes ambulatory, inpatient, ACS, behavioral health, SNF, home health, hospice, pharmacy, imaging, laboratory, optical, dental, and insurance
Kaiser PermanenteLargest nonprofit health plan in the U.S
“the incentives are toward less medical care, because the less care
they give them, the more money they make.“ Ehrlichman
29/04/2015Acute v Elective 21

29/04/2015Acute v Elective
22
Hospital bed usage if extrapolated to a population equivalent to Ireland’s would be 4500
Ireland’s hospital bed usage = 12,000 Success attributed to:
o strong emphasis on preventive care, reducing costs later ono doctors are salaried rather than paid per service, which removes the main
incentive for doctors to perform unnecessary procedures.o minimizing time patients spend in high-cost hospitals by planning their stay and
by shifting care to outpatient clinics
Kaiser PermanenteLargest nonprofit health plan in the U.S
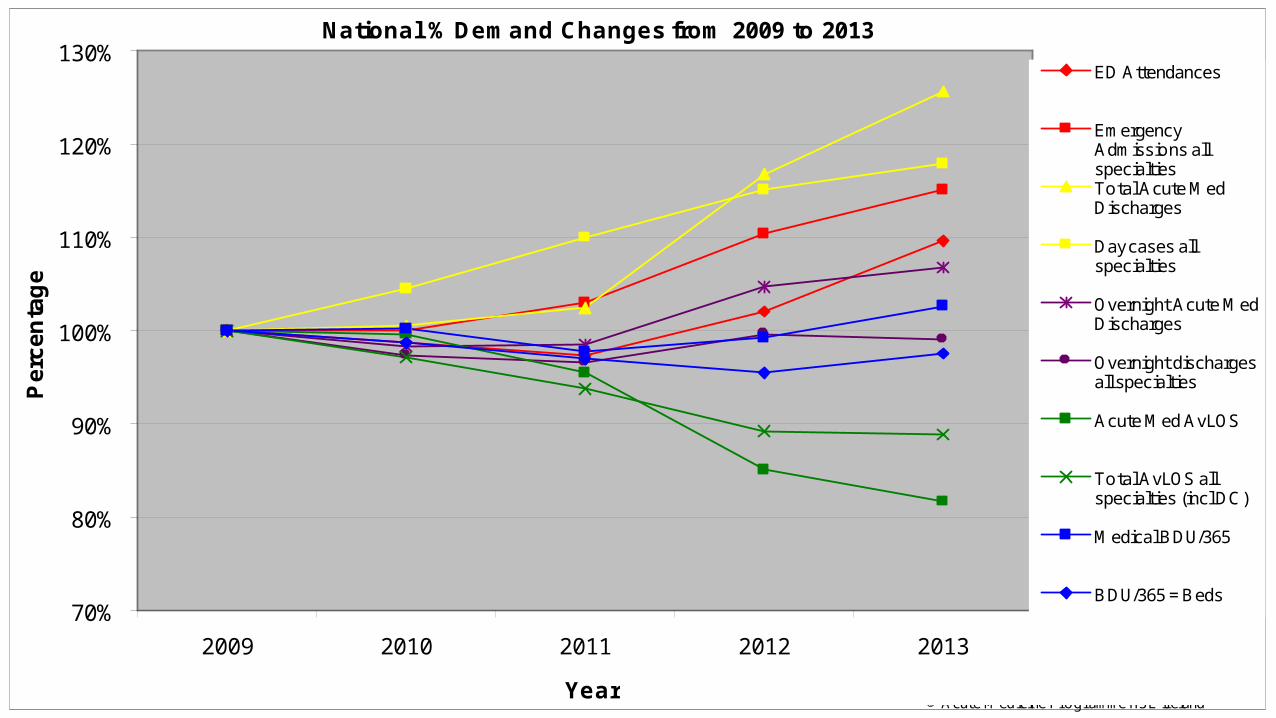
National % Demand Changes from 2009 to 2013
70%
80%
90%
100%
110%
120%
130%
2009 2010 2011 2012 2013
Year
Pe
rce
nta
ge
ED Attendances
EmergencyAdmissions allspecialtiesTotal Acute MedDischarges
Day cases allspecialties
Overnight Acute MedDischarges
Overnight dischargesall specialties
Acute Med AvLOS
Total AvLOS allspecialties (incl DC)
Medical BDU/365
BDU/365 = Beds
Data Source: HIPE, Healthcare Pricing Office; BIUData Analysis: HSE/ 26 M ay 2014© Acute M edicine Programme HSE Ireland

Challenges: old and new
1. Health inequality
2. Changing role of hospitals in Ireland
3. Changing role of hospitals internationally
4. Demographics: the push to integrated care

0
5
10
15
20
25
2011 2013 2015 2017
All ages
65+
1. Demographics: increase in health service cost pressures due to demographic
effects
Source: CSO census of population and provisional DOH data projections to 2017, Based on cost relativities from the 2012 Ageing Report: European Commission 2012

Cumulative effective reduction in resources, budget reductions and demographic deficit combined, 2009-2014
-25
-20
-15
-10
-5
0
2010 2011 2012 2013 2014
Demographicpressure
Budgetrestriction


Demographics: examining the limits of what we can give
The Hospital-Dependent Patient‘Medicine has yet to acknowledge the ethical and practical predicament of having created a population of incurable, fragile, but not yet terminally ill patients without concurrently developing a healthcare system that can meet their needs’Reuben and Tinetti, NEJM February 20th 2014
Being Mortal: Medicine and what matters in the end‘ The waning days of our lives are given over to treatments that addle our brains and sap our bodies for a sliver’s chance of benefit. They are spent in institutions – nursing homes and intensive care units – where regimented, anonymous routines cut us off from all the things that matter to us in life. Our reluctance to honestly examine the experience of ageing and dying has increased the harm we inflict on people and denied them the basic comforts they most need’.Atul Gawande, Metropolitan Press 2014

The Kings Fund Specialists in out of hospital settings 2014
The health care workforce is not currently designed to staff an integrated system in which patients move seamlessly between organisations and more patients have their care managed outside hospital. Specialist knowledge is concentrated in the hospital, and moving care outside it will require a redistribution of roles and responsibilities across the health care workforce (Bohmer and Imison 2013).