Embed Size (px)
Citation preview

Sinus Floor Elevation ProceduresRegistrar: Dr Rakesh Chandran
Supervisor: Dr Yusuf Jadwat

• ANATOMY OF THE MAXILLARY SINUS• MEDICATION• SINUS FLOOR ELEVATION PROCEDURES• POST SURGICAL INSTRUCTIONS• COMPLICATIONS• REVIEW OF THE LITERATURE
PRESENTATION OUTLINE

ANATOMY OF THE MAXILLARY SINUS
• Pyramidal in shape• Apex pointed towards the zygomatic bone• Volume in an adult ≈15ml (range 9ml to 20ml)
BASE- lateral wall of nose• (≈33mm X 33mm)• Base to apex ≈ 23mm• Sinus ostium is placed high and is in an
unfavourable position for gravity dependent drainage

ANATOMY OF THE MAXILLARY SINUS
SUPERIOR WALL- floor of the orbit• Infraorbital nerves and vessels
POSTERIOR WALL • internal maxillary artery, • pterygoid plexus, • sphenopalatine ganglion• greater palatine nerve
FLOOR- alveolar process of the maxilla
LATERAL WALL-facial surface of the maxilla• infraorbital foramen• thickness ranges from 0.5 to 2.5mm

• Also known as Underwood’s septa• Almost 30% of dentate maxilla have septa• 75% appearing in the premolar region. • Complete septa are very rare (1%)• Primary septa are developmental• Secondary septa are caused by irregular
pneumatisation following loss of posterior teeth
SEPTA

• Mucosal lining of the sinus• Pseudo-stratified columnar ciliated
respiratory epithelium covering a thin layer of connective tissue
• 0.45 to 1.40mm in thickness• Considered normal if less than 4mm
Increased thickness associated with• thick gingival biotype• chronic sinus inflammation• smoking
SCHNEIDERIAN MEMBRANE

VASCULAR SUPPLY
Anastomosis• Infraorbital• posterior superior alveolar artery.• posterior lateral nasal (medial aspect of the sinus).
The formation of the intraosseous and extraosseous anastomoses is termed the double arterial arcade.

Coronal sections
The intraosseous branch of the posterior superior alveolar artery most frequently runs through a bony groove inside the lateral wall of the maxillary sinus.
Rarely the artery may run within a bony canal.
Hur MS et al., 2009. Clinical implications of the topography and distribution of the posterior superior alveolar artery. J Craniofac Surg.

The courses of the intra osseous branch of the posterior superior alveolar artery
Straight (78.1%)
U-shaped (21.9%)
Hur MS et al., 2009. Clinical implications of the topography and distribution of the posterior superior alveolar artery. J Craniofac Surg.

Mean and range values of the height of the IObr of the PSAA from the CEJ in mm.
The minimum mean height from the cervix to the IObr• 21.1mm in the first molar region• 26.9mm in the first premolar region
More precautions should be taken at the first molar region than the first premolar region.
Hur MS et al., 2009. Clinical implications of the topography and distribution of the posterior superior alveolar artery. J Craniofac Surg.

VENOUS DRAINAGEAnterior facial veinPterygoid venous plexus
LYMPHATIC DRAINAGESubmandibular lymph node
NERVE SUPPLYMaxillary division of trigeminal nerve (V2)

ABSOLUTE LOCAL CONTRAINDICATIONS
• local aggressive benign tumours • malignant tumours • large maxillary cysts• acute sinusitis• allergic rhinitis

RATIONALE FOR ANTIBIOTIC PROPHYLAXIS
• Endoscopically normal sinuses were shown to be non sterile• Most common bacteria
• Streptococcus viridans• Staphylococcus epidermidis• Streptococcus pneumonia
• Sinus graft procedure often violate the sinus mucosa and bacteria may contaminate the graft site
RATIONALE FOR ANTIBIOTIC IN THE GRAFT• the bone graft is a dead space prone to infection• systemic antibiotic drugs do not enter the area until revascularization

Systemic antibiotic prophylaxis
No allergy to penicillinAugmentin 825mg/125mg.
One tablet twice daily starting 1 day before/ 5 days after
Non anaphylactic allergy to penicillinCefuroxime axetil 500mg. (Cephalosporin)
One tablet twice daily starting 1 day before/ 5 days after
Anaphylactic reaction to penicillinLevofloxacin 500mg. (Fluoroquinolone)
One tablet starting 1 day before/ 5 days after
Misch CE. Contemporary Implant Dentistry 3rd Ed. 2008

Antibiotic in graft
Cefazolin (1gm) dilute with 2ml saline (cephalosporin)100mg add to collagen membrane400mg add to graft material
Clindamycin 150mg/1ml30mg add to collagen membrane120mg add to graft material
Capsules and tablets should not be used as they contain fillers that are not conducive to osteogenesis.
Misch CE. Contemporary Implant Dentistry 3rd Ed. 2008

Glucocorticoid medicationDexamethazone (4mg)Two tablets in the morning the day before and day of surgeryOne tablets in the morning for 2 days after surgery
Decongestant medicationOxymetazoline 0.05% (Vicks)
Analgesic medicationAnalgesic containing codeine as codeine is a potent antitussive.
CryotherapyIce or cold dressings for the 24 to 48 hoursThen heat applied to increase blood and lymph flow
Misch CE. Contemporary Implant Dentistry 3rd Ed. 2008

SINUS FLOOR ELEVATION TECHNIQUES
LATERAL WINDOW
TRANSCRESTAL APPROACH

HISTORY
1980: Boyne and James reported on elevation of the maxillary sinus floor in patients with large, pneumatized sinus cavities as a preparation for the placement of blade implants. Boyne, P. J. & James, R. A. (1980) Grafting of the maxillary sinus floor with autogenousmarrow and bone. Journal of Oral Surgery 38, 613–616.
1994: Summers described a crestal approach, using tapered osteotomes with increasing diameters.Summers, R. B. (1994) A new concept in maxillary implant surgery: the osteotometechnique. Compendium 15, 152–154–156, 158 passim; quiz 162.

ATROPHIC POSTERIOR MAXILLA
Favourable interarch relationship
Insufficient bone height for standard implant
Vertical bone height ≤6mm or oblique sinus
floor
Lateral window technique
Vertical bone height >6mm and horizontal
sinus floor
Transcrestal
TREATMENT GUIDELINES- INTERNATIONAL TEAM FOR IMPLANTOLOGY (ITI)

LATERAL WINDOW TECHNIQUESModified Caldwell-Luc approach (Tatum)Ultrasonic ostectomy (Torella)Piezoelectric bony window osteotomy (Vercellotti et al)Trephine (Emtiaz)Antral membrane balloon elevation ( Soltan and Smiler)
Other variationsHinge osteotomyElevated osteotomyCrestal osteotomy
TRANSCRESTAL APPROACH TECHNIQUESOsteotome technique (Summers)Modified osteotome technique (Davarpanah et al 1996)Hydraulic pressure- saline (Sotirakis and Gonshor)
SINUS FLOOR ELEVATION TECHNIQUES

LATERAL WINDOW APPROACH
Katsuyama H., Jensen SS. ITI Treatment Guide. Volume 5. 2011
Handling the cortical bone
1. fracture the cortical bony plate like a trap-door and use it as the new sinus floor, leaving it attached to the underlying mucosa.
2. removal of the cortical bone and use it as the new sinus floor- elevated osteotomy
3. removal of the bone by thinning it out.
4. remove the cortical bony plate and replace it on the lateral aspect of the graft at the end of the grafting procedure.

LATERAL WINDOW APPROACH
Pjetursson BE., Lang NP. Clinical Periodontology and implant Dentistry. 2008
Removal of cortical bone
1. Round bur2. Ultrasonic instruments3. Piezoelectric4. Trephine

LATERAL WINDOW APPROACH- ANTRAL MEMBRANE BALLOON ELEVATION
Soltan M., Smiler DG. Antral membrane balloon elevation. Journal of oral Implantology. 2005

TRANSCRESTAL APPROACH- SUMMERS TECHNIQUE
Pjetursson BE., Lang NP. Clinical Periodontology and implant Dentistry. 2008
X
Larger diameter osteotomes

TRANSCRESTAL APPROACH- MODIFIED SUMMERS TECHNIQUE
Davarpanah M et al., 2011. The Modified Osteotome Technique. Int J Periodont Rest Dent

TRANSCRESTAL APPROACH- HYDRAULIC PRESSURE- SALINE

Do not blow your noseDo not use tobacco Do not drink with a strawDo not lift or pull up the lip to look at the sutures Sneeze with the mouth open
Notify the office if • you feel granules in your nose
POSTOPERATIVE INSTRUCTIONS

INTRA-OPERATIVE COMPLICATIONS1. Sinus membrane perforation (10 to 20%)2. Excessive bleeding (bony window/ sinus membrane/wound dehiscences)3. Injury of the infraorbital neurovascular bundle4. Implant migration5. Hematoma6. Adjacent tooth sensitivity
POST-OPERATIVE COMPLICATIONS1. Infection of the grafted sinus (3-7 days post-op) (3%). 2. Sinusitis
COMPLICATIONS

Confounding factorsStudy designPatient factors (age, gender, health, SES, hygiene…..Operator factors (experience, techniques…..Regenerative material propertiesFollow up periodImplant properties
LITERATURE REVIEW
Up to 1996?? Currently used

4th ITI Consensus conference onSinus Floor Elevation Procedures, 2008
ITI Treatment Guide (Volume 5)Review published 2011 with updated literatureJensen SS.
LITERATURE REVIEW

LITERATURE REVIEW
Jensen SS. 4th ITI Consensus conference: Sinus Floor Elevation Procedures, 2008 in ITI Treatment Guide 2011
Technique Study characteristics Implant survival
Lateral window technique
85 studies, 4807 patients, 14944 implants,after 12 to 107 months loading
Machined implant surfaces: 61.2% to 100%Rough surface implants: 88.6% to 100%
Transcrestal technique
18 studies, 1096 patients, 1744 implants,after 12 to 64 months loading
83% to 100%

LITERATURE REVIEW
Jensen SS. 4th ITI Consensus conference: Sinus Floor Elevation Procedures, 2008 in ITI Treatment Guide 2011
Lateral window technique
Study characteristics Implant survival
Bone substitute only
19 studies,740 patients, 2481 implants,after 12 to 107 months loading
82% to 100%
Excluding smooth surface88.6% to 100%
Autograft only or combined with bone substitute
36 studies,1210 patients, 4218 implants,after 12 to 107 months of loading
61.2% to 100%
Excluding smooth surface96% to 100%
LITERATURE REVIEW
Jensen SS. 4th ITI Consensus conference: Sinus Floor Elevation Procedures, 2008 in ITI Treatment Guide 2011
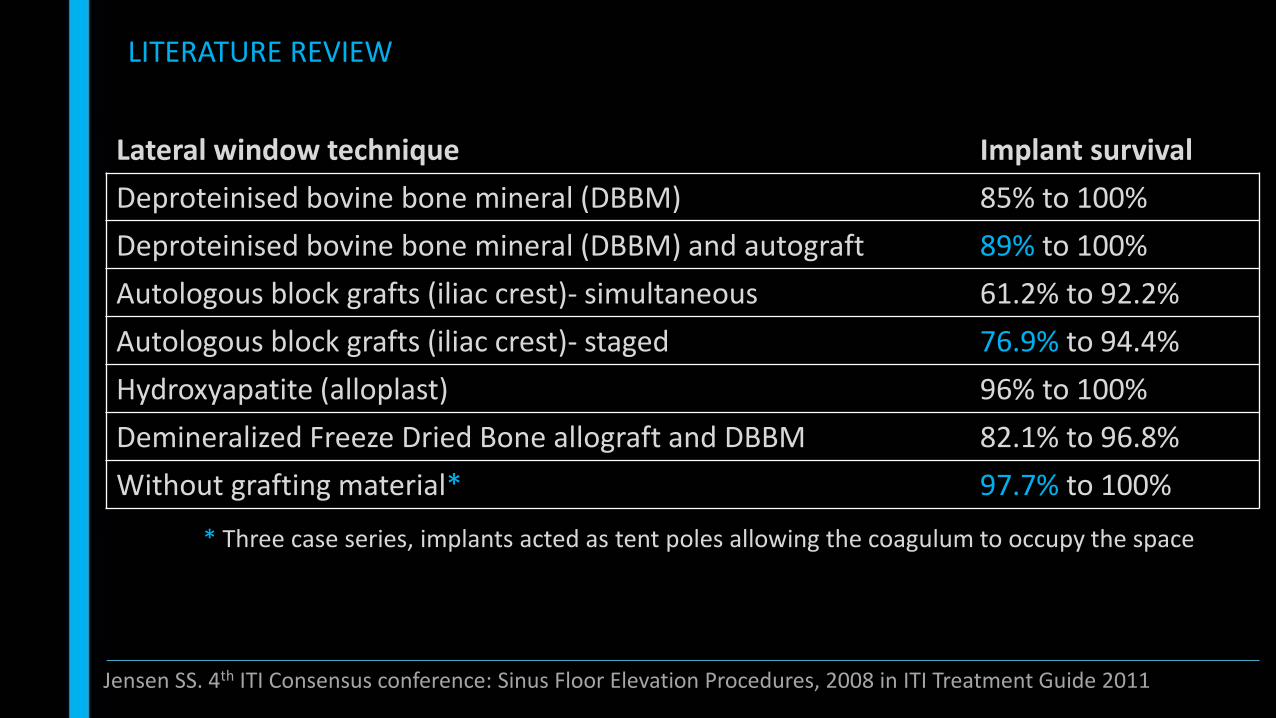
Lateral window technique Implant survival
Deproteinised bovine bone mineral (DBBM) 85% to 100%
Deproteinised bovine bone mineral (DBBM) and autograft 89% to 100%
Autologous block grafts (iliac crest)- simultaneous 61.2% to 92.2%
Autologous block grafts (iliac crest)- staged 76.9% to 94.4%
Hydroxyapatite (alloplast) 96% to 100%
Demineralized Freeze Dried Bone allograft and DBBM 82.1% to 96.8%
Without grafting material* 97.7% to 100%
* Three case series, implants acted as tent poles allowing the coagulum to occupy the space

LITERATURE REVIEW
Jensen SS. 4th ITI Consensus conference: Sinus Floor Elevation Procedures, 2008 in ITI Treatment Guide 2011
Lateral window technique Implant survival Implant survivalExcluding smooth surface
Membrane over the lateral window 92% to 100% 92% to 100%
Without the use of a membrane 61.2% to 100% 93% to 100%

LITERATURE - TRANSCRESTAL TECHNIQUE
Jensen SS. 4th ITI Consensus conference: Sinus Floor Elevation Procedures, 2008 in ITI Treatment Guide 2011
Transcrestal technique Study characteristics Implant survival
Without grafting material 8 studies, 249 patients, 443 implantsafter 12 to 36 months of loading
91.4% to 100%
Deproteinised bovine bone mineral (DBBM)
4 studies, 122 patients, 195 implantsafter 12 to 45 months of loading
95% to 100%
Autologous bone 2 studies?, 489 patients, 771 implantsafter 20 to 54 months of loading
93.8% to 97.8%

• Maxillary sinus elevation is a predictable technique.• Autogenous bone grafts were considered the gold standard – now allografts with
particulate autografts are associated with better implant survival rates (Esposito et al., 2006).
• Rough surface implants have more favourable clinical outcomes.• Simultaneous and delayed give equivalent results.
CONCLUSION
Jensen SS., Katsuyama H., 2011. ITI Treatment guide. Volume 5. Sinus floor elevation procedures.Testori T et al., 2009. maxillary sinus surgery and alternatives in treatment.

Thank you