Embed Size (px)
Citation preview

Maxillary sinus floor elevation usingthe (transalveolar) osteotome techniquewith or without grafting material.Part I: implant survival and patients’perception
Bjarni E. PjeturssonClaude RastUrs BraggerKurt SchmidlinMarcel ZwahlenNiklaus P. Lang
Authors’ affiliations:Bjarni E. Pjetursson, Faculty of Odontology,University of Iceland, Reykjavik, IcelandBjarni E. Pjetursson, Claude Rast, Urs Bragger,Niklaus P. Lang, University of Bern, School ofDental Medicine, Bern, SwitzerlandKurt Schmidlin, Marcel Zwahlen, ResearchSupport Unit, Institute of Social and PreventiveMedicine, University of Bern, Bern, SwitzerlandNiklaus P. Lang, Prince Philip Dental Hospital,University of Hong Kong, Hong Kong, SAR-PRC
Correspondence to:Bjarni E Pjetursson, DDS, Dr med. dent., MASDepartment of ProsthodonticsUniversity of IcelandVatnsmyrarvegur 16IS- 101 Reykjavik, IcelandTel.: þ 354 525 4850Fax: þ 354 525 4874e-mail: [email protected]
Key words: biological complications, bone augmentation, bone grafting, complications,
crestal approach, dental implants, failures, longitudinal, osteotome technique, patients’
perception, patients’ satisfaction, peri-implantitis, sinus augmentation, sinus floor eleva-
tion, sinus grafting, success, survival, transalveolar approach
Abstract
Objectives: To analyze the survival and success rates of implants installed utilizing the
(transalveolar) osteotome technique, to compare peri-implant soft tissue parameters and
marginal bone levels of osteotome-installed implants with implants placed using standard
surgical procedures, and to evaluate patient-centered outcomes.
Material and methods: During 2000 to 2005, 252 Straumanns
dental implants were
inserted in 181 patients. The surgical technique was a modification of the original
osteotome technique presented by Summers. In addition to the clinical examination, the
patients were asked to give their perception of the surgical procedure, utilizing a visual
analogue scale.
Results: The cumulative survival rate of the osteotome-installed implants after a mean
follow-up time of 3.2 years, was 97.4% (95% confidence intervals: 94.4–98.8%). From the
252 implants inserted, three were lost before loading and another three were lost in the
first and second year. According to residual bone height the survival was 91.3% for implant
sites with � 4 mm residual bone height, and 90% for sites with 4 mm and 5 mm, when
compared with that of 100% in sites with bone height of above 5 mm. According to implant
length the survival rates were 100% for 12 mm, 98.7% for 10 mm, 98.7% for 8 mm and only
47.6% for 6 mm implants. Soft tissue parameters (pocket probing depth, probing attach-
ment level, bleeding on probing and marginal bone levels) did not yield any differences
between the osteotome-installed and the conventionally placed implants. More than 90%
of the patients were satisfied with the implant therapy and would undergo similar therapy
again if necessary. The cost associated with implant therapy was considered to be justified.
Conclusion: In conclusion, the osteotome technique was a reliable method for implant
insertion in the posterior maxilla, especially at sites with 5 mm or more of preoperative
residual bone height and a relatively flat sinus floor.
Elevation of the maxillary sinus floor
was first reported by Boyne in the 1960s.
Fifteen years later, Boyne & James (1980)
reported on elevation of the maxillary sinus
floor in patients with large, pneumatized
sinus cavities as a preparation for the place-
ment of blade implants. A two-stage
procedure, was described where the max-
illary sinus was grafted using autogenous
particulate iliac bone at the first stage of
surgery. At the second stage of surgery,
after approximately 3 months, the blade
Date:Accepted 15 December 2008
To cite this article:Pjetursson BE, Rast C, Bragger U, Schmidlin K,Zwahlen M, Lang NP. Maxillary sinus floor elevationusing the (transalveolar) osteotome technique with orwithout grafting material. Part I: implant survival andpatients’ perception.Clin. Oral Impl. Res. 20, 2009; 667–676.doi: 10.1111/j.1600-0501.2009.01704.x
c� 2009 John Wiley & Sons A/S 667

implants were placed and later used to
support fixed or removable reconstructions
(Boyne & James 1980).
With time it became eminent that the
posterior maxillary region was often lim-
ited for standard implant placement, be-
cause the residual vertical bone height was
reduced. An elevation of the maxillary
sinus floor was thus one option in solving
this problem. Several surgical techniques
have been presented to enter the sinus
cavity, elevating the sinus membrane and
placing bone grafts. A transalveolar ap-
proach for sinus floor elevation with sub-
sequent placement of implants was first
suggested by Tatum (1986). Utilizing this
approach, a ‘socket former’ for the selected
implant sizes was used to prepare the im-
plant site. A ‘green-stick fracture’ of the
sinus floor was accomplished by hand tap-
ping the ‘socket former’ in a vertical direc-
tion. After preparation of the implant site,
a root-formed implant was placed and al-
lowed to heal in a submerged way.
Summers (1994) later described another
transalveolar approach, the osteotome
technique for sinus floor elevation, using
a set of osteotomes of varying diameters to
prepare the implant site. The concept in-
tended to increase the density of the soft,
Types III and IV (Lekholm & Zarb 1985)
maxillary bone resulting in better primary
stability of inserted dental implants. Bone
was conserved by the osteotome technique
because drilling was not performed.
The bone-added osteotome sinus floor
elevation (BAOSFE), also referred to as the
‘Summers technique,’ may be considered
more conservative and less invasive than
the conventional lateral approach of sinus
floor elevation. A small osteotomy is
made through the alveolar crest of the
edentulous ridge, at the inferior border of
the maxillary sinus. This intrusion osteot-
omy procedure elevates the sinus mem-
brane, thus resulting in a ‘tent’ effect.
This creates space for bone graft placement.
It should be noted that the bone grafts are
placed blindly into the space below the
sinus membrane. Hence, the main dis-
advantage of this technique is the un-
certainty of a possible perforation of the
Scheiderian sinus membrane. However, an
endoscopic study has revealed that the
sinus floor may be elevated up to 5 mm
without perforating the membrane (Engelke
& Deckwer 1997).
In a multicenter retrospective study
(Rosen et al. 1999) that evaluated the
application of the Summers technique in
the placement of 174 implants in 101
patients, the survival rate was 96%, when
residual bone height was 5 mm or more,
but dropped to 85.7%, when residual bone
height was 4 mm or less. From these data it
would appear that the residual bone height
had a significant influence on the outcome
of these procedures.
In a recent study, survival and success
rates of 588 implants placed in 323 con-
secutive patients with a residual bone
height ranging from 6 to 9 mm were eval-
uated. After a mean observation period of
5 years, the survival and success rates
were, 94.8% and 90.8%, respectively (Fer-
rigno et al. 2006). During the study period,
only 13 perforations of the Schneiderian
membrane were detected, resulting in a
perforation rate of only 2.2%. It was con-
cluded, that the installation of short im-
plants in conjunction with osteotome sinus
floor elevation was predictable and may
reduce the indications for more invasive
and complex procedures, such as the sinus
floor elevation by the lateral approach
(Ferrigno et al. 2006).
Moreover, a systematic review (Emmer-
ich et al. 2005) evaluated the effectiveness
of sinus floor elevation using osteotomes.
The inclusion criteria considered studies
that had more than 10 patients and at least
6 months of functional loading. Eight stu-
dies met these inclusion criteria. Within
the limits of such limited long-term data,
the reviewers concluded that the short-
term success rates were similar to success
rates of implants conventionally placed in
the partially edentulous patients (96% after
36 months). Long-term data on outcomes
(45 years) of implants placed with the
osteotome technique are still scarce. As
the database of this systematic review
was heterogeneous, no statistical analysis
was performed with regards to the different
surgical techniques, implant types and/or
grafting materials.
The aims of this prospective cohort study
were to analyze the survival and success
rates of implants installed utilizing the os-
teotome technique, to compare peri-implant
soft tissue parameters and marginal bone
levels of osteotome-installed to conven-
tionally placed implants and to evaluate
the patients’ perception of the treatment.
Material and methods
During the period of 2000–2005, 252 den-
tal implants were inserted in a group of
181 patients at the Department of Per-
iodontology and Fixed Prosthodontics,
University of Bern, Switzerland. These
patients presented with an edentulous
space in the posterior maxilla with reduced
residual bone height, thus making standard
implant placement impossible. One-third
(35%) of the patients had lost their teeth
due to periodontal diseases, 43% of pa-
tients had lost their teeth due to other
reasons like caries, trauma or endodontic
failures and the remaining 22% could not
recall the reason for their tooth loss. Before
implant insertion, the patients had been
treated for existing periodontal disease
according to a comprehensive treatment
strategy (Lang et al. 1998). The operators
were either Faculty members at the De-
partment of Periodontology and Fixed
Prosthodontics, University of Bern, or
postgraduate students in the Department
directly supervised by Faculty members.
In this prospective cohort study, the
survival of implants placed in conjunction
with sinus floor elevation using the osteo-
tome technique (test) was evaluated. The
incidence of biological complications was
also evaluated. Implants placed utilizing
standard surgical procedures, in the same
sextant or on the contra-lateral side served
as the control implants to compare peri-
implant soft tissue conditions and marginal
bone levels between test and control
implants. Patients’ perception on the im-
plant therapy was also assessed using a
visual analogue scale (VAS) questionning
method.
Surgical protocol
The surgical technique utilized was a mod-
ification of the original ‘Summers techni-
que’ (Summers 1994):
� Presurgical patient preparation included
rinsing with 0.1% chlorhexidine for
1 min.
� A local anesthesia was administered in
the buccal and palatal regions of the
surgical area.
� A mid-crestal incision with or without
releasing incision was made and a full-
thickness mucoperiosteal flap was
raised.
Pjetursson et al . Sinus floor elevation
668 | Clin. Oral Impl. Res. 20, 2009 / 667–676 c� 2009 John Wiley & Sons A/S

� With a surgical stent or a distance
indicator, the implant position was
marked on the alveolar crest with a
small round bur (+1.4 mm). After
locating the implant position, the open-
ing of the preparation was widened with
two sizes of round burs (+2.3 mm and
+3.1 mm).
� After confirming the distance from the
alveolar crest to the sinus floor, pilot
drills with diameters of 2.2 and 2.8 mm
were used in sequence to prepare the
implant site to a distance of approxi-
mately 2 mm below the sinus floor.
In soft Type IV bone with a residual
bone height of 5–6 mm, there was
usually no necessity to use the pilot
drills. It was sufficient to perforate the
cortical bone at the alveolar crest with
round burs.
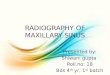
� The first osteotome (Straumann Osteo-
tome Kits
, Straumann AG, Walden-
burg, Switzerland) (Fig. 1) used was a
small diameter (1.6 mm) tapered osteo-
tome. With light tapping, the osteo-
tome was pushed toward the compact
bone of the sinus floor. After reaching
the sinus floor, the osteotome was
pushed about 1 mm further with light
tapping in order to create a ‘greenstick’
fracture on the compact bone of the
sinus floor. A tapered osteotome with
small diameter was chosen to mini-
mize the force needed to fracture the
compact bone.
� The second osteotome used was also a
tapered osteotome, but with a larger
diameter (2.2 mm). This increased the
fracture area of the sinus floor. The
second osteotome was applied to the
same length as the first one.
� The third osteotome used was a
straight osteotome with a diameter of
2.8 mm or about 1 mm smaller than
that of the implant to be placed.
The decision to utilize grafting material
or not was made by the operator. Following
this, the continuation of the surgical pro-
cedures were dependent on whether or not
grafting material was to be placed.
Implant placement without grafting
material:
� Without applying grafting material, the
straight osteotome with a diameter of
2.8 mm was pushed further until it
penetrated the sinus floor.
� The last osteotome used had a form
and diameter suitable for the implant.
For a standard diameter 4.1 mm im-
plant, the final osteotome was a
straight osteotome with a diameter of
3.5 mm and for a wide-body 4.8 mm
implant, the last osteotome used was a
straight osteotome with a diameter of
4.2 mm.
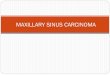
� The final step before placing the im-
plant was to check for membrane
perforation and to check that the pre-
paration was patent to the planned
insertion depth. A depth gauge for the
relevant implant diameter was inserted
to the decided length (Fig. 2).
Implant placement with grafting mate-
rials
� If grafting materials were used, the
osteotomes were not supposed to enter
the sinus cavity per se. Before place-
ment of any grafting material, the sinus
membrane was tested for any perfora-
tions. This was done with the Valsalva
manoeuvre (nose blowing test). The
nostrils of the patient were closed
with the patient blowing against the
resistance. If air leaked through the
implant site, it has to be assumed that
the sinus membrane was perforated,
and no grafting material was placed
into the sinus cavity.
� If the sinus membrane was judged to be
intact, the preparation was filled with
deproteinized bovine bone mineral
(BioOsss
Geistlich Sons Ltd, Wolhu-
sen, Switzerland). The grafting material
was then slowly pushed into the sinus
cavity with the same (+2.8 mm)
straight osteotome. This procedure
was repeated several times.
� After the application of the grafting
material, the tip of the osteotome was
allowed to enter about 1 mm into the
maxillary sinus cavity to test for any
resistance in the preparation site and
finally, before implant placement, the
preparation was checked for patency, as
mentioned before, and the Valsalva
manoeuvre was repeated.
The postsurgical care after the implant
placement with the osteotome technique
was similar to that after standard implant
placement. In addition to the standard oral
home care, antiseptic rinsing with 0.1–0.2%
chlorhexidine twice daily for the first 3
weeks after surgery was recommended. In
cases where bone substitutes were used, the
patients were placed on antibiotic prophy-
laxis (Clamoxyls
750 mg three times daily)
for a period of 1 week (Glaxo-Smith-Kline
AG, Munchenbuchsee, Switzerland).Fig. 1. The Straumann Osteotome Kits
with a range of tapered and straight osteotomes.
Fig. 2. A depth gauge, for the relevant implant
diameter, was inserted to check the potency of
the osteotomy site and to decide on the implant
length.
Pjetursson et al . Sinus floor elevation
c� 2009 John Wiley & Sons A/S 669 | Clin. Oral Impl. Res. 20, 2009 / 667–676

Prosthetic procedure
After a healing period of 4–6 months,
impressions were taken. At impression-
taking or couple of weeks later, prosthetic
abutments were inserted with a 35 N cm
torque and reconstructions were issued.
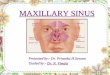
The implants were used to support single
crowns (SCs), solely implant-supported
fixed dental prostheses (FDPs) (Fig. 3) and
combined tooth-implant-supported FDPs.
Clinical examination
At the annual clinical examination follow-
ing functional loading, the following clin-
ical parameters were evaluated:
� survival of implants and reconstruc-
tions.
� distance between the implant shoulder
and the mucosal margin (DIM) in
millimeters (recession scored as nega-
tive value) measured at six sites per
implant.
� pocket probing depth (PPD) in milli-
meters measured at six sites per
implant.
� probing attachment level (PAL) in
millimeters was calculated by subtract-
ing PPD from DIM.
� bleeding on probing (BOP) was mea-
sured at four sites per implant.
All soft tissue measurements were made
by one examiner with a UNC-15 perio-
dontal probe (Hu-Friedys
, Chicago, IL,
USA). Readings were made to the nearest
millimeter.
Radiographic examinations
Radiographs were taken using a Rinn film
holder (XCPs
Instruments, Rinn Corpora-
tion Elgin, IL, USA) with a rigid film-
object X-ray source. In order to perform
the measurements, the radiographs were
captured using a black and white video
camera (Canon, Still Video Products
Group, Tokyo, Japan) and viewed on a
light box. The images were transferred to
a computer and digitized with frame grab-
ber hardware (Matrox Electronic Systems
MVP/AT, Dorval, QC, Canada). Using
image-processing software, digitized images
were stored with a resolution of 512 �512 � 8 bit pixels (256 shades of gray).
Stored images were then displayed on a
monitor and linear measurements were per-
formed by two calibrated examiners with
the help of a cursor (Bragger et al. 1996).
The following measurement was made:
Marginal bone level – the distance from
the implant shoulder (S) to the alveolar
bone crest (AC) mesial and distal.
Patients’ perceptions
Before the clinical examination was per-
formed the patients were asked to give their
perception on the surgical procedure and
the implant therapy in general. The pa-
tients were also asked to evaluate nine
statements concerning general satisfaction,
chewing comfort, cost of therapy, pain and
discomfort during and after the surgical
procedure utilizing a VAS in which 0
indicated ‘total discontent’ and 100 ‘total
satisfaction.’
Statistiscal analysis
We provide descriptive statistical informa-
tion on baseline characteristics of patients
and implants: mean and standard deviation
(SD) or range for continuous characteristics
and percentage distribution for categorical
characteristics. For implant loss the unit
of analysis was the implant. We provide
cumulative survival or cumulative inci-
dence estimates and their 95% confidence
intervals (CI) derived from Kaplan–Meier
calculations (Kaplan & Meier 1958). We
calculated separate 3-year survival esti-
mates according to implant length and
residual bone height categories.
To formally compare mean probing
pocket depth (PPD) (mm), mean probing
attachment levels (mm) and mean BOP
(%) between osteotome and standard im-
plants we fitted multilevel linear regression
models which account for the fact that the
measurements at the same implant and in
the same patient are correlated to some
degree. We report P-values for the mean
difference between osteotome and standard
implants from these models.
For the comparison between osteotome
and standard of categories of PPD and
categories of marginal bone levels we fitted
multilevel logistic regression models and
report the overall P-value derived from
these models. In situations where observa-
tions are not nested and correlated within
levels, these P-values correspond exactly to
P-values derived from the w2 statistics used
for testing differences in categorical vari-
able. In our situation these models allow to
account for the correlated nature of the
measurements within patient and implant.
All analyses were conducted using Stata
version 10 (Stata Corporation, College
Station, TX, USA).
Results
Over the 6-year period (2000–2005), 181
patients with mean age of 54.9 (range 17–
90) years at the time of implant insertion,
were included in the study. The patients
were medically healthy. Fort-one percent
of the patients were non-smokers, 39%
were former smokers and the remaining
36 patients or 20% were smokers. Sixteen
of the smokers, smoked o10 cigarettes per
day, 19 smoked between 10 and 20 cigar-
ettes per day and one was a heavy smoker,
smoking 420 cigarettes per day.
These 181 patients received 252 im-
plants placed in conjunction with maxil-
lary sinus floor elevation using the
osteotome technique (test). For 109 of
these osteotome-installed implants, im-
plants placed in the same sextant or on
the contra-lateral side using standard surgi-
cal procedures served as controls. All
implants were Straumanns
solid screw
implants. The majority of those (60%)
were standard implants with a diameter of
4.1 mm, 35% were wide-body implants
with a diameter of 4.8 mm and the remain-
ing 5% were implants with a reduced
diameter of 3.3 mm. The most frequently
used (62%) implant length was 8 mm fol-
lowed by 10 mm implants that were used
in 31% of the cases. Long 12 mm implants
and short 6 mm implants were used only in
4% and 3% of the cases, respectively.
Forty-six percent of the implant placed
with the osteotome technique were placed
in the position of the second premolar. The
second most common position was the
first molar with 35%, and the third most
common position was the first premolar
with 14% of the implants. Only 5% of the
Fig. 3. A four-unit fixed dental prosthesis supported
by three implants. The implants in positions 24 and
26 were installed with the osteotome technique.
Pjetursson et al . Sinus floor elevation
670 | Clin. Oral Impl. Res. 20, 2009 / 667–676 c� 2009 John Wiley & Sons A/S

implants were placed in the position of
second molars or canines (Fig. 4).
The residual bone height was on average
7.5 mm (SD 2.2 mm) and the apices of the
implants penetrated on average 3.1 mm
(SD 1.7 mm) into the sinus cavity. During
the implant site preparation, membrane
perforations diagnosed by the Valsalva
manoeuvre were detected in 10.4% of the
sites. Two-thirds (65%) of the osteotome-
installed implants were placed without
utilizing grafting material. In the remaining
35%, deproteinized bovine bone mineral
(BioOsss
Geistlich Sons Ltd) was used as
the sinus grafting material.
Survival and failure rates
With the exception of four patients who
experienced excessive hematoma after
surgery, wound healing was uneventful.
Eighteen patients with 18 implants that
only received the implants at the at the
Department of Periodontology and Fixed
Prosthodontics, University of Bern, but the
implant-supported reconstructions were
made by the referring dentist, did not
participate in the follow-up.
The cumulative survival rate of the os-
teotome implants after a mean follow-up
time of 3.2 years, was 97.4% (95% CI:
94.4–98.8%) (Table 1, Fig. 5).
From the original 252 implants inserted,
three implants were lost before loading.
In one case, an 8 mm diameter implant
was inserted without grafting material in
position of tooth 25 in a fully edentulous
patient. The residual bone height was
5 mm. After 6 weeks, the implant became
loose and was removed. The reason for the
implant loss was probably due to the pres-
sure of the provisional removable dental
prosthesis on the implant site during the
early-healing phase. Ten weeks after the
implant was removed a second 8 mm im-
plant was placed and grafting material was
utilized. The healing was uneventful and
the implant was later used as an abutment
to support a 3-unit FDP.
The second implant that was lost before
loading was a short 6 mm diameter implant
placed without grafting material in a site
with a mean residual bone height of 5 mm
(7 mm mesial and 3 mm distal). The im-
plant did not osseointegrate and was re-
moved after 8 weeks. Again, the patient
was wearing a provisional removable dental
prosthesis during the healing period. The
third implant lost before loading was a
10 mm diameter implant placed in position
of tooth 25, in a site with 5 mm residual
bone height. At abutment connection, at
10 weeks postimplant insertion, the im-
plant was not stable and rotated (spinner).
Despite, a prolonged healing time of an-
other 10 weeks the implant did not become
stable and was finally removed after 5
months. The remaining 249 implants
were followed for a mean period of 3.2
years (range 1–7 years). Three additional
implants were lost during the follow-up
time. Two of these patients had received
short 6 mm implants placed in sites with a
residual bone height of only 3–4 mm with-
out utilizing any grafting material. One of
those implants was used as an abutment
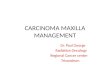
for a 4-unit FDP (16XX13). After a loading
time of 6 months, the patient heard a
‘crack sound’ and felt pain in the anterior
implant (region 13). A couple of weeks
later, the bridge together with the 6 mm
implant was lost (Fig. 6). Subsequently, a
two-stage sinus floor elevation was per-
formed using the lateral approach, and
0
20
40
60
Fre
quen
cy
16 15 14 13 23 24 25 26 27Osteotome implant region
Distribution of osteotome implants in the maxilla
Fig. 4. Distribution of implant position in the maxilla.
Table 1. Cumulative implant survival
Time(years)
Number ofimplants
Implantslost
Survivorfunction
95% CI
1 234 3 0.988 0.963–0.9962 200 2 0.979 0.951–0.9913 144 1 0.974 0.944–0.9884 74 0 0.974 0.944–0.9885 38 0 0.974 0.944–0.9886 13 0 0.974 0.944–0.9887 2 0 0.974 0.944–0.988
CI, confidence interval.
0.00
0.25
0.50
0.75
1.00
Sur
viva
l pro
port
ion
0 2 4 6 8Time
Implant Survival
Fig. 5. Implant survival.
Pjetursson et al . Sinus floor elevation
c� 2009 John Wiley & Sons A/S 671 | Clin. Oral Impl. Res. 20, 2009 / 667–676

two new implants were inserted. For the
second patient, a short 6 mm implant was
lost after a follow-up period of 18 months.
The third patient who lost an implant
in function was the only heavy smoker. He
received two implants in positions 16 and
26 using the osteotome technique. The
residual bone height was between 4 and
5 mm and grafting material was used to
elevate the sinus floor. After 6 months, the
implant in position of tooth 26 had a
diagnosis of peri-implantits with substantial
marginal bone loss. The peri-implantitis
was treated according to the implant main-
tenance and treatment protocol cumulative
interceptive supportive therapy (CIST)
(Lang et al. 2000). The implant, neverthe-
less, became mobile and was removed
3 months later.
According to the implant length, the
survival rates were 100% for 12 mm im-
plants, 98.7% for 10 mm implants, 98.7%
for 8 mm implants and only 47.6% for the
short 6 mm implants (Table 2).
According to residual bone height, the
survival rates were 91.3% for implant sites
with � 4 mm residual bone height and
90% for sites with residual bone height
between 4 and 5 mm, compared with a
survival rate of 100% if the residual bone
height was above 5 mm (Table 3).
Peri-implant soft tissue conditions
One-hundred and nine osteotome-installed
implants (test) were compared with 109
implants placed with standard surgical pro-
cedures (control).
The mean PPD of the test implants was
3.44 compared with 3.51 mm for the con-
trol implants (Table 4). In a frequency
analysis, the majority (83.1%) of the im-
plant sites had a PPD of 1–4 mm, 11.9% of
the sites had a PPD of 5 mm, and the
remaining 5% had a PPD of 6 mm or
more (Table 5). When the frequency analysis
of the PPDs (P¼has changed now:0.999)
and the mean PPDs (P¼ 0.364) were com-
pared, there were no significant differences
between the test and control implants.
The mean PAL of the test implants was
2.47 mm compared with 2.04 mm for the
control implants (Table 4). Moreover, 49%
of the sites around the osteotome-installed
implants BOP positive compared with 51%
for the control implants (Table 4).
When peri-implantitis was defined as
sites with PPD � 5 mm and BOP positive
(Mombelli & Lang 1994), 11.5% of the
sites and 40% of the examined implants had
peri-implantitis. On the other hand, when
the threshold was set at PPD � 6 mm and
BOP positive (Mombelli & Lang 1994), the
number of sites with peri-implantitis was
reduced to 3.7% and the number of im-
plants to 13.8%. With regards to the in-
cidence of peri-implantitis, there was no
significant difference between test and con-
trol implants. At the time of the final
clinical examination, 3% of the implants
had already been treated according the to
the CIST protocol (Lang et al. 2000).
Fig. 6. A short implant that supported a four-unit fixed dental prostheses became loose after a loading time of 6
months and the whole bridge together with the 6 mm implant was lost.
Table 2. The 3-year survival rates according to implant lengths
Implantlength (mm)
Number ofimplants
Implantslost
Survivalrate (%)
95% CI
6 7 3 47.6 0.075 0.8098 157 2 98.7 0.948 0.99710 77 1 98.7 0.911 0.99812 9 0 100 0.717 1
CI, confidence interval.
Table 3. The 3-year survival rates according to residual alveolar bone height
Residualboneheight (mm)
Number ofimplants
Implantslost
Survivalrate (%)
95% CI
� 4 24 2 91.3 0.695 0.9784–5 20 2 90 0.656 0.9745–6 34 0 100 0.916 16–7 39 0 100 0.926 1
� 7 103 0 100 0.971 1
CI, confidence interval.
Table 4. Mean probing pocket depths, probing attachment levels, marginal bone levelsand bleeding on probing
Osteotomeimplants
Standardimplants
P-valuen
Mean SD Mean SD
Mean probing pocket depth (mm) 3.44 1.13 3.51 1.11 0.364Mean probing attachment levels (mm) 2.47 1.05 2.04 0.98 0.185Mean bleeding on probing (%) 49.1 32.1 50.2 29 0.744Mean marginal bone levels (mm) 2.67 0.96 2.75 0.95 .29
nDerived from multilevel linear regression.
SD, standard deviation.
Pjetursson et al . Sinus floor elevation
672 | Clin. Oral Impl. Res. 20, 2009 / 667–676 c� 2009 John Wiley & Sons A/S

Radiographic examinations
Linear measurements to evaluate the mar-
ginal bone levels were performed on digi-
tized images. With the help of a cursor, the
marginal bone level [the distance from
implant shoulder (IS) to the first bone-to-
implant contact (BIC)] was measured. The
mean marginal bone level of the test im-
plants was 2.67 (SD 0.95 mm) compared
with 2.75 mm (SD 0.95 mm) for the con-
trol implants (Table 4). Performing a fre-
quency analysis, the 62.9% of the implants
showed stable bone levels, 28.3% of the
implants had marginal bone levels 0–1 mm
below the expected marginal bone level for
Straumanns
implants, 7.1% of the im-
plants had marginal bone levels 1–2 mm
below and 1.7% of the implants had sig-
nificant (42 mm) bone loss (Table 6).
When comparing marginal bone levels of
the test and control implants, there was no
significant difference, both in the fre-
quency analysis (P¼ 0.200) as well as in
the mean values (P¼ 0.290).
Patient-centered outcomes
The 163 patients examined at the follow-
up were asked to express their opinion
about nine statements. The first two state-
ments dealt with general satisfaction with
the treatment. The patients were asked if
they would undergo similar treatment
again if needed; On the VAS, the mean
VAS score was 91� 17. The median was
98 (range 0–100) (Fig. 7). Moreover,
the patients were asked if they would
recommend this treatment to a friend
or relative, if indicated. On the VAS, the
mean VAS score was 90� 17. The med-
ian was 97 (range 0–100). For both state-
ments only 5% or 3% of the patients
would not be willing to undergo such a
treatment again, respectively.
The third statement addressed the cost
for implant therapy. The cost of implant
therapy was also deemed to be reasonable
to a large extent. On the VAS, the mean
VAS score was 78� 22. The median was
84 (range 0–100) (Fig. 8).
The fourth statement compared the
chewing comfort of teeth with that of
implants. 22.2% felt more secure when
masticating on teeth, 60.2% perceived no
difference and 17.6% preferred masticating
on implants. The mean VAS score was
52� 28. The median was 50 (range 0–
100). The patients, who felt comfortable
when masticating on implant-supported
reconstruction were also asked about the
time it took to adjust to masticating on the
implant-supported reconstruction. Fifty-
two percent of the patients answered ‘im-
mediately,’ 28% answered 1 month, 13%
answered 3 months and the remaining 6%
stated that it took at least 6 months be-
fore they could adjust to their new recon-
structions. The remaining five statements
addressed the surgical procedure. Approxi-
mately 23% of the patients found the surgi-
cal experience unpleasant (Fig. 9). Upon
asking about other surgical complications,
Table 5. Frequency analysis of the probing pocket depth around test and control implants
Probing pocketdepth (PPD) (mm)
All implants(%)
Osteotomeimplants (%)
Standardimplants (%)
P valuen
1–3 59.6 62.8 56.3 0.9994 23.5 20.9 26.15 11.9 11.5 12.46 3.8 3.4 4.3
�7 1.2 1.4 0.9
nDerived from multilevel linear regression.
Table 6. Frequency analysis of the marginal bone levels around test and control implants
Marginal bonelevels (mm)
All implants(%)
Osteotomeimplants (%)
Standardimplants (%)
P valuen
0–3 62.9 66.3 59.4 0.23–4 28.3 26.8 29.74–5 7.1 4.6 9.7
�5 1.7 2.3 1.2
nDerived from multilevel linear regression.
0
20
40
60
80
100
Fre
quen
cy
0–9.9 10–19.9 20–29.9 30–39.9 40–49.9 50–59.9 60–69.9 70–79.9 80–89.9 90–100
Willingness for Retreatment
Fig. 7. Visual analogue scale for willingness to, undergo the treatment again if needed.
0
20
40
60
Fre
quen
cy
0–9.9 10–19.9 20–29.9 30–39.9 40–49.9 50–59.9 60–69.9 70–79.9 80–89.9 90–100
Costs Appropriate
Fig. 8. Visual analogue scale for cost of implant therapy.
Pjetursson et al . Sinus floor elevation
c� 2009 John Wiley & Sons A/S 673 | Clin. Oral Impl. Res. 20, 2009 / 667–676

5% of the patients felt their head was tilted
too far back during the surgery, 5% of the
patients experienced vertigo, nausea and
felt disoriented after the surgical procedure,
but no patient had any problem with unu-
sual eye movements. A small group of five
patients had psychological problems after
the treatment and had to seek medical
assistance.
Discussion
This study has demonstrated that from
the originally 252 implants inserted, 1.3%
were lost before loading. In the first and
second year of function, an additional 1.3%
of the implants were lost, resulting in a
cumulative survival rate of 97.4% for im-
plants placed with the osteotome techni-
que after a mean follow-up time of 3.2
years. These implant losses before func-
tional loading and the annual failure rate
were similar to those reported in systema-
tic reviews on conventionally inserted im-
plants (Lang et al. 2004; Pjetursson et al.
2004; Jung et al. 2008). These survival
rates are also in agreement with previous
studies (Bruschi et al. 1998; Zitzmann &
Scharer 1998; Rosen et al. 1999; Deporter
et al. 2005) reporting on implants inserted
using the transalveolar osteotome techni-
que. Furthermore, a systematic review by
Emmerich et al. (2005) concluded that the
short-term survival rates of osteotome-
installed implants was 96%.
During the entire implant site prepara-
tion, it was crucial to maintain a pre-
cise control of the penetration length of
the osteotomes. These should just pene-
trate through the sinus floor without
entering the sinus cavity. Following dis-
placement of the sinus floor, the grafting
material that was introduced elevated the
Schneiderian membrane without the in-
struments entering the sinus cavity.
Regular osteotomes have sharp cutting
edges. Thus, entry into the sinus cavity
with the tip of the instrument would in-
crease the risk of membrane perforation. In
the present study, membrane perforation
with 10%, was the most common compli-
cation using the osteotome technique. In
cases in which a membrane perforation was
noted, no grafting material was placed.
These complications, however, did not
influence the integration of the implants.
In all such cases the implants were stable
and could be used as abutments for im-
plant-supported reconstructions.
Morphological features such as an obli-
que sinus floor (4451 inclination) may
affect the treatment outcome. This does
not provide a suitable situation for utilizing
the osteotome technique (Fig. 10). The
reason for this lies within the geometry of
the penetration of the osteotome that will
first enter the sinus cavity at the lower
level of an oblique sinus floor, while still
having bone resistance on the higher level.
Consequently, there will be a higher risk
for perforating the Schneiderian membrane
with the sharp margins of the osteotome.
It has to be realized that the final osteo-
tome should enter the preparation site only
once. If is the largest osteotome is used
several times to introduce the grafting ma-
terial into the sinus cavity or if several
attempts were performed to prepare the
site with the largest osteotome, there is a
high risk of increasing the diameter of the
preparations in sites with Type III or Type
IV bone. Hence, this may jeopardize
achieving primary stability of the implants.
On the other hand, if the last osteotome
diameter is too small compared with the
implant diameter, too much torque will
be used when inserting the implant. Ex-
cessive compression of the bone results in
more trauma to the bone and hence, greater
bone resorption may be encountered. This,
in turn, may delay the osseointegration
process (Abrahamsson et al. 2004). When
placing implants in sites with reduced bone
volume, it is important to keep a fine
balance between primary stability and
minimizing trauma to the bone.
In the present study, no attempts were
made to optimize the outcomes by using
strict exclusion criteria. Hence, periodontal
patients, smokers, patients with parafunc-
tional habits and patients wearing remova-
ble provisional reconstructions were also
included. The only inclusion criterion was
that the patients were in good general
health and were treated for existing perio-
dontal diseases and rampant caries accord-
ing to a comprehensive treatment strategy
before implant insertion (Lang et al. 1998).
Moreover, no restrictions were made re-
garding the minimal preoperative bone
height. The decision on whether or not
the osteotome technique was suitable,
was made individually by each Faculty
member.
Regarding existing residual bone height,
20% of the implants in the present study
were placed in sites with residual bone
height of � 5 mm. This, in turn, means
that the limit of the osteotome technique
was indeed tested. It was evident that the
failure rates of the osteotome-installed im-
plants increased in correlation to reduced
0
10
20
30
40
Fre
quen
cy
0–9.9 10–19.9 20–29.9 30–39.9 40–49.9 50–59.9 60–69.9 70–79.9 80–89.9 90–100
Intervention Unpleasant
Fig. 9. Visual analogue scale of the unpleasantness of the surgical experience.
Fig. 10. Radiograph showing an oblique sinus floor
(4451 inclination), where the osteotome technique
is not suitable due to a high risk of membrane
perforation.
Pjetursson et al . Sinus floor elevation
674 | Clin. Oral Impl. Res. 20, 2009 / 667–676 c� 2009 John Wiley & Sons A/S

residual bone height and reduced implant
length. No implants were lost if the resi-
dual bone height was 45 mm, compared
with a failure rate of approximately 10% if
the residual bone height was o5 mm.
Moreover, for short 6 mm implants the
survival rate was only 48%. This clearly
demonstrated that the transalveolar sinus
floor elevation technique was most predic-
able with residual alveolar bone height of
5 mm or more and with implants of 8 mm
or more.
Moreover, peri-implant soft tissue para-
meters and marginal bone levels around the
osteotome-installed implants (test) were
compared with those parameters around
implants placed with standard surgical pro-
cedures (control). Such a comparison has
previously not been reported. There were
no statistically significant differences be-
tween test and control implants regarding
either PPD, probing attachment levels,
percentage of sites that bled on probing
and marginal bone levels. In the present
study, the prevalence of peri-implantitis
did not differ between the test and control
implants either. However, the prevalence
of peri-implantitis was influenced by the
threshold chosen for the definition of peri-
implantitis. When peri-implantitis was de-
fined as PPD � 5 mm and BOP-positive
sites, 40% of the examined implants had at
least one site with peri-implantitis. When
the definition was limited to PPD � 6 mm
and BOP positive, the percentage of im-
plants with at least one site with peri-
implantitis was reduced to 13.8%. This
high incidence of peri-implantitis can, at
least partly, be explained by the fact that
when implants are placed in edentulous
spaces with reduced bone height in the
positions of first or second premolar or
the first molar in the maxilla, the bone
levels on the adjacent teeth are often more
coronal that the alveolar crest in the eden-
tulous space (Fig. 11). This unequal level in
the alveolar bone may have lead to an
increased PPD mesial to those implants.
Because the prevalence of implants with
progressive bone loss (42 mm) was only
1.7% in the present study, such pockets
may be considered as ‘pseudopockets.’
From a total of 163 questionnaires dis-
tributed, questionnaires were completed
with rates varying between 94 and 100%.
This, in turn, reflected a reliable and accu-
rate subjective assessment of the implant
therapy with a high objective treatment
outcome.
When comparing the chewing function
on teeth and implants, 60% of the patients
revealed no preference. Twenty-two per-
cent of the patients felt more comfortable
when masticating on teeth and surpris-
ingly, 18% felt more comfortable when
masticating on implant-supported recon-
structions. In the present study, over 80%
of the patients confirmed that it took them
o1 month to adapt to the implant recon-
struction, following which the implant
contacts felt like ‘natural’ teeth.
Even though 23% of the patients re-
ported the surgical procedure as unpleasant,
490% of the patients would be willing to
undergo implant therapy again if necessary
and dentally indicated. Only five out of the
163 patients assessed the VAS at the lower
units, indicating a lack of willingness to
undergo the same implant therapy again.
In the present study, a small group of
5 patients had psychological problems
after the treatment and, therefore, had to
seek medical assistance. It must be rea-
lized, however, that the most difficult
patients to treat are patients with high or
unrealistic expectations for both implant
therapy in general as well as the osteotome
technique in particular. The proportion of
such patients in the present study pointed
to the fact that the psychological aspects
associated with such treatment are not to
be underestimated.
In conclusion, the transalveolar osteo-
tome technique was demonstrated to re-
present a reliable and predictable method
for implant insertion in the posterior max-
illa, at sites with 5 mm or more preopera-
tive residual bone height and a relatively
flat sinus floor.
Soft tissue parameters, such as PPD,
PAL and BOP and marginal bone levels
did not differ between the osteotome-
installed implants and conventionally
placed implants.
More than 90% of the patients were
satisfied with the implant therapy per-
formed and would be willing to undergo
such therapy again if necessary. The cost
associated with implant therapy was also
considered to be justified. Because the pre-
sent study covered a mean observation
period of 3.2 years following implant in-
stallation, there is still a need for long-term
clinical documentation (45 years) of the
outcomes of implants installed transalveo-
lar utilizing the osteotome technique.
Acknowledgements: This study has
been supported by the Clinical
Research Foundation (CRF) for the
promotion of oral health, University of
Bern, Switzerland.
References
Abrahamsson, I., Berglundh, T., Linder, E., Lang,
N.P. & Lindhe, J. (2004) Early bone forma-
tion adjacent to rough and turned endosseous
implant surfaces. An experimental study in
the dog. Clinical Oral Implants Research 15:
381–392.
Boyne, P.J. & James, R.A. (1980) Grafting of
the maxillary sinus floor with autogenous
marrow and bone. Journal of Oral Surgery 38:
613–616.
Bragger, U., Hugel-Pisoni, C., Burgin, W., Buser, D.
& Lang, N.P. (1996) Correlations between radio-
graphic, clinical and mobility parameters after
loading of oral implants with fixed partial den-
tures. A 2-year longitudinal study. Clinical Oral
Implants Research 7: 230–239.
Bruschi, G.B., Scipioni, A., Calesini, G. & Bruschi,
E. (1998) Localized management of sinus floor
with simultaneous implant placement: a clinical
report. International Journal of Oral & Maxillo-
facial Implants 3: 219–226.
Deporter, D.A., Caudry, S., Kermalli, J. & Adeg-
bembo, A. (2005) Further data on the predictabil-
ity of the indirect sinus elevation procedure used
Fig. 11. Radiograph showing an implant inserted in
edentulous space with reduced bone height com-
pared with the bone level distal on the adjacent
tooth.
Pjetursson et al . Sinus floor elevation
c� 2009 John Wiley & Sons A/S 675 | Clin. Oral Impl. Res. 20, 2009 / 667–676

with short, sintered, porous-surfaced dental im-
plants. International Journal of Periodontics and
Restorative Dentistry 25: 585–593.
Emmerich, D., Att, W. & Stappert, C. (2005) Sinus
floor elevation using osteotomes: a systematic
review and meta-analysis. Journal of Perio-
dontology 76: 1237–1251.
Engelke, W. & Deckwer, I. (1997) Endoscopically
controlled sinus floor augmentation. A preliminary
report. Clinical Oral Implants Research 8: 527–531.
Ferrigno, N., Laureti, M. & Fanali, S. (2006) Dental
implants placement in conjunction with osteotome
sinus floor elevation: a 12-year life-table analysis
from a prospective study on 588 ITI implants.
Clinical Oral Implants Research 17: 194–205.
Jung, R.E., Pjetursson, B.E., Glauser, R., Zembic,
A., Zwahlen, M. & Lang, N.P. (2008) A systema-
tic review of the 5-year survival and complication
rates of implant-supported single crowns. Clinical
Oral Implants Research 19: 119–130.
Kaplan, E.L. & Meier, P. (1958) Nonparametric
estimation from incomplete observations. Jour-
nal of the American Statistical Association 53:
457–481.
Lang, N.P., Siegrist, B.E. & Bragger, U. (1998)
Strategically important abutments. Schweizer
Monatsschrift fur Zahnmedizin 6: 632–643.
Lang, N.P., Pjetursson, B.E., Tan, K., Bragger, U.,
Egger, M. & Zwahlen, M. (2004) Systematic
reviews of fixed partial dentures (FPD) after an
observation period of at least 5 years. Part II:
implant–-tooth supported bridges. Clinical Oral
Implants Research 15: 643–653.
Lang, N.P., Wilson, T.G. & Corbet, E.F. (2000)
Biological complications with dental implants:
their prevention, diagnosis and treatment. Clin-
ical Oral Implants Research 11 (Suppl. 1): 146–
155.
Lekholm, U. & Zarb, G. (1985) Patient selection
and preparation. In: Branemark, P-I, Zarb, G &
Albrektsson, T, eds. Tissue Integrated Prosthesis:
Osseointegration in Clinical Dentistry, 199–210.
Chicago: Quintessence.
Mombelli, A. & Lang, N.P. (1994) Clinical para-
meters for the evaluation of dental implants.
Periodontology 2000 4: 81–86.
Pjetursson, B.E., Tan, K., Lang, N.P., Bragger, U.,
Egger, M. & Zwahlen, M. (2004) Systematic
reviews of fixed partial dentures (FPD) after an
observation period of at least 5 years. Part I:
implants supported bridges. Clinical Oral Im-
plants Research 15: 625–642.
Rosen, P.S., Summers, R., Mellado, J.R., Salkin,
L.M., Shanaman, R.H., Marks, M.H. & Fugaz-
zotto, P.A. (1999) The bone added osteotome
sinus floor elevation technique: multicenter retro-
spective report of consecutively treated patients.
International Journal of Oral & Maxillofacial
Implants 14: 853–858.
Summers, R.B. (1994) A new concept in maxillary
implant surgery: the osteotome technique.
Compendium 15: 152, 154–156, 158 passim;
quiz 162.
Tatum, H. Jr. (1986) Maxillary and sinus implant
reconstructions. Dental Clinics of North America
30: 207–229.
Zitzmann, N.U. & Scharer, P. (1998) Sinus eleva-
tion procedures in the resorbed posterior maxilla.
Comparison of the crestal and lateral approaches.
Oral Surgery Oral Medicine Oral Pathology Oral
Radiology Endodontology 85: 8–17.
Pjetursson et al . Sinus floor elevation
676 | Clin. Oral Impl. Res. 20, 2009 / 667–676 c� 2009 John Wiley & Sons A/S

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具