Embed Size (px)
Citation preview

Maxillary Sinus Membrane Repair: Updateon Technique for Large and
Complete PerforationsMichael A. Pikos, DDS
Grafting of the maxillary sinuswas first described by Tatum,1
Boyne and James,2 and latermodified by others. It has become ahighly predictable surgical techniquefor posterior maxillary site develop-ment and implant reconstruction ifproper treatment planning, careful sur-gical technique, adequate clinicianexperience, and patient compliancecriteria are met.1,3–8 There are, how-ever, complications associated withthis technique that would be expectedwith any surgical procedure. Althoughthe overall complication rate is low,the most common complication ismembrane perforation.8–10
The purpose of this article is to re-port on a modification of a previouslypublished technique that can be used forpredictable repair of large and completesinus membrane perforations.
Anatomy
The maxillary sinus begins at ap-proximately the third month of fetal lifeas an invagination from the middle me-atus of the nasal cavity into the maxilla.It is the first and largest of the paranasalsinuses to develop, and continues to in-crease in size until the permanent teethhave erupted. Cervin11 examined 107people with CT and showed that themean transverse dimension (mediolat-eral) and width (anteroposterior) of thenormal adult sinus are 27 and 35.6 mm,respectively. This study also showed adirect correlation of adult sinus width
with body weight and interzygomaticbuttress distance. Another study usingaxial CT in 115 patients aged more than20 years showed the average volume ofthe normal adult maxillary sinus torange from 4.56 to 35.21 cm3 (mean,14.71 cm3).12
In a well done cadaver study,Stammberger13 showed that the heightand the width of the maxillary sinus inedentulous specimens are significantlygreater than those of dentate cadavers.However, no significant difference inthe anteroposterior length or volumewas reported. This same study in-cluded a simulated sinus lift that re-vealed an inferior sinus graft volumeof 3.5 cm3 needed for a 15 mm aug-mentation and 5.66 cm3 required for a20 mm augmentation.
The maxillary sinus has a horizon-tal pyramidal shape consisting of abase, an apex, and 4 sides. The base(medial wall) forms the vertical lateralwall of the nasal cavity, and the apexis at the junction of the maxillary andzygomatic bones. The remaining 3sides of the pyramid form the superior,anterior, and posterior walls of the si-nus. The superior wall makes up theroof of the sinus, which is also theorbital floor. The anterior wall formsthe facial portion of the maxillarybone. The posterior and lateral walls
merge to form the posterolateral wallsof the sinus, and separates the sinusfrom the infratemporal fossa andforms the maxillary tuberosity andpterygoid fossa.14
The medial wall demarcates themaxillary sinus from the nasal fossaand supports the lower and middleconchae. Located in the anterosuperiorarea of the medial wall is the ostium, a7 to 10 mm long passage that is vari-able in size, location, and efficacy indraining the sinus.15 The ostium, theinfundibulum, and the middle meatusare often referred as the osteomeatalcomplex. This communication be-tween the maxillary sinus and thenasal cavity must be maintained toassure health of the maxillary and ad-joining paranasal sinuses.
Maxillary Sinus Physiology
The maxillary sinus is lined with arespiratory mucosa similar to that ofthe nose and other paranasal sinuses. Itconsists of a mucoperiosteum with 3layers: an epithelial covering, a laminapropria, and periosteum.16 The maxil-lary sinus membrane varies in thick-ness, but is generally 0.3 to 0.8 mm.17
The epithelial lining is a singlelayer of pseudostratified columnar cil-iated epithelium with few blood ves-
Private Practice, Palm Harbor, FL.
ISSN 1056-6163/08/01701-024Implant DentistryVolume 17 • Number 1Copyright © 2008 by Lippincott Williams & Wilkins
DOI: 10.1097/ID.0b013e318166d934
Maxillary sinus membrane perfo-ration is the most common complica-tion that occurs with sinus elevationaugmentation surgery. A technique us-ing a slow resorbing type I collagenmembrane for repair of large andcomplete sinus membrane perfora-tions is described. The biocompatibil-
ity and semirigid structural integrityof this membrane, along with externaltack fixation, allows for optimal mem-brane stabilization and maintenance.(Implant Dent 2008;17:24–31)Key Words: sinus elevation augmen-tation, osteomeatal complex, collagenmembrane, external fixation
24 MAXILLARY SINUS MEMBRANE REPAIR

sels and is thicker than that of theother paranasal sinuses. Numerousgoblet cells are present within the mu-cosa and are the major source of mu-cous secretion. The highest density ofthese cells is located near the sinusostium. The density of ciliated cells ishigh, ranging from 91.3% to 97.7%, ex-cept near the ostium, where the densityis decreased by half.18 The cilia movemucous and debris in a spiral fashiontoward the ostium. They beat approxi-mately 1000 times/min while movingthe mucociliary blanket19 at a flow rateof 6 mm/min.20,21 Normally the cilia canclear the sinus in 10 to 30 minutes underphysiologic conditions.13,22
The lamina propria consists of athin layer of connective tissue withfew elastic fibers. It is thickest at themedial wall and contains more sero-mucous glands than the lateral wall.23
The periosteum is tightly bound to theoverlying lamina propria, but is easilydetachable from the underlying bone,making membrane separation duringthe sinus lift procedure relatively easy.
Any factors that compromise mu-cous production, ciliary function, orpatency of the ostium can increase therisk of sinusitis. As a result, with sinuselevation augmentation surgery, it isimportant to maintain membrane in-tegrity to allow for confinement of theparticulate graft and to decrease therisk of infection.
Maxillary Sinus Membrane Perforationand Repair
The most common complicationinvolving sinus elevation augmenta-tion is membrane perforation.8 –10
The incidence of this occurrence hasbeen reported to range from 10% to56%.8,9,24 –26 A variety of techniqueshave been proposed to managethese perforations. These include su-turing,27,28 the use of collagen mem-branes,9,27–31 fibrin sealants,32–35
freeze dried human lamellar bonesheets,27,28,36 and oxidized regener-ated cellulose.37
All these techniques involve re-pair of sinus membrane perforationsthat range in size from 2 mm toapproximately 1.5 cm with one ex-ception.9,10 Pikos has reported on theuse of a slow resorbing collagenmembrane for repair of large (�1.5
cm) perforations and for sinuses thatinvolve complete tears.9
Surgical Technique for Large andTotal Perforations
The technique involves a modifi-cation of the one reported in 1999.9 Itincludes the use of a slow resorbingcollagen membrane with adequatestructural integrity to adapt and main-tain itself within the internal bonyanatomy of the sinus.
Once the bony window is outlinedit should be removed to allow for visu-alization of the existing sinus mem-brane. Remnants of the sinus membranecan then be elevated from the bony floorand all walls including the posteriorwall. This is important to allow for di-rect contact of the graft with its bonyblood supply and to prevent epithelialinvagination into the graft.
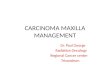
Next, a 30 � 40 collagen mem-brane (Biomend; Zimmer Dental,Carlsbad, CA) is modified by round-ing the corners and creating approxi-mately 1 cm slits at each corner (Fig.1). The generic cuts allow the mem-brane to fold on itself after placementwithin the sinus. It is easier to makethese cuts before hydrating the mem-brane in either saline or PRP (Har-vest Technologies, Plymouth, MA).One end of the membrane is thenplaced at the anterior, posterior, andsuperior bony window and fixatedexternally with tacks (Figs. 2 and 3).This stabilizes the membrane and al-lows it to drape internally as it adaptsto the internal anatomy of the sinus.This external fixation is especially im-portant to contain the particulate bonegraft in the more pneumatized sinuswhere the anterior–posterior and/ormedial–lateral dimension is largerthan normal. As mentioned previ-ously, it is important to not cover thebony floor or inferior segment (�10mm) of the bony walls (anterior, pos-terior, medial, and superior). Themembrane may need to be custom-trimmed once external fixation is com-plete. Also, it may be necessary to usea second collagen membrane as anextension that can be sutured with 4-0chromic suture to the fixated mem-brane and trimmed appropriately (Fig.4). The use of platelet rich plasma actsas an adhesive to adapt the membraneto all walls.
CASE REPORTS
A healthy 52-year-old whitemale was referred for implant eval-uation on June 11, 2002. The patientexpressed a desire to have permanentteeth to replace his failing dentitionin the maxillary left posterior quad-rant. His maxillary arch treatment
Fig. 1. Biomend collagen membrane (30 � 40mm2) with rounded edges and cut corners.Fig. 2. Biomend collagen membrane with 3point external tack fixation at anterior, supe-rior, and posterior windows.Fig. 3. Particulate graft of tibial marrow, Bio-Oss, and PRP.Fig. 4. Biomend collagen membrane withsecondary extension membrane sutured with4-0 chromic suture (arrows).
IMPLANT DENTISTRY / VOLUME 17, NUMBER 1 2008 25

plan for reconstruction included a3-unit implant-supported bridge.
Clinical, panoramic (Fig. 5), andCT (Fig. 6) examinations revealed apartially pneumatized left maxillarysinus with a well-defined radiopaquemass measuring 2.5 � 2.0 cm2 located
on the sinus floor adjoining the poste-rior wall. Also a failing maxillary leftsecond bicuspid and first molar werenoted.
Initial treatment included surgicalextraction of the failing teeth withsocket graft preservation. This wasfollowed 4 months later by left sinuselevation augmentation surgery thatincluded intentional perforation of the
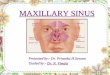
sinus membrane to remove the sus-pected mucous retention cyst (Figs. 7and 8) for biopsy. The biopsy reportwas consistent with the preoperativediagnosis of mucous retention cyst.This resulted in complete membraneperforation (Fig. 9) that required ele-vation of all mucosal remnants fromthe bony walls including the floor ofthe sinus. A 30 � 40 mm2 Biomendcollagen membrane was then trimmedand cut (Fig. 1) to allow for placementinto the sinus creating a customizedbarrier to prevent graft migration. Thismembrane was fixated externally (Fig.10) for stabilization. Next, the partic-ulate graft complex of mineralized ir-radiated cancellous allograft (Puros;Zimmer Dental, Tutogen Medical,Alachua, FL), Bio-Oss (Osteohealth,Shirley, NY 11967), and PRP (HarvestTechnologies) was placed into the cul-de-sac created by the slow resorbingcollagen membrane (Fig. 11). Carefulattention was paid to avoid coveringthe inferior 10 mm of the bony wallsso as to not compromise bony bloodsupply to the graft.
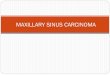
A 20 � 30 mm2 Biomend Extendcollagen membrane was then placedover the lateral window (Fig. 12) andfixated with 2 titanium tacks. Twelvemonths later, the graft was found to bewell incorporated with only minimalbone resorption found at the anteriorsuperior border (Fig. 13). Core biopsyof the graft revealed many areas ofmature bone with a lamellar patternaround the allograft particles (Fig. 14).Three 4.7 � 16 mm2 tapered, threadedroot form implants (Zimmer Dental,Carlesbad, CA) were placed one eachin the maxillary left second bicuspid,first molar and second molar sites.Stage II surgery was then followed 3months later by fabrication of a 3-unitimplant-supported bridge (Figs. 15and 16).
DISCUSSION
An important aspect of sinus aug-mentation surgery is to maintain theintegrity of the native membrane. Thisis done solely to confine the particu-late graft material (excluding use ofblock bone) within the bony housingof the sinus. The purpose for mem-brane repair is also to prevent graftextravasation. Sinus membrane perfo-
Fig. 5. Panoramic radiograph indicating ex-tent of mucous retention cyst. Maxillary leftsecond bicuspid and first molar subsequentlyextracted before sinus elevation.Fig. 6. CT showing mucous retention cyst ofleft maxillary sinus.Fig. 7. Removal of mucous retention cyst viaintentional perforation of sinus membrane.Fig. 8. Mucous retention cyst.
Fig. 9. Complete membrane perforation sec-ondary to cyst removal.Fig. 10. External fixation of collagen mem-brane.Fig. 11. Particulate graft of mineralized irradi-ated allograft, Bio-Oss, and PRP.Fig. 12. Biomend Extend collagen mem-brane (20 � 30 mm2) placed over windowwith tack fixation.
26 MAXILLARY SINUS MEMBRANE REPAIR

rations that are not repaired or areinadequately repaired can result inboth short-term and long-term compli-cations.8 Bacterial penetration andmucous invasion into the graft cancompromise the amount of bone for-mation. Graft material may leak
through the perforated site, can mi-grate to the ostium, and be eliminatedthrough the nose or obstruct the os-tium and prevent drainage.8 Ostiumobstruction can also occur as a resultof swelling of the membrane duringsurgery. All these conditions increasethe risk of infection. Most important tothe success of graft incorporation,however, is maintenance of the bonyblood supply to the graft. As a result,it becomes critical to not cover thebony floor or the inferior 10� mm ofthe anterior, posterior, medial, and lat-eral bony walls during the repair. Thisbecomes especially challenging forcomplete membrane perforation. Fu-gazzotto and Vlassis28 reported onlarge sinus membrane perforation re-pair with a pliable porcine membraneexternally fixated and completely cov-ering the internal bony wall anatomyof the sinus. The Loma Linda pouchtechnique38 involves use of a slowresorbing collagen membrane with ex-ternal tack fixation that also results incomplete membrane coverage of allinternal bony walls including thefloor. It is the author’s opinion thatcomplete coverage of all internal sinusbony anatomy with a slow resorbingcollagen membrane can impede bloodsupply to the graft and result in incom-plete graft incorporation.
Large perforations (�1.5 cm) arethe most challenging to repair and canoccur for a number of reasons. Theseinclude operator error, manipulationof inherently thin membranes (�0.3mm), presence of septae, presence ofpathology, and secondary to previoussurgery. The previously mentioned tech-niques for membrane repair can beproblematic and unpredictable for bothlarge perforations and membranes withcomplete tears.27–37 Suturing is not pos-sible because the membrane edges can-not be approximated. In addition, thesemembranes can be thin and will tearupon suturing.
The use of cyanoacrylate adhesiveor autologous fibrin glue for mem-brane repair is also not feasible be-cause these techniques require themembrane edges to be approximatedbefore application of the glue.34,35 Sev-eral authors have proposed the use offreeze dried human lamellar bonesheets for membrane repair.27,28,36 Thismaterial has significant stiffness and is
not easily adaptable to the internalbony anatomy for large perforations.The use of oxidized regenerated cellu-lose37 is also not practical for largeperforations and complete tears be-cause of its lack of rigid structuralintegrity and fast resorbing properties.
Collagen membranes can be used;however, studies reported by some au-thors include the use of a fast resorb-ing collagen membrane that possessesno rigidity and as a result may beinadequate for large perforation repair.Proussaefs et al30 used a split-mouthdesign with 5 patients and reportedthat nonperforated sites demonstratedsignificantly more bone formation(34.40%) than perforated sites (12.80%).Implant survival at second stage surgerywas significantly inferior in perforatedsites (54.5%) when compared with non-perforated sites (100%). Proussaefs etal31 again used a split mouth designthat included 12 patients with bilateralsinus grafting and found that nonper-forated sites demonstrated signifi-cantly more bone formation (33.58%� 7.45%) than perforated sites(14.17% � 7.06%). Perforated sitesalso demonstrated significantly moresoft tissue formation than nonperfo-rated sites. Also, in nonperforatedsites, residual graft particles had moreof their surface in contact with bonethan perforated sites. In both studies, afast resorbing collagen membrane(Collatape—Zimmer Dental) wasused. Choi et al34 reported on the ef-ficacy of autologous fibrin glue in themanagement of large perforations ofthe maxillary sinus membrane occur-ring during sinus lifts. In this doubleblind study, 6 adult female mongreldogs were used. A laceration approx-imately 2 cm in length was made withone side repaired with fibrin glue andthe control side covered with a fastacting bioabsorbable collagen mem-brane. Wound areas were biopsied 2weeks after the operation. Wounds re-paired with fibrin glue showed newlyformed continuous epithelium acrossthe previous perforation site. However,wounds treated with the collagenmembrane exhibited extensive fibrosis,inflammatory infiltration, and absent ep-ithelium. This study may suggest thatutilization of fast resorbing collagenmembranes is not adequate for largemembrane perforations.
Fig. 13. Re-entry 12 months postgraft. Notewell-incorporated graft and slight bone lossat anterior superior margin.Fig. 14. High power photomicrograph withlamellar pattern of mature bone (arrow)around the allograft particles.Fig. 15. Radiograph of completedprosthetics— 4 years functional load. Notemaintenance of crestal bone height anduniform trabecular bone pattern.Fig. 16. Completed prosthetics—4 years.
IMPLANT DENTISTRY / VOLUME 17, NUMBER 1 2008 27

Although small membrane repairusing fast resorbing collagen mem-branes (Collatape) has been well doc-umented, no data are available on theconsistent repair of large membraneperforations or repairs with no sinusmembrane present. As describedherein, the Biomend collagen mem-brane has been used successfully forpredictable membrane repair since19969,10 with no increased incidence ofinfection. In addition, this material hasbeen successfully used for particulategrafting of sinuses in which no mem-brane was present as a result of previoussurgery or pathology. This membranehas unique physical and biologic prop-erties that make it very suitable formembrane repair or replacement. It isprepared from purified bovine Achillestendon in a chemically cross-linkedform and supplied in sterile individualsections. Its rigid structural integrity ismaintained for approximately 6 to 8weeks before resorbing. This type Icollagen is biocompatible and resorbsthrough catabolic processes, includingdegradation of extracellular enzymesand collagenolytic enzymes, and maybe replaced by new collagen.39,40 Thecollagen membrane is well toleratedby soft tissues and possesses biologicproperties that aid in optimal heal-ing.41 Collagen is chemotactic for fi-broblasts,42,43 which aids in promotingcell migration. It also possesses hemo-static properties through its ability toaggregate platelets, which may facili-tate early wound stabilization andmaturation.44
The same collagen membrane hasalso been used to cover the osteotomywindow of the sinus elevation proce-dure. This protocol has been followedsince 1996. This not only prevents softtissue invagination but also results information of a cortical plate as early as6 to 9 months over the window area.This author recommends use of theBiomend collagen membrane for allperforations regardless of size. The mainadvantage in using this membrane evenfor small perforations that would nor-mally be treated with Collatape is that itcreates space facilitating graft placement.The biocompatibility and semirigidstructural integrity of this membraneallow this versatile application to allsize membrane perforations. There is
also no need to abort a sinus elevationaugmentation procedure when even acomplete tear occurs.
CONCLUSIONS
This case presentation demon-strates the application of a slowresorbing collagen membrane that canbe used not only for repair of large andsmall sinus membrane perforations,but also for circumstances in which nomembrane exists (previous surgery,pathology). The biocompatibility andsemirigid structural integrity of thismembrane, along with external tackfixation, allow for optimal membranestabilization and maintenance.
Disclosure
The author claims to have no fi-nancial interest, directly or indirectly,in any entity that is commercially re-lated to the products mentioned in thisarticle.
REFERENCES
1. Tatum H Jr. Maxillary and sinus im-plant reconstructions. Dent Clin North Am.1986;30:207-229.
2. Boyne PJ, James RA. Grafting of themaxillary sinus floor with autologous mar-row and bone. J Oral Surg. 1980;38:613-616.
3. Wallace SS, Froum SJ. Effect ofmaxillary sinus augmentation on the sur-vival of endosseous dental implants. A sys-tematic review. Ann Periodontol. 2003;8:328-343.
4. Misch CE. Maxillary sinus augmen-tation for endosteal implants: Organizedalternative treatment plans. Int J Oral Im-plantol. 1987;4:49-58.
5. Zinner ID, Small SA. Sinus-lift graft:Using the maxillary sinuses to support im-plants. J Am Dent Assoc. 1996;127:51-57.
6. Tidwell JK, Blijdorp PA, StoelingaOJW, et al. Composite grafting of the max-illary sinus for placement of endosteal im-plants. A preliminary report of 48 patients.Int J Oral Maxillofac Surg. 1992;21:204-209.
7. Triplett RG, Schow SR. Autologousbone grafts and endosseous implants:Complementary techniques. J Oral Maxil-lofac Surg. 1996;54:486-494.
8. Misch CE. The maxillary sinus lift andsinus graft surgery. In: Misch CE, ed. Con-temporary Implant Dentistry. Chicago, IL:Mosby;1999:469-495.
9. Pikos MA. Maxillary sinus mem-brane repair: Report of a technique forlarge perforations. Implant Dent. 1999;8:29-34.
10. Pikos MA. Complications of maxil-lary sinus augmentation. In: The SinusBone Graft, 2nd Ed, Vol. 9. Hanover Park,IL: Quintessence Publishing Co, Inc; 2006:103-125.
11. Cervin A. Relations between bloodflow and mucociliary activity in the rabbitmaxillary sinus. Acta Orolarygol (Stockh).1988;105:350-356.
12. Cervin A, Lindberg S, Mercke U.The effect of neuropeptide Y on mucocili-ary activity in the rabbit maxillary sinus.Acta Otolaryngol (Stockh). 1991;111:960-966.
13. Stammberger H. Endoscopic nasalsurgery: Concepts in treatment of recur-ring rhinosinusitis. Part I: Anatomic andpathophysiologic considerations. Otolar-yngol Head Neck Surg. 1986;2:143-147.
14. Abubaker AO. Applied anatomy ofthe maxillary sinus. Oral Maxillofac SurgClin North Am. 1999;11:1-13.
15. Alberti PW. Applied surgical anat-omy of the maxillary sinus. Otolaryngol ClinNorth Am. 1976;9:12-15.
16. Scharf KE, Lawson W, Shapiro JM,et al. Pressure measurement in the normaland occluded rabbit maxillary sinus. Laryn-goscope. 1995;105:570-574.
17. Morgensen C, Tos M. Quantitativehistology of the maxillary sinus. Rhinology.1977;15:129-134.
18. Halma AR, Decreton S, Bijloos JM,et al. Density of epithelial cells in the normalhuman nose and the paranasal sinusmucosa: A scanning electron microscopicstudy. Rhinology. 1990;28:25-32.
19. Watzek G, Bernhart T, Ulm C.Complications of sinus perforations andtheir management in endodontics. DentClin North Am. 1997;1:463-583.
20. Anderson L, Camner P, Jensen P,et al. Nasal clearance in monozygotic twin.Am Rev Respir Dis. 1974;110:301-305.
21. McCafferey TR, Kern EB. Clinicalevaluation of nasal obstruction. Arch Otolar-yngol Head Neck Surg. 1979;105:542-545.
22. Chapnik JS, Bach MC. Bacterialand fungal infections. Otolaryngol ClinNorth Am. 1976;9:44-57.
23. McGowan DA, Baxter PW, JamesJ. The Maxillary Sinus and Its Dental Impli-cations. Oxford: Butterworth-HeinemannLtd.; 1993:1-39.
24. Kasabah S, Krug J, Sim[ring]unekA, et al. Can we predict maxillary sinus mu-cosa perforation? Acta Medica (HradecKralove). 2003;46:19-23.
25. van den Bergh JP, ten Bruggen-kate CM, Disch FJ, et al. Anatomical as-pects of sinus floor elevations. Clin OralImplants Res. 2000;11:256-265.
26. Jensen J, Sindet-Pedersen S, Ol-iver AJ. Varying treatment strategies for re-construction of maxillary atrophy withimplants: Results in 98 patients. J OralMaxillofac Surg. 1994;52:210-216.
28 MAXILLARY SINUS MEMBRANE REPAIR

27. Vlassis JM, Fugazzotto PA. A clas-sification system for sinus membrane per-forations during augmentation procedureswith options for repair [Review]. J Peri-odontol. 1999;70:692-699.
28. Fugazzotto PA, Vlassis J. A sim-plified classification and repair system forsinus membrane perforations. J Peri-odontol. 2003;74:1534-1441.
29. Aimetti M, Romagnoli R, Ricci G, etal. Maxillary sinus elevation: The effect ofmacrolacerations and microlacerations ofthe sinus membrane as determined by en-doscopy. Int J Periodontics RestorativeDent. 2001;21:581-589.
30. Proussaefs P, Lozada J, Kim J. Ef-fects of sealing the perforated sinus mem-brane with a resorbable collagenmembrane: A pilot study in humans. J OralImplantol. 2003;29:235-241.
31. Proussaefs P, Lozada J, Kim J, et al.Repair of the perforated sinus membranewith a resorbable collagen membrane: A hu-man study. Int J Oral Maxillofac Implants.2004;19:413-420.
32. Waldrop TC, Semba SE. Closure oforoantral communication using tissueguided tissue regeneration and an absorb-able gelatin membrane. J Periodontol.1993;64:1061-1066.
33. Sullivan SM, Bulard RA, MeadersR, et al. The use of fibrin adhesive in sinuslift procedures. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 1997;84:616-619.
34. Choi BH, Zhu SJ, Jung JH, et al.The use of autologous fibrin glue for clos-ing sinus membrane perforations during si-nus lifts. Oral Surg Oral Med Oral PatholOral Radiol Endod. 2006;101:150-154.
35. Choi BH, Kim BY, Huh JY, et al.Cyanoacrylate adhesive for closing sinusmembrane perforations during sinus lifts.J Craniomaxillofac Surg. 2006;34:505-509.
36. Shalom B, Horwitz I, Kahn A, et al.The effect of sinus membrane perforationand repair with Lambotte on the outcomeof maxillary sinus floor augmentation: A ra-diographic assessment. Int J Oral Maxillo-fac Implants. 2004;19:559-562.
37. Simunek A, Kopeck D, Carny M.The use of oxidized regenerated cellulose(surgical) in closing Schneiderian mem-brane tears during the sinus lift procedure.West Indian Med J. 2005;54:398-399.
38. Proussaefs P, Lozada J. The“Loma Linda pouch”: A technique for re-pairing the perforated sinus membrane. IntJ Periodontics Restorative Dent. 2003;23:593-597.
39. Steiner GG, Pearson JK, AinamoJ. Changes of the marginal periodontiumas a result of labial tooth movement inmonkeys. J Periodontal. 1988;52:314-320.
40. Wennstrom JL, Lindhe J, Sinclair F,et al. Some periodontal tissue reactions toorthodontic tooth movement in monkeys.J Clin Periodontol. 1987;14:121-129.
41. Wang HL, MacNeil RL, Shieh AT, etal. Utilization of a resorbable collagenmembrane in repairing gingival recessiondefects. Pract Periodontics Aesthet Dent.1996;8:441-448.
42. Postlewaite AE, Seyer JM, KangAH. Chemotactic attraction of human fi-broblasts for type I, II and III collagen andcollagen derived peptides. Proc Natl AcadSci USA. 1978;75:871-875.
43. Lowenberg BF, Aubin JE, DeporterDA. Attachment, migration, and orientationof human gingival fibroblasts to collagen-coated, surface-demineralized, and un-treated root slices. J Dent Res. 1985;64:1106-1110.
44. Steinberg AD, LeBreton G, WilleyR. Extravascular clot formation and plateletactivation on variously treated root sur-faces. J Periodontol. 1986;57:516-522.
Reprint request and correspondence to:Michael A. Pikos, DDSCoastal Jaw Surgery2711 Tampa roadPalm Harbor, FL 34684Phone: 727-786-1631Fax: 727-785-8477E-mail: [email protected]
Abstract Translations
GERMAN / DEUTSCHAUTOR: Michael A. Pikos, DDS. Schriftverkehr: MichaelA. Pikos, DDS, Coastal Jaw Surgery, 2711 Tampa road,Palm Harbor, FL 34684. Telefon: 727-786-1631, Fax: 727-785-8477. eMail: [email protected] der Oberkiefersinusmembran: Aktualisierungder Technik bei großen bzw. kompletten Perforationen
ZUSAMMENFASSUNG: Die Perforation der Oberkiefersi-nusmembran ist die am weitesten verbreitete Komplikation,die bei einem chirurgischen Eingriff zur Sinusanhebungund -anreicherung auftreten kann. Es wird eine Technikunter Anwendung einer langsam resorbierenden Kollagen-membran des Typs I zur Wiederherstellung großer undkompletter Sinusmembranperforationen beschrieben. DieBiokompatibilitat und halbfeste strukturelle Integritatdieser Membran zusammen mit einer externen Stiftbefes-tigung ermoglicht eine optimale Membranstabilisierungund -erhaltung.
SCHLUSSELWORTER: Sinusanhebung und -anreicherung, os-tiomeataler Komplex, Kollagenmembran, externe Befestigung
SPANISH / ESPAÑOLAUTOR: Michael A. Pikos, DDS. Correspondencia a: MichaelA. Pikos, DDS, Coastal Jaw Surgery, 2711 Tampa Road, PalmHarbor, FL 34684. Telefono: 727-786-1631, Fax: 727-785-8477. Correo electronico: [email protected] de la membrana del seno maxilar: Actualiza-cion de la tecnica para perforaciones completas ygrandes
ABSTRACTO: La perforacion de la membrana del seno es lacomplicacion mas comun que ocurre en la cirugıa para au-mentar la elevacion del seno. Se describe una tecnica que usauna membrana de colageno tipo I de lenta reabsorcion para lareparacion de perforaciones completas y grandes del senomaxilar. La biocompatibilidad e integridad estructuralsemirıgida de esta membrana, junto con la fijacion externa,permite una estabilizacion y mantenimiento optimo de lamembrana.
PALABRAS CLAVES: aumento de la elevacion del seno,complejo osteomeatal, membrana de colageno, fijacionexterna
IMPLANT DENTISTRY / VOLUME 17, NUMBER 1 2008 29

PORTUGUESE / PORTUGUÊSAUTOR: Michael A. Pikos, DDS. Correspondencia para:Michael A. Pikos, DDS, Coastal Jaw Surgery, 2711 Tamparoad, Palm Harbor, FL 34684. Telefone: 727-786-1631, Fax:727-785-8477. e-Mail: [email protected] da Membrana da Cavidade Maxilar: Atualizacao daTecnica para Perfuracoes Grandes e Completas
RESUMO: A perfuracao da membrana da cavidade maxilar ea complicacao mais comum que ocorre com a cirurgia deaumento da elevacao da cavidade. E descrita uma tecnicausando uma membrana tipo I reabsorvente lenta para reparode perfuracoes grandes e completas da membrana da cav-idade. A biocompatibilidade e a integridade estrutural semi-rıgida desta membrana, junto com a fixacao da tacha externa,permite otima estabilizacao e manutencao da membrana.
PALAVRAS-CHAVE: aumento da elevacao da cavidade,complexo ostiomeatal, membrana do colageno, fixacaoexterna
RUSSIAN /�����: Michael A. Pikos, ������ ����������.����� ��� ���������� : Michael A. Pikos, DDS,Coastal Jaw Surgery, 2711 Tampa road, Palm Harbor, FL34684. ������: 727-786-1631, ����: 727-785-8477.����� ��������� ���: [email protected]�������� � �������� � �� � ������ �-����: ���� �� ������� � ���, ���� � ������ ������� � ������� � �������
� !"# . � �������� ������� � ��� � ������������ — ����� ����� ���� ���� ������� �� , ������ ������� � ��� �� �� ���
��� �� ��� ������ ����� �� �� � � ��� � ������������. ������ � ��� ������������ � � ���� ������� ��� ��� ����� � ����� ���� I ����������� ��� !������ � ������ � � ��������� ��� � ������ �������. "������ �������� ����� ����� ����������� � �������� #���� ����� , � ���� �������� ���������� �� ������ ���������� ��������� � ������-����� �������.
$%"& �' (%���: �� �� �� ��� ����� ������ ����� �� �� � � ��� � ������ ������,������ ����� � ���� ��, ��� ����� � ������,�������� ��������.
TURKISH / TURKCEYAZAR: Diçs Hekimi Michael A. Pikos. Yazyþma icin: Mi-chael A. Pikos, DDS, Coastal Jaw Surgery, 2711 Tamparoad, Palm Harbor, FL 34684 ABD. Telefon: 727-786-1631,Faks: 727-785-8477, E-posta: [email protected] Sinus Membran Onarymy: Buyuk ve Tam Per-forasyonlar icin Teknik Guncellemesi
OZET: Maksiller sinus membranının perforasyonu, sinuselevasyon ogmantasyon cerrahisinde en yaygın gorulenkomplikasyondur. Bu calısma, buyuk ve tam sinus mem-bran perforasyonlarının onarımında yavas resorbe olan tipI kollajen membranının kullanıldıgı bir teknigi tarif etmek-tedir. Eksternal tack fiksasyonunun yanı sıra, bu membra-nın biyo-uyumlulugu ve yarı-rijid yapısal butunlugu, opti-mal duzeyde membran stabilizasyonu ve bakımı saglar.
ANAHTAR KELYMELER: sinus elevasyon ogmanta-syonu, ostiomeatal kompleks, kollajen membran, eksternalfiksasyon.
JAPANESE /
30 MAXILLARY SINUS MEMBRANE REPAIR

CHINESE /
KOREAN /
IMPLANT DENTISTRY / VOLUME 17, NUMBER 1 2008 31