Embed Size (px)
DESCRIPTION
A rare disorder with another rare congenital variant
Citation preview

Case 11853 Fahr's syndrome with congenital cavum variants
Muhammad Asim Rana , Ahmed F. Mady , Omar E. Ramadan , Intekhab Ahmed , Waleed T.1 1 1 1
Hashim , Abdulrehman Alharthy , Mostafa Yaseen , Tarik M. Alsaqat , Ahmed F. Farakha , Dina1 1 1 2 2
M. Khalil 2
King Saud Medical City, Riyadh Saudi Arabia
Neuroradiology Section: 2014, Jun. 13 Published:
19 year(s), malePatient:
Authors' Institution
1. King Saud Medical City, Riyadh Saudi Arabia
2. Prince Salman Hospital, Riyadh, Saudi Arabia
Email:[email protected]
Clinical History
Patient admitted via ER in status epilepticus developed cardio-respiratory arrest because of hypoxia,
15 minutes CPR done. History of abnormal movements started a few months ago and seizures for
the last two weeks. Family history of abnormal movements in brother who died five years ago
undiagnosed. No previous investigations available.
Imaging Findings
Non enhanced CT Brain showing extensive bilateral calcifications involving the basal ganglia,
thalami and subcortical white matter of both cerebral and cerebellar hemispheres in symmetric
fashion, compatible with Fahr's disease.
Cavum variants, "cavum septum pellucidum" and "cavum vergae" are also seen.
Infarct involving the right and left occipital lobes and right cerebellar hemisphere are seen. The area
of involvement corresponds to the posterior circulation territory.

No signs of intracranial hemorrhage are seen.
The ventricular size is prominent for the patient's age without any mid-line shift. Basal cisterns
appear normal. Mastoid air cells are sclerotic bilaterally.
Discussion
Fahr disease also called Idiopathic Basal Ganglia Calcification is a rare inherited disorder
characterized by abnormal deposits of calcium (carbonate and phosphate) in movement controlling
areas of the brain. First described by German neurologist Karl Theodor Fahr in 1930 [1]
Genetic heterogeneity is suggested in this disease[2] as latest research has identified a locus at
14q[3], second on chromosome 8[4] and third on chromosome 2[5]. A mutation in the gene
encoding the type 3 sodium dependent phosphate transporter 2 (SLC20A2) located on chromosome
8 has been reported suggesting that phosphate transport is involved.[6]
Basal ganglia calcification may occur in several other known conditions [7-10].
The disease usually manifests itself in 3rd to 5th decade but may appear earlier. It usually presents
with gait ataxia, slurred speech, involuntary movements, and seizures. Neuropsychiatric symptoms
range from changes in personality to psychosis and dementia[11].
Calcification commonly affects lenticular nucleus especially globuspallidus but caudate, dentae,
putamen, and thalami are also involved (Fig 1d, 2a). Sometimes it may predominate regions outside
the basal ganglia (See Fig2b, 2c). Classification seems to be progressive and can involve cerebellar
gyri, brain stem, and subcortical white matter (Fig 3b, 3c).
Diagnosis requires the following criteria:
1) Bi lateral basal ganglia calcification
2) Progressive neurologic dysfunction
3) Absence of an alternative cause (Metabolic, Infectious, Toxic, or Traumatic)
4) A positive family history consistent with autosomal dominant inheritance.
The diagnosis is usually made on CT scan but calcification may be visible on plain x-ray films of
the skull.
All these criteria were met in our case. The work up to search for an alternative cause including
investigations like calcium, phosphorus, magnesium, alkaline phosphatase, calcitonin and
parathyroid hormone were normal. The infarcts found in the CT were probably related to hypoxic
ischemic event i.e. long CPR.
There is currently neither a known cure nor a standard course of treatment for Fahr's Syndrome
except symptomatic control. Some data suggests that haloperidol or lithium carbonate may help
with psychotic symptoms [12] and some improvement was shown with bisphosphonate[13].
Genetic counseling may help to avoid passage of this disease in future generations.
The prognosis of this disease is variable and cannot be predicted easily because there is no reliable
correlation among age, extent of calcium deposits in the brain, and neurologic deficit. A CT scan
can be negative in a gene carrier.
Progressive neurological deterioration results in disability and death.
Additional incidental findings in our case were presence of cavum variants, cavum septum
pellucidum (Fig2b, 2c) and cavum vergae (Fig3a, 3b, 3c).
Final Diagnosis

Fahr's Syndrome with incidental finding of congenital cavum variants
Differential Diagnosis List
Idiopathic calcification as in aging, Toxic calcification as in lead poisoning and mineralizing
microangiopathy, Calcifications from infections like TORCH, CNS Tuberculosis, AIDS,
Neurocysticercosis, Inherited like mitochondrial diseases e.g. MELAS, Cockayne syndrome
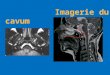
Figures
Figure 1 Fahr Syndrome
CT Scan Brain showing sclerotic air cells © Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Calcifications / Calculi;

Scattered calcifications and ischemic changes in posterior circulation area. © Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Calcifications / Calculi;
CT Brain (Plain) Bilateral calcifications including right basal ganglia involvement can beappreciated.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences;

Special Focus: Calcifications / Calculi;
Non enhanced CT Brain image showing bilateral basal ganglia and thalami calcifications.Ischemic changes in posterior circulation territory are also evident.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Calcifications / Calculi;
Figure 2 Fahr Syndrome and cavum variant cavum septum pellucidum
Non contrast enhanced CT Brain showing bilateral basal ganglia and frontal lobe

calcifications, changes typical of Fahr's disease. Additional finding of Cavum variant,"cavum septum pellucidum" can be appreciated.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Congenital;
Another axial cut of plain CT Brain with bilateral basal ganglia, thalami and frontal lobecalcifications. Cavum septum pellucidum can be identified more clearly.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Calcifications / Calculi;

Extensive bilateral calcification involving basal ganglia, thalami and subcortical whitematter.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Calcifications / Calculi;
Figure 3 Fahr Syndrome and cavum variant cavum vergae
Bilateral calcifications are evident in basal ganglia, thalami and cortex. Cavum variant,"cavum vergae" is seen.
© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia

Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Congenital;
Bilateral calcifications are evident in cortex. Cavum vergae can be seen. © Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Congenital;
Scattered calcifications are evident in cortex. Cavum vergae can be appreciated.

© Rana M. A. King Saud Medical City, Riyadh, Saudi Arabia
Area of Interest: Head and neck; Imaging Technique: CT;
Procedure: Imaging sequences; Special Focus: Congenital;
References
[1] Fahr, T. (1930) IdiopathischeVerkalkung der Hirngefässe ZentralblattfürallgemeinePathologie
und pathologische Anatomie 50: 129-133.
[2] 2) Oliveira JR, Spiteri E, Sobrido MJ, et al. (2004) Genetic heterogeneity in familial idiopathic
basal ganglia calcification (Fahr disease) Neurology Neurology63 (11): 2165-7.
[3] Geschwind DH, Loginov M, Stern JM (1999) Identification of a locus on chromosome 14q for
idiopathic basal ganglia calcification (Fahr disease) Am. J. Hum. Genet. 65(3):764-772.
[4] Dai X, Gao Y, Xu Z, et al. (2010) Identification of a novel genetic locus on chromosome
8p21.1-q11.23 for idiopathic basal ganglia calcification Am. J. Med. Genet. B
Neuropsychiatr.Genet. 153B (7): 1305-10.
[5] Volpato CB, De Grandi A, Buffone E, et al. (2009) 2q37 as a susceptibility locus for idiopathic
basal ganglia calcification (IBGC) in a large South Tyrolean family J. Mol. Neurosci. 39 (3):
346-53.
[6] Wang C, Li Y, Shi L, et al. (2012) Mutations in SLC20A2 link familial idiopathic basal ganglia
calcification with phosphate homeostasis Nat. Genet. 44 (3): 254-6.
[7] Niwa A, Naito Y, Kuzuhara S (2008) "Severe cerebral calcification in a case of LEOPARD
syndrome" Intern. Med. 47 (21): 1925-9.
[8] Preusser M, Kitzwoegerer M, Budka H, Brugger S (2007) Bilateral striopallidodentate
calcification (Fahr's syndrome) and multiple system atrophy in a patient with longstanding
hypoparathyroidism Neuropathology 27 (5): 453-6.
[9] Saito Y, Shibuya M, Hayashi M, et al. (2005) Cerebellopontine calcification: a new entity of
idiopathic intracranial calcification? ActaNeuropathol. 110 (1): 77-83.
[10] Tojyo K, Hattori T, Sekijima Y, Yoshida K, Ikeda S (2001) A case of idiopathic brain
calcification associated with dyschromatosissymmetricahereditaria, aplasia of dental root, and aortic
valve sclerosis RinshoShinkeigaku 41 (6): 299-305
[11] Chiu HF, Lam LC, Shum PP, Li KW (1993) Idiopathic calcification of the basal ganglia
Postgrad Med J. 69 (807): 68-70.
[12] Munir KM. (1986) The treatment of psychotic symptoms in Fahr's disease with lithium
carbonate J ClinPsychopharmacol. 6 (1): 36-8.
[13] Loeb JA (1998) Functional improvement in a patient with cerebral calcinosis using a
bisphosphonate Mov.Disord. 13 (2): 345-9.

Citation
Muhammad Asim Rana , Ahmed F. Mady , Omar E. Ramadan , Intekhab Ahmed , Waleed T.1 1 1 1
Hashim , Abdulrehman Alharthy , Mostafa Yaseen , Tarik M. Alsaqat , Ahmed F. Farakha , Dina1 1 1 2 2
M. Khalil (2014, Jun. 13) 2
Fahr's syndrome with congenital cavum variants {Online}URL: http://www.eurorad.org/case.php?id=11853