Embed Size (px)
Citation preview

BUDGETING EXECUTION - SLOVENIA
E VA H E L E N A Z V E R I N S T I T U T E O F M A C R O E C O N O M I C A N A LY S I S A N D D E V E L O P M E N T
D U S A N J O S A R
M I N I S T RY O F H E A LT H
2 N D H E A L T H S Y S T E M J O I N T N E T W O R K M E E T I N G F O R C E N T R A L , E A S T E R N A N D S O U T H E A S T E R N E U R O P E A N C O U N T I R E S – T H E F I N A N C I A L S T A B I L I T Y O F H E A L T H
S Y S T E M S – I M P R O V I N G D I A L O G : 1 - 2 D E C E M B E R 2 0 1 6 , T A L L I N N , E S T O N I A

Contents
1. Health financing system in Slovenia
2. Health budget formulation process
3. Health budget execution process
4. In-year changes in budget execution
5. Key methods used to reduce expenditure to the level of
expected revenues
6. Conclutions

Health financing system in Slovenia is based on social health insurance
Compulsory health insurance: Health Insurance Institute of Slovenia
(HIIS) is a single public insurer. All population is covered. In 2014 covered
68 % of CHE.
Voluntary complementary health insurance (VHI): It covers cost-sharing
levied on health services included in the benefits package. Covers more
than 95% of the population liable for co-payments. In 2014: 14,8 % of CHE
General taxation at national and local level: directly covers governance
of the health system, public health and prevention programmes. Only 3.3%
of CHE in 2014. Additional are transfers to HIIS to cover compulsory
insurance for specific groups of population and voluntary insurance for
socialy protected population.
Out-of-pocket payments: Only 12,4 % of CHE in 2014. Mainly spend for
and over-the-counter drugs and privately provided services

Nearly all HIIS resources come from social security contributions
66
68
70
72
74
76
78
80
82
Other socialsecuritycontributions
Self-employedcontributions
Employer andemployeecontributions

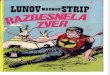
Because a large share of public resources come from payroll contributions, HIIS revenues are very
susceptible to labor market fluctuations
-4%
-2%
0%
2%
4%
6%
8%
10%
12%
14%
16%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Growth in Social Security Contributions to HIIS
Rate of unemployment by ILO in %
Gross wage per employee - real growth in %
Source: WHO, Observatory for health systems, MoH: Expenditure review, 2014

Health budget formulation process
HIIS prepares proposal of the Financial Plan with
max overall amount of expenditure for the upcoming year
Annual planning of
the national budget
HIIS and MoF establish cap for total
expenditure on health insurance
Financial Plan is approved
by the government
Financial Plan is discussed and
accepted by HIIS Board By the end of the year
for t+1

Health budget execution process
All partners negotiate about recommendations to amend or
change the existing GA (100% agreement among partner is
needed)
1. step:
2. step: Arbitration about controversial issues – if 100% agreement is
not reached then the government reaches the decision
Contracting providers: HIIS and each provider within the public health
network specify the type and volume of services, prices, methods of
payment, quality requirements and supervision.
Starts with partnership negotiations to define the General Agreement
(GA)

Partners in negotiations to define The General Agreement
The Ministry of Health,
HIIS,
Association of Health Institutions of Slovenia,
Medical Chamber, Pharmaceutical Chamber,
Association of Social Institutions of Slovenia,
Community of Organizations for Education of Special
Needs Children
Slovene Spas Association
VHI companies do not participate in the negotiation process to define the
GA, but they are obliged to pay providers the total value of benefits
covered by complementary VHI.

In-year changes: General Agreement is amended every year – ones, twice or even more times…
During the year any partner can propose changes to GA
All partners should agree on amendments 100%; if
not arbitration process starts again.
All amendments to GA should be taken into account in revised
Finacial Plan for current year
Flexibility: In-year budget
reallocations
Doesn‘t work well
If GA is not reached, the Government decides which
services, scope and prices have to be paid by the HIIS

Slow process leading to the GA
(and contracts) leads to uncertainty among actors
Generally, contracts are relatively unspecific
Effectiveness and/or cost-effectiveness is not taken into
account
Providers very frequently seek arbitration
Patient groups are not represented in the GA negotiation
Lacking control and monitoring systems.
Key challenges regarding purchasing process
Source: Analysis of Health Care System in Slovenia: WHO, Observatory, MoH
Performing: Programmed
but not output based
Doesn‘t work well
Timely
Doesn‘t work well

In-year changes: Almost every year HIIS Financial Plan is revised because of new level of estimated revenues
Since 2005 HIIS must respect ,fiscal rule‘. It has to be financed:
- without any borrowing from the central government and
- without increases in insurance contribution rates.
HIIS is responsible for monitoring the level of
revenues and expenditure and report to the MoF
and MoH with a delay up to max. 2 month!
HIIS Financial Plan for the current budgetary year is revised in
autoum according to new estimates of the flow of revenues by the
end of the budgetary year.
Accountability
and Sustainability:
Financial monitoring
system
Works very well

HIIS expenditures are constrained to revenues and reserves
-4.00%
-2.00%
.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Growth in revenues Growth in expenditures
Source: WHO, Observatory for health systems, MoH: Expenditure review, 2014

HIIS can record deficit only to the amount of accumulated reserves from previus years
-100,000,000
-80,000,000
-60,000,000
-40,000,000
-20,000,000
0
20,000,000
40,000,000
60,000,000
80,000,000
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Reserves Surplus / deficit
Source: WHO, Observatory for health systems, MoH: Expenditure review, 2014
HIIS cannot contribute to public debt!

Key methods used to reduce HIIS annual expenditure during the year
1) Changes in prices
Volumes are maintained while revenues decline
2) Changes in coinsurance
Costs shifted onto VHI without damaging access to
services
3) Delaying payments to providers
~150 million EUR in liabilities (2010-2013)

One of the key factors behind the slowdown in expenditures
has been the declining value of DRG points
1. Changes in prices

2. Changes in co-payment rates
95
105
115
125
135
2008 2009 2010 2011 2012 2013 2014Public expenditure Private health insurance
Households (OOP)
To maintain the volume of services one of the most flexible
measures was to increase co-payment rate;
Households were protected from higher OOP

3. HIIS delayed payments to providers to avoid deficit
When HIIS reserves fund was empty:
HIIS delayed payments to privders until the following year
150 million EUR in liabilities (2011-2013)
-4.00
-3.00
-2.00
-1.00
.00
1.00
2.00
3.00
4.00
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
In %
of to
tal h
ea
lth
exp
en
ditu
re
Deficit/Surplus and delayed playments to providers to avoid deficit
Delayed payment to providers
Deficit/Surplus

Consequences: lower prices for services and delayed payments burdened providers
…Ministry of Finance provided some loans to support providers…
Providers has to reduce costs and operate efficiently
Many hospitals suffered loss and their kumulative debt has incresed!

To conclude: How effective is health budget execution in Slovenia?
Predictable
Ad-hoc changes to budget are agreed between all partners; usually minimal – works well
Timely Delay in release of funds were often during the crisis
Flexible Flexibility – to some extent, but slowed down due complicated partnetship negotiations
Accountably Financial monitoring system works well – funds are spent on intended purpose
Sustainable Very strict – works well Expenditure cannot exceed the level of revenues and accumulated reserves
Performing Expenditures are not linked to ouputs