Embed Size (px)
Citation preview


Contents of chapter:-
1- definition2- anatomy of maxillary sinus.
3- histology of max. sinus.
4- function of max. sinus5- blood supply , innervation & lymphatic drainage.6- drainage of sinus.
7- enlargement of sinus.
8- relation between maxillary teeth , sinus.9- clinical consideration.

1- definition: it’s the largest bi-lateral air-containing cavity occupying the body of the maxilla , open into the nasal cavity by a single or multiple opening.N.B: maxillay sinus varies in size , shape & postion.

2- anatomy of maxillary sinus:- its described as a 4 sided pyramid . 1. base located medialy toward the nasal cavite.
2. apex directed laterally toward the body of zygomatic bone.
The walls of sinus (4 sided pyramid) are related to the surface of maxilla as follow.
1- anterior wall: to facial surface of Maxilla (region of canine , premolars). 2- posterior wall: to infra-temporal surface of maxilla. 3- inferior floor: to alveolar process , 1 mm below the level of floor of the nose. 4- superior roof: floor of orbit.

N.B: the floor of sinus is lateral to hard palate. Thus hard palate doesn’t enter into the formation of hard palate.

3- histology of maxillary sinus:- walls of sinus are lined by thin mucos membrane (epith. & C.T)
similar to respiratory type but thinner , continuous with that lining the nasal cavity.
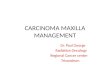
its composed of psedo-stratified columner ciliated epithelium, C.T layers which are separated from bone by peri-osteal layer. Thus its form muco-peri-ostium.
Goblet cells
Lamina propria
Epithelium
Mixed glands

A) Epithelial layer: * its pseudos-tratified columnar ciliated epithelium rich in goblet cells * its rested on nearly straight basement membrane..

Cilia site: at free end of most columnar cells.functions: drainage of sinus.structure: microtubules .
mechanism of action: provide motile apparatus of sinus epith. , they beat automatically in direction which move any substance from interior of the sinus toward the nasal cavity through its opening.
N.B: cilia beat automatically not under neural control

Goblet cells• Its uni-cellular gland which poures its secretion by rupturing of apical cell membrane which will aging regenerate , the secretion contains parts from apical cytoplasm , apical cell membrane.
• This cell looks like glass with stalk (apically: head of glass & basally stalk of glass)
swollen apical part: full of mucin
basal end: nucleus is situated

B) Lamina propria:
* consist of loose C.T , very few elastic fibers. Mixed glands
* its moderately vascular. * mixed glands. * its secretion reaches the sinus lumen through excretory ducts.
N.B: its separated from epith. Layer by nearly straight basement membrane & fused with peri-ostium of underlying bone.

4) Functions of maxillary sinus:-
1- warming , moistening of inhaled air.2- resonance of voice.3- producing bacterial lysozyme to nasal cavity.4- enhancement of facio-cranial growth (pneumatization)5- lightening of the skull.6- pressure danpening.7- increase olfactory surface area.8- heat insulation of the brain.9- assisting in regulation of intra-nasal pressure , serum gas
pressure.

5- blood supply , lymphatic drainage & innervation:-
1- blood supply: from nasal mucosa , osseous vasculature of
surrounding structure.
2- lymphatic drainage: lymph vessels pass through the infra-orbital foramen to the nasal cavity then into sub-mandibular lymphnode.
3- innervation: nerve supply is derived from branches from
maxillary division of trigeminal nerve

6- drainage of sinus:- * Maxillary sinus is drained to nasal cavity throught a
perforation into its base ( ostium maxillare ). * this opening located in lateral wall of nasal cavity in the middle meatus, between middle , inferior conchae
in concavity called (hiatus semilunaris) * this opening varies in size , postion & efficiency in draining the sinus * accessory ostium may occur in a lower level than the ostium maxillae , is slightly more advantageously placed for drainage.


HiatusSemilunaris


7- enlargement of sinus
Its enlarged by process of pneumatization. pneumatization: is a process of growth by bone resorption on
internal wall of sinus & bon deposition on outer surface of maxilla
Maxillary sinus extended to many processes : its extend 1. outward to zygomatic process. 2. inward , upward to frontal process. 3. downward to alveolar process.
When it extend downward into alveolar process ; the apices of the roots may appears protruded into the sinus.

8- relation between maxillary teeth , sinus:- * the teeth which in direct relation to the maxillary sinus is
vary from one individual to another according to the shape , size of sinus.
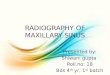
* the apices of the roots (specially palatal roots) of first , second molars are usually near to the floor of the sinus followed by second , first premolar & canine and third molar respectively.

Relationship of the floor of the sinus to the roots of the maxillary teeth

9- clinical consideration.
1- maxillary sinusitis of one side may cause pain in maxillary teeth of the same side (toothache) , may cause pain like pulp pain.
2- infection of teeth which are close to sinus may cause sunus infection.
3- extraction of first , second molars carry the greatest risk to formation of fistula (oro-antral comunication) & roots of these teeth may forced into the sinus.
4- A fractured root may be forced accidentally during surgical manipulation into the sinus if the bone is thin .
5-true sinus infection increase if the patient bends over , place head below the
knees.
6- sinus may be divided into parts which may interfere with drainage.

1. In pitutary gaintism all sinuses assum a much large volume than in healthy individuals .
2. Congenital infections (by spirochetes in congenital syphilis) the pneumatic processes are greatly suppressed, resulting in small sinuses .
3. Transfer of a pathologic condition from the sinus to the orodental apparatus , or vice versa by :
- Mechanical connection . - Way of the blood or lymphatic
pathways .

4. Surgical manipulation on upper 1st molar may damage the sinus (oroantral fistula) .
5. Extraction of hypercemetosed tooth may also lead to a perforation (radiograph should be considered before extraction) .
6. Chronic infections of mucoperiosteal layer of the sinus might involve superior alveolar nerves, and may neuralgia that mimics possible dental dental origin .

8. Due to vascular connection between the sinus and teeth by the superior alveolar vessels, bacterial sinusitis may be followed by some oral manifestation .
9. A fractured root may be forced accidentally during surgical manipulation into the sinus if the bone is thin .
10. Mlignant lesions of the sinus may produce their primary manifestation in the maxillary teeth (pain, loosening, supraeruption, or gingival bleeding) .

thanks