Embed Size (px)
DESCRIPTION
Citation preview

Dental Biochemistry 2 – (Lec. 2,3)
Heme and Hemoglobin

Introduction • Red blood cells (RBC) are biconcave discs, with a
diameter of about 7 microns.
• RBCs live for about 120 days in peripheral circulation.
• 100 ml blood contains about 14.5 g of Hb.
• Mature RBC is non-nucleated; have no mitochondria and does not contain TCA cycle enzymes.
• RBC formation in the bone marrow requires amino acids, iron, copper, folic acid, vitamin B12, vitamin C, pyridoxal phosphate, pantothenic acid and hemopoietin.

Red Blood Cells

Structure of Hemoglobin
• Hemoglobin is a conjugated protein having heme as the prosthetic group and the protein, the globin.
• It is a tetrameric protein with 4 subunits, each subunit having a prothetic heme group and the globin polypeptide.
• The polypeptide chains are usually two alpha and two beta chains.
• Hemoglobin has a molecular weight of about 67,000 Daltons.
• Each gram of Hb contains 3.4 mg of iron.


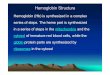
Structure of Heme
• Heme is a derivative of the porphyrin.
• Heme is produced by the combination of iron with a porphyrin ring.
• Since an atom of iron is present, heme is a ferroprotoporphyrin.
• Prophyrins are cyclic compounds formed by fusion of 4 pyrrole ring linked by methenyl (=CH-) bridges.
• The pyrrole rings are named as I,II,III,IV and the bridges as alpha, beta, gamma and delta. The possible areas of substitution are denoted as 1 to 8.

• Type III is the most predominant in biological systems.
• The usual substitution are:
a) Propionyl (-CH2-CH2-COOH) group
b) Acetyl (CH2-COOH) group
c) Methyl (-CH3) group
d) Vinyl (-CH=CH2) group

Porphyrin ring Structure of heme

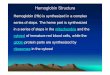
Heme molecule
Pyrrole-N H2O N-Pyrrole
↖ ↑ ↗
F
↙ ↓ ↘
Pyrrole-N N-Histidine N-Pyrrole
Fe

Biosynthesis of Heme
• Heme can be synthesized by almost all the tissues in the body.
• Heme is synthesized in the normoblasts, but not in the matured ones.
• The pathway is partly cytoplasmic and partly mitochondrial.

Catabolism of Heme
1. Generation of Bilirubin.
2. Transport to Liver.
3. Conjugation in liver.
4. Excretion of Bilirubin to Bile.
5. Fate of Conjugated Bilirubin in Intestine.
6. Enterohepatic Circulation.
7. Final Excretion.

1- Generation of bilirubin • The end product of heme catabolism are bile
pigments.
• The old RBCs breakdown, liberating the
hemoglobin.
• The iron liberated from heme is re-utilized.
• The porphyrin ring is broken down in
reticuloendothelial cells of liver, spleen and bone
marrow to bile pigments, mainly bilirubin.
• Approximately 35 mg of bilirubin is formed from 1
g of Hb.
• About 300 mg of bilirubin is formed every day.

Breakdown of heme

Production and excretion of bilirubin

2- Transport to liver
• The liver plays the central role in the further disposal of the bilirubin.
• Bilirubin is lipophilic so it transport in plasma bound to albumin.
• Albumin takes bilirubin in loose combination.
• So when present in excess, bilirubin can easily dissociate from albumin.

3- Conjugation in liver
• Liver takes up the bilirubin from the
transported complex.
• Inside the liver cell, the bilirubin is conjugated
with glucuronic acid, to make it water soluble,
mainly as bilirubin diglucuronide.
• Drugs like primaquine, chloramphenicol,
androgen may interfere in this conjugation
process and may cause jaundice.

4- Excreation of bilirubin to bile
• The water soluble conjugated bilirubin is
excreted into the bile by an active
process.
• This is the rate limiting step in the
catabolism of heme.
• It is induced by phenobarbitone.

5- Fate of conjugated bilirubin in
intestine
• The conjugated bilirubin reaches the intestine through
the bile.
• Intestinal bacteria deconjugate the conjugated bilirubin.
• This free bilirubin is further reduced to a colorless
tetrapyrrole urobilinogen (UBG).
• Further reduction of the vinyl substituent groups of
UBG leads to formation of mesobilinogen and
stercobilinogen (SBG).
• SBG is mostly excreted through feces (250-300
mg/day).

6- Enterohepatic circulation
• Twenty percent of the UBG is reabsorbed
from the intestine and returned to the liver
by portal blood.
• The UBG is again re-excreted (enterohepatic
circulation).
• Since the UBG is passed through blood, a
small fraction is excreted in urine (less than
4 mg/day).

7- Final excretion
• UBG and SBG are both colorless compound
but are oxidized to colored products,
urobilin or stercobilin respectively by
atmospheric oxidation.
• Both urobilin and stercobilin are present in
urine as well as in feces.

Plasma Bilirubin • Normal plasma bilirubin level ranges from 0.2-0.8
mg/dl. The unconjugated bilirubin is about 0.2-0.6 mg/dl, while conjugated bilirubin is only 0- 0.2.
• If the level of plasma bilirubin exceeds 1 mg/dl, the condition is called hyperbilirubinemia.
• Levels between 1 and 2 mg/dl are indicative of latent jaundice.
• When the bilirubin level exceeds 2 mg/dl, it diffuses into tissues producing yellowish discoloration of skin and mucous membrane resulting in jaundice.
• Van den Bergh test is a test for detection of bilirubin.

Hyperbilribunemias
• Depending on the nature of the bilirubin elevated, the condition may be grouped into conjugated or unconjugated hyperbilirubinemia.
• Based on the cause it may also be classified into congenital and acquired.

1- Congenital Hyperbilirubinemias
• They results from abnormal uptake, conjugation or excretion of bilirubin due to inherited defects.
Crigler-Najjar syndrome: Here the defect is in conjugation.
In type 1 (Congenital non-hemolytic jaundice), there is sever deficiency of UDP glucuronyl transferase.
The disease is often fatal and the children die before the age 2.
Jaundice usually appears within the first 24 hours of life.
Unconjugated bilirubin level increases to more than 20 mg/dl, and hence Kernicterus is resulted.

2- Acquired Hyperbilirubinemias
Physiological Jaundice:
It is also called as neonatal hyperbilirubinemia.
In all newborn infants after the second day of life, mild jaundice appears.
This transient hyperbilirubinemia is due to an accelerated rate of destruction of RBCs and also because of the immature hepatic system of conjugation of bilirubin.
In such cases, bilirubin does not increase above 5mg/dl.
It disappears by the second week of life.

3- Hemolytic Jaundice A) Hemolytic Disease of the Newborn:
This condition results from incompatibility between maternal and fetal blood groups.
Rh+ve fetus may produce antibodies in Rh-ve mother, leading to Rh incompatibility.
When blood level of bilirubin is more than 20mg/dl, the capacity of albumin to bind bilirubin is exceeded.
In young children before the age of 1 year, the blood-brain barrier is not fully matured, and therefore free bilirubin enters the brain (Kernicterus).
It is deposited in brain, leading to mental retardation.

B) Hemolytic Diseases of Adults:
This condition is seen in increased rate of hemolysis.
It usually occurs in adults.
The characteristic features are increase in unconjugated bilirubin in blood, absence of bilirubinuria and excessive excretion of UBG in urine and SBG in feces.
Common causes are:
1. Congenital spherocytosis.
2. Autoimmune hemolytic anemias.
3. Toxins like carbon tetrachloride.

4- Hepatocellular Jaundice
• The most common cause is viral hepatitis, caused by hepatitis viruses A, B, C, D, or G.
• Conjugation in liver is decreased and hence free bilirubin is increased in circulation.

5- Obstructive Jaundice
• Conjugated bilirubin is increased in blood, and it is excreted in urine.
• UBG will be decreased in urine or even absent.
• Since no pigment are entering into the gut, the feces become clay colored.
• The common causes are:
1. Intrahepatic cholestasis. This may be due to cirrhosis or hepatoma.
2. Extrahepatic obstruction. This may be due to stones in the gallbladder or biliary tract; carcinoma of head of pancreas.

Hemoglobin (HbA)
• Normal level of hemoglobin (Hb) in blood in males is 14-16g/dl and in female 13-15g/dl.
• Hemoglobin is globular in shape.
Function of hemoglobin • It carries oxygen from the lungs to the body
tissues and take carbon dioxide from the tissues to the lungs.

Transport of oxygen by hemoglobin Hemoglobin has all the requirements of an ideal respiratory pigment: - It can transport large quantities of oxygen. - It has great solubility. - It can take up and release oxygen at appropriate partial pressures. - It is a powerful buffer.

Oxygenation and oxidation
• When hemoglobin carries oxygen, the Hb is oxygenated. The iron atom in Hb is still in the ferrous state.
• Oxidized hemoglobin is called Met-Hb; then iron is in ferric state and the oxygen carrying capacity is lost.

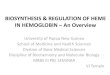
Oxygen Dissociation Curve (ODC)
• The ability of hemoglobin to load and unload oxygen at physiological pO2 (partial pressure of oxygen).
• At the oxygen tension in the pulmonary alveoli, the Hb is 97% saturated with oxygen. Normal blood with 15mg/dl of Hb can carry 20ml of O2/dl of blood.
• In the tissue capillaries, where the pO2 is only 40mm of Hg, the Hb is about 60% saturated. So physiologically, 40% of oxygen is released.


Oxygen Dissociation curve (ODC)

Transport of Carbon Dioxide
• At rest, about 200 ml of CO2 is produced per minute in tissues.
• The CO2 is carried by the following 3 ways:
1. Dissolved form.
2. Isohydric transport of carbon dioxide.
3. Carriage as Carbaminohemoglobin.

1. Dissolved Form:
• About 10% of CO2 is transported as dissolved form.
CO2 + H2O → H2CO3 → HCO3- + H+
• The hydrogen ions thus generated, are buffered by the buffer systems of plasma.

2. Isohydric Transport of Carbon Dioxide
• Isohydric transport constitutes about 75% of CO2. It means that there is minimum change in pH during the transport. The H+ ions are buffered by the deoxy-Hb and this is called the Haldane effect.
• In tissues:
• Inside tissues, pCO2 is high and carbonic acid is formed.
• It ionizes to H+ and HCO3- inside the RBCs.
• The H+ ions are buffered by deoxy-Hb and the HCO3- diffuses out into the plasma.
• Thus the CO2 is transported from tissues to lungs, as plasma bicarbonate, without significant lowering of pH.
• The H+ are bound by N-terminal NH2 groups and also by the imidazole groups of histidine residues.

• Oxy-Hb is more negatively charged than deoxy-Hb:
• The iso-electric point of oxy-hemoglobin is 6.6, while that of deoxy-Hb is 6.8.
• Thus, oxy-Hb is more negatively charged than deoxy-Hb.
• The reaction in tissues may be written as:
• OxyHb= + H+ → HHb- + O2
• Therefore some cation is required to remove the extra negative charge of Oxy-Hb.
• So H+ are trapped.
• 1 millimol of deoxy-Hb can take up 0.6 mEq of H+.

• In the lung:
• In lung capillaries, where the pO2 is high, oxygenation of hemoglobin occurs.
• When 4 molecules of O2 are bound and one molecule of hemoglobin is fully oxygenated, hydrogen ions are released.
• H-Hb + 4O2 → Hb(O2) + H+
• The protons released in the RBC combine with HCO3
- forming H2CO3 which would dissociate to CO2, that is expelled through pulmonary capillaries.

3. Carriage as carbaminohemoglobin
• The rest 15% of CO2 is carried as carbamino-hemoglobin, without much change in pH.
• A fraction of CO2 that enters into the red cell is bound to Hb as a carbamino complex.
• R-NH2 + CO2 → R-NH-COOH
• The N-terminal amino group (valine) of each globin chain forms carbamino complex with carbon dioxide.

Fetal Hemoglobin (HbF) 1. HbF has 2 alpha chains and 2 gamma chains.
Gamma chain has 146 amino acids.
2. The differences in physicochemical properties when compared with HbA are:
• Increase solubility of deoxy HbF.
• Slower electrophoretic mobility.
• Increase resistance of HbF to alkali denaturation.
• Decreased interaction with 2,3-BPG (2,3-Bisphosphoglycerate).

3. The ODC of fetus and newborn are shifted to left.
• This increase in O2 affinity is physiologically advantageous in facilitating trans placental oxygen transport.
• The major reason is the diminished binding of 2,3-BPG to HbF.
• When pO2 is 20mmHg, the HbF is 50% saturated.
4. At birth, 80% of Hb is HbF. During the first 6 months of life, it decreases to about 5% of total.

2,3-Bisphosphoglycerate or 2,3-diphosphoglycerate
• 2,3-BPG is present in human red blood cells (RBC; erythrocyte) at approximately 5 mmol/L. It binds with greater affinity to deoxygenated hemoglobin (e.g. when the red cell is near respiring tissue) than it does to oxygenated hemoglobin (e.g., in the lungs) due to spatial changes