Embed Size (px)
Citation preview

Digestive System Digestive System PhysiologyPhysiology

The digestive system is formed of
1. Alimentary canal 2. Digestive glands


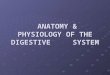
Mucosa submucosa circular m layer longtudinal m layer serosa
Structure of alimentary canalStructure of alimentary canal

Gastrointestinal wall

Types of movement of GITPeristalsisStretch →circular contraction behind & relaxation in frontStretch → serotonin sensory nerves → myenteric plexus -Retrograde cholinergic neurons (subs P & a.ch) → contraction -Antegrade cholinergic neurons (VIP, NO & ATP) → relaxationMixing movement•Peristaltic wave in blocked sphincter•Constrictive movement

Innervation of the GIT 1. Intrinsic innervation: Enteric
Nervous System.
2. Extrinsic innervation: Parasympathetic and sympathetic innervations.

Myenteric plexus (Auerbach's plexus).
Submucous plexus (Meissner's plexus).
Enteric nervous systemEnteric nervous system

Submucous plexus Myenteric plexus
between the circular layer and the mucosa.
between the outer longitudinal and inner circular muscle layers
Exocrine and endocrine functions of the GIT
Motor function of the GIT
Mainly excitatory, some inhibitory
Enteric nervous systemEnteric nervous system



The plexuses are interconnected.
They contain motor neurons; secretory neurons; sensory neurons that respond to stretch, tonicity, glucose, or amino acids; and interneurons.
Substances secreted by the ENS: acetylcholine, serotonin, GABA, and vasoactive intestinal peptide.

2. Extrinsic Innervation: Parasympathetic:
Cranial (Abdominal viscera)Preganglionic : vagusRelay: terminal ganglia on the wall of the visceraPostganglionic : in the myenteric and submucosal plexus
Sacral:2nd , 3rd , 4th (pelvic viscera)Preganglionic : pelvic nerves. Relay: terminal ganglia on the wall of the visceraPostganglionic ends on : in the myenteric and submucosal plexusIncrease in the activity of
ENS


2. Extrinsic Innervation: Sympathetic:
(Abdominal viscera)Preganglionic : lower 6th thoracicRun as greater splanchnic nerve.Relay: coeliac and superior mesenteric ganglia Postganglionic: pass with blood vessels to all parts of the gut
(Pelvic viscera)Preganglionic : T12 , L1, 2, 3. Run as lesser splanchnic nerve.Relay: inferior mesenteric ganglia Postganglionic: pass with blood vessels to all parts of the gutInhibition of GIT function: directly
Inhibition of enteric nervous system

Regulation of the GIT1. Nervous control of GIT: Reflexes that occur inside the ENS: self
regulation (local enteric reflexes)
Reflexes from the gut to symp ganglia then back to GIT (enterogastric reflex)
Reflexes from the gut to parasymp n. in BS or sc back to GIT (conditioned and unconditioned reflexes).

2. Hormonal control:Polypeptides secreted by APUD cells (amine precursors uptake and decarboxylation).
Hormones fall into one of 2 families: Gastrin family: the primary members of which are gastrin and cholecystokinin (CCK).
Secretin family: the primary members of which are secretin, glucagon, VIP, and gastrin inhibitory polypeptide (GIP).
Others: motilin and somatostatin

Mastication (Chewing)Mastication (Chewing)
•Mechanical breakdown of large food particles into smaller ones in the mouth.
•Increase exposed surface area to enzymes and help swallowing.

Center: pons Mastication muscles: motor branch of trigeminal. May be voluntary or involuntary (autonomic
reflex)
Mastication (Chewing)Mastication (Chewing)

Swallowing (Deglutition)Swallowing (Deglutition)
•Propelling of food from mouth to stomach through pharynx and oseophagus

Salivary Secretion
Saliva is secreted primarily by three pairs of glands:
1. the parotid glands: 20%
2. the submandibular: 75%.
3. the sublingual glands: 5%.
4. many small buccal glands in mouth cavity.


99.5% water0.5% Solids: a. organic: K+, Na+, HCO-
3, Cl-, Na2HPO4.
b.Organic: Ptyalin enzyme Mucin Lysozymes Immunoglobulin A
Composition of saliva: Composition of saliva: 1500ml/day 1500ml/day

Salivary Secretion Saliva•800- 1500 ml/day with proteins & electrolytes•pH→ 6- 7.0 ( 8.0 during active secretion)•Hypotonic ( Na+ & Cl- less , K+ & HCO3 more than plasma•Contains IgA, lysozyme, lactoferrin, mucin prolin rich proteins

The parotid glands acini are serous.
The sublingual glands acini are mucous.
The submandibular glands acini are mixed.
The buccal glands secrete only mucous.
Types of Salivary glands:Types of Salivary glands:


Stages of Salivary Secretion:
I-Primary secretion in the acini: contains ptyalin and/or mucin in a solution of ions which shows no great difference from extracellular fluid.
II- Modification of Primary secretion in the ducts: the following occur under effect of aldosterone.Sodium ions (Na+) are actively reabsorbed. Potassium ions (K+) are actively secreted. Sodium reabsorption is higher than potassium secretion in the salivary ducts Chloride ions (Cl-) to be passively reabsorbed. Therefore, the sodium ion and chloride ion concentrations of the saliva are markedly reduced whereas the potassium ion concentration becomes increased during passage through the ducts.


Bicarbonate ions (HCO3-) are actively secreted into the lumen of the duct.
The ducts are relatively impermeable to water. Therefore, the saliva that reaches the mouth is hypotonic and alkaline (pH= 8.0).

Salivary secretion

Functions of Saliva:
Protection of oral mucosa: Cooling hot foods. Neutralizing acid. Lysozyme attacks the walls of bacteria. Antibodies (immune globulin IgA) destroy
oral pathogenic bacteria.

Teeth protection: The buffers in saliva: bicarbonate, phosphate buffers,
mucin, help to keep the oral pH at about 7.0. At this pH, the saliva is saturated with calcium and so the teeth do not lose calcium. Loss of Ca2+ from the teeth enamel leads to dental caries.
Digestion: Saliva contains the digestive enzyme ptyalin
(salivary α-amylase) that digests starch into disaccharides.

Lubrication and Wetting: Swallowing: Saliva contains mucin
(glycoproteins) that lubricates the food
Speech: Keeping mouth moist facilitates movements of the lips and tongue during speech.
Taste: Saliva acts as (a solvent for the molecules that stimulate taste receptors.

Innervation of salivary glands
Parasympathetic efferentIncrease secretion & VD ( Ach & VIP)Sublingual & submandibular glands
Superior salivary nucleus →facial ( corda tympani) Parotid gland
Inferior salivary nucleus → glossopharyngeal nerve

Sympathetic efferentSmall amount of saliva rich in organic constituents- VC
Superior & inferior salivary nuclei → T 1 & 2 → superior cervical ganglion → all salivary glands
Both sympathetic & parasympathetic are complementary in salivary secretion

Submandibular and sublingual
Parotid gland
Superior salivary nucleus in medulla
inferior salivary nucleus in medulla
Preganglionic fibers arise
Chorda tympani (facial)
Glossopharyngeal n.
Run as
Submandibular ganglon
Otic ganglion relay
Supply Submandibular and sublingual
gland
Supply parotid gland
Postganglionic fibers
Innervation of salivary glands:Innervation of salivary glands: parasympathetic fibers parasympathetic fibers



Sympathetic efferent fibres: Preganglionic fibres arise from the lateral horn cells of
the upper 2 thoracic segments of the spinal cord. They relay in the superior cervical ganglion.
Postganglionic fibres arising from this ganglion reach all the salivary glands along the wall of their blood vessels.
Stimulation of the sympathetic nerve supply to the salivary glands causes vasoconstriction, and secretion of a small amount of saliva rich in mucin.

Control of Salivary secretion:
Stimulation of salivary secretion is entirely under neural control in response to conditioned or unconditioned stimuli.

Unconditioned reflexes:
Mechanical and chemical stimulation of taste buds in mouth causes reflex secretion of large amount of watery saliva:

Conditioned reflexes: Salivary secretion is easily conditioned as
shown in Pavlov's original experiment. Sight, smell, hearing, preparation of food, or even thinking of food, result in reflex increase in the secretion of saliva. The impulses arrive to the salivary nuclei from the cerebral cortex, in response to any conditioned stimulus.

Swallowing (Deglutition)Swallowing (Deglutition)
•Buccal (oral phase)
•Pharyngeal phase
•Oesophageal phase.Involuntary
Voluntary



Tongue is elevated upwards and Tongue is elevated upwards and backwards with bolus of food on its backwards with bolus of food on its dorsum. dorsum.
Bolus of food is rolled backwards to Bolus of food is rolled backwards to back of tongue.back of tongue.
Bolus is forced to pharynx by Bolus is forced to pharynx by contraction of mylohyoid muscle.contraction of mylohyoid muscle.
Buccal phaseBuccal phase

Receptor: Receptor: swallowing receptor area swallowing receptor area on the tonsillar pillars at the on the tonsillar pillars at the oropharyngeal junction.oropharyngeal junction.
Afferent: Afferent: glossopharyngeal nerve.glossopharyngeal nerve. Centre: Centre: swallowing centre in swallowing centre in
medulla and lower pons.medulla and lower pons. Efferent: Efferent: 55thth , 9 , 9thth , 10 , 10thth , 12 , 12thth nerves. nerves.
Pharyngeal phasePharyngeal phase

Actions:Actions:1.Rapid peristaltic 1.Rapid peristaltic wave: wave: cont. of cont. of superior, middle & superior, middle & inferior inferior pharyngeal pharyngeal muscles.muscles.
Pharyngeal phasePharyngeal phase

Actions:Actions:2. Protective reflexes: 2. Protective reflexes: Nose: elevation of soft palateNose: elevation of soft palate Mouth: elevation of tongue, cont. of Mouth: elevation of tongue, cont. of
myelohyoid muscle.myelohyoid muscle. Larynx: elevation of larynx to be covered by Larynx: elevation of larynx to be covered by
epiglottis, inhibition of respiration.epiglottis, inhibition of respiration.
Pharyngeal phasePharyngeal phase

Actions:Actions:3. Relaxation of pharyngeoesophageal 3. Relaxation of pharyngeoesophageal sphinctersphincter
Opening way for bolus of food to Opening way for bolus of food to oesophagusoesophagus
Pharyngeal phasePharyngeal phase

Swallowing ( deglutition) Oral voluntary stageFood is rolled posteriorly by pressure of tongue upward
Pharyngeal stage ( involuntary)Soft palate close nares , vocal cords approximate
Epiglottis close larynx, upper esophageal sphincter relaxes, pharynx contract( peristalsis) -respiration stops
Esophageal stage ( involuntary)Primary peristalsis→ pharynx to stomach
Secondary peristalsis from distention of esophagus by food ( enteric nervous system & vago-vagal reflex)



Peristaltic waves:Peristaltic waves:1. 1ry peristaltic wave:1. 1ry peristaltic wave:Continuation of peristaltic wave in Continuation of peristaltic wave in pharynx.pharynx.Start in upper part of oesophagus and Start in upper part of oesophagus and travels whole length in 9 sec. travels whole length in 9 sec.
Oseophageal phaseOseophageal phase
If failedIf failed
2ry peristaltic 2ry peristaltic wavewave

Peristaltic waves:Peristaltic waves:2. 2ry peristaltic wave:2. 2ry peristaltic wave:As a result of distension of oesophagus As a result of distension of oesophagus by retained food (bolus).by retained food (bolus).
A 2ry wave at site of bolus empty A 2ry wave at site of bolus empty all contents into the stomachall contents into the stomach..
Oseophageal phaseOseophageal phase

Upper half of oesophagus: Upper half of oesophagus: vagovagal reflex.vagovagal reflex.
Bilateral vagotomy: ???Bilateral vagotomy: ???
Lower half of oesophagus: local Lower half of oesophagus: local reflex.reflex.
Control of oseophageal phaseControl of oseophageal phase

Oesophageal musclesOesophageal muscles

Lower Esophageal Sphincter LES• Remains tonically contracted• Receptive relaxation (relaxes LES ahead of
peristaltic waves) → easy propulsion• Between meals LES prevent reflux of gastric
content into esophagus• Tone of LES
Ach→ contraction of LES
NO & VIP → relax LES • ↓ tone of LES → gastro esophageal reflux

It is a physiological sphincter at the It is a physiological sphincter at the lower end of oesophagus. lower end of oesophagus.
Tonically contracted to prevent Tonically contracted to prevent regurgitation of acidic gastric regurgitation of acidic gastric contents to oesophagus. contents to oesophagus.
During swallowing, it relaxesDuring swallowing, it relaxes
Lower Oesophageal sphincter Lower Oesophageal sphincter (LES)(LES)

StomachStomach

Stomach
Functional anatomy

- Parietal cells secret HCl & intrinsic factor- Cheif cells secret pepsinogen- Entero-Chromafin-Like cellssecret histamin-mucous cells

Fundus Fundus Body Body Antrum Antrum PylorusPylorus
Stomach is divided Stomach is divided anatomicallyanatomically

Cardia
Lesser curvature
Duodenum
Pylorus
Esophagus Fundus
Body
Greater curvature
Antrum

Function of the StomachFunction of the Stomach
1.Motor function of stomach
2.Secretory function of stomach


Secretory function of stomachSecretory function of stomach
Gastric gland

H2OH2O Ions: Ions: HH++, Cl, Cl--, Na, Na++, K, K++
Enzymes: Enzymes: pepsin, gelatinase, pepsin, gelatinase, lipaselipase
MucousMucous Intrinsic factorIntrinsic factor
Composition of acid secretionComposition of acid secretion

Acid secretionAcid secretion
H2O
OH-
H2O
1
2
3
5
46 7
8

Acid secretionAcid secretion
1
2


Functions of HCl• Killing bacteria• Dissolve food into chyme• Activate pepsinogen• Iron & calcium absorption• Stimulate secretin hormone & bile flow

Stimuli of HCl secretion:• Histamine: acts via H2 receptors
increases intracellular cAMP.• Acetylcholine: acts via M3 muscarinic
receptors increases intracellular Ca++.• Gastrin: it acts either directly on
oxyntic cells by increasing intracellular Ca++ (like acetylcholine) or indirectly through stimulating the secretion of histamine from enterochromaffin-like cells (ECL cells).

Mechanism of action of HCl stimuli:•Parietal cells contain receptors for these stimuli. Binding of these stimuli with their receptors release 2nd messengers which transfer the H+/K+ ATPase proteins from the membranes of intracellular vesicles to the plasma membrane thus increasing the number of pump proteins in the plasma membranes.


Acetyl choline.Acetyl choline.
Gastrin hormone.Gastrin hormone.
HistamineHistamine.
Stimulation of acid secretionStimulation of acid secretion

Phases of gastric secretionPhases of gastric secretionCephalic phase ( nervous)- Condition & unconditioned reflexes → vagus nerve → acetylcholine & gastrin → ↑HCl, pepsinogen & mucous ( one third of secretion)
Gastric phase ( nervous & hormonal) 2/3 of secretionLong vagovagal reflexesLocal enteric relexesGastrin secretion
Intestinal inhibitory phase ( nervous & hormonal) Presence of food in intestine → entero gastric reflex & secretion of GIP, VIP, CCK & secretin which inhibit secretion

Cephalic phase: (nervous):Cephalic phase: (nervous):Conditioned & unconditionedConditioned & unconditionedGastric phase: (nervous and hormonal):Gastric phase: (nervous and hormonal):Vagovegal reflexVagovegal reflexLocal enteric reflexesLocal enteric reflexesGastrin mechanismsGastrin mechanismsIntestinal phase: (nervous and Intestinal phase: (nervous and hormonal):hormonal): Entergastric reflexEntergastric reflexHormones: GIP, VIP, CCK, secretinHormones: GIP, VIP, CCK, secretin
Regulation of acid secretionRegulation of acid secretion

Gastric motility Physiologically- based the stomach is
divided into- Proximal motor unit ( fundus & body)
responsible for storage of food ( receptive relaxation)
- Distal motor unit ( antrum & pylorus) responsible for • mixing & partial digestion of food• gastric peristaltic waves & emptying food

1- storage function of stomach ( receptive relaxation)Gastric distention → relaxation of stomach to increase capacity to 1- 1.5 L from 50 ml ( efferent fibers in vagus, sympathetic & ENS)2- Mixing & propulsion of foodGastric slow waves start at mid point of greater curvature ( 3-5 cycles/min) → spiks →peristaltic waves → contraction of antrum followed by pyloric region & duodenum3- stomach emptying


Regulation of gastric evacuation1- gastric factors
Distention of stomach & gastrin hormone →increase gastric emptying2- intestinal factorsEnterogastric relex ( acid, irritation, distention, fats & proteins → inhibit gastric emptyingFat in duodenum → CCK, GIP & secretin → inhibit gastric emptying3- Liquids are evacuated more rapidly, carbohydrates more than fats or proteins4- Pain inhibits & emotions increase or decrease gastric emptying

Proximal motor unit:Proximal motor unit: fundus body fundus body
Distal motor unit: Distal motor unit: Antrum Antrum PylorusPylorus
Stomach is divided Stomach is divided physiologicallyphysiologically

Innervation of the Stomachnnervation of the Stomach 1. Parasympathetic (vagus nerve):
Cholinergic excitatory fibers
•Distal motor unit
Purinergic inhibitory fibers
• Proximal motor unit

Innervation of the Stomachnnervation of the Stomach2. Sympathetic Fibers: Origin: Lower 6th thoracic segments
Preganglionic: greater splanchnic nerve.
Relay in: Celiac ganglion
Postganglionic: pass to stomach to inhibit PMU

1.Motor function of stomach1.Motor function of stomach
Storage of food.
Mixing and partial digestion of food to form chyme.
Slow empting of the chyme into duodenum.

1.Motor function of stomach1.Motor function of stomachStorage of food (receptive relaxation):
Reflex initiated by the arrival of food into the stomach to increase its capacity for food.
50ml 1-1.5L (So stomach bulge outwards while pressure remains low).

Storage of food (receptive relaxation):Storage of food (receptive relaxation):
Gastric distension.
Afferent fibers
Vagal nucleus Sympathetic ganglia
Local enteric plexus
Purinergic vagal fibers
Myenteric inhibitory
fibersAdrenergic
sympathetic

Motor function of stomachMotor function of stomach2. Mixing of food and empting of stomach:
Weak peristaltic wave start in the middle of the body towards pylorus (stronger and faster at pyloric antrm).
Antral contents to be forced back to the proximal part leads to mixing of food

Motor function of stomachMotor function of stomach2. Mixing of food and empting of stomach:
Antrum, pylorus and upper duodenum function as one unit contraction of antrum followed by contraction of pylorus and duodenum gastric contents prevented from entering duodenum but mixed and crushed.

Motor function of stomachMotor function of stomach2. Mixing of food and empting of stomach:
Strong peristaltic wave
at pylorus (pyloric pump)
Tonic contraction of
pyloric sphincter
Slow gastric emptingSlow gastric empting

Motor function of stomachMotor function of stomach
Factors affecting gastric empting:
1.Gastric factors:Gastric distension Gastric
empting ( ++ Pyloric pump , -- pyloric
sphincter) Nervous reflexes Gastrin hormone

Motor function of stomachMotor function of stomach
Factors affecting gastric empting:
2. Intestinal factors (entergastric reflex):
Presence of the following factors inhibits gastric empting (-- pyloric pump, cont. pyloric sphincter):
fats and proteins. Increased pH. Distension of duodenum.

Entergastric reflexEntergastric reflex
Fats and proteins.Increased pH.Distension of duodenum.
Afferent fibers
Vagal nucleus
Sympathetic ganglia
Purinergic vagal fibers
Adrenergic sympathetic
SecretinCCKGIP
SecretinCCKGIP

Motor function of stomachMotor function of stomach
Factors affecting gastric empting:
3.Consistency of food: Liquids > solids

VomitingReflex abnormal emptying of gastric content through esophagus & mouth
Causes of vomiting1.Reflex → mechanical stimulation of posterior tongue – irritation of gastric mucosa- intestinal obstruction- sever pain – coronary thrombosis
2.central →stimulation of CTZ by drugs, hypoxia, acidosis, morning sickness of pregnancy & motion sickness

Mechanism of vomiting- Relaxation of stomach & LES – contraction of pyloric sphincter- Deep inspiration , strong contraction of diaphragm& abdominal muscles to increase intra-abdominal P →squeeze the contents of stomach up- Protection of air passages

Pancreatic secretion
It is the most important digestive juice because it contains enzymes for digestion of most of food stuffs• Volume → 1500 ml / day• pH → 8-8.3, Alkaline ( HCO3)
• Pancreatic Digestive enzymes

Pancreatic Digestive enzymes1. Proteolytic enzymes trypsin, chymotrypsin, carboxypeptidase, ribonuclease & deoxyribonuclease2. Pancreatic amylase3- Pancreatic lipase. 4- cholesterol esterase5- phospholipase


Regulation of pancreatic secretionNervous regulationVagal stimulation (conditioned &unconditioned reflex) → acetyl choline → pancreatic enzymesHormonal regulationSecretinAcid in intestine → secretin → pancreatic juice rich in HCO3 Cholecystokinin CCKPolypeptides, amino acids & fats → CCK → pancreatic juice rich in enzymes


Liver & Biliary system

Functions of the liverLiver acts as a chemical factory, an excretory system, an exocrine and an endocrine gland
1- Vascular Functions for Storage and Filtration of Blood:store 200-400 ml. of bloodKupffer cells(remove 90% of bacteria in the portal venous blood (the colon bacilli)

2- Metabolic Functions: Carbohydrate metabolism: (glucostat" )Glycogenesis- glycogenolysis- gluconeogenesis- Cori cycle ( formation of glycogen from lactic acid)
Lipid metabolism:oxidation of fatty acids - Formation of lipoproteins - lipogenesis
Protein metabolism:Deamination of amino acids - Formation of urea , plasma proteins, most of coagulation factors & non-essential amino acids
Storage of vitamins: Such as vitamin A, D, E, K and B12. & iron Detoxification or excretion of drugs, hormones and other substances

3- Secretory and excretory functions: Formation of bile:• Bile is required for the digestion and absorption of fats ( bile salts) and for the excretion of water-insoluble substances such as cholesterol and bilirubin• Secretion is continuous through all the day & is stored in gall bladder

Composition of bile
• 500-1500 ml/day• Fresh bile is alkaline• Becomes acidic during storage in gall
bladder to prevent precipitation of calcium

Water 97.00 %
Bile salts 0.70 %
Bile pigments 0.20 %
Cholesterol 0.06 %
Inorganic
salts
0.70 %
Fatty acids 0.15 %
Lecithin 0.10 %
Fat 0.10 %

Bile salts•
sodium and potassium salts of bile acids conjugated to glycine or taurine ( glycocholic & taurocholic acids)- The bile acids are synthesized from cholesterol.•
– Primary bile acids: cholic acid and chenodeoxycholic acid.•
– Secondary bile acids:In the colon, bacteria convert cholic acid to deoxycholic acid and chenodeoxycholic acid to lithocholic acid.

Function of bile salts1- Digestion of fata-activation of pancreatic lipaseb- emulsification of fat preparatory to its digestion and absorption by - detergent action → reduce surface tension between fat globules - hydrotropic action

2-Absorption of fat & fat soluble vitamins- form micellesmicelles are bile acid-lipid water-soluble complexes that play an important role in keeping lipids in solution and transporting them to the brush border of the intestinal epithelial cells, where they are absorbed.

Phospholipids
Free fatty acids, cholesterol
Bile acidsBile acids
OH group
Peptide bond
Carboxyl group


The Gallbladder
Functions of the Gallbladder:Storage of BileConcentration of Bile removal of sodium by the gallbladder mucosa through an active transport mechanism, which passively draws chloride, bicarbonate and water.Prevention of marked rise in the Intrabiliary pressureSecretion of white bile Acidification of Bile: (absorption of bicarbonate)

Control of Gallbladder Emptying = Cholagogues
Cholecytokinin (CCK)major stimulus for gallbladder contraction and sphincter of Oddi relaxation.Vagal stimulationcephalic stage of digestion and vago-vagal reflex during the gastric phase of digestion

Types of movement of GITPeristalsisStretch →circular contraction behind & relaxation in frontStretch → serotonin sensory nerves → myenteric plexus -Retrograde cholinergic neurons (subs P & a.ch) → contraction -Antegrade cholinergic neurons (VIP, NO & ATP) → relaxationMixing movement•Peristaltic wave in blocked sphincter•Constrictive movement


Movement of small intestineSegmentation movements & peristalsis help mixing & propagation of the contents down the intestine
1- Segmentation ( mixing) contractionsDivide the chyme, increase blood &lymph fow & mix food with secretion
Duodenum & jejunum → 12/min
Ileum → 8-9/min
Controlled by slow wave ( basic electrical rhythm – myenteric nerve plexus)


2- Peristalsis • Faster in proximal part & slower in distal part• Progression of the chyme 1-2 cm/min ( 3-5hr for
travel from pylorus to ileocecal valve)
Stretch → contraction behind → (subs P & a.ch) & relaxation in front→ VIP, NO & ATP• Increased after meal by stretch of duodenum, gastro enteric reflex & hormones (gastrin- CCK-insulin• Inhibited by secretin & glucagone

Thank Thank
youyou