Embed Size (px)
Citation preview

Chest Pain Scenario

The Dispatch
• You are dispatched to a bridal store for a 50 y/o female patient with chest discomfort. After
determining that the scene is safe, you enter and find your patient sitting on a sofa, complaining of
slight discomfort in her chest. She and her daughter have been looking a wedding dresses all
day
Next

General Impression
• She presents conscious, breathing, has a slightly irregular pulse with pale and clammy skin, but does not seem to be in any acute distress
• What is you transport decision?
Load and Go Stay and PlayChoose your Answer

Are you Sure??
• This patient is not that sick, but has the potential to become sicker. You can safely take the time to perform an more thorough
assessment
Next

Yes, that’s the right choice
• CORRECT. This patient is sick, but not at risk of dying if you stay and continue your assessment.
Continue

Your assessment
• LOC: responsive• CC: slight chest discomfort• Airway open and patent• Breathing 22 BPM, symmetrical chest rise and fall• Circulation radial pulse present• Skin pale and clammy
While your partner obtains Vital signs, What should you do next?
Next

What to Do???
• Chose the best Choice from the list:• Apply Oxygen• Administer ASA• Administer NTG• Obtain a 12 lead EKG

Yes, Yes , Yes
•A 12 lead EKG is what is needed now, before any treatment is
made. Let’s get a 12 lead, shall we??

WOW Next

What is it??
• If you said ACUTE INFERIOR WALL MI, you are correct
Click Here
Next

ACS
• Now that we have identified the problem, what do we do?• Administer 324 ASA (if no allergies/GI bleed, etc..)• Obtain Vital Signs:• P 82, B/P 135/94, R 22 with bilateral clear breath sounds,
O2Sat 91% • Initiate Oxygen therapy according to saturation
reading
• Then What??
Next

The Sample History
• S – Slight discomfort, general malaise• A – Demerol• M – Hormone Therapy• P – None that she knows of• L – coffee and a donut 4 hrs. ago• E – Looking at dresses all day
Next

OPQRSTU
• O - about 90 minutes ago • P - None• Q - Slight pressure• R - Radiates to the back• S - Rates 6/10• T - about 90 minutes• U - Nothing seems to help
Next

What else should we ask?
• The bystander is often a great source of information:• The daughter tells you the patient has been having trouble
with her stamina for a couple of months. She can no longer walk any distance without becoming very tired. She refuses to see her doctor, tells her family “I’m just out of shape”
Next

Now what
• Based on the assessment, Vital signs, EKG and patient interview, what is your continued treatment plan. The closest hospital is 17 miles away and the roads aren’t that great??
Next

• You start an IV of normal saline• You continue to monitor the patients rhythm• Would you administer Nitroglycerine?
NO YES

No Nitro?
• Good thinking• You figured out the patient is having an inferior AMI, the
patient is suffering from the chest pain! Before you proceed with nitroglycerine administration, you MUST determine whether or not your patient has Right Ventricle Involvement (RVI) and will survive the administration of the Nitro
• You MUST perform a right sided EKG to determine whether or not she has RVI before administering a potent vasodilator
Next

Nitro Yes?
• Not so fast….• Nitro will reduce the blood pressure, the pre-load and the
afterload• It could result in major hypovolemia• You MUST determine whether or not your patient has
Right Ventricle Involvement (RVI) before proceeding with the administration of Nitro
Next

Why not Nitro ??
• The rationale for giving nitroglycerin has been that it will vasodilate both sides of the systemic circulation, reducing both preload (venous return) and afterload (forward systemic resistance), which reduces the workload on the heart and therefore oxygen and glucose consumption
• Because the right ventricle pumps blood to the lungs, it does not pump against a high pressure, its functional abilities are dependent upon preload.
• NTG administration will cause vasodilation, thus reducing the preload to the heart (low pressure in the vena cava, poor suction ability of the right atrium), and affect the ability of the chambers to fill
Next

NTG Effects on RV
• A reduction in venous return will result in diminished pumping pressure by the right ventricle, diminished pulmonary circulation, diminished left ventricular filling, diminished cardiac output, diminished systemic blood pressure and, if not corrected, possible dysrhythmias, shock and death
• Since the coronary arteries receive their blood during the diastole, one can easily understand that a drop in stroke volume as a result of lessened preload will eventually result in a drop in coronary artery filling pressures
• SO, LETS CHECK THE RIGHT SIDE, SHALL WE
Next

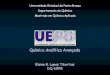
The Right Sided EKG Next
• Lead Placement for a Right Sided EKG

RVI on the EKG
ST segment elevation in V4R is considered to be diagnostic for right ventricular infarction; however, any ST elevation in the right V-leads 3 through 6 should signal suspicion for a right-sided MI
Next

Let’s get a Right Sided EKG
This is our initial EKG. We can’t tell, can we??
Next

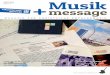
OK, Now we have it!!!
Significant ST Segment elevation in V4R, V5R and V6R! Still want to give Nitro??
Next

To Give or Not To Give
• In the case of an inferior MI with right ventricular involvement, the administration of nitroglycerin could cause an abrupt drop in blood pressure
• Some authorities state categorically that nitroglycerin should be avoided, while others simply urge extreme caution
• NTG should not be given without a systolic blood pressure of at least 100
• NTG infusion is preferable to tablets or spray, since an infusion can be titrated.
• Nitroglycerin paste is probably contraindicated due to the unpredictable onset of action and longer duration of effects
Next

Giving NITRO
• Prior to NTG administration, obtain IV access. • Many practitioners recommend two IV lines in cardiac
patients• If NTG is administered before an RVI is recognized and
hypotension results, fluids should be given. As much as two to three liters of normal saline may be required to restore preload to adequate levels
• As always, when administering fluids, lung sounds and oxygenation should be monitored
Next

Back to our Patient
• So you administered 1 sublingual Nitro tab to your patient
• You wait 3 minutes and re-assess her blood pressure, now 98/52
• Your patient becomes lethargic, and complains of a headache and some dizziness
• What now??
Next

Treat the Patient!!!
• Position the patient in a supine position• Administer fluids in 250 ml boluses until the blood
pressure returns to a perfusing rate• Listen to lung sounds, checking for fluid overload• What other intervention do the current protocols
allow us to perform?
Next

Choices, Choices…
What is your best answer?• Epinephrine 1:10000 infusion at 2 to 10 mcg/min titrated
to effect• Dopamine infusion 5 to 20 MCG/kg/min, titrated to
effect• Norepinephrine infusion 1 to 30 µg/min, titrated to effect• Vasopressin 0.04 Units/min, titrated to effect

Rock on… What else?
• Norepinephrine infusion 1 to 30 µg/min, titrated to effect is the preferred agent after infusion of fluids
• For patients with chest pain, Fentanyl is a great analgesic that does not affect blood pressure like Morphine may, and should be considered
• Anytime we can reduce pain in the chest pain patient, we reduce anxiety as well, thus reducing the overall severity of the event
Next

Conclusion 1 of 3
• Not all heart attacks are the same. Thirty to 50% of patients with inferior MIs have involvement of the right ventricle, usually with an obstruction of the right coronary artery above the first branches
• The main goals of field treatment for patients with RVI are to maintain preload to the right ventricle, cardiac output, blood pressure, coronary artery filling pressures and prevent shock
Next

Conclusion 2 of 3
• Because nitroglycerin is a vasodilator, it is contraindicated as standard treatment, or must be given with extreme care. Nitroglycerin should not be given unless specifically authorized by local protocols. Fentanyl may be given instead of Morphine, since Morphine also causes vasodilation
• Contrary to the practice of limiting fluids in MI patients without right ventricular involvement, fluids should be given to the RVI patient to maintain cardiac output, blood pressures and coronary artery filling pressures
Next

Conclusion 3 of 3
• EMS providers play a special role in early diagnosis and proper treatment of any patient who is having a heart attack. • By doing the right things, they can give the
RVI patient a better chance for recovery