Embed Size (px)
Citation preview

POSTGRADUATE DEPARTMENT OF CONSERVATIVE DENTISTRY AND ENDODONTICS
SEMINAR TOPIC:-
RESTORATIVE MANAGEMENT OF WORN DENTITION - II
(Assesment & role of occlusion in tooth wear)
Presenter- Ashish ChoudharyPG student
UNDER GUIDANCE OF :-
Prof. Dr Riyaz Farooq (HOD)Dr Aamir Rashid (Asst. Prof.)Dr Fayaz Ahmed (lecturer)

CONTENTS
PATIENT’S HISTORY
EXAMINATION OF WEAR’s PATIENT
DIAGNOSIS
MEASUREMENT OF SEVERITY & PROGRESSION OF WEAR
DILEMA OF OCCLUSION
RESTORATION OF WORN DENTITION-II( Assesment & Role of Occlusion in tooth wear)

MOUNTING CAST (Articularors & Facebow transfer)
PROBLEM OF SPACES (increasing Vertical Dimension)
RESTORATION OF WORN DENTITION
REHABILIATION OF WORN DENTITION
MAINTENANCE
CONCLUSION
REFERENCES
RESTORATION OF WORN DENTITION-III( Treatment Planning)

TOOTH WEAR’S MULTI-FACTORIAL AETIOLOGY
ABRASION
ABFRACTION
ATTRITION
EROSION
BRUXISM

PATIENT’S HISTORY*
The successful management of any case of tooth wear is based on deriving an accurate diagnosis, having a clear understanding of the basic principles of occlusion, and a good working knowledge of available materials and techniques to treat such cases using both active and passive means
*BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The formulation of a comprehensive treatment plan relies on an accurate history and examination of the patient
The management of tooth wear depends to an extent on the ability of the patient’s understanding of the condition in order to provide information to allow the clinician to arrive at a differential diagnosis
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

According to Holbrook and Arnadottir, in order toprevent or reduce non-carious destruction of toothsubstance it is important to:
• Recognise that the problem is present• Grade its severity• Diagnose the likely cause or causes• Monitor progress of the disease in order toassess the success, if any, of any preventativemeasures
Br Dent J 2003; 195: 75–81
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The accuracy and importance of the chief complaint must be first evaluated
CHIEF COMPLAINT
Common complaints associated with dentitions displaying tooth wear include concerns relating to:
• Aesthetic impairment (fractured, unattractive teeth/restorations or tooth discoloration)
• Difficulties with function, such as the efficiency of mastication or lip/cheek or tongue biting
• Less commonly, comfort (pain and sensitivity)
Dahl B, Carlsson G, Ekfledt A. Occlusal wear of teeth and restorative materials. Acta Odontol Scand 1993; 51: 299–311
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

MEDICAL HISTORY
may reveal underlying conditions which preclude the provision of complex treatment plans, and may also provide a valuable insight into the aetiology of the wear pattern observed to be present
1. Medication asthma inhalers containing steroid or effervescent medication aspirin (salicylic acid) chewable vitamin C preparations (ascorbic acid) various iron preparations diuretic agents and antidepressant drugs
2. Presence of a gastro-oesophageal reflux as seen in patients diagnosed with :anorexia nervosa, bulimia nervosa or those with hiatus hernia,
sphincter incompetence, oesophagitis, or increased gastric pressure (and volume)
Br Dent J 1984; 157: 16-19
Quintessence Int 1997; 28: 305–313
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

3. Female patients are affected by eating disordersmore frequently than males at a ratio of 10:1.5Cyclical vomiting syndrome and voluntary regurgitation
(rumination) have also been reported as aetiological conditions
respectively
4. Pregnancy inc. in abdominal pressure Morning sickness
5. A history of heartburn or reflux is a key factor to note
Dent Update 2000; 27: 175–183
Quintessence Int 1996; 27: 123–127
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

PAST DENTAL HISTORY
will provide useful information as to the patient’sprevious level and experience of dental care
1. Oral hygiene habits should be ascertained, such as : type of toothbrush used, the intensity, the frequency and timing of toothbrushing as well as
the abrasivity of the dentifrice being used.
2. A poorly motivated patient or one with negative views
towards dental care or indeed a phobic patient may not be the
best candidate at first instance when considering complextreatment provision
3. Establish (where relevant) any previous experience of
removable appliance/prosthesis wear experience
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

SOCIAL HISTORY
lifestyle stresses occupational details which may also have a bearing on
their ability to attend for treatment plans which sometimes take numerous visits to execute
SwimmersCopper mine workers
HABITS & DIETARY ANALYSIS
Smoking, alcohol consumption or dietary trends
A detailed dietary analysis Of particular relevance to diet/beverages and tooth surface loss are the copious consumption of citrus fruits, pickles, vinegar (acetic acid), coarse food, cola, fruit juices and carbonated drinks
Br Dent J 1996; 180: 349–352
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

The frequency and quantity of daily intake, theduration of consumption and the method ofeating/drinking should be established
The presence of other habits which may be aetiological bynature such as that of pipe-smoking, pen/pencil biting, andholding objects between teeth
Patients affected by tooth wear should undertake athree day consecutive comprehensive diet diary(Watson and Burke)
Dent Update 2000; 27: 175–183
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

EXAMINATION OF THE WEAR’s PATIENT
Clinical examination of the dentition has two primary objectives:
1. To document and record the location, appearance and degree of toothwear
2. To evaluate the progress of toothwear over time
Dent Update 2002; 29: 162–168
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

EXAMINATION OF WEAR’s PATIENT*
Extra-oral examination
Include a meticulous assessment of theirtemporomandibular joints and associated musculature
The presence of any joint or muscle tenderness, clicking, crepitation,mandibular deviation on opening or closure or any associated aches/pain
The maximum jaw opening should be recorded (that less than 40mm between incisal edges is considered to be restricted)
Presence of parotid gland enlargement is often seen in bulimicpatients Quintessence Int 1996; 27: 123–127
*BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

include an assessment of the freeway space (FWS),by determining the patient’s resting verticaldimension (RVD) and occlusal vertical dimension(OVD), with the aid of callipers or by the use of a Willisgauge
The facial vertical proportions should also becarefully examined
Other techniques that can be used for the evaluation ofvertical dimension include the use of phonetic assessments(particularly the sibilant sounds), facial soft tissue contouranalysis, jaw tracking and the use of electrical musclestimulation techniques
The smile line and lip line should also be noted, as wellas any midline discrepancies
Dent Clin North Am 1993; 36: 651–663
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

a typical appearance resulting from loss ofocclusal vertical dimension; note the presence ofan ‘inverted lip profile’
BDJ;2012 ; VOLUME 212 NO. 1

Relationship between lower lip line and incisaledges of worn anterior teeth
Elongation of the worn anterior teeth is feasible
Elongation of the wornteeth would lead to anexcessively long clinicalcrown
(A) (B)
Dent Update 2002; 29: 162–168

Intra-oral Examination
Presence of buccal keratoses, scalloping of thetongue or signs of xerostomia
The level of oral hygiene should be recorded togetherwith the undertaking of a Basic Periodontal Assessment(BPE)
A dental chart should be completed, detailing thepresence or absence of teeth, dental caries, restorations,failed restorations, fractures, abrasions and erosive lesions
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

palatal erosion suggests an intrinsic aetiology labial erosion implicates extrinsic factors. Lesions involving incisal edges and cusps are generallyassociated with attrition, Asymmetric lesions may be due to abrasion In addition to examining the teeth present, the absence of anyteeth should be noted, given that lack of posterior support canpredispose to anterior tooth wear
may provide additional clues to the underlyingcause.For example,
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
BDJ;2012 ; VOLUME 212 NO. 1

Once diagnosed, the location of tooth wear
(localised, anterior/posterior or generalised) and
severity of the tooth surface loss should be recorded
(as being restricted to enamel only, into dentine or
severely affecting the teeth or series of teeth)
Tooth Wear Index of Smith and Knight
the presences (or absence) of:
• Crowding• Rotations• Tilting• Drifting• Spacing• Over-eruption• Mobility
A comprehensive occlusal assessment is mandatory.
The overbite and overjetshould also be measuredand recorded
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The presence of a stable centric occlusion(CO) should be determined, and toothcontacts in the intercuspal position (ICP)described
The ease with which the patient can be manipulatedinto their retruded arc of closure should also beestablished
Where a patient cannot be readily manipulated into centric relation(CR), due to protective neuromuscular reflexes, the use of
deprogramming devices should be considered
1. use of cotton wool rolls and wood spatulas2. anterior bite planes (Lucia jig)3. full coverage stabilisation splints
BDJ;2004 ; VOLUME 196 NO. 7
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

DEPROGRAMMING DEVICES
BDJ;2004 ; VOLUME 196 NO. 7
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Permissive splints as muscle deprogrammers
Are designed to unlock the occlusion to remove deviating tooth inclines fromcontact
When this is accomplished, the neuromuscular reflex that controls closureinto maximum intercuspation is lost
The condyles are then allowed to return to their correct position in CR ifcondition of the articular components permits
Because all corrective tooth inclines are either separated or covered withsmooth plastic, permisive splints allow the muscles to function according totheir own coordinated interactions, thus eliminating the cause & the effects ofmuscle incoordination
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
PETER E. DAWSON; Evaluation, diagnosis & treatment of occlusal problems; 2ND EDITION

CENTRIC RELATION OCCLUSAL SPLINTS
Waxup showing contacts &anterior guidance
Lateral view showingposterior disclusion inlateral excursions
PETER E. DAWSON; Evaluation, diagnosis & treatment of occlusal problems; 2ND EDITION
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

CENTRIC RELATION OCCLUSAL SPLINTS
Adjusted splint-holdingcontacts(black), lateralcanine guidance(red), &protrusive(green)
Centric relation occlusal splints should be fabricated with anterior guidance inclines that disclude posterior contact in all eccentric jaw positions
PETER E. DAWSON; Evaluation, diagnosis & treatment of occlusal problems; 2ND EDITION
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

HAWLEY BITE PLANE (ANTERIOR BITE PLANE)
Allows the occlusal verticaldimension to be increased byonly a small amount withoutexceeding the VDR
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
Martin D. Gross; Occlusion in Restorative Dentistry; 1st edition

The first point of tooth contact in CR, hence theretruded contact point (RCP) should be identifiedand the presence of any ‘slides’ (and the directionof the latter) from CR to CO established.
Tooth contacts during lateral excursive (canine guidance orgroup function) and protrusive movements of the mandibleshould be determined
It is also important to note whether the slide from CRto CO has a larger vertical or horizontal component
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

If present, any working side/non-working sideocclusal interferences should be described
Where the patient may be partially dentate, anevaluation of the denture bearing areas must beundertaken, as well as the fit of any removableprostheses
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
ESTHETICAL CONSIDERATIONS WHILE EXAMINING THE PATIENT…….
EXTRA-ORAL INTRA-ORAL
Facial Symmetry Facial-Dental Midline Comissural-Bipupillaryline Smileline Lower teeth-Lip Symmetry Lower Lip Length
Tooth Axis Balance of Gingival Levels Zenith positioning Level of interdentalcontact Relative Tooth Dimension / Tooth Form Transitional lines Tooth Characterization

MIDLINE ANALYSIS
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

BALANCE OF GINGIVAL LEVELS
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

TOOTH DISPLAY
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

OCCLUSAL CONSIDERATIONS
OVERJET OVERBITE OCCLUSAL PLANE
STRUCTURAL COSIDERATIONS
LACK OF TOOTH STRUCTURE IN WORN DENTITION PROBLEM OF SPACE FOR RESTORATIONS
BIOLOGICAL CONSIDERATIONS
PUPAL INVOLEMENT NEED FOR POST & CORE NEED FOR CROWN LENGTHENING
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

OCCLUSAL PLANE
NORMAL STEP UP / STEP DOWN(Alternate pattern)
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
LABIOLINGUAL INCLINATION
Draw a perpendicularfrom the central toocclusal plane

Radiographs
Good quality, accurate long cone periapicalradiographs
presence of any signs of alveolar bone loss
Other factors, such as the root surface morphology, anatomy of the pulpchambers of affected teeth, quality of pre-existing endodontic treatment(s),presence of dental caries, widening/disturbance of the lamina dura, presenceof retained roots or any signs of periapical pathology (radiolucencies or radio-opacities) should also be assessed.
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Articulated study casts
Good quality study casts poured in vacuum mixed die-stone should be mounted on at least a semi-adjustable articulator in centric relation
Study casts will permit an assessment of the occlusion in theabsence of soft tissue/muscular interferences
The impact of tooth over-eruption can be more readilyassessed together.
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The vertical and horizontal components of the slide fromCR to CO can also be examined at this stage
Tooth contacts in CR, during lateral excursiveand protrusive movements, and the presence ofocclusal interferences can be more easilydetermined
The space gained by manipulating the mandible into CRcan be noted and the effect of ‘opening the bite’ on thearticulator on the residual dentition also seen, along withthe effect of any trial occlusal adjustments
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Sensibility tests
Loss of vitality
important to establish the health status of thedental pulp prior to embarking upon anycomplex prosthodontic rehabilitation
application of ethyl chloride, warmed gutta percha or electric stimuli to the tooth
However, the ‘true’ vitality status of a tooth can strictly beonly established with the use of Doppler flow techniques
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Intra-oral photographs
Including anterior, posterior (left/right) views andocclusal views of both arches are very important
Images should be appropriately stored.
Salivary analysis
can be undertaken for both stimulated and un-stimulatedsecretion rates and respective buffering capacities.
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Diagnostic wax mock-ups
may be fabricated with the desired finalocclusal scheme and aesthetic requirementsas prescribed by the operator
They form a useful visual aid and communication tool, to assist in theevaluation of aesthetics, tooth shape, length, and inclination
wax up once duplicated by the means of a stone model can be used tofabricate a vacuum formed PVC matrix that can initially be used todemonstrate the proposed changes intra-orally by the application of aprovisional crown and bridge material into the vacuum formed matrix
The matrix helps fabricate definitive restorations using direct resincomposite
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

wax mock-up can used as an aid tohelp form tooth reduction guides,assist with the fabrication ofprovisional restorations, or used toform a polyvinylsiloxane (PVS) index,which helps form direct resincomposite restorations
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

A) Study casts of a patient displayingtooth wear, mounted in centricrelation on a semi-adjustablearticulator
B) Diagnostic wax up fabricated inaccordance with an accurate occlusal-aesthetic prescription
C & D) Information derived from the wax up has been used to guide theplacement of restorative materials
BDJ;2012 ; VOLUME 212 NO. 1

The diagnosis of a patient presenting withtooth wear should include a description ofthe type(s) of lesions observed, togetherwith an account of their extent/locationand severity.
DIAGNOSIS OF TOOTH WEAR
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Diagnose the lesion!!
ATTRITIONABRASION
ABFRACTION EROSION
HISTORYChief ComplaintMedical historyHabitsOccupationLifestyle
EXAMINATIONExtra-oralClinicalpresentation
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

SEVERITY OF TOOTH WEAR
Tooth Wear Index by Smith & Knight
BEWE (Basic Erosive Wear Examination)
THE ACE Classification
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

LOCATION OF TOOTH SURFACE LOSS
Finally, the pattern of tooth surface loss seenshould be sub-classified into being eitherlocalised or generalised tooth wear
In the case of localised tooth wear, it is important tospecify the region affected, such as anterior, posterior,mandibular or maxillary
Mandibular anterior teeth are relatively less affected bythe process of erosion than the maxillary anterior dentition.
Posterior teeth are protected by secretions from theparotid glands
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

For cases of localised wear, it is also worthconsidering whether there may be spaceavailable for the placement of restorativematerials
For cases of generalised tooth wear, it is important tocategorise the amount of dento-alveolar compensationthat might have taken place
The loss of tooth structure may or may not result in anincrease in the Freeway space (FWS)
BDJ;2012 ; VOLUME 212 NO. 1
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Following an evaluation of the existing vertical dimension of occlusion (OVD) patients presenting with generalised wear may be assigned to three categories according to Turner and Missirlian
Category 1
Category 2
Category 3
excessive wear with loss of vertical dimension ofocclusion
excessive wear without loss of verticaldimension of occlusion, but with space available
excessive wear without loss of verticaldimension, but with limited space
J Prosthet Dent 1984; 52: 467–474
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Dent Update 2002; 29: 162–168

Dent Update 2002; 29: 162–168

Dent Update 2002; 29: 162–168

Measurement of Severity & Progression of Tooth Wear
Tooth Wear Index by SMITH & KNIGHT
PROFILOMETRY
Diagnostic Casts / Study Models
Silicone Impressions
CONTACT STYLUS TECHNIQUE
“FITTING” the Computer Models together
OPTICAL TECHNIQUES ( LASER & WHITE LIGHT)
MICROCOMPUTER TOMOGRAPHY SCANNINGMETHOD
J Oral Rehabill. 2012 ;39; 217–225
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Silicone Impressions Technique:
A silicone putty impression is taken in an sectional tray
The putty (e.g. Rapid) is removed from the tray
It is sliced into sections with a scalpel
When a section is placed over the tooth, it is a perfect fit. If wear progresses, a gap will become visible at future visits

Xhonga et al. (1972) used profile tracings fromsectioned study models to estimate an avg. dailyrate of erosion in cervical lesions
The real problem of measurement of tooth wear byprofilometry is that volumetric loss of tissue has a complexshape which defies assessment by simple geometriccalibration, such as a ruler might give
Answer to the problem ofcourse lies in the capture ofentire anatomical tooth surfaces of the before and after timeinterval
This requires a digital technique with software facilitiesfor computer image rendering, fitting & measurement
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

CONTACT STYLUS TECHNIQUE :
Null point stylus fixed in space & the model of the tooth which moves underneath the stylus
Digital scanningrendered to thecomputer , giving theappearance of tooth
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

“FITTING” the Computer Models together :
Wear on the incisaledge of a canine
The gray scalingshows the anatomicaldetail before (B), &wear is superimposedas a color reference 2yrs after baseline (2y)
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

OPTICAL TECHNIQUES ( LASER & WHITE LIGHT) :
White light digital profiler
(A) Light being emitted from one port& detected by a CCD in the other
(B) 3 point triangulationnecessary to determine theanatomical location of thewear area
Toothwear: ABC of the worn dentition; 1st ed

MICROCOMPUTER TOMOGRAPHY SCANNING:
Micro-Computer Tomography derived model of long term cervicalabrasive wearNote the inclusion of undercut in the total profile of lesion
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

REPORTING TOOTHWEAR
VOLUME REPORTING
DEPTH LOSS
INCREASE IN AREA OF CONTACT
DEPTH × AREA = VOLUME
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

OBJECTIVES of Tooth Wear Measurement by Profilometry :
Is Occlusal Attrition or Erosion the more rapidprocess?
Does the rate of Erosion differ in different molars?
Does the rate of Erosion differ on differentcusps on the same tooth?
Is the rate of erosion affected by preventive therapy?
Is the rate of attrition affected by splint therapy?
Does the rate of cervical tisssue loss relate to occlusalloss?
Toothwear: ABC of the worn dentition; 1st ed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Problems with these latest gadgets!!!!
× despite improved accuracy and reliability,new sophisticated measuring tools are costlyand require specialised hardware andsoftware, restricting their use in everydaydental practice
Al-Omiri et al. compared the reliability of three different methodsto detect incisal wear over a 6-month period.The methods used were a CAD–CAM laser scanning machine, atool maker microscope for micromeasurement applications and aconventional toothwear index (Smith and Knight wear index).It was found that the tooth wear index was the least sensitive fortooth wear quantification and was unable to identify wearprogression in most cases
J Dent. 2010;38:560–568
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Problems with these latest gadgets!!!!
× However, the fundamental problem with invivo wear studies is the inherent patientfactor
× In addition, the sensitivity of measurementand replica techniques are an important consideration
Therefore, appropriate training and calibration areimportant to minimise subjective errors and a combination ofmethods should be used for a more reliable quantitativeanalysis
J Oral Rehabil. 2001;28:1048–1055
J. Engineering Tribology. 2005;219:2–19
J Oral Rehabill. 2012 ;39; 217–225
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

DILEMA OF OCCLUSION
The three-dimensional relationship of themandible to the maxilla, and the clinician'sunderstanding of it, is fundamental in clinicaldental practice
No matter the degree of restorative dental treatmentprovided, be it a small occlusal restoration to a full-mouth rehabilitation, the occlusion is affected to agreater or lesser extent
British Dental Journal 2004; 196: 395–40
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

.
Occlusion has been defined simply byDavis and Gray as ‘the contactsbetween teeth'
These contacts can be considered statically or dynamically,as teeth slide over each other during mandibular movement
In addition to the occlusion, the masticatory system is alsocomposed of the periodontal ligaments, TMJ , the muscles ofmastication and their associated ligaments
The system is under the control of higher centres in thecentral nervous system
Br Dent J; 2001; 191: 235-245
Br Dent J 2001; 191: 291-302
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Various School of Thoughts for mandibularpositions
The early Conical and Spherical theories weresuperseded by the mechanical models of theGnathologists
These theories were largely driven by developments inarticulator design
In recent years, the engineering model of occlusion has beentempered by an increased appreciation of the biological aspectsof the masticatory system.
degree of adaptability
J Prosthodont 1993; 2: 33-43
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The occlusion achieved during normalfunctional mandibular movements, such asswallowing and chewing, occurs within a relativelysmall space called the “envelope of motion”
Abnormal movements are dysfunctional, caused byderangement of the articular disc and musclehypertrophy
Parafunctional activity is usually habitual, the patientoften being unaware of the movement, and includesbruxism, clenching, jaw posturing, lip and pencil biting
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

These activities can create excessive forcesbetween teeth or produce normal forces at anabnormal frequency, producing a risk of: fractured cusps or restorations; increased tooth mobility; muscle fatigue; and toothwear
“A harmoniously functioning occlusion allows for smoothuninterrupted movements over the area of tooth contact”
Some occlusions may not permit such free movements,yet the patient does not exhibit the problems described;his/her neuromuscular system has adapted to thedisharmony
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

However, if a restoration is placed whichchanges the occlusion, the adaptive capacity ofthe system may be exceeded, leading to the signsand symptoms
“ Therefore restorations should be planned so thatthey do not cause effects that exceed the adaptiveTolerance ”
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

They represent the movement of the tip of the lowerincisor when viewed in the sagittal or frontal plane
Posselt described the extreme or bordermovements of the mandible as an“envelope of motion“
Dent Update 2003; 30: 150-157
J Prosthet Dent 1957; 7: 787–797
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Acta Odontol Scand 1952; 10: Suppl 10

The mandible initially opens with a hingemovement about a horizontal axis known as theretruded axis or terminal hinge axis (THA), with thecondyles in the retruded position (RP) (centricrelation)
This is described as the most superior position ofthe condyles in their fossae
When the mandible rotates around this axis the first tooth contact occurs – the retruded contact position (RCP)
The mandible then slides forwards bringing the teeth into maximum intercuspation – the intercuspal position (ICP) (centric occlusion)
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The discrepancy between RCP and ICP has both avertical and horizontal component and may be upto 1 mm.
However, patients with this slide usually close straight intoICP from the rest position – the habitual path of closure
Acta Odontol Scand 1952; Suppl 10
Contact between opposing teeth can occur in the area ofthis discrepancy during swallowing, mastication andparafunctional activity.
When teeth are in the intercuspal position the occlusalvertical dimension (OVD) is defined as a measurement of faceheight
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

When not in contact, teeth are held apart inthe rest position by the muscles of masticationacting on the mandible creating a freeway spaceor Interocclusal distance of 2–4 mm
In practice, this position is variable, being affected by postureand muscle activity
When mandibular teeth move from ICP to maximumprotrusion their path is determined by the articulatingsurfaces of the anterior teeth, creating anterior guidance
This does not exist in anterior open bites or edge-to-edgeincisor relationships, where during protrusion the guidanceis obtained from the occlusal surfaces of the posterior teeth
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The angle and length of the movement isdetermined by the incisor relationship
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

ICP is maintained and occlusal forces directedaxially by two types of Interocclusal contact:
The maxillary buccal and mandibular lingual cusps aretherefore the non supporting cusps.
The palatal cusps of the maxillary teeth and buccal cuspsof the mandibular teeth (called supporting cusps) contactthe inclined planes of the opposing dentition or the cusptips contact the opposing fossae
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

During lateral excursions, the side to which themandible moves is the working side and theopposite side the non-working side
On the working side, when only the canines are in contactduring lateral excursions, the occlusion is canine guided; if twoor more pairs of teeth contact in this movement the occlusion isin group function. This may involve both anterior and posteriorteeth
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

On opening from RCP the mandible rotatesaround the THA in an arc of a circle (point Y)
This creates an incisal separation of about 2.5 cm.
On further opening the condyles translate or slidedownwards and forwards along the articular eminencies ofthe glenoid fossae to a point of maximum opening
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

During lateral movements, the working side orrotating condyle may rotate and move laterally aswell as upwards, downwards or backwards. Thelateral component is termed the Bennettmovement
The first part is calledimmediate sideshift and ismeasured on average at 0.5 mm.The progressive sideshiftdescribes a more graduallateral movement
The non-working side orbiting condyle movesdownwards, forwards andinwards, creating the Bennettangle
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

The free-sliding movement of the mandible canbe disturbed by an occlusal interference occurringbetween opposing teeth
The interference may arise as a result of tooth movement,over-eruption or occlusal wear in the unrestored dentition orof poorly contoured restorations
To maintain occlusal stability there must be adequateocclusal contact to prevent such interferences
This stability can be maintained by assuring occlusalcontacts are not on inclined planes but ideally in a cusp-to-fossa or cusp to marginal ridge position
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

ASSESSMENT OF THE OCCLUSION
The diagnostic process begins with carefulhistory taking and clinical examination
The examination should include:
Extra-oral components – temporomandibular joints,muscle hypertrophy/spasm
Mandibular movement – painful, deviated, abnormalor restricted
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

ASSESSMENT OF THE OCCLUSION
Intra-oral features:
1. Intercuspal position, retruded contact position, lateral &anterior guidance.
2. Presence, angle & smoothness of any slide from RCP to ICP.
3. Location and extent of occlusal faceting.
4. Ease of movement between mandibular positions as in 1.
5. Extent of posterior support.
6. Over-erupted, tilted or mobile teethDent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

DETECTING OCCLUSAL CONTACTS
Articulating paper is used to mark or indicatethe position of occlusal contacts. Thin articulatingpaper such as GHM occlusion foil which is 19 micronsthick, marks true contact points; thicker paper (70–200microns) can produce inaccurate and often largerpoints
To show occlusal contacts the teeth must be dry
Articulating paper, held in Miller’s forceps , is placedbetween the teeth and the mandible guided into whicheverposition is being assessed to record the points of toothcontact
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Articulating paper held in Miller’s forceps
Different occlusalindicators – wax, paper, shimstock
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

T-SCAN III SYSTEM(Computerised occlusal analysis Technology)
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Contacts with articulating paper
Occlusal analysis with T-scan III
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Articulated study casts, mounted on a semi-adjustable articulator using a facebow record,provide more detailed information that cannot bereadily assessed in the mouth
The casts must be articulated in RP so any slide from thisposition to ICP is detectable
The interocclusal records must also include lateralexcursions and protrusion so both the horizontal and verticalcondylar guidance and incisal guidance can be programmedinto the articulator
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Retruded Contact Position
“Guided occlusal relationship occurring atthe most retruded postion of the condylesin the joint cavities”
A position that may be more retruded than thecentric relation position
The Academy of ProsthodonticsGlossary of prosthodontic terms
J Prosthet Dent 1999; 81: 48-106
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

“The maxillomandibular relationship in whichthe condyles articulate with the thinnestavascular portion of their respective discs,with the complex in the anterior-superiorposition against the slopes of the articulareminences”
This position is independent of tooth contact. It is restricted to a purely rotary movement about thetransverse horizontal axis
CENTRIC RELATION
The Academy of ProsthodonticsGlossary of prosthodontic terms
J Prosthet Dent 1999; 81: 48-106
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Intercuspal position
“The complete intercuspation of the opposingteeth independent of condylar position.”
Sometimes referred to as the best fit of the teeth regardlessof the condylar position
Centric occlusion
“The occlusion of opposing teeth when the mandibleis in centric relation”
This may or may not coincide with the intercuspalposition
The Academy of ProsthodonticsGlossary of prosthodontic terms
J Prosthet Dent 1999; 81: 48-106
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

IMPORTANCE OF RCP
RCP is said to be a “relatively reproducibleposition” and as such is useful in the restorativemanagement of dentate and edentulous individualsand as a reference point for the registration oftransfer records, so that casts can be mountedon articulators
Posselt in his classic treatise ‘Studies in the Mobility of theHuman Mandible', found that the retruded position of themandible was reproducible to within 0.08 mm and thuscould be termed a border movement
Acta Odontol Scand 1952; 10: Suppl 10.
J Prosthet Dent 1964; 14:,266-278
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

In Dentate subjects….
RCP is an unstrainedposition of the mandiblerelative to the maxillaoccurring at initial toothcontact
This contact follows closure about the terminal hinge axiswhere the condylar heads are in their most anterior andsuperior position in the glenoid fossae
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
British Dental Journal 2004; 196: 395–402

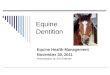
Relevant bony anatomy of the skull baseand the right TMJ articulation
A: mastoid process
B: right glenoid (articular)fossa with the antero-superior aspect shaded,
C: zygomatic arch
D: posterior hard palate,
E: pterygoid plates, and
F: styloid process
British Dental Journal 2004; 196: 395–402
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Posselt in 1952 found that in 10% of dentateindividuals, the RCP coincided with the intercuspalposition.
For the remainder, the RCP is infero-posterior to ICP by0.5—2 mm
The movement from the RCP tothe ICP is known as a “slide”
A slide has the potential for acombination of horizontal, verticaland lateral components along itspath
Acta Odontol Scand 1952; 10: Suppl 10.
Dent Update 1991; 18: 141-145.
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Subjects with an easily identifiable, stable andcomfortable ICP may only require a conformativeapproach rather than reorganisation at RCP.
Reorganisation involves altering a patient's existingICP to a new ICP.
This new ICP is made coincident with RCP becauseof the reproducibility of the latter.
This will eliminate the RCP-ICP slide
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
British Dental Journal 2004; 196: 395–402

In Edentulous subjects…
There are no natural tooth contacts to define aretruded contact
In this situation, prosthetic toothcontact (or wax occlusal rim contact) willbe along the retruded arc of closure atsome point
This is dictated by the occlusalvertical dimension (OVD) appropriate forthat patient. Therefore, the mandible andmaxilla are in CR at this occlusal verticaldimension and it is from here that theprosthetic occlusal scheme is constructed
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
British Dental Journal 2004; 196: 395–402

USES OF RCP IN THE DENTATE PATIENT
Mounting models on an articulator.Mandibular movement can be simulatedbecause of pure rotation about theterminal hinge axis
Helkimo M. Prosthodontic treatment of partially edentulous patients. Various centricpositions and methods of recording them. Zarb G A, Bergman B, Clayton J A, MacKay H F(eds) pp171-187. St Louis: CV Mosby, 1978
Reorganising a patient's occlusion at a new occlusalvertical dimension
Occlusal analysis in cases of toothwear, toothmobility, drifting, pain or repeatedly failingrestorations.
Br Dent J 2001; 191: 291-302
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Occlusal splint therapy
J Prosthet Dent 2001; 86: 539-545
‘Distalising' the mandible to create palatalspace for anterior restorations
J Oral Rehab 2000; 27: 1013-1023
Restoring a tooth which is involved indetermining the RCP
Br Dent J ;1982; 152: 160-165
USES OF RCP IN THE DENTATE PATIENT
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Midline analysis in cases of facial asymmetry,in order to separate dental and skeletal causes
Determining the magnitude and directionof the RCP to ICP slide in order to assessthe resultant force applied to anteriorrestorations
J Oral Rehab;2001; 28: 55-63
Ramfjord S P, Ash M M. Occlusion. 4rd edition, p 305.Philadelphia: WB Saunders Co, 1995
USES OF RCP IN THE DENTATE PATIENT
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

It has been suggested that RCP is attainableduring mastication and deglutition, and thatrestoring a patient to this position may result inenhanced masticatory efficiency and occlusalstability
J Oral Rehab 2000; 27: 1013-1023
Ramfjord S P, Ash M M. Occlusion. 4rd edition, p 305.Philadelphia: WB Saunders Co, 1995
Furthermore, it has been demonstrated that thereorganisation of patients to a situation where RCPcoincides with ICP will relapse after a period of time so thata slide between the two is re-introduced
Prosthet Dent 1973; 30: 591-598
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

FACTORS AFFECTING THE RCP RECORDING
Recording RCP is dependent upon a number offactors including the patient, operator experience andtraining ,the registration material and recordingmethod employed, the time of the recording, guidanceof the mandible, neuromuscular conditioning andrecord handling and storage
The diurnal variance of recording maxillomandibularrelationships has been studied in 13 subjects by Shafagh et al
Shafagh et al. found that retruded mandibular recordings madein the evening were more posterosuperior than those made in themorning
J Prosthet Dent 1975; 34: 574-576
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

In the dentate individual the RCP record is takenat a slightly increased OVD just prior to toothcontact (CR) with the mandible rotating about theterminal hinge axis
If tooth contact occurs, involuntary programmedmandibular deviation from the hinge axis will result due tosensory feedback from periodontal ligamentmechanoreceptors
Neuromuscular conditioning and the abolition of reflex patternsof closure can be achieved by the patient biting the teeth togetherhard, biting on cotton rolls, holding the mouth open wide, use ofan anterior jig or use of an occlusal splint
Br Dent J 2001; 191: 291-302
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Other influences that affect the RCP recordinginclude general health, attitude to treatment, co-operation and comprehension of the procedure, thepatient's body, head and tongue position, state ofrelaxation, medication and state of anaesthesia
The number of teeth, their condition or the ridge form ofedentulous patients will effect the stability of the recordingmedium and thus the quality of the recording
Pain from the operator's guidance technique, thetemporomandibular joints or from muscle tension willresult in reflex mandibular protrusion and hence erroneousrecordings
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

MANDIBULAR GUIDANCE & RCP
The aim of mandibular guidance is “to help locatethe condylar heads in the glenoid fossae at theterminal hinge axis in a consistent manner, thusproducing mandibular closure about the terminalhinge axis”Can be divided into those which are
PATIENT-GUIDED
Schuyler technique
Physiological technique
Gothic arch (Arrow-point)tracing
Myo-monitor
OPERATOR-GUIDED
Chin-point guidance method
Three finger chin-point guidance
Bimanual manipulation method
Anterior guidance by a Lucia Jig,Leaf Gauge , tongue blade ,OSU Woelfel Gauge
Power-centric registration method
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Schuyler technique
J Am Dent Assoc 1932; 19: 1012-1021
Physiological technique
uses cones of soft wax placed posteriorly. IN EDENTULOUS patientsJ Prosthet Dent 1955; 5: 319-322
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
PATIENT-GUIDED…

Gothic arch (Arrow-point) tracing
Maxillary andmandibular occlusalrims with a metal plateon the upper (left) andstylus on the lower(right)
Dent Cosmos 1910; 52: 1-19
Br Dent J 1994; 176: 386-393
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Gothic arch (Arrow-point) tracing
Where the lines meet on the plate represents theretruded mandibular position
The stylus scribes anarrow-head shapedtracing on the maxillaryplate outlining theprotrusive and right andleft lateral excursions ofthe mandible
Br Dent J 1994; 176: 386-393
Dent Cosmos 1910; 52: 1-19
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Gothic arch (Arrow-point) tracing
A system of recording a gothicarch tracing extra-orally
The stylus plate system isattached to the rims via forks
Br Dent J 1994; 176: 386-393
Dent Cosmos 1910; 52: 1-19
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Myo-monitor
an electrical jaw muscle stimulating devicewhich is reputed to achieve musclerelaxation and produce a neuromuscularmandibular position Eg. J-4 Muscle Stimulator which produces pulsed ultra-low
frequency stimulation of facial and masticatory muscles Stimulating electrodes are placed over the coronoid notches
& a common electrode is located at the nape of the neck Proponents of the myo-monitor suggest that the‘jaw-closer' muscles act simultaneously, via reflex contraction,to produce a reproducible retruded mandibular position
J Prosthet Dent 2000; 83: 83-89
Quintessence Int 1972; 12: 57-62
Prosthet Dent 1975; 34: 245-253

Chin-point guidance method
Patient's mandibleis guided into ahinge closure bythe thumb andindex finger of theoperator
Prosthet Dent 1960; 10: 849-855
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION
OPERATOR-GUIDED…

Three finger chin-point guidance method
A tripod is created at thechin-point and lowerborder of the mandibleon both sides by thethumb, index and thirdfinger
not recommended foredentulous subjects
Int J Perio Rest Dent 1984; 4: 62-66
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Bimanual manipulation method
Technique is carried out with the patient supine and the operator seated directly behind.
fifth finger of each hand is placed behind the angle of the mandible, with the fourth fingers positioned just in front of the angle
Prosthet Dent 1973; 29: 100-104
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Bimanual manipulation method
Third fingers are placed on the inferior surface of the body of the mandible, and theindex fingers submentallyin the midline
Thumbs are positioned laterally to the symphysis
An alternative method, with the operator in front of thepatient, is to use the index fingers to stabilise the lowerrecord base and guidance is from the thumbs on the chin
Prosthet Dent 1973; 29: 100-104
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a Lucia Jig
The basis of the Lucia jig method and the techniques that follow, is to provide an anterior reference point
J Pros Dent 1964; 14: 492-505.
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a Lucia Jig
An anterior stop also stabilises the mandibleduring recording and permits minimal toothseparation so that the recording medium is as thin aspossible
The lingual aspect should slope posteriorly and superiorlyat an angle of between 40–60°
A selected lower incisor scribes an arrow-head pattern, the‘wings' and ‘tail' of which can be ground away to leave the apex
J Pros Dent 1964; 14: 492-505.
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a Lucia Jig
This process is repeated until a raised areaof acrylic at the apex remains
This is the location of the retruded position and thevertical height is then adjusted until the posterior teeth arejust out of contact
The record is made at this position with the jig in the mouth
It is important to note that while the jig is being adjusted outof the mouth, the patient must bite on a cotton wool roll or asaliva ejector
J Pros Dent 1964; 14: 492-505.
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a tongue blade
The degree of tooth separationcan be altered by the number ofspatulas used
The patient's teeth must bediscluded for a period of time,usually between 10–20 minutesprior to registration
J Prosthet Dent 1970; 23: 11-24
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a Leaf Gauge
J Prosthet Dent 1973; 29: 608-610.
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Anterior guidance by a OSU Woelfel Gauge
was developed by Woelfel at Ohio State University (OSU)
The specially designed device has a graduated acetate biteplatform, the position of which is adjusted antero-posteriorlyuntil the teeth are minimally out of contact
J Prosthet Dent 1986; 56: 716-727
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Power-centric registration method
Operator employs a directed force to achievea retruded mandibular position
With the dentist standing in front and to the right of thesupine patient, the left thumb and forefinger are placed overthe upper teeth
right thumb is placed on the superior aspect of the chin,while the second and third fingers take up position along theinferior border of the mandible
Clin Orth 1981; 15: 32-46
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Power-centric registration method
Operator's right arm is stiffened and pressure is applied from the shoulder by leaning
It has been suggested that reflex muscle shortening acts to retrude the mandible
Clin Orth 1981; 15: 32-46
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Wise described RCP location techniques for thedentate patient based upon the relative ease ofmandibular manipulation
‘EASY' bimanual manipulation
‘manipulation with slight difficulty'
Anterior guidance from a tongue bladefollowed by bimanual manipulation
‘manipulation with more difficulty'
Lucia jig which may need to be left in situ for up to30 minutes
Br Dent J 1982; 152: 160-165
For some very difficult patients, an occlusal splint for anextended period
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

Discrepancy Between RCP and ICP
The mandible is manipulated into RCP and thepatient instructed to slide his or her teeth togetheruntil they meet in ICP or in the position that feelscorrect to them
This is identified using articulating paper
Lateral excursions are then made to detect the nature ofthe guidance and finally protrusive movement is used todemonstrate the type of anterior guidance
Dent Update 2003; 30: 150-157
HISTORYEXAMINATIONDIAGNOSISANALYSISOCCLUSION

THANKYOU………