Embed Size (px)
Citation preview

The evaluation of direct composite restorations for the worn
mandibular anterior dentition – clinical performance and
patient satisfaction
N. J. POYSER*,†, ‡, P . F. A. BRIGGS*,†, H. S. CHANA*,§, M. G. D. KELLEHER†,
R. W. J. PORTER*,† & M. M. PATEL* *Department of Restorative Dentistry, St George’s Hospital, London,†Department of Restorative Dentistry, King’s College London Dental Institute at Guy’s, King’s College and St Thomas’ Hospitals, London,‡Department of Hospital Dentistry, Mayday University Hospital, London and §Department of Restorative Dentistry, Kingston Hospital, Surrey,
London
SUMMARY This prospective split-mouth clinical trial
evaluated the performance and patient satisfaction
of 168 Herculite XRV direct composite restorations
bonded to the worn anterior dentition of 18 patients
with localized anterior tooth surface loss. One hun-
dred and six of these restorations were placed on the
mandibular anterior teeth. The restorations in-
creased the anterior occlusal vertical dimension
between 0Æ5 and 5 mm and the posterior occlusal
contacts were restored after a mean duration of
6Æ2 months (range: 3–13 months) in 14 out of the 15
‘Dahl’ sub-group patients. The restorations were
evaluated after 2Æ5 years of service by five examiners.
Four patients and 23 mandibular restorations were
lost to follow-up. Multiple clinical and restorative
variables were assessed to determine their influence
on restoration performance. Complete failure oc-
curred in 6% of the restorations. Circumferential
preparation and height of the restorative addition
did not influence the performance of the restorations.
A Visual Analogue Scale (VAS) was used to assess the
patient’s opinion regarding sensitivity, aesthetics,
longevity and function of the worn mandibular
anterior teeth. A statistically significant difference
(95% CI) was found between the pre-operative and 1-
month review VAS responses for aesthetics and
longevity and this was maintained at the 2Æ5-year
review. Direct composite restorations placed at an
increased occlusal vertical dimension are a simple
and time-efficient method of managing the worn
mandibular anterior dentition. Patient’s acceptance
and adaptation to the technique is good and the
results are accompanied with a high level of patient
satisfaction that is maintained for the medium-term.
KEYWORDS: composite resins, vertical dimension,
tooth attrition, tooth erosion, patient satisfaction,
prospective studies, adult
Accepted for publication 31 August 2006
Introduction
Tooth surface loss (TSL) can be caused by attrition,
erosion, abrasion and abfraction (1). The frequent
clinical finding is that they are often acting in combi-
nation (2). The management of the worn mandibular
anterior dentition is a restorative challenge. The prob-
lems frequently encountered are the lack of interoc-
clusal space owing to dento-alveolar compensation (3),
and problems related to the diminutive nature of these
teeth. Adopting a conventional prosthodontic approach
(i.e. conventional crowns) to manage the worn man-
dibular anterior dentition is not without complication.
Optimal preparation design will significantly weaken
the residual tooth tissue and often compromise the
integrity of the pulp. Frequently insufficient and inap-
propriate reduction is performed and the resulting
restoration may compromise periodontal health or
aesthetic outcome. In such situations, the placement
of direct composite restorations at an increased occlusal
ª 2007 Blackwell Publishing Ltd doi: 10.1111/j.1365-2842.2006.01702.x
Journal of Oral Rehabilitation 2007 34; 361–376

vertical dimension and utilizing the ‘Dahl Concept’ (4)
by relative axial tooth movement might be beneficial.
The reader is invited to refer to a paper recently
published by the authors that provides a summary of the
‘Dahl Concept’ and discusses these issues further (5).
Direct composite is increasingly being used for the
restoration of worn teeth as the material is inexpensive,
easy to use and repair, and can provide an acceptable
aesthetic result. Importantly, it can be placed with
minimal tooth preparation. Although the evidence for
its use as a medium-term restorative material is increas-
ing (6, 7), there has been limited research regarding the
technique specifically for the worn mandibular anterior
dentition. Evidence relating to the patient satisfaction of
this restorative technique is also limited.
This clinical study was prospectively designed and
executed to evaluate the following:
1 The re-establishment of posterior occlusal contacts
following the placement of anterior fixed composite
‘Dahl’ appliances at an increased occlusal vertical
dimension.
2 The internalization of the restorations. (When the
patient accepts the restoration as being part of them)
3 The time taken to place the restorations.
4 The medium-term performance of the restorations
placed for the worn mandibular anterior teeth.
5 To ascertain whether tooth preparation improved the
performance of the restorations.
6 To identify factors associated with restoration failure.
7 To determine patients’ thoughts about the treatment
and whether positive benefits are maintained over a
period of time.
Method
Pre-operative
Sample. Ethical approval for the study was obtained
from the St George’s Hospital ethical standards com-
mittee. The patients were recruited from the new
patient restorative consultation clinics at St George’s
Hospital. All of the patients had been referred by their
general dental practitioner for the management of TSL.
The inclusion criteria for acceptance into the study are
shown in Table 1. Patients were invited to join the
study and all were provided with verbal and written
information (5).
The proposed treatment and implications were dis-
cussed with the patient prior to gaining informed
consent and commencing treatment. An aspect of the
study was to investigate whether tooth preparation
influenced the survival of the restorations. The patients
were randomly allocated into two groups (by the toss of
a coin) and this determined which side of the dental
arch was to receive tooth preparation prior to the
placement of the restorations.
VAS questionnaire. All patients were assessed and
treated by one clinician with predefined procedures
and criteria. At the initial visit, prior to recording
baseline records or commencing treatment, patients
were asked to complete a ‘before treatment question-
naire’. The questionnaire asked the patients to mark
their response to four questions on a 100-mm
horizontal VAS, marked ‘Not at all ’ at left end and
‘A lot ’ at the right end. It was stated that the
questions were specifically in relation to their worn
lower anterior teeth. The questions were concerned
with sensitivity, aesthetics, longevity and function of
these worn lower teeth. The patients were asked four
questions:
1 How badly do hot or cold drinks, cold air or sweet
foods affect your lower teeth?
2 How concerned are you about the look of your lower
teeth?
3 How concerned are you about the life span of your
lower teeth?
4 How much do your lower teeth reduce your ability to
chew foods?
The response on each VAS was measured to the
nearest millimetre.
Pre-operative records. A thorough history and clinical
examination was undertaken and baseline records were
recorded on a ‘Clinical Assessment Sheet’. Every effort
was made to determine the aetiology of the TSL and to
assess whether parafunctional habits were involved.
Patients were offered appropriate preventative advice
Table 1. Inclusion criteria
Tooth surface loss primarily affecting the mandibular anterior
teeth
At least four teeth affected and require treatment
Teeth to have no existing restorations
Significant tooth wear with dentine involvement
and a reduction in clinical height
Stable periodontal status
N . J . P O Y S E R et al.362
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

prior to commencing any restorative treatment.
Pre-operative radiographs were taken to assess the
periapical status. The clinical features recorded during
the baseline record taking are shown in Table 2. The
incisal relationship and aetiology of the TSL was
independently evaluated by the authors using infor-
mation from the patients’ history, clinical examination,
digitized colour slides and pre-operative study models.
A consensus was made for those cases where there was
disagreement.
Clinical procedure
Clinical set-up. Great effort was made to control the
variables encountered during the clinical procedure.
1 All of the teeth requiring restorations were restored
with Herculite XRV composite and Optibond dentine
bonding agent*.
2 All of the mandibular teeth were restored at the same
visit. If the opposing dentition required restoration,
then this was provided at a subsequent appointment,
usually 4 weeks later.
3 All the patients were treated in the same clinical
setting with the same conventional light-curing unit†.
4 Clinical assistance was provided by the same experi-
enced dental nurse who was familiar with the compos-
ite build-up technique.
5 A dental shade‡ was taken prior to commencing the
clinical procedures.
6 Alginate impressions were taken for study casts and
all impressions were poured immediately by the same
qualified dental technician.
7 Pre-operative clinical photographs (1:1 magnified)
were taken using a Yashica Dental Eye III camera§ and
Kodachrome 64 colour slide film¶
Tooth preparation. The teeth on the side of the arch
chosen for preparation were prepared to a chamfer
margin to the criteria shown in Fig. 1 with a rounded-
ended tapered diamond bur (Bur No. 723Æ10C¶) in a
water-cooled air-turbine. All margins were kept in
enamel wherever possible. The aim was to improve the
resistance form of the restoration and to increase the
area of enamel available for bonding. No tooth prepar-
ation of the contra-lateral teeth was undertaken. An
alginate impression and clinical photographs (1:1 mag-
nification) were taken of the preparations.
Clinical procedure. A stopwatch was started to record the
time required for the remainder of the procedure. The
teeth were isolated with rubber dam and then cleaned
with a slurry of pumice and water. Clear cellulose strips
were used to separate interproximal contact points if
required. The enamel was etched for 30 s with 37%
phosphoric acid gel, washed for 30 s, and then dried
with a light stream of air from the 3-in-1 to avoid
desiccation of the dentine. Enamel and dentine bonding
was carried out according to the manufacturer’s instruc-
tions. The teeth were individually built-up with a bulk of
composite material. The aim was to restore the natural
height and aesthetic form. The composite was cured for
Table 2. Clinical features recorded at baseline
Incisal relationship
Occlusal vertical dimension
Periodontal parameters (pocket probing depth, bleeding on
probing, mobility and labial gingival recession)
Sensibility (ethyl chloride and electric pulp tester)
Degree of wear (Smith and Knight Tooth Wear Index) (8)
Height of the teeth
Shape of the incisal edge
Nature of the opposing dentition
1·0 mm
0·5 mm
Fig. 1. Preparation design for the circumferential enamel
chamfer.
*Kerr UK Ltd, Peterborough, UK†UnoDent Curing Light, UnoDent Ltd, Witham, UK‡Vitapan Classic, VITA Zahnfabrik, H Rauter GmbH, Bad Sackingen,
Germany
§Kyocera Corporation, Denville, NJ, USA¶Eastman Kodak Company, Rochester, NY, USA
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 363
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

40 s labially and a further 40 s lingually. Additional
increments were applied, if necessary. Gross adjustment
of the morphology of the composite was performed with
a tapered diamond bur in a water-cooled air-turbine
prior to commencing the build-up of the adjacent tooth.
Once all of the teeth were restored, the rubber dam was
then removed. The incisal aspects of the restored teeth
were adjusted to provide stable and even contacts with
as many opposing teeth as possible. Protrusive and
lateral excursive contacts were assessed with articula-
ting paper and adjusted to provide as smooth and even
anterior guidance as possible. Judicious adjustment was
carried out so that the appearance of the restorations
was not compromised. Canine guidance was established
in lateral excursion, if possible. The restorations were
finished with composite finishing burs, Sof-Lex discs
and interproximal polishing strips**. The stopwatch was
stopped and the time taken was recorded.
Immediate post-operative records. Post-operative clinical
observations were recorded of the occlusal contacts in
the new intercuspal jaw relationship, occlusal contacts
in excursions and the height of the restored teeth.
A post-operative measurement of the occlusal vertical
dimension was taken (if maxillary restorations were to
be provided, this measurement was recorded after these
were placed at a subsequent appointment). An alginate
impression, wax interocclusal registration and clinical
photographs (1:1 magnification) were taken of the
restorations.
Once again patients were warned about the increased
occlusal vertical dimension and advised what to expect.
They were instructed on appropriate methods of
homecare for their restored dentition.
Post-operative review – initial reviews until occlusal re-
establishment (N.P. only)
Post-operative follow-up was at 1, 3 and 6 months
following the placement of the mandibular restorations,
and then 3 monthly if the occlusion was yet to re-estab-
lish occlusal contacts. The patients were then reviewed
at 6 monthly intervals. At the initial 1-month review
appointment, patients were asked to complete an ‘after
treatment questionnaire’. The questionnaire was iden-
tical to the ‘before treatment questionnaire’ and the
patients were asked to focus on their lower anterior teeth
now that they had been restored. The patients did not
have access to their ‘before treatment questionnaire’.
At the review visits, the patients were questioned
regarding pulpal, periodontal and musculoskeletal
symptoms. They were asked when they considered
the restorations were part of them, a concept referred to
as internalization. The restored teeth were then
assessed with regard to their periodontal status, vitality
and restoration status. The re-establishment of posterior
occlusal contacts was assessed with Shimstock metal
foil††. Alginate impressions, a wax interocclusal regis-
tration and clinical photographs (1:1 magnified) were
taken.
Post-operative review – 2Æ5-year review (N.P., P.B., H.C.,
M.K., R.P., M.P.)
A multi-examiner assessment of the patients was
carried out at 2Æ5 years. All of the initial 18 patients
were invited by post to attend the review day. Non-
responders were contacted by telephone on two occa-
sions. Patients were given an appointment time as
convenient as possible for them but on a first-come-first
serve basis. The patients were not seen for review in the
same order in which they had been treated. Clinical
assessment of all the respondents was carried out on a
single day by five examiners.
Prior to clinical review. Patients were asked to complete a
questionnaire and VAS questionnaire immediately
prior to the clinical assessment. The VAS questionnaire
was the same as what had been used at the 1-month
re-assessment.
Assessment by N.P. The patients were questioned
regarding pulpal, periodontal and musculoskeletal
symptoms. The restored mandibular anterior teeth
were assessed with regard to their periodontal status
(pocket probing depth, bleeding on probing, mobility,
tenderness to percussion and labial gingival recession).
Sensibility testing was performed with an electric pulp
tester‡‡ and a cotton pellet cooled with Ethyl Chlor-
ide§§. The height of the teeth, the pattern of wear and
the nature of the opposing dentition were recorded.
**3M ESPE Dental Products, St Paul, MN, USA
††Hanel-GHM-Dental GMBH, Nurtingen, Germany‡‡Kerr Vitality Scanner; Kerr UK Ltd, Peterborough, UK§§Roche Consumer Healthcare, Welwyn Garden City, Hertfordshire,
UK
N . J . P O Y S E R et al.364
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

Alginate impressions were taken for study casts.
Clinical photographs (1:1 magnified) were taken using
a Yashica Dental Eye III camera§ and Kodachrome 64
colour slide film¶.
Assessment by, P.B., H.C., M.K., R.P., M.P. The restorations
were assessed according to a predetermined assessment
protocol that is shown in Table 3. The team had devised
and tested the protocol at an examiner-training day
4 weeks prior to the review day.
During the assessment, each patient remained in the
same dental chair and each examiner independently
assessed the patient in turn. Visual assessment was
performed on dry teeth using the dental light and
without auxiliary magnification. The teeth were dried
using a stream of air from the 3-in-1. Tactile assessment
was carried out under the same conditions and with a
WHO periodontal probe. In addition to the evaluation
of the composite restorations, some of the examiners
had other aspects of evaluation to complete. Occlusal
assessment was carried out with shimstock occlusal foil
[Shimstock metal foil†† by one examiner (H.C.) and
interocclusal wax registration* of the position of maxi-
mum intercuspation by one examiner (P.B.)]. One
examiner (M.K.) took parallel technique periapical
radiographs of the mandibular anterior teeth. The
radiographs were examined using a light-box and
magnification. The examiners had access to the imme-
diate post-operative study models to help determine the
loss of restorative material.
The data were entered into a MICROSOFT EXCEL database
for statistical analysis.
Results
Initial group – 18 patients
Eighteen patients (14 males and four females) between
31 and 75 years of age (mean 52 years) participated in
this clinical study. The tooth wear was thought to be of
combined aetiology in eight patients, predominantly
erosive in eight patients and predominantly attritional
in two patients. One hundred and sixty-nine direct
composite restorations were placed on the worn anter-
ior teeth of these 18 patients. One hundred and six of
these restorations were placed on the mandibular
anterior teeth.
Fifteen of the patients had the restorations placed as
fixed ‘Dahl’ appliances. The other three patients had the
restorations placed as part of a planned treatment to
reorganize the occlusal scheme at an increased vertical
dimension. The restorations created an immediate post-
operative increase in the occlusal vertical dimension
between 0Æ5 and 5 mm anteriorly. The demographics
and clinical findings of the 18 patients that participated in
the study are shown in Table 4. No preparation was
Table 3. Clinical assessment criteria used to evaluate the restorations
Visual assessments – dry teeth, dental light, visual inspection without magnification
Anatomical form (% of tooth volume lost) I <10% loss
II 50–90% still remaining
III <50% still remaining
Restoration staining (labial/incisal surfaces only) I None – no staining on the surface of the restoration is visible
II Mild – <25% of the surface of the restoration is stained
III Moderate – <50% of the surface of the restoration is stained
IV Severe – >50% of the surface of the restoration is stained
Marginal discolouration (whole labial margin only) I No staining – no staining of the margin is visible
II Staining – staining of the margin is visible
Colour match (labial/incisal surfaces only) I Acceptable – the restorative material matches the adjacent tooth structure
II Unacceptable – the match between the restorative material and
adjacent tooth structure is beyond an acceptable range
Tactile assessments – dry teeth, dental light, WHO probe
Surface roughness (labial/incisal surfaces only) I Smooth – the surface of the restoration feels smooth to the probe
II Rough – the surface of the restoration feels rough, pitted or grooved
Marginal adaptation (whole labial margin only) I No catch – the probe does not catch when drawn over the
margin of the restoration
II Catch – the probe does catch when when drawn over the margin of
the restoration
¶¶Dental Wax, Moyco Union Broach, York, PA, USA
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 365
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

carried out for patients 8 and 10. Patient 8 had TSL
predominantly affecting the labial and interproximal
aspects of his teeth and there was minimal loss of clinical
height. Tooth preparation would have led to the loss of
the little enamel that was remaining. Patient 10 had TSL
that was predominantly erosive in nature and affecting
the incisal edges. It was felt that there was no need to
prepare the ‘cupped-out’ erosive facets.
The majority of the patients’ mandibular anterior teeth
had Tooth Wear Index (TWI) (8) scores of 3 and 4 on the
incisal aspect of the teeth (Loss of enamel and substantial
loss of dentine with exposure of secondary dentine in
many cases) (Table 4). The majority of the buccal aspects
had TWI scores of 1 and 2 (Loss of enamel characteristics
and loss of enamel just exposing dentine). The mean
height and range of heights of the anterior mandibu-
lar dentition pre-operative and post-operatively is
presented for each patient in Table 5. The composite
restorations restored approximately 28% (range: 8–
48%) of the final post-operative tooth volume.
Re-establishment of occlusal contacts. In the ‘Dahl’ sub-
group of patients, the posterior occlusion was restored
after a mean duration of 6Æ2 months (range:
3–13 months) in 14 out of the 15 cases. One of the
cases (patient 3) had failed to re-establish posterior
occlusal contacts.
Internalization. Seventeen patients fully accepted the
restorations as being part of themselves and therefore
had achieved internalization. The patient who failed to
achieve internalization reported actively avoiding the
restorations whilst eating in an attempt not to fracture
them. The majority of patients reported that internal-
ization occurred after approximately 1 week (range:
0Æ5–12 weeks).
Procedure time. The mean time taken to place the
restorations on the mandibular anterior teeth for each
patient was 64 min (range: 48–80 min). The mean time
per tooth was calculated to be approximately 11 min.
Review group – 14 patients
Patient demographics and clinical status. Fourteen patients
of the initial 18 study patients participated in the
clinical review day (a review rate of 78%). Four
patients were lost to follow-up; one patient had died,
Table 4. Patient demographics, clinical features, Tooth Wear Index (8) (incisal and buccal) of the mandibular anterior teeth to be restored
(previously restored teeth were not included) and restoration status
Pt.
No. Age Sex Aet.*
Incisal
rel.
TWI incisal
mean (range)
TWI buccal
mean (range)
Total no. of
restns placed
No. of restns
placed LLS
Previously
estored LLS †teeth
Prep.
side
Incr.
OVD‡ (mm)
Dahl
case
1 48 M E II div. 1 3Æ60 (3–4) 1Æ60 (1–3) 10 6 1 L 2 d
2 53 M E I 4Æ00 1Æ00 12 6 0 R 2Æ5 d
3 54 M E III 4Æ00 1Æ00 12 6 0 L 1Æ5 d
4 75 F C I 4Æ00 3Æ80 (3–4) 6 6 1 R 2 d
5 65 M E I 4Æ00 2Æ40 (1–3) 10 5 0 L 5
6 59 M C II div. 1 4Æ00 1Æ00 6 6 0 L 2 d
7 38 F A II div. 1 4Æ00 0Æ00 8 6 0 R 2 d
8 58 M E III 3Æ40 (3–4) 3Æ00 11 5 0 None 0Æ5 d
9 42 F C II div. 1 3Æ83 (3–4) 0Æ00 6 6 0 R 2Æ5 d
10 31 M E I 3Æ00 1Æ00 6 6 1 None 1 d
11 34 M A II div. 1 3Æ50 (2–4) 0Æ00 7 6 0 R 2Æ5 d
12 65 M C II div. 2 4Æ00 1Æ00 10 6 1 L 2Æ513 71 M C II div. 1 4Æ00 1Æ25 (1–2) 6 6 2 R 1 d
14 46 M E I 4Æ00 1Æ00 11 6 0 R 1Æ5 d
15 52 M E I 4Æ00 1Æ83 (1–3) 12 6 0 L 4 d
16 34 F C II div. 2 2Æ17 (1–4) 0Æ67 (0–1) 12 6 0 L 2Æ5 d
17 44 M C III 4Æ00 1Æ67 (1–3) 11 6 0 R 4
18 63 M C II div. 1 4Æ00 0Æ00 12 6 0 L 3 d
*Aetiology: A-attrition, E-erosion, C-combination†LLS: Lower labial sextant‡OVD: occlusal vertical dimension
N . J . P O Y S E R et al.366
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

one refused to attend because of work commitments,
and it was not possible to contact two patients. The
absence of these four patients resulted in the loss of 23
mandibular restorations to follow-up. The patients of
the review group were aged between 31 and 75 years of
age (mean age 53 years) when the composite restora-
tions were initially placed. A total of 133 direct
composite restorations were placed on the worn anter-
ior dentition. Of these 83 restorations were placed on
the worn mandibular anterior teeth. Each patient had
all of their six mandibular anterior teeth restored except
patient 8 who had five of his six mandibular anterior
restored, as the other tooth did not require restoration.
Six of the mandibular restorations were excluded from
the study as the teeth had existing restorations present
(patients 1, 4, 10, 12 and 13).
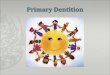
Occlusal contacts. After initial placement, 50 of the 77
restorations (65%) had contact with the opposing
dentition in the new intercuspal position. Fifty-four of
the 77 restorations (70%) were involved in excursive
guidance. The contacts by tooth are shown in Fig. 2.
Nature of the opposing dentition. The nature of the
occlusal surfaces of the teeth of the upper labial sextant
when the composite restorations were placed initially is
presented in Table 6. For the majority of patients, this
remained the same throughout the study. However,
some restorations were changed. Patient 18 had the
UR2 changed from composite to a porcelain fused-to-
metal crown with a palatal surface comprising of metal
and ceramic. Patient 12 had the UR2-UL2 changed from
composite restorations to four units of porcelain fused-
to-metal crown and bridgework with palatal surfaces
comprising of metal and ceramic. The UR3 changed
Table 5. The mean height of the anterior mandibular dentition pre-operatively and post-operative, and the mean height the composite
addition of the teeth (previously restored teeth were not included)
Pt. ID
Pre-operative height (mm)
Buc. rec.*
Post-op height (mm) Height of comp. addition to
incisal aspect of tooth (mm)
Mean (range) Buccal (range) Mean (range) Buccal (range) Mean (range)
1 5Æ2 (2–7) – 1Æ8 7Æ2 (5–9) – 2Æ0 (1–3)
2 5Æ5 (4–8) 5Æ3 (3–8) – 7Æ5 (6–10) – 2Æ0 (1–3)
3 8Æ0 (7–10) 7Æ5 (6–10) 0Æ7 9Æ0 (8–11) – 1Æ04 8Æ0 (7–9) 4Æ0 (2–6) – 8Æ4 (8–9) – 0Æ4 (0–1)
5 8Æ8 (7–11) 6Æ4 (5–10) – 11Æ0 (10–13) – 2Æ2 (2–3)
6 8Æ3 (7–10) 6Æ3 (5–8) – 9Æ7 (8–11) 9Æ0 (8–11) 1Æ33 (1–2)
7 4Æ7 (4–6) – – 7Æ5 (7–9) – 2Æ83 (2–3)
8 10Æ0 (9–13) – – 10Æ0 (9–13) – 0†
9 5Æ3 (4–7) 4 (2–6) 1Æ8 7Æ3 (6–9) 7Æ0 (5–9) 2Æ0 (1–3)
10 7Æ8 (7–8) 7Æ6 (7–8) – 8Æ4 (7–9) – 0Æ6 (0–1)
11 7Æ3 (6–10) 6Æ7 (5–9) – 8Æ5 (7–10) – 1Æ2 (1–2)
12 8Æ0 (7–9) 5Æ6 (5–7) – 9Æ0 (8–10) – 1Æ013 5Æ5 (4–7) 5Æ3 (4–7) – 8Æ5 (8–9) – 3Æ0 (1–5)
14 6 (5–7) 5Æ7 (5–7) – 8Æ3 (7–10) – 2Æ3 (2–3)
15 7 (6–8) 6Æ0 (5–7) – 8Æ2 (7–9) – 1Æ2 (1–2)
16 6Æ2 (5–8) 4Æ3 (2–7) – 7Æ8 (7–9) – 1Æ7 (1–2)
17 3Æ7 (3–5) 2Æ8 (1–5) – 6Æ2 (5–7) – 2Æ5 (2–3)
18 5Æ2 (4–6) 4Æ5 (4–5) – 7Æ5 (7–9) – 2Æ3 (1–3)
*Buccal gingival recession.†Labial composite addition.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
LR3 LR2 LR1 LL1 LL2 LL3
ICP contact Exc. contact
Fig. 2. Percentage of restorations with contacts in the intercuspal
position (ICP) and excursive movements.
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 367
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

from composite to a nickel–chromium metal alloy resin
bonded bridge wing retainer.
Restoration performance
Inter-examiner agreement. The level of agreement be-
tween the examiners for each clinical assessment
variable is shown in Table 7. For example, when
assessing the anatomical form, for 44% of the restora-
tions, all five examiners rated the restorations in the
same category, for 24% of the restorations four out of
the five examiners rated the restorations in the same
category, and for 32% of the restorations three out of
the five examiners rated the restorations in the same
category. Where there was disagreement between
examiners, the rating was never different by more than
one rating increment. The mathematical ‘mode’ of the
examiner results was used to definitively score the
restorations.
Complete failures. Six per cent of the study restorations
failed completely (i.e. total loss of the restoration)
during the study period. These were complete bulk
failure with no remaining composite on the tooth
surfaces. The clinical features of these failure cases are
shown in Table 8.
Because of the small sample size and small number of
failures, statistical evaluation was inappropriate. How-
ever, the majority of the failed restorations were
situated on the right hand side. This might be due to
operator technique and the fact that restorations might
be more difficult to place in this site for a right-handed
operator.
Partial failures Eighty-six per cent of those restorations
that had not completely failed had greater than 90% of
the post-restorative tooth volume. The other 14% had
between 50% and 90% still remaining. The loss of
material was due to wear rather than fractures and
chipping reported by other authors (6, 7). A frequent
observation was that the majority of composite resto-
rations had evidence of incisal wear at the early
reviews. The restorations were frequently constructed
with a flat incisal edge; however, at the initial reviews
(1 or 3 months) faceting of <10% was noted, which
provided an inclined contact area of a greater surface
area with the opposing dentition. Following this ‘self-
adjustment’, the progression of restoration wear was
minimal.
Restoration staining. Eight-one per cent of the remaining
restorations had no staining on the labial and/or incisal
surfaces. The other restorations (19%) exhibited mild
staining, but none of the patients were concerned about
this. In the authors’ experience, the degree of compos-
ite surface staining is greater in patients that smoke
tobacco products compared with non-smokers. Unfor-
tunately, it was not possible to investigate this further
as none of the patients in the study smoked. Composite
staining, especially in smokers, might be one of the
main disadvantages of this technique. Smokers should
be informed of the likelihood of composite staining pre-
operatively and the potential need for frequent main-
tenance and/or restoration replacement. If restoration
staining is likely to be a significant cosmetic issue, then
a move towards alternative restorations, such as the use
of ceramics, may be required.
Marginal discolouration. Seventy-four per cent of the
remaining restorations had no evidence of marginal
discolouration on the labial aspect. The remainder
(26%) had evidence of staining, which was of no
concern to the patient and required monitor and
review. None of the restorations required refinishing,
repair or replacement.
Colour match. Of the remaining restorations, all were
deemed to have an acceptable colour match. The colour
Table 6. Nature of the opposing static and dynamic occlusal
contacts
Nature of opposing occluding surface No. of teeth % of teeth
Direct composite resin 38 49
Natural tooth/composite 14 18
Natural tooth only 10 13
PFM* – metal and ceramic 12 15
PFM – ceramic only 3 4
RBB† – metal wing 1 1
*PFM: porcelain fused-to-metal restoration.†RBB: resin bonded bridge.
Table 7. Level of agreement between examiners for each clinical
assessment variable
Level of agreement 5 examiners 4 examiners 3 examiners
Anatomical form 44% 24% 32%
Restoration staining 33% 28% 39%
Marginal discolouration 49% 33% 18%
N . J . P O Y S E R et al.368
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

stability of the composite resin appeared to be good and
a change in the intrinsic colour of the teeth was not
apparent during the study period.
Surface roughness. Of the remaining restorations, all
were deemed to have a smooth surface on the labial
and incisal surfaces.
Marginal adaptation. Forty-six per cent of the restora-
tions had no catch on the labial aspect. The remainder
(54%) had evidence of a catch requiring monitoring.
No restoration required refinishing, repair or replace-
ment.
Wear of the opposing dentition. There was no evidence of
wear of the natural tooth substance by the composite
restorations.
Periodontal health. The presence of the restorations did
not have a detrimental effect on periodontal parame-
ters. The pre-operatively and the 2Æ5-year review
findings are shown in Table 9. The periodontal pocket
depths and bleeding on probing was not assessed for
one patient (patient 14) as they required antibiotic
prophylaxis for periodontal probing.
Pre-operatively 7 out of 13 patients (54%) and 16 out
of 71 sites (23%) exhibited bleeding on probing. At the
2.5-year review, 5 out of 13 patients (38%) and 10 out
of 71 sites (14%) had evidence of bleeding on probing.
This observation supports the findings of other studies
regarding this technique (7). The improvement in
bleeding on probing might be due to the fact that
many patients report difficulty and soreness whilst
brushing their teeth when they are short and worn.
Also patients might prefer the appearance of their teeth
post-operatively and wish to make more of an effort to
look after their teeth now that they have been restored.
Increased tooth mobility was seen in one patient
(patient 16) as two teeth exhibited grade 1 mobility
(LL2 and LL3) at review. These teeth were periodon-
tally intact. This patient had combination TSL. The two
restored teeth had no features that were significantly
different from the other restored teeth.
Occlusal re-establishment. All of the ‘Dahl’ subgroup of
review patients had experienced re-establishment of
the posterior occlusal contacts by 13 months. Closer
examination of the posterior occlusal contacts was
performed at the 2Æ5-year review with the use of
Shimstock metal foil. This revealed that one-third of
the ‘Dahl’ subgroup of patients had only achieved
Table 8. Details of completely failed restorations – (a) patient and
tooth demographics and (b) restorations details
(a)
Pt.
ID Age Sex Aet. Incisal rel. Tooth
Surface
shape*
TWI
I
TWI
B
1 48 M E II div. 1 LL3 Cup 4 1
4 75 F C I LR3 Incline 4 3
4 75 F C I LR2 Incline 4 4
13 71 M C II div. 1 LR2 Flat 4 1
15 52 M E I LR2 Cup 4 1
(b)
Pt.
ID
Pre-
operative
height
(mm)
Prep.
Post-
operative
height
(mm) Comp
add.
(mm)
Immediate
Post-
operative
tooth
contactsOpposing
surfaceMax Buc Max Buc ICP† Excur.
1 7 7 Y 9 – 2 Y Y Dir. Comp.
4 9 6 Y 9 – 0 Y Y Enamel
4 9 5 Y 9 – 0 Y Y PFM-M/C
13 4 4 Y 9 – 5 N Y Enamel
15 7 7 N 8 – 1 N N Dir. Comp.
*Shape of worn tooth surface: cup-cupped facet, inclined-inclined
surface, flat-horizontal surface.†ICP: intercuspal position.‡Aetiology: A-attrition, E-erosion, C-combination.
Table 9. The periodontal status of the restored mandibular
anterior teeth pre-operatively and at 2Æ5-year review [(a) tooth
basis and (b) patient basis]
Pre-operative Review
(a)
Number of restored teeth
Bleeding on probing
(one or more sites per tooth) (n ¼ 71)
16 10
Pocket depth (4 mm or greater) (n ¼ 71) 1 0
Mobility (n ¼ 77) 0 2
Tenderness to percussion (n ¼ 77) 2 1
(b)
Number of patients
Bleeding on probing
(one or more sites per tooth) (n ¼ 13)
7 5
Pocket depth (4 mm or greater) (n ¼ 13) 1 0
Mobility (n ¼ 14) 0 1
Tenderness to percussion (n ¼ 14) 2 1
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 369
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

partial re-establishment as incomplete occlusal contact
was observed in the premolar regions. These findings
are similar to those found by Redman et al. (7).
However, none of the patients were aware of this or
expressed a desire to have more biting contacts.
Statistical analysis
Preparation versus no preparation. The influence of pre-
paration on the performance of the composite restora-
tions was assessed statistically using Fisher’s exact test.
Preparation was shown not to statistically influence
restoration survival, marginal adaptation, or marginal
discolouration. The contingency tables and P-values are
shown in Table 10.
Effect of restoration height on performance. The height of
restorative material added to the teeth was statistically
shown not to influence the performance of the resto-
rations with regard to restoration survival, marginal
adaptation and marginal discolouration. The height at a
cut-off point of 1-, 2- and 3-mm additions was statis-
tically assessed. The contingency tables and P-values for
a 1-mm cut-off height are shown in Table 11.
Patient satisfaction
VAS scores. The mean and standard deviation for the
VAS scores of the 14 review patients recorded pre-
operatively, at the 1-month review and at the 2Æ5-year
review for sensitivity, aesthetics and longevity are
presented in Fig. 3.
Following the placement of direct composite restora-
tions on the worn mandibular anterior teeth, a
statistically significant difference (95% CI) was found
between the pre-operative and 1-month review VAS
responses for aesthetics (t ¼ 6Æ41; d.f. 13;
P ¼ 0Æ000023) and longevity (t ¼ 5Æ93; d.f. 17;
P ¼ 0Æ00005). No statistically significant difference
was seen for sensitivity.
This difference was maintained during the review
period as a statistically significant difference was found
between the pre-operative and 2Æ5-year review VAS
responses for aesthetics (t ¼ 5Æ15; d.f. 13; P ¼ 0Æ0002)
and longevity (t ¼ 3Æ46; d.f. 17; P ¼ 0Æ004). Again no
statistically significant difference was seen for sensitivity.
Subjective assessment. All of the patients felt that the
treatment was in line with what they were expecting, all
felt that they were provided with sufficient information
prior to the procedure, and all would recommend the
procedure to a friend. These positive responses might be
related to the time and information, both verbal and
written, provided at the initial consultation.
Pulpal Vitality. Using a combination of clinical signs and
symptoms, sensibility testing and radiographic assess-
ment, it was determined that none of restored teeth lost
vitality following the placement of the composite
restorations.
Periapical resorption. None of the radiographs showed
evidence of periapical resorption.
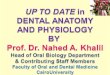
Case example
An example of a typical case is shown in Fig. 4.
Table 10. Statistical evaluation of whether tooth preparation
influences restoration survival, marginal adaptation or marginal
discolouration
Restoration
survival
Marginal
adaptation
Marginal
discolouration
Present Lost Catch
No
catch Staining
No
staining
Preparation 30 4 21 10 10 20
No preparation 42 1 19 23 9 33
P-value
(two-tailed)
0Æ1637 0Æ0947 0Æ2886
Stat sign* No No No
*Statistical significance.
Table 11. Statically evaluation of whether the height of the
composite addition (£1 mm vs. ‡2 mm) influences restoration
survival, marginal adaptation or marginal discolouration
Restoration
survival
Marginal
adaptation
Marginal
discolouration
Present Lost Catch
No
catch Staining
No
staining
‡ 2 mm 39 2 21 18 12 27
£ 1 mm 28 3 15 13 7 21
P-value
(two-tailed)
0Æ6457 1Æ000 0Æ7843
Stat sign* No No No
*Statistical significance.
N . J . P O Y S E R et al.370
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

Discussion
Occlusal re-establishment
The posterior occlusion failed to re-establish occlusal
contacts in one of the 15 patients (6%) in which the
composite restorations had been placed as a ‘fixed Dahl
appliance’. This patient was a 54-year-old partially
dentate male, with a Class III incisal relationship, who
exhibited erosive TSL predominantly affecting his
anterior maxillary and anterior mandibular teeth. The
only pre-operative posterior occlusal contact was
0
10
20
30
40
50
60
70
80
90
100
Sensitivity Aesthetics Longevity
Rat
ing
on a
100
mm
VA
S
Pre-operative1-month review2.5-year review
Fig. 3. The pre-operative, 1-month
review and 2.5-year mean Visual
Analogue Scale scores for sensitivity,
aesthetics and longevity (standard
deviation is shown as a vertical line).
Pre-operative anterior view –Intercuspal position
Pre-operative anterior view –Lower labial sextant
Pre-operative occlusal view –Lower labial sextant
Circumferential PreparationLR3 LR2 LR1
Direct Composite RestorationsLR3 to LL3 – Immediate Post-op
One-month review
Six-month review Eleven-month review Thirty-three month review
Fig. 4. Pre-operative and review images illustrating the performance of direct composite restorations over a period of 33 months. The
restorations were placed to restore the worn LR3 to LL3 (LR3 LR2 LR1 were the prepared teeth).
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 371
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

between the upper left 7 and lower left 7 due to a lack of
posterior opposing units. The 12 anterior teeth were
restored as a sextant at a time with a 1-month interval
between appointments. A post-operative increase in the
occlusal vertical dimension of 1Æ5 mm was recorded
anteriorly. There is no obvious explanation for the
failure of the re-establishment of posterior occlusal
contacts. The patient was not concerned and no further
intervention was required. Many authors have attrib-
uted this failure of occlusal movement to a lack of or less
effective eruptive potential (7, 9). The lack of occlusal
movement in this study is in agreement with other
authors. Gough and Setchell (10) reported a failure of
occlusal re-establishment in 4% of cases and Hemmings
et al. (6) reported the same finding in 6% of cases.
The mean time taken for the occlusion to re-establish
was 6Æ2 months. This is in agreement with the time
reported by Hemmings et al. (6) (4Æ6 months), Gough
and Setchell (10) (5Æ9 months), and Redman et al. (7)
(7 months).
Procedural time
It has been suggested that up to 30 minutes per tooth
(6) is required for the restoration of worn anterior teeth
with direct composite resin. This prolonged clinical time
might be a significant reason why alternative indirect
approaches have been suggested. The use of indirect
techniques such as laboratory fabricated composite
polyglass restorations (9) has been suggested to simplify
the clinical method and save chair-side time. However,
the optimal bonding and finishing of indirect adhesive
restorations is technically demanding and can be as
time-consuming as the placement of direct composite
restorations. The use of an indirect technique might
require a greater number of visits and the restorations
are likely to incur a laboratory cost. It is not possible to
make a direct comparison from the literature, as there is
no evidence relating to the time taken to place either
type of restorations.
The reason for adopting one technique over the other
should be related to how well the material performs
clinically and how amenable it is to maintenance. It is
the authors’ opinion that the direct freehand build-up
of teeth with composite resin is the most adaptable and
maintainable. Alternative direct techniques with the
use of a vacuum-formed matrix of a diagnostic wax-up
have been suggested to facilitate the placement of
multiple direct composite build-ups (11, 12). In this
clinical study, the mean time taken to place and finish
six direct composite restorations on the worn mandib-
ular anterior teeth was found to be 64 minutes. The
mean time per tooth to place the 106 direct composite
restorations on the worn mandibular anterior teeth of
all 18 patients was calculated to be approximately
11 minutes. This time is substantially less than the
suggested figure of 30 minutes per tooth (6). The
reasons for the efficient use of time during this study
are thought to be due to having a dedicated surgery
session where all of the equipment and materials are
laid out pre-operatively, working with an experienced
dental nurse, and the type of build-up technique.
Bulk build-up technique
The authors feel that the main reason for the compar-
atively short placement time is because the restorations
were constructed by using a bulk build-up technique. It
is the authors’ opinion that composite resin appears to
survive better if it is placed in thick sections. It is
possible to achieve this thickness if the teeth are built
up to their original morphology and thus increase the
occlusal vertical dimension significantly. In cases with
minimal TSL, it may be better to monitor the situation
rather than to place composite in thin sections that are
more vulnerable to fracture. This is especially true for
mandibular anterior teeth because of the shear and
tensile forces that these teeth are subjected to.
An incremental build-up technique (13) is considered
to be the optimal technique for the placement of
composite resins. The reasons for this are to ensure
complete penetration of the curing light through the
composite and to minimize contraction stresses during
polymerization. The manufacturer recommends that
Herculite XRV composite is not placed in increments
>2 mm. They also suggest that each surface of the
increment is cured for a minimum of 40 s. The
mandibular anterior teeth have a relatively narrow
bucco-lingual dimension, especially at the incisal edge.
Considering these dimensions, there is little concern
about inadequate penetration of the curing light leaving
uncured composite, especially if the restoration is cured
both buccally and lingually for the recommended times.
Filled resin-based materials contract by approxi-
mately 2–3% by volume on polymerization. Polymer-
ization contraction can lead to the formation of stresses
within the cured material or at the bonding surfaces.
These stresses can lead to the deterioration of the
N . J . P O Y S E R et al.372
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

material or debonding at the margins. The potential for
this phenomenon is greatest in cavities with a high ratio
of bonded surfaces to free surfaces, for example a Class I
restoration. In a Class I restoration, there are four
bonded walls and one bonded floor and only one free
unbonded occlusal surface at which contraction may
take place. The ratio of bonded to unbonded surfaces is
known as the Configuration Factor (14). Ideally, this
should be equal to, or less than one, if stresses are to be
avoided. Teeth that have been subjected to TSL tend to
exhibit a relatively flat incisal/occlusal surface for
which to bond to. A composite restoration placed on
such as surface has a favourable configuration factor as
there is one bonded surface and five free unbonded
surfaces at which contraction may take place. For this
reason, a bulk build-up technique for worn teeth with a
relatively flat bonding surface can be confidently
utilized. A bulk build-up technique significantly redu-
ces the time taken to place these restorations as it avoids
the multiple stages involved with the addition and
curing of the increments of composite. It might also
improve the surface integrity as it avoids the potential
of trapping air between increments or insufficient
material adaptation to the previous increment. With a
bulk build-up technique, the restorations can be over-
built and rapidly trimmed to the correct gross mor-
phology with a diamond bur in a high-speed turbine.
Final finishing can be completed in the usual way with
polishing discs, interproximal abrasive strips and pol-
ishing pastes.
Assessment criteria
Modifications of the USPHS assessment have been used
to assess restorations previously. The criteria used in
this study were based on the USPHS criteria, but the
authors felt that modification was necessary in order to
reflect the type of restorative material used, the
conservative management philosophy, patient involve-
ment in the decision-making process, and to provide a
more ‘clinical practice’-based assessment rather than
‘research’-based. The criteria were developed through
group discussion and successfully piloted during the
examiner-training day.
When assessing the performance of different types of
restorations, there is a pressure within the profession to
compare newer alterative restorations to the perceived
‘gold standard’ of a full coverage crown. However,
restorative materials, bonding systems and treatment
philosophies have evolved, so direct comparison is
inappropriate. Large composite restorations placed in
clinical situations where historically a crown would
have been indicated are likely to experience a greater
deterioration of some performance parameters if com-
pared with a crown. The survival of direct composite
restorations is likely to be reduced, but maintenance is
likely to be more favourable. The biological cost of
minimal preparation is preferable.
The USPHS criteria grade restorations according to the
categories Alpha (A), Beta (B) and Charlie (C). A
indicates everything is perfect and intact. B indicates
that inadequacies are evident but clinically acceptable,
and the restorations can be monitored, refinished or
repaired. C indicates that inadequacies are evident and
clinically unacceptable, and replacement of the restor-
ation is required. Unfortunately the USPHS criteria are a
clinician-based assessment system that does not consider
the patients’ concerns or wishes. The criteria lack
objective grading and is open to subjective error. How
can a clinician decide whether a restoration needs to be
replaced because of surface roughness, margin colour or
surface colour, as long as its presence is not detrimental to
the remaining tooth structure? A degree of staining
acceptable to one patient may be unacceptable to
another and the decision to replace the restoration is
extremely patient and operator dependant. It is for this
reason that you have to question the value of a clinician-
based C assessment; we did not include one. Our criteria
attempted to eliminate this subjective bias and simply
determined whether a variable was present or not.
The assessment needed to be patient-focused and
evaluate the restorations from a patient-based perspec-
tive. With regard to the restorations, the patients’ main
concerns are whether the restoration stays on or not,
and whether the visible surfaces look acceptable. It is
for this reason that only the labial and incisal surfaces of
the restored teeth were assessed with regard to areas of
potential aesthetic concern (i.e. restoration staining,
marginal discolouration, colour match, surface rough-
ness and marginal adaptation). Even if the lingual
surface was stained, this is likely to be of no concern to
the patient and it is likely that a monitor and review
approach would be adopted.
Restoration performance
Loss of restorative volume was due to wear rather than
fractures as described by previous authors. This might be
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 373
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

due to the fact that the composite restorations were
placed in bulk rather than increments and thus elimin-
ating the potential for failure at these interfaces. The
delamination of indirect Artglass restorations has been
reported (9).
Eighty-six per cent the composite restorations exhib-
ited <10% loss of volume and 14% exhibited 50–90%
loss of volume. None of the patients received an
occlusal coverage splint following the re-establishment
of occlusal contacts. Theoretically, the use of a
protective occlusal splint might reduce the wear of the
composite restorations but the patient compliance with
wearing these appliances is questionable.
According to the examining clinicians, marginal
discolouration was evident in 57% of patients, but
only affected 26% of the remaining restorations.
None of the patients remarked on the staining and
none requested replacement or rectification. The
patients’ aesthetic acceptance of the restorations was
good. This might be because the mandibular anterior
teeth are less visible than the maxillary dentition so
that the stained margin is less visible than if it
affected the labial surface of the maxillary teeth. But,
it must be remembered that eight of the patients also
had maxillary composite restorations placed (50
restorations). If these had stained unacceptably, then
the patient could have had a more pessimistic view of
the mandibular restorations.
The restorations placed as ‘fixed Dahl appliances’
performed as well as those placed as part of a planned
treatment reorganizing the occlusion at an increased
occlusal vertical dimension. This is despite the theoret-
ical risk that the ‘Dahl’ restorations would be subject to
greater loading until re-establishment of posterior
occlusal contacts occurred. This is in agreement with
other adhesive ‘Dahl’ techniques. Chana et al. (15)
reported no difference in the performance of resin-
bonded gold alloy restorations irrespective of the
method employed for interocclusal space creation.
Comparison with other reports
This study has specifically assessed the performance of
direct composite restorations placed on worn mandibular
anterior teeth. Although the use of direct composite resin
for the management of the worn anterior dentition has
been reported previously (6, 7), comparison with our
results is not possible, as these studies do not differentiate
between maxillary and mandibular restorations.
If the performance of restorations placed on worn
maxillary teeth is compared with those placed on
mandibular teeth, a lower survival rate of the mandib-
ular restorations would be expected. The mandibular
teeth have a smaller bonding area and the restorations
are likely to experience greater shear and tensile forces
in protrusive guidance. Gow and Hemmings (9) repor-
ted no bulk failures of 75 Indirect Artglass restorations
placed on the palatal aspect of worn maxillary anterior
teeth at 2 years. Hemmings et al. (6) reported the bulk
failure of 7 out of 104 (7%) direct composite restora-
tions placed on the anterior dentition at 30 months.
This is similar to the figure of 6% at 2Æ5 years reported
in this study.
Circumferential preparation
This study questions the need for pre-operative tooth
preparation prior to the placement of direct composite
restorations. The presence of a circumferential pre-
paration and the ability to provide cervical extension
of the restorations did not statistically influence the
survival of the restorations. Admittedly, this might be
due to the medium-term results of the study and the
fact that few restorations have failed. The need for
cervical extension has been questioned in other
studies. Walls (16) reported a similar finding when
he assessed porcelain onlays with buccal cervical
extensions that were used to restore worn anterior
teeth with occlusal wear predominantly. Two out of
54 porcelain onlay restorations, followed up for a
minimum of 50 months, underwent partial loss of
material in the cervical region relatively early in the
life of the restoration. These restorations were then
essentially attached only to the flat dentine surfaces.
This suggests that extensions are not necessary to aid
retention of adhesively retained onlays. Chana et al.
(15) reported that the degree of coverage of posterior
resin-bonded gold alloy restorations had no influence
on survival. The onlay type of preparation had no
mechanical retentive features, other than approxi-
mately 1–2-mm chamfer on the axial surfaces, and
these performed as well as a three-quarter type
preparation.
There may be some situations where pre-operative
tooth preparation is advised. The use of a chamfer
margin can aid the technician as it provides a finish line
for constructing indirect restorations. An enamel bevel
might be advocated for aesthetic reason as it can
N . J . P O Y S E R et al.374
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

provide a better transition between the restorative
material and adjacent tooth structure.
Patient opinion
The majority of studies related to the restoration of worn
anterior teeth with this type of technique report a high
level of patient satisfaction (6, 7, 9). This study attempted
to provide greater objective data of the patients’ opinions
regarding the direct composite build-up technique.
Choice of composite system
A single layer composite system was used and patient
satisfaction of appearance was high. Herculite XRV
composite (hybrid composite) and Optibond (dentine
bonding agent) was used as there is some evidence that
it performs significantly better than Durafill (microfill
composite) bonded with Scotchbond Multipurpose
(dentine adhesive system) (6) in the TSL environment.
Other composite systems are available on the market,
which involve the incremental build-up of the restor-
ation using different shades and opacities of composite
resin. These materials may produce a more natural
aesthetic appearance; however, they involve greater
chair-side time because of the placement and curing of
multiple increments of composite rather than a bulk of
composite as described above. There is no clinical
evidence relating to how these materials perform in a
TSL situation. The high level of satisfaction of appear-
ance might be greater in TSL patients as there is often a
dramatic change from the pre-operative status. The
patients enjoy the overall improvement and are less
concerned about the minutiae of aesthetics.
Conclusion
Composite restorations are not the same as conven-
tional extra-coronal restorations and therefore have
their own distinct advantages and disadvantages.
Direct composite restorations have distinct biological
advantages compared with crowns and for the major-
ity of patients they perform well, offer a high degree of
patient satisfaction and require an acceptable level of
maintenance.
It can be concluded from this prospective clinical trial
that direct composite restorations placed at an increased
occlusal vertical dimension are a simple and time-
efficient method of managing the worn mandibular
anterior dentition. Pre-operative circumferential pre-
paration was not required to improve the restoration
survival or patient aesthetic satisfaction. The technique
did not have a detrimental effect on temporo-mandib-
ular joint, periodontal, pulpal or periapical health. The
placement of these restorations provided an improve-
ment in the aesthetics of the teeth, a reduction in the
concern over the longevity of the worn lower anterior
teeth, and improvements with regard to sensitivity
experienced with hot or cold foods or drinks. The
patient’s accommodation to the technique was good
and the results were accompanied with a high level of
patient satisfaction. Marginal breakdown and staining
was the more common form of deterioration of these
composite-based restorations. For the majority of
patients, this was not of concern. Bulk failure and
fracture were uncommon.
Acknowledgments
The authors would like to acknowledge Miss Kelly
Romeo and Mr Paul Kensit for their involvement in this
study.
References
1. Kelleher M, Bishop K. Tooth surface loss: an overview. Br
Dent J. 1999;186:61–66.
2. Eccles JD. Tooth surface loss from abrasion, attrition and
erosion. Dent Update. 1982;35:373–381.
3. Berry DC, Poole DFG. Attrition: possible mechanisms of
compensation. J Oral Rehabil. 1976;3:201–206.
4. Dahl BL, Krogstad O, Karlsen K. An alternative treatment of
cases with advanced localised attrition. J Oral Rehabil.
1975;2:209–214.
5. Poyser NJ, Porter RW, Briggs PFA, Chana HS, Kelleher MGD.
The Dahl Concept: past, present and future. Br Dent J.
2005;198:669–676.
6. Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated
with direct composite restorations at an increased vertical
dimension: results at 30 months. J Prosthet Dent.
2000;83:287–93.
7. Redman CDJ, Hemming KW, Good JA. The survival and
clinical performance of resin-based composite restorations
used to treat localised anterior tooth wear. Br Dent J.
2003;194:566–572.
8. Smith BGN, Knight JK. An index for measuring the wear of
teeth. Br Dent J. 1984;156:435–438.
9. Gow AM, Hemmings KW. The treatment of localised anterior
tooth wear with indirect Artglass� restorations at an increased
occlusal vertical dimension. Results after two years. Eur J
Prosthodont Rest Dent. 2002;10:101–105.
D I R E C T C O M P O S I T E F O R T H E M A N D I B U L A R A N T E R I O R D E N T I T I O N 375
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376

10. Gough MB, Setchell DJ. A retrospective study of 50 treatments
using an appliance to produce localised occlusal space by
relative axial tooth movement. Br Dent J. 1999;187:134–139.
11. Firas Daoudi M, Radford JR. Use of a matrix to form directly
applied resin composite to restore worn anterior teeth. Dent
Update. 2001;28:512–514.
12. Mizrahi B. A technique for simple and aesthetic treatment of
anterior toothwear. Dent Update. 2004;31:109–114.
13. Wieczkowski G, Joynt RB, Klockowski R, Davis EL. Effects of
incremental versus bulk fill technique on resistance to cuspal
fracture of teeth restored with posterior composites. J Prosthet
Dent. 1988;60:283–287.
14. Feilzer AJ, DeGee AJ, Davidson CL. Setting stress in composite
resin in relation to the configuration of the restoration. J Dent
Res. 1987;66:1636–1639.
15. Chana H, Kelleher M, Briggs P, Hooper R. Clinical evaluation
of resin-bonded gold alloy veneers. J Prosthet Dent.
2000;83:294–300.
16. Walls AWG. The use of adhesively retained all-porcelain
veneers during the management of fractured and worn
anterior teeth: Part 2. Clinical results after 5 years of follow-
up. Br Dent J. 1995;178:337–340.
Correspondence: Neil J. Poyser, Department of Restorative Dentistry,
Maxillofacial Unit, Nottingham Univeristy Hospital NHS Trust.
Queen’s Medical Centre Campus. Derby Road, Nottingham. NG7
2UH, UK.
E-mail: [email protected]
N . J . P O Y S E R et al.376
ª 2007 Blackwell Publishing Ltd, Journal of Oral Rehabilitation 34; 361–376