Embed Size (px)
Citation preview

5/14/19
1
Lyme, Mold and Mycotoxins: When and Why You
Should Be Concerned
NationalAutismAssociationConferenceMay2019
LindseyE.Wells,ND
www.lindseywellsND.com
OUTLINE
• MoldandMycotoxins• LymeDisease• EvaluationandTesting• Treatment

5/14/19
2
MOLD
SOURCES OF MOLD • Bathrooms, Laundry rooms, Basements • Leaking pipes, poorly fitting drains, roof leaks • Walls
• Air conditioning systems • Underneath sinks
• Closets • Window Sills
• Refrigerator • Mold can be present in areas of home with
condensation, poor ventilation, window/air drafts, roofing issues, plumbing leaks, etc.
• Lower risk for mold if humidity < 60% in summer and 45% in winter

5/14/19
3
SOURCES OF MOLD
• Mattress• Pillows• Cups• Bathtoys• Teethingtoys• Rottenfoods
MOLD TOXICITY
• Thisisnotanewconceptalthoughlimitedresearch• DescribedintheOldTestament(Leviticus14)
• Warnsthatifaman’shouseiscontaminatedwithplagues,mold,andleprosythat“heshallhavetheinsideofthehousescrapedallaroundandtheplasterthattheyscrapeofftheyshallpouroutinanuncleanplaceoutsidethecity”
• During1970-1980sUSDefenseDepartmenthadconcernsregardingtheuseofmycotoxinsforbiologicalwarfare
• MayoClinicin1990madestatementthatchronicsinusinfectionsmaybeduetofungalinfectioninsteadofbacteria

5/14/19
4
MOLD TOXICITY
• In1997,Dr.RitchieShoemakerinMarylandobservedunusualsymptomsinhispatientsinatthesametimetherewasdeathofthousandsoffishinlocalenvironmentofChesapeakeBay
• DiscoveredthattheillnesswasduetothepresenceoftoxinscreatedbydinoflagellatePfiesteria
• Hefoundthatthesetoxinscouldbeboundbycertainbinders,suchasCholestyramine
• Moldtoxicitycanalsooccurfrommoldsporefragments,volatileorganiccompounds(VOCs),andothermicroorganisms.
MYCOTOXINS
• Moldsproducemycotoxinsasawaytokeepothermoldoutoftheirecologicalniche
• Mycotoxinssporescanbeinhaledintoourlungs,absorbedthroughourskinbytouch,orconsumedthroughfoodintotheGItract

5/14/19
5
BIOTOXICITY
• Microbes(i.eyeast,bacteria,spirochetes,parasites,etc)cancauseillnessduetoinfection.
• Whentreatmentisimplementedtokilloffthesemicrobes,themicrobescanreleasetoxinsinresponsetobeingkilledàbiotoxins
• Biotoxinsaredifficulttodetoxifyandcanaccumulateinthesystem
• WillaccumulateintheliverforexcretionandbeboundtobileastheymovethroughtheGItracttobeexcreted.However,theenterohepaticcirculationwillconservethebile,thereforerecyclingthebiotoxinsaswell.

5/14/19
6
BIOTOXIN PATHWAY
• Mold Toxins are ionophores • One end lipophilic (dissolves in lipids) • Other end Hydrophilic (dissolves in water)
• After inhalation, ingestion, contact the Ionophores insidiously move throughout the body
• End result is inflammatory immune response
MYCOTOXIN INFLAMMATORY RESPONSE
Mycotoxins • Enter Fat Cell
Binding releases 2nd Messenger • Activates NF Kappa B
Moves into Nucleus • Turns on gene
transcription • Cytokine production

5/14/19
7
MYCOTOXIN INFLAMMATORY RESPONSE
Cytokines• Block Leptin Receptors
Fat cells produce more Leptins • To override creating Leptin
resistance
Hypothalamus no longer makes MSH, VIP • Critical regulators of neurologic,
immunologic, endocrine function

5/14/19
8

5/14/19
9
SYMPTOMS OF MOLD TOXICITY
• Electricshocksensations• Icepickorlightingboltpains• Vibratingorpulsingsensations(especiallydownspine)
• Muscleweakness• Numbnessandtingling• Disequilibrium• Dizziness• Anxiety• MusclePain• GIsymptoms• Chesttightness
SYMPTOMS OF MOLD TOXICITY
• ChronicSinusCongestion/RecurrentSinusInfections
• BrainFog• OCD• Sleepdisturbances• Headaches• Rashes

5/14/19
10
HISTORY
Takeacarefulhealthhistoryincludingenvironmentalhistory
Whatyearwasthehousebuilt?
Istherevisiblemoldinhis/herenvironment?
Isthereamustyodorinhis/herenvironment?
Anywaterleaksorfloodinginhis/herenvironment?
Anyventilationissuesinhis/herenvironment?
Dobehaviors/symptomsdecreaseorincreaseincertainenvironments?
Anyoneinthefamilywithsimilarsymptoms?
PHYSICAL EXAM
FINDINGS
• Tenderness of sinuses on palpation • Nasal Congestion • Inflammation of turbinates • Resting tremor, (often subtle, can be
Parkinsons-like) • Cool and/or discolored hands and feet,
pallor • Unilateral weakness, especially in shoulder
muscles • Note: evaluating the ability to maintain the arms
outstretched with downward pressure on the hands and then rechecking this will usually reveal weakness

5/14/19
11
TESTING
MycotoxinUrineTest• Bestdoneaftertwoweekcourseoforalglutathione,IVglutathione,and/orSauna• Watchforworseningofsymptomsduringchallenge• Morespecificandlessinvasivetesting• Mayworsenatstartoftreatment• Nof1(testingasguide)
VisualContrastSensitivityTest• Biotoxinexposurecanimpairopticnerves• Abilitytoseepatternsimpaired• 98%whofailVCSandhave8symptomsormore,haveabiotoxinillness
• Monitorchangesovertreatmentcourse• Canbetestedonline
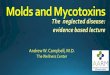
MYCOTOXIN TEST • Mycotoxinurinetestwillscreenforelevendifferentmycotoxins,from40speciesofmold
• Firstmorningurine(10mlrequired)
• Fastingfor12hoursmayincreasetheexcretionofmycotoxinsfromtheadiposetissue
Metabolite Results(ng/g creatinine) Common Range of Positive Results
Aspergillus
Aflatoxin-M1 0.00 3.5 - 20
Ochratoxin A 62.12 4 - 20
Gliotoxin 1366.35 200 - 2000
Penicillum
Sterigmatocystin 2.43 0.2 - 1.75
Mycophenolic Acid 91.04 5 - 50
Stachybotrys
Roridin E 0.00 1 - 6
Requisition # Physician Name
Patient Name Date of Collection 12/18/2018
Patient BirthDate Time of Collection 7:00 AM
Sex Print Date 12/31/2018
MycoTox Profile
11813 West 77th Street Lenexa, KS 66214 | (913) 341-8949 | Fax: (913) 341-6207 | www.GPL4U.com
Testing performed by The Great Plains Laboratory, Inc., Lenexa, Kansas. The Great Plains Laboratory has developed and determined the performance characteristics of this test. The test has not been evaluated by the U.S. Food and Drug Administration. The FDA does not currently regulate such testing.
Patient Name: Jennifer Nelson Requisition #: 640040

5/14/19
12
VISUAL CONTRAST SENSITIVITY • Nothing visible in Row E • Barely able in Row D • Test failed = biotoxicity
• Interpretation – note hand drawn checks & ovals
• Check = black and white component seen clearly
• Oval means component not seen
TOXIC by Neil Nathan, MD
TESTING • C3a–elevated• C4a–elevated• TGFbeta-1–elevated• MMP9-elevated
• VEGF–low• VIP–low• Leptin-low• MARCONsNasalSwab-
Multiple Antibiotic Resistant Coagulase Negative Staph
• Identified by nasal culture; Barrier to immune defenses; colonization (not infection)
LABMARKER NORMALRANGES
VIP 23-63(ARUPlabsonly)
MSH 35-81
MMP-9 85-332
c4a <2380
TGF-beta-1 <2380
Leptin Male:0.5-13.8;Female:1.1-27.5

5/14/19
13
TESTING
ERMItests• EnvironmentalRelativeMoldinessTest• vacuumeddustofspace(home,office,school,other)examinedfor36moldtoxins
• Thehigherthenumber,thegreatertherelativemoldburden
HERTSMI–2• HealthEffectsRosterofTypeSpecificFormsofMycotoxinsandInflammagens
• Looksfor5SpeciesofMold(alsoincludedinERMI)• Scoringsystem(www.survivingmold.com/diagnosis/hertsmi-2)• <10–SAFE• 11-15–Borderline;cleanandretest• >15–DangerousforthosewithCIRS
EvaluationbyMoldSpecialist
TREATMENT
Shoemaker and House, 2006 Neil Nathan, TOXIC
• Avoid exposure to toxic molds! • Leave environment, remediate environment, prevent re-
exposure get out • Increase Essential Fatty Acids
• 3-4 grams/day • Use Binders
• Cholestyramine • Activated Charcoal • Bentonite Clay • Chlorella • S. Boulardii • Okra
• Add Oral or Nasal Antifungals • Oral Antifungals:
• Prescription • Herbals: berberine, oil of oregano, grapefruitseed
extract, gymnema, uva ursi, pau d’arco, caprylic acid, garlic, plant tannins
• Nasal Sprays: • Xyltiol • Argentyn 23

5/14/19
14
TREATMENT
Breakupbiofilms
• Biofilmenzymes• NAC
AvoidConstipation
• Magnesium,aloe,vitaminC
Supportliveranddetoxfunction
• Glutathione,NAC,MilkThistle,Dandelion,Phosphatidylcholine,antioxidants,oilpulling,ioncleanse
Mitochondrialsupport
• CoQ10,MCToil,PQQ,antioxidants
Removeglutenifpositive;anti-inflammatory,amylose-freediet
TREATMENT
• Makesuretotest/treatforLymeorLymecoinfectionsasthiscancomplicatehealingfrommoldtoxicity
• ThereisageneticpredispositioninsusceptibleindividualstobiotoxinsincludingMoldandLyme
• ConsiderHLA-DRtesting• HLADR8andDQ• 4/3/53• 11• 12/3/52G• 14/5/52B

5/14/19
15
LYME
CDC estimates 300,000 new cases of Lyme Disease are discovered each year in the
United States.
20% of population will have tick-borne diseases and up to 35% in
some areas (like CT)
LYME DISEASE

5/14/19
16
LYME HOSTS
• > 22 species of borrelia (burgdorferi, afzelli, garinii, miyamotoi…) • Ixodes transmitted tick borne diseases
• Borrelia burgdorferi, miyamotoi, mayonii • Babesia, Ehrlichia, Barotonella, Anaplasma species
• Ixodes ticks bite a variety of hosts • Mice, rats, squirrels, shrew • Incidental hosts – humans, domesticated animals, lizards • Gestational
• Tick dispersion over wider distances • Many species of songbirds • Deer
LYME TRANSMISSION
• Tick saliva injected into dermis – it is not just about the infection (anesthetic, anticoagulant, immune modulating properties)
• Borellia Myomata - Can be transmitted without a full tick (that has NOT eaten)
• Gestational and Perinatal Transmission
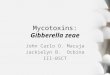
7
20
40
60
80
100
24 48 72 96
Attachment time
Trans-mission
Rate
No Guaranteed Minimum
7% transmission in under 24h
At 60h, transmission rate = 50%
Peisman J. J Clin Microbio 1987
Risk very small if < 24h attachment but not fictitious
Slide courtesy of Elizabeth L. Maloney, MD

5/14/19
17
LYME RASH
• “Typical” rash – EM (Erythema Migrans)
• Central clearing, raised expanding border
• Oval, erythematous, spreading • Painless, warm, may be itchy,
raised
• < 32% have “classic” bulls-eye rash • Any shape possible • Faint pink – deep scarlet; can be
solid coloring • Vesicular (especially on legs) • Check skin folds, hairy areas
LYME SYMPTOMS
BORRELIA• Flu-likesymptoms• Bulls-eyerash(erythemamigrans)• Nervepain• Peripheralneuropathy• Vertigo• Headaches(wholeheadhurts)• Neckpain• Jointpain• Cardiacsymptoms

5/14/19
18
BARTONELLA SYMPTOMS
• Sensitivitytonoise/light/chemicals/smells• Paininsolesoffeet• Sensationofvibration/trembling• Numbness/tingling• Joint/musclepain• Emotionalinstability• Anxiety,panicattacks• Headaches(locatedinbackofhead)• GIsymptoms• Pelvic/bladdersymptoms
BABESIA SYMPTOMS
• Nightsweats• Shortnessofbreath(”airhunger”)• Headaches(frontal)• Cognitivedysfunction• Hallucinations• Cognitiveimpairment

5/14/19
19
EHRLICHIA SYMPTOMS
• Headache • Myalgias • Malaise • Vomiting • Cough, pneumonitis • Repetitive stress injuries
• Signs:
• Initial leukopenia, thrombocytopenia • Then leukocytosis, elevated liver
enzymes
PHYSICAL EXAM
• ErythemaMigrans–BORRELIA• Striaethatblanches–BARTONELLA
• SwollenLymphNodes• Heartrhythmirregularities• Facialpalsyandneuropathy• Swellingofjoints

5/14/19
20
TESTING
• Testing (not positive for several weeks after tick bite) • Extended western blot (18, 23-25, 31, 34, 37, 39, 83, 93) • Coinfections (babesia, bartonella, ehrlichia) • CD57 (decreased levels, inaccurate, not sensitive) • PCR (poor sensitivity < 30%) • Inflammatory and immune markers (ANA, ESR, hsCRP) • Metabolic markers (homocysteine, B12 (MMA), plasma
zinc, RBC magnesium, T3, T4, thyroid antibodies) • Mitochondrial markers (carnitine, ammonia, lactate, CK,
amino acids, urine organic acids) • Other germs (mycoplasma, viruses, strep and yeast) • Intracellular infection – VEGF, TGF beta, C3a, C4a)
TREATMENT
InitialtreatmentforLyme(4-6weeksoforalagent)• Doxycycline(preferredantibiotic)• Amoxicillin• Cefuroxime• Azithromycin
BabesiaTreatment• AtovaquoneandAzithromycinORClindamycinandQuinine(CDC2015TreatmentGuidelines)
• Bioavailabilityofatovaquoneislowandvariableandishighlydependentonformulationanddiet
• Atovaquoneshouldbetakenwithfattyfood• Withfood,bioavailabilityisapproximately47%• Withoutfood,bioavailabilityis23%
EhrlichiaTreatment• DoxycyclineandRifampin(Dumler2009)
BartonellaTreatment• Treatment-nosingletreatmentiseffective;(Spach2015)• RifampinandBactrim;RifampinandAzithromycin;BactrimandAzithromycin

5/14/19
21
LYME TREATMENT
• JapaneseKnotweed• Cat’sClaw• Teasel• Andrographis• Biocidin• Samento• Banderol• Cumanda• IFYOUFINDATICK–CONSIDERLEDUM30C(HomeopathicRemedy)
LYME CO-INFECTION TREATMENT
Babesia• Cryptolepis• ChineseSkullcap• Bidenspilosa• Artemisinin• RedSage• SidaAcuta
Bartonella• JapaneseKnotweed• EGCGwithquercetin• L-arginine• Cordyceps• SidaAcuta• RedRoot• Argentyn23• A-Bart
Ehrlichia• Cordyceps• Redsage• Houttuynia• ChineseSkullcap• Astragalus• Kudzu• Quercetin

5/14/19
22
HERXHEIMER REACTION
Evaluating Undesirable Outcomes
Correct Diagnosis?
Right Rx for Lyme?
Jarisch-Herxheimer?
Other possibilities …
Other tick-borne disease?
Yes No
Yes No
Lyme + Co-infection?
Unexpected Course
50Slide courtesy of Elizabeth Maloney, MD
Select Appropriate
Antibiotic
• Herxheimer” reaction ~20% of patients
• First described with PCN treatment of syphilis
• Intensification of baseline symptoms
• Variable duration, onset often within hours
• HerxSupport:• Epsomsaltbaths• Activatedcharcoal• Burburpinella• Alkalization• Otherbinders
Pound MW. J Clin Pharm Thera. 2005

5/14/19
23
NUTRITION
• Remove sugars, processed food, GFCF
• Stevia – antimicrobial benefits
• Pomegranate Juice – antimicrobial benefits
• Increase antimicrobial spices and herbs in diet
• Oregano, cinnamon, clove, garlic, ginger, rosemary, etc.
• Add bone broth, fermented foods
• Increase foods high in antioxidants (berries, nuts, green leafy vegetables, etc.)
PREVENTION • KnowEndemicareas• ClothingProtection
• Tuckinpants• Hats• Longsleeves
• UseNaturalTickSpray• Recipe:
• 25dropsGeraniumessentialoil• 10dropsCitronellaessentialoil• 5dropsLemonessentialOil• 2ozofWitchHazel• 2ozWater
• Makesuretodotickchecks!

5/14/19
24
IMPORTANCE OF PROPER
TREATMENT CIRSLymeandLymeCo-Infections
MoldToxicity
Mycoplasma
Viruses
Strep
CHRONIC INFLAMMATORY RESPONSE SYNDROME
Toxinsand/ormicrobes
StimulatedImmuneResponse
INFLAMMATION

5/14/19
25
CHRONIC INFLAMMATORY
RESPONSE SYNDROME
• Symptomsin6clusters
• Commonlyupto10
TREATMENT

5/14/19
26
CLOSING REMARKS
ThereisarelationshipbetweenLymeandMoldToxicity
Multisystemtreatmentisneeded
Treatthewholechildandthewholeillness(yourNof1)
IdentifyunderlyingproblemsbylookingatINDIVIDUALhistory,physicalexamcluesandlaboratorydata
Thinkenvironmentalexposures(i.emoldandLyme)whennotmakingprogresswithtreatmentasexpected
Besttoincludeherbalsandsupplementsintreatmentplanforsuccessfullongtermoutcomes!
THANK YOU!
www.lindseywellsnd.com
Instagram:@lindseywellsndFacebook:LindseyWellsND,LLC