Embed Size (px)
Citation preview

VILNIUS UNIVERSITY HOSPITALSANTARISKIU KLINIKOS
Common variable Common variable immunodeficiency immunodeficiency
in adultsin adultsK. Cerniauskas, A. Blaziene K. Cerniauskas, A. Blaziene
Common variable immunodeficiency - Common variable immunodeficiency - most prevalent of the primary most prevalent of the primary immunodeficiency disorders.immunodeficiency disorders.
RReeduction in serum levels of both IgG duction in serum levels of both IgG and IgA, with or without low IgM.and IgA, with or without low IgM.
Recurrent bacterial sinopulmonary Recurrent bacterial sinopulmonary infections, which led to complications, infections, which led to complications, especially pulmonary damage.especially pulmonary damage.
Definition
PrevalencePrevalence
1-2 / 100 000 1-2 / 100 000 Lithuanian population 3.5 mln.Lithuanian population 3.5 mln. Expected number of Expected number of patientspatients 3 35-705-70.. Number of diagnosed Number of diagnosed CVID CVID is 5 is 5
cases in our clinic.cases in our clinic.

ExperienceExperience
From 1998 From 1998 toto 2006. 2006. FiveFive cases (3 males, 2 females). cases (3 males, 2 females). Diagnosis made between 23 - 48Diagnosis made between 23 - 48
yearyearss of life of life.. An average An average diagnostic diagnostic delay ~ delay ~ 7 7 y.y.

Which specialist Which specialist suspectedsuspected hypogammaglobulinemiahypogammaglobulinemia??
1 – haematolog1 – haematologistist 1 – rheumatolog1 – rheumatologistist 33 – pulmonolog – pulmonologistist
Where is primary physician ???Where is primary physician ???

OnsetOnset
In 4 cases disease manifested with In 4 cases disease manifested with recurrent infections of upper and recurrent infections of upper and lower respiratory tractlower respiratory tract..
In 1 In 1 casecase recurrent infections of recurrent infections of respiratory tract were associated respiratory tract were associated with benign lymphadenopathywith benign lymphadenopathy..
In 1 case In 1 case -- enterogenic reactive enterogenic reactive arthritis and urinary tract infection arthritis and urinary tract infection ..
Laboratory testsLaboratory tests
- Low level of IgG, IgA and IgM was - Low level of IgG, IgA and IgM was foundfound..
- Number and function of T - Number and function of T lymphocytes – Nlymphocytes – N..
- Number of B lymphocytes – 7-9 %- Number of B lymphocytes – 7-9 %..

ComplicationsComplications
Bronchiectasis Bronchiectasis waswas detected in 3 detected in 3 casescases ( (byby CT) CT)..
Amyloidosis of AA type in 3 cases Amyloidosis of AA type in 3 cases (renal or gum biopsy).(renal or gum biopsy).
1 1 death in 5th y after CVIDdeath in 5th y after CVID was was revealed.revealed.
Associated diseasesAssociated diseases
Benign lymphadenopathy – 1Benign lymphadenopathy – 1 Reactive arthritis – 2Reactive arthritis – 2 COPD – 1COPD – 1 Rhinosinusitis – 1Rhinosinusitis – 1
TreatmentTreatment
Substitutional therapy with Substitutional therapy with intravenous immunoglobulin intravenous immunoglobulin (Endobulin) was initiated in(Endobulin) was initiated in 2 cases. 2 cases.
Concomitant pathology treated in Concomitant pathology treated in ordinary way. ordinary way.
Exacerbation of infections were Exacerbation of infections were treated with antibiotics.treated with antibiotics.
CasesCases

Case 1Case 1
Patient P.S., male, 38 years old. Rhinosinusitis - since 9 years old. Subfebrile fever - 12 y. Loss of weight - 16 y. Recurrent infections of the respiratory
tract - since 22 years (bronchitis 3 times a year).
Bronchiectasis was diagnosed - 29 y. Dyspnea, weakness, often exacerbations of
bronchiectasis were presenting.
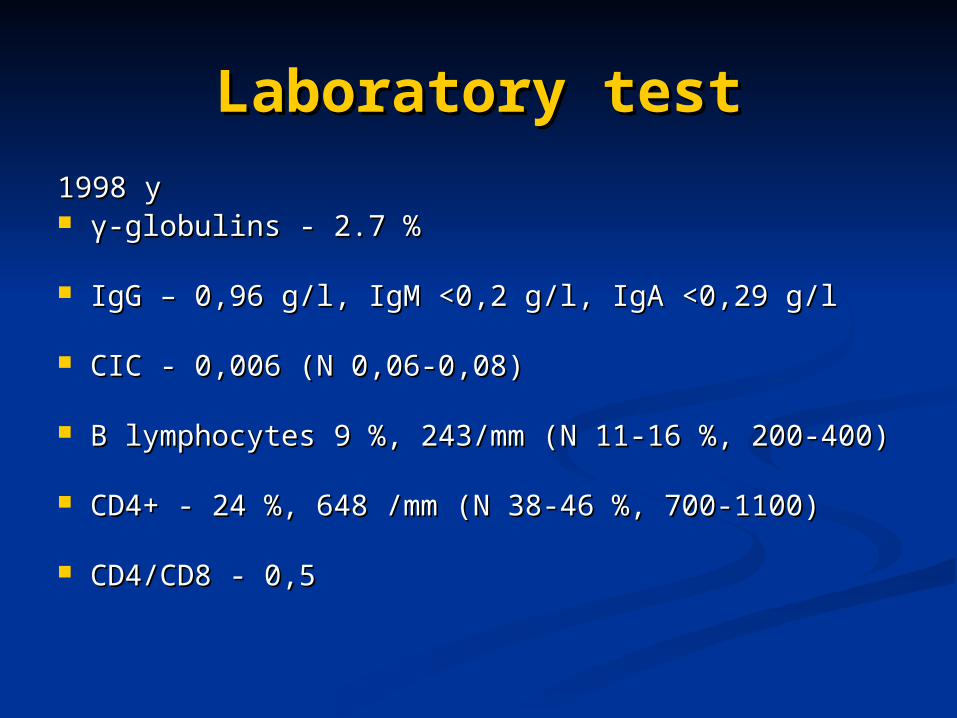
Laboratory testLaboratory test
1998 y1998 y γγ-globulins -globulins - 2.7 - 2.7 %%
IgGIgG – – 0,960,96 g/l g/l,, IgM <0,2 g IgM <0,2 g//ll,, IgA <0,29 g/l IgA <0,29 g/l
CICICC - - 0,0060,006 ((N N 0,06-0,08)0,06-0,08)
B lymphocytesB lymphocytes 9 9 %,%, 243/mm ( 243/mm (N N 11-16 11-16 %%, 200-400), 200-400)
CD4+ CD4+ - - 24 24 %%, 648 , 648 //mmmm ((N N 38-46 38-46 %,%, 700-1100) 700-1100)
CD4/CD8CD4/CD8 - - 0,5 0,5
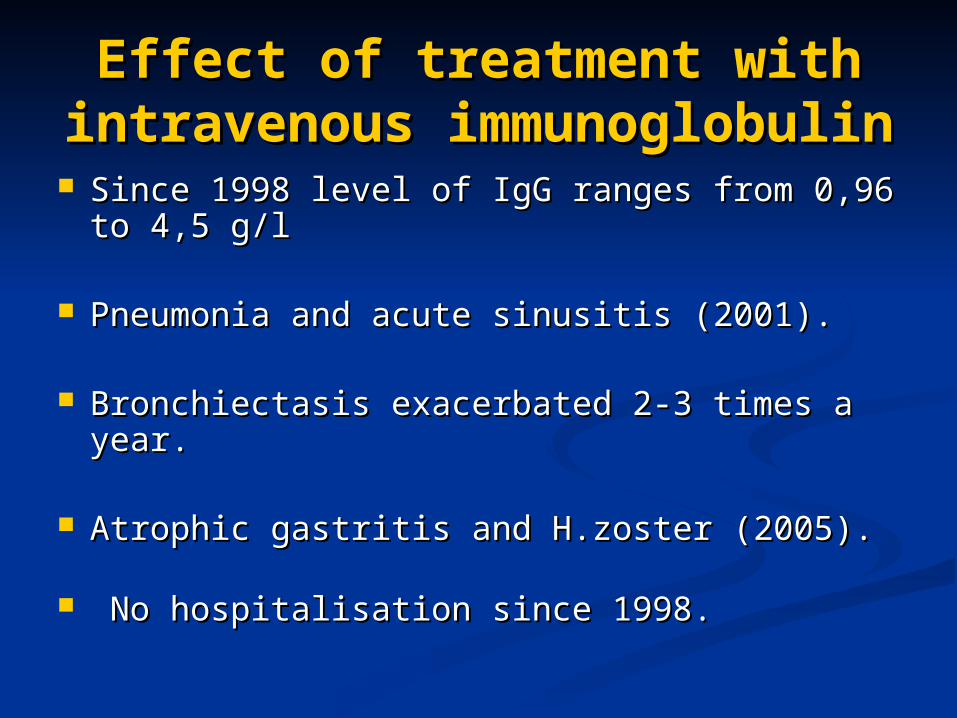
Effect Effect of tof treatment with reatment with intravenous intravenous
immunoglobulinimmunoglobulin Since 1998 level of Since 1998 level of IgG IgG ranges fromranges from 0,96 0,96 toto
44,,55 g/l g/l
Pneumonia and acute sinusitis (Pneumonia and acute sinusitis (20012001).).
Bronchiectasis exacerbated 2-3 times a year. Bronchiectasis exacerbated 2-3 times a year.
Atrophic gastritis and H.zoster (Atrophic gastritis and H.zoster (20052005). ).
No hospitalisation since 1998.No hospitalisation since 1998.
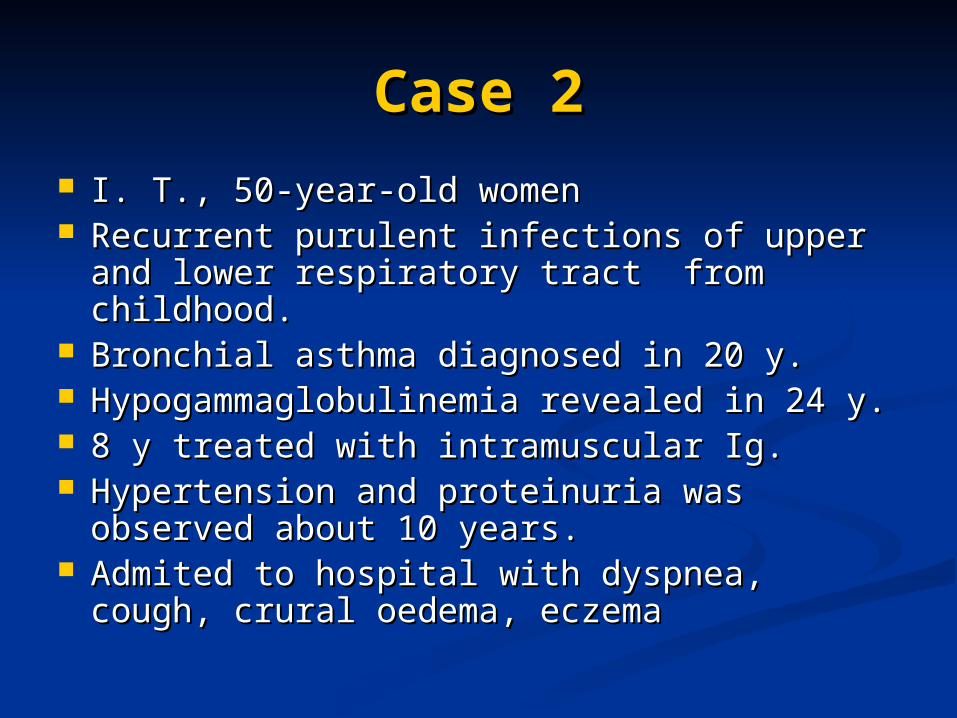
Case 2Case 2 I. T., 50I. T., 50--year-old womenyear-old women Recurrent purulent infections of upper and Recurrent purulent infections of upper and
lower respiratory tract from childhood. lower respiratory tract from childhood. Bronchial asthma diagnosed in 20 y.Bronchial asthma diagnosed in 20 y. Hypogammaglobulinemia revealed in 24 y. Hypogammaglobulinemia revealed in 24 y. 8 y treated with intramuscular Ig8 y treated with intramuscular Ig.. Hypertension and proteinuria was Hypertension and proteinuria was
observed about 10 years.observed about 10 years. Admited to hospital with dyspnea, cough, Admited to hospital with dyspnea, cough,
crural oedema, eczemacrural oedema, eczema
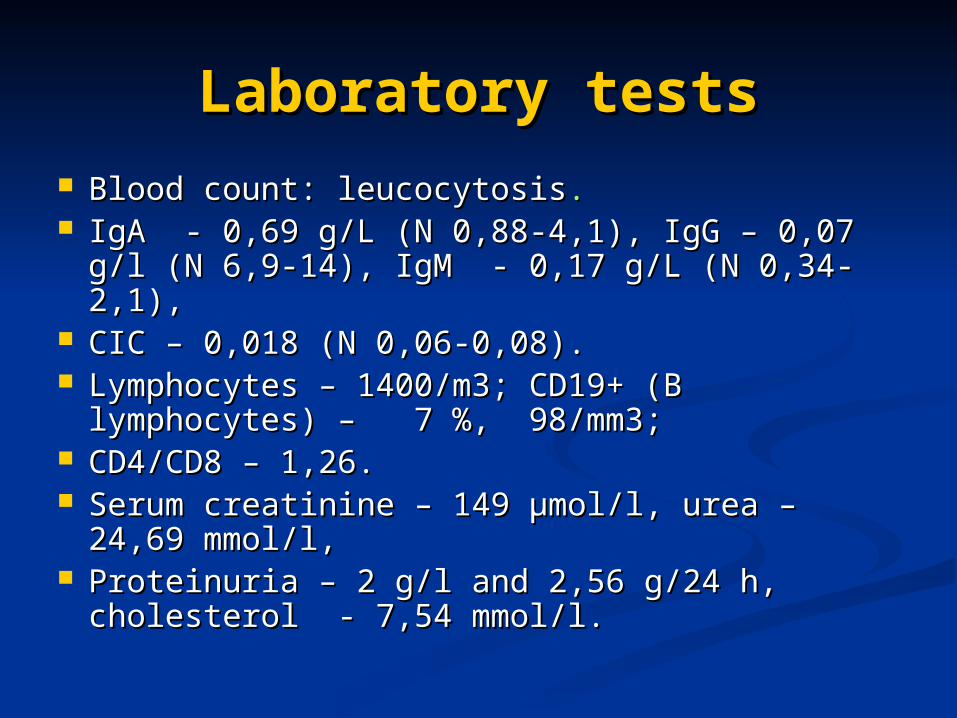
Laboratory testsLaboratory tests Blood countBlood count: leucocytosis: leucocytosis.. IgA - 0IgA - 0,,69 g/L 69 g/L ((N N 0,88-4,1)0,88-4,1), IgG – 0, IgG – 0,,07 g/l 07 g/l
((N N 6,9-14)6,9-14), IgM - 0, IgM - 0,,17 g/L 17 g/L ((N N 0,34-2,1), 0,34-2,1), CIC CIC – 0– 0,,018 018 ((N N 0,06-0,08). 0,06-0,08). LymphocytesLymphocytes – 1400/m3; CD19+ (B – 1400/m3; CD19+ (B
lymphocyteslymphocytes) – ) – 7 %, 7 %, 98/mm3; 98/mm3; CD4/CD8 – 1,26. CD4/CD8 – 1,26. Serum creatinine – 149 μmol/l, urea – 24Serum creatinine – 149 μmol/l, urea – 24,,69 69
mmol/l, mmol/l, Proteinuria – 2 g/l and 2,56 g/24 h, Proteinuria – 2 g/l and 2,56 g/24 h,
cholesterol - 7,54 mmol/l.cholesterol - 7,54 mmol/l.

Imaging studies and Imaging studies and biopsy biopsy
CT revealed pneumofibrosis, atelectasis CT revealed pneumofibrosis, atelectasis of S10/9, mediastinal lymphadenopathy of S10/9, mediastinal lymphadenopathy and pleural effusion.and pleural effusion.
PPleural fluid was transudate, specific or leural fluid was transudate, specific or atypical cells were absent (flow atypical cells were absent (flow cytometry)cytometry)..
Renal ultrasound showed parenchymas Renal ultrasound showed parenchymas changes typical to chronic renal disease. changes typical to chronic renal disease.
Renal biopsy elicited amyloidosis (AA). Renal biopsy elicited amyloidosis (AA).
CommentComment
No bronchiectasis in the presents of No bronchiectasis in the presents of amyloidosis.amyloidosis.
Long outlive without treatment.Long outlive without treatment.

Case 3Case 3
J.M., female, 27 years oldJ.M., female, 27 years old.. Gastrointestinal infection 26 y Gastrointestinal infection 26 y
(salmoneliosis?)(salmoneliosis?).. Urinary tract infectionsUrinary tract infections.. Admited to hospital with pain and Admited to hospital with pain and
swelling in the left knee, diarrheaswelling in the left knee, diarrhea..
Laboratory testLaboratory test
Blood count - iron deficiency anemiaBlood count - iron deficiency anemia.. CRP - 136 mg/lCRP - 136 mg/l.. RF RF -- N N.. Faeces culture Faeces culture -- Campylobacter Campylobacter.. γγ-globulin – 5-globulin – 5,,1 %1 %.. IgG < 1IgG < 1,,7 g/l, IgA <07 g/l, IgA <0,,24 g/l, IgM – 24 g/l, IgM –
11,,7 g/l7 g/l.. B lymphocytes B lymphocytes -- N N..

Imaging testsImaging tests
Chest x-ray - NChest x-ray - N Chest CT - N.Chest CT - N. Sonography and x-ray of the knee: Sonography and x-ray of the knee:
arthritis.arthritis.
CommentComment
Enterogenic reactive arthritis or Enterogenic reactive arthritis or arthritis associated with primary arthritis associated with primary agammaglobulinemia?agammaglobulinemia?
Case Case 44
G.J., male, 27 y.G.J., male, 27 y. RRecurrent infections of ecurrent infections of the the respiratory respiratory
tract since childhoodtract since childhood.. SSevere pneumonias occured since 21evere pneumonias occured since 21yy.. PPleuritisleuritis three times since 22 y three times since 22 y.. HHypogammaglobulinemia ypogammaglobulinemia iin 23 y n 23 y ReactiveReactive arthritis was suspected arthritis was suspected in 25 in 25
y. y.
Case 4 (cont.)Case 4 (cont.)
At the age of 27 y At the age of 27 y admited to admited to hospital because ofhospital because of fever, cough, fever, cough, diarrhdiarrhooea, pain of shoulders and ea, pain of shoulders and kneesknees,, crural oedema. crural oedema.
Chest CChest CT elicited bilateral T elicited bilateral bronchiectasisbronchiectasis..
AAmyloidosis was confirmed by gummyloidosis was confirmed by gum and gutand gut biopsy biopsy

Laboratory testsLaboratory tests
IgG<1,35 g/l, IgM-0,17 g/l, IgA<0,23 g/l. IgG<1,35 g/l, IgM-0,17 g/l, IgA<0,23 g/l. CD19+ - 8 %CD19+ - 8 %,, CD4+ - 15 %, CD4/CD8 - CD4+ - 15 %, CD4/CD8 -
00,,19.19. Blood count Blood count - - leucocytosisleucocytosis. . CRP – 72 mg/l.CRP – 72 mg/l. HypoproteinemiaHypoproteinemia (30,9 g/l), (30,9 g/l),
hypoalbuminaemia (14,8 g/l). hypoalbuminaemia (14,8 g/l). PProteinuria (8,4 g/l, 21,42 g/24 h), granular roteinuria (8,4 g/l, 21,42 g/24 h), granular
casts in urine. casts in urine. Urea and creatinin values were normal. Urea and creatinin values were normal.
CommentComment
4 years without treatment were 4 years without treatment were crucial for the development of crucial for the development of complicationscomplications..
Patient died 2 y after initiation of Patient died 2 y after initiation of replacement therapyreplacement therapy..
Problem?Problem?
Long delay in diagnosis and Long delay in diagnosis and treatment of CVID.treatment of CVID.