Embed Size (px)
Citation preview

British Journal of Plastic Surgery (1985) 38,23C-233 0 1985 The Trustees of British Association of Plastic Surgeons
Vertical abdominal fasciocutaneous flaps in the reconstruction of chest wall defects
Y. MARUYAMA, K. OHNISHI and C. C. CHUNG
Department of Plastic and Reconstructive Surgery, Toho University Hospital, Tokyo, Japan
Summary-The use of a vertical abdominal fasciocutaneous flap in the reconstruction of chest wall defects is described. The technique has been successfully used in 8 patients and the advantages of such a fasciocutaneous flap in chest wall reconstructions are emphasised.
The effects of previous surgery and/or radiotherapy for carcinoma of the breast, along with locally recurrent tumour, may require extensive resection of the chest wall including the soft tissues, underly- ing bone and pleura. The repair of these com- plicated excisional defects demands an air-tight closure of the skin and subcutaneous tissues, possibly with reconstruction of a skeletal layer.
Numerous flaps can be designed, depending upon the defect to be corrected and ingenuity of the surgeon. The blood supply should be autonomous and axial for reliability: primary healing must be the goal and a one-stage reconstruction is highly desirable in patients who may already be debilitated.
Muscle and musculocutaneous flaps, because of their versatility and reliability, have become ex- tremely popular and the rectus abdominis muscu- locutaneous flap is one of the most widely used flaps in anterior chest wall reconstruction. How- ever the rectus abdominis is an important constitu- ent of the abdominal musculature and its loss may severely weaken the abdominal wall and so limit the usefulness of this particular myocutaneous flap (Mathes and Nahai, 1982).
The purpose of this paper is to describe the vertical abdominal fasciocutaneous flap in re- construction of chest wall defects. In this flap the anterior rectus sheath is taken but not the rectus muscle.
Procedure After resection of the tumour the defect is measured and a suitable flap is designed with its base situated
superiorly (Figs. lA, B). The elevation of the flap is started distally and the deep fascia overlying the rectus abdominis is included in the flap (Fig. 1C). It is safe to raise the flap with a base to length ratio of 1:3 or more. In the proximal part of the dissection, one should preserve and include all the perforating vessels at the level of the costal margin.
The flap is transposed into the excisional defect and any excess skin is removed (Fig. 1D). The donor defect on the abdominal wall is usually closed primarily without any difficulty after suit- able undermining.
To date, 8 patients with major excisional defects of the anterior chest wall have been successfully treated with a vertical abdominal fasciocutaneous flap.
This technique for chest wall reconstruction is a single stage procedure and can be used as the primary breast reconstruction (Fig. 2).
As the flap is raised without the rectus abdominis muscular component there is no significant motor disability and there is no ventral hernia or ab- dominal weakness because the rectus muscle and posterior rectus sheath remain intact. The patient does not need to be turned over on the operating table and the abdominal donor defect can be closed primarily.
Cormack and Lamberty (1983) stated that skin flaps raised to include the deep fascia in the expectation of increasing reliability, safety and length to width ratio, must not be raised in a random manner but must be planned to take into account the scientific evidence for the anatomical basis of the fasciocutaneous flaps. The vascular
230

VERTICAL ABDOMlNAL FASCIOCUTANEOUS FLAPS 23
Fig. 1
Figure I-(A) Design of the vertical abdominal fasciocutaneous flap and its arc of rotation. (B) At operation the lung is exposed in the excisional defect after resection of the recurrent breast carcinoma and chest wall. The dissection of the fasciocutaneous flap is complete. (C) The fasciocutaneous flap is raised to show that the underlying rectus muscle is left intact. (D) Result after completion of the repair.

232 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 2
Figure 2-Defect after radical primary surgery for breast cancer. Closed by immediate vertical abdominal fasciocutaneous flap.
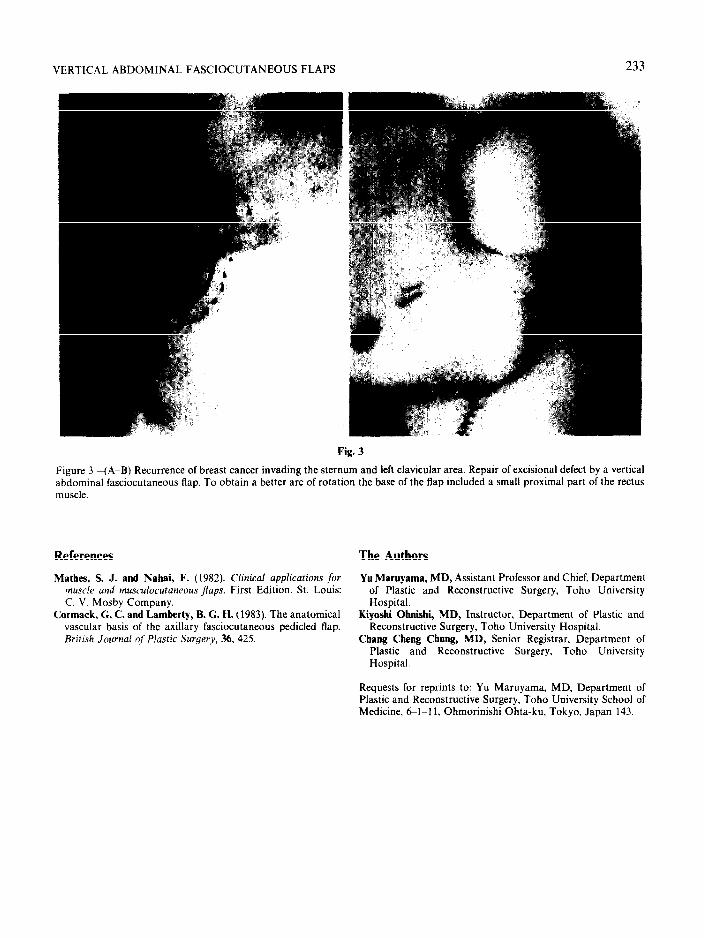
supply of this flap comes from the superior epigas- margin, one can obtain a longer arc of rotation of tric vessels, which supply the cutaneous tissues and this flap (Fig. 3A, B). fascia of the upper abdomen through perforating In our series of repairs using the vertical ab- vessels: one or two perforating vessels from below dominal fasciocutaneous flap we have raised flaps the costal margin should be included in the flap and extending as far distally as the lower third of the if one includes a small part of the rectus muscle and abdomen without any evidence of circulatory em- the superior epigastric vessels at the level of costal barrassment or necrosis.
VERTICAL ABDOMINAL FASCIOCUTANEOUS FLAPS 233
F
Figure 3-(A-B) Recurrence of breast cancer invading the stern abdominal fasciocutaneous flap. To obtain a better arc of rotatil muscle
References
Mathes, S. J. and Nahei, F. (1982). Clinica/ applications for muscle and musculocutaneous ~4aps. First Edition. St. Louis: C. V. Mosby Company.
Cormack. G. C. and Lamberty, B. G. H. (1983). The anatomical vascular basis of the axillary fasciocutaneous pedicled flap. British Journal of Plastic Surgery, 36. 425.
-- .-
ig. 3
urn and left clavicular area. Repair of excisional defect by a vertical on the base of the flap included a small proximal part of the rectus
The Authors
Yu Mnruyama, MD, Assistant Professor and Chief, Department of Plastic and Reconstructive Surgery, Toho University Hospital.
Kiyoshi Ohnishi, MD, Instructor, Department of Plastic and Reconstructive Surgery, Toho University Hospital.
Chang Cheng Chung, MD, Senior Registrar, Department of Plastic and Reconstructive Surgery, Toho University Hospital.
Requests for reprints to: Yu Maruyama, MD, Department of Plastic and Reconstructive Surgery, Toho University School of Medicine, 61-I I, Ohmorinishi Ohta-ku, Tokyo. Japan 143.