-
λ~:(, 1ft. 4‘1*있챔샤,~ f깐 갚 i:1\ 23 장 찌, 4 싸 pp. 626 - 635, 1987
.Journal 01 Korean Radiological Society , 23(4) 626-635, 1987
〈국문초록〉
Venographic Features of Varicocele
Seoung Oh Yang, M .D., Myung Joon Kim , M.D. , In WOO Ro ,
M.D.
Department of Radiology, Capital Armed Forces Ceneral
Hospital
정계정맥류의 정맥조영술 소견
국군수도영원 방사선과
양승오·김명준·노인우
정계정맥류에 대한 원인 및 불입증을 유말하는 기전은 많은 가설이 있을 뿐 정확한 규명응 아직
없다. 저자들은 최근 l 년간 정계정액류의 원인과 발생기선을 연쿠하고자 국군수도벙원에 업원한
좌측의 정계정액류 환자 30 예에 대해 치료전의 정맥조영술을 시행하여 그 방사선학척 소켠에 대
한 다음의 결과를 얻었다.
l. 좌측신정맥 조영술상 10 예 (33 %)에서 신정맥 압박현상과 7 예 (23 %)에서유샤소견을판찰
했£며 , 29 예 (97%)에서 내정계정맥으로의 수통적 역류가 보였는데 이 역류의 정도는 정계정백류
의 임상등급과 연판성이 있었다.
2. 선택적 좌측 내정제정맥 조영숭상 내정계정액의 수는 18 예 (60 % )에서 l 개였고 냐머지는 2
개이상이었으며, 그 확장정도는 임상등급과 유판하였으며 측부 문합의 위치는 상부 골반부외 외측
(LIII)파 상부 요추부의 내외측 (L I. M])에 많음을 알 수 있었다.
3. 좌측 총장골 정맥 조영숭상 총장골 정액 압박현상이 11 예 (37 %)에서 , 유사소견운 8 예 (
27
%)에서 관찰되었으며 이중에 신정액 앙박현상이 동반된 경우가 13 예 (43 %)였다.
4. 대퇴정액을 통한 내정계정액의 선택은 20 예 (67%)에서 용이하였고. 6 예에서는 카테타의 변
형등이 필요했으며 .4 예에서는 직각의 혈관주행띠l운에 곤란하였마
5. 2 예의 조영제 유출과 1 예의 총장골 정액의 경련이 있었으냐 임상척인 의의는 없었다.
6. 정계정액류의 진단과 치료에 있어서 정액조영술은 정계정맥류의 해부학적 i녕변파 형성기천을
파의L하게 하여 경피석 색전숭이냐 수술방법의 결정에 중요한 역 할을 할 수 있다
The results 01 a prospective study 01 30 patients with scrotal
varicocele on the left side during the past
12 months are presented
8y means 01 preoperative venography 01 the renal , internal
spermatic and common i1 iac veins, the e tiologic
id entilication is possible. Varicoce le could be distinguished
in which the cause arises in the internal spermatic
이 논문은 1987 년 5 월 9 일에 접수하여 1987 년 6월 4 일에 채택되었음.
Recei vecl lVlay 9 , acceptecl June 4 , 1987
- 626
-
Seoung Oh Yang, et al.: Venograph ic Features of Varicoc
ele-
vein and/or proximal nutcracker phenomenon (by compression 01
ISV between the aorta and superior mesenteric
artery) and/or distal nutcracker phenomenon (by obstruction 01
common iliac vein)
Use 01 preoperative venography is essential to estabilish the
etiology and anatomy 01 the lesion and its
proper selection 01 treatment methods including subsequent coil
embo lization
Key Words: Venography, etiologic evaluation, Varicocele
Spermatic venography was introduced by Ah1berg et al. in 1966.
1.2) Using this diagnostic method the reflux into the interna1
spermatic vein(ISV) was suggested to be characteristic of
varicoce1e , but a clearer explication of the etio1ogy of
varicoce1e shou1d be investigat ed. 3 , 4) The re1ationship between
ma1e subfer-tility and varicoce1e of the testis has been well
documented. S , 6 , 7 ,B) More recent1y , attention has been
directed at the subclinica1 varicoce1e, which can be conclusive1y
demonstrated on1y by spermatic venography.9)
We present our experience with 30 patients who underwent
preoperative or preemboliza tiona1 venography of the rena1 ,
interna1 sper matic , and common iliac veins to determine possib1e
causes of varicoce1e and venous ar-chitecture between May 1986 and
April1987 , This report dea1s primari1y with the detai1ed
radio1ogic aspects of the procedure . The ex-perience of
percutaneous spermatic vein em bolization, when indicated , and
postocclusion response will be covered in a separate report.
Materials and Methods
A prospective study of 30 consecutive pa-tients during the past
12 months with a vari-coce1e on the 1eft side whose age ranged from
20 to 26 years has been done. The clinica1 size of varicoce1e was
classified as grade 1 varicoce1e pa1pab1e on1y during Va1sa1va ’s
maneuver, grade 2 - varicoce1e visib1e on1y during Va1sa1va ’s
maneuver , and grade 3 - varicoce1e visib1e without Va1sa1va ’s
maneuver. 10)
With the transfemora1 venographic techni-que 25-30 m1 Hypaque
50% were injected for
627
3 sec into the 1eft rena1 vein through cobra catheter with
performing the Va1sa1va ’s maneuver. The initial fi1ms were made to
deter-mine wheather passive reflux into the ISV or fill-ing of the
intrarena1 veins and other collatera1s occurred. Reflux out of the
rena1 vein into the vena cava , anomalies of the rena1 vein itse1f
and a proxima1 nutcracker phenomenon were assessed.
Then se1ective venography of the ISV was done using 15 m1
Hypaque for 2 sec through suitab1e catheter. Films were made to
show the ISV and possib1e collatera1s and the scrota1 varicocele
.
Last1y , venography of the 1eft common i1-iac vein was performed
to eva1uate a dista1 nutcracker phenomenon with same technique as
1eft rena1 venography.
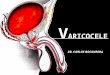
In order to classify reflux, mu1tiplicity , and anastomoses of
the ISV s we devide the ISV into six subsegments as shown in Fig. 5
(A) according to Marsman.9) We distinguish six grades of spermatic
venous reflux during 1eft rena1 venography: 0 = no reflux or reflux
down into the crania11umbar subsegment of the ISV shorter than the
height of the L-3 vertebra1 body; 1 reflux down into the crania1
1um-bar subsegment 10nger than the height of L-3; 11 reflux down
into the cauda1 1umbar subsegment; 111 = reflux down into the
crania1 pe1vic subsegment; IV = reflux down into the cauda1 pe1vic
subsegment; V = reflux down into or beyond the inguina1 segment of
the ISV.
Mu1tip1icity of the ISV is distinguished from the presence of
small paralle1 anastomo-tic veins. In case of thicker paralle1
veins aris ing from the rena1 vein , we speak of mu1tip1e
-
-大훼)jJ(!j‘t짧뽑작l샘참“ 짜23卷 짜 4 ~iJi. 1987-
ISVs. Anastomoses that run medially or
laterally from the ISV are often visualized. We
used topographic classification for anastomo-
ses based on two criteria. First, we record wheather an
anastomosis joins the ISV
medially or laterally(M or L). Secondly, we record the level at
which the anastomosis joins
the ISV (1 to V). Consequently, we classify medial and lateral
anastomoses from M 1 to
L V.
Results
(1) F indings of left renal venography
(Table 1,2)
1n 10 patients a severe to moderate prox-
imal nutcracker phenomenon (PNP) was observed with obvious
compression at the
level of the junction between the aorta and
superior mesenteric artery(SMA) by the “ pm-ching" effect (Fig.
1). In 7 patients a similar
Table 1. Findings of Left Renal Venography (N = 30)
Findings No (%)
Proximal nutcracker phenomenon 10 (33)
Suspicious PNP 7 (23)
Passive reflux into the ISV 29 (97)
Proximal renospermatic shunt 6 (20)
Circumaortic renal vein l ( 3)
Table 2. Clinical and Venographic Grading and Degree of
the ISV ’s Dilatation ‘
Venographic Reflux ISV’s Dilatation
Clinical Grade 0 1 II III IV V min. mod. severe
CJ
。ι
?l
6
9
2
η
-4
2
6
6
1
-7
2
5
-7
2
4
1
7
14
?“
。ι
[D
-2
l
3
-1
-1
m
페 씨
떼
(
(
(
(
。a
nι --
k
k
ιx 때
겐 3
…m 야
mε me
g T
A B C
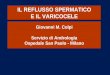
Fig. 1. Proximal nutcracker phenomenon (Severe case) A. Inferior
vena cavogram of the case . B. Left renal venogram shows passive
reflux into the ISV and paravertebral collateral veins and
hemiazygos continuation (arrows) of the left renal vein without
drainage into IVC C. Subtraction film of A,B to demonstrate the
compression site (arrows) made by SMA/Aortic angle
- 628
-
-Seollng Oh Yang. et a l.: Venographic Featllres of
Varicocele
but less pronounced minimal compreS5ion was observed. In 9
patients the adrenal vein and paravertebral plexus in 10 patients
and hemiazygos continuation of the left renal vein in 11 patients
were demonstrated.
Passive reflux into the ISV was seen in 29 patients(97%). Six
out of 11 patients with grade 3 varicocele revealed venographic
reflux of grade V.
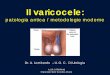
The number of the ISV is single in 18 pa-tients and multiple
(mainly two) in 12 patients with various collaterals including
vertical anastomosis. Renospermatic shunt is seen in 6 patients
(Fig. 2) . In two of these 6 patients , PNP was present , too.
Circumaortic venous ring is shown with renospermatic shunt in
one patient (Fig. 3).
(2) Findings of selective internal spermatic venography (Table
2, 3)
Degree of the ISV ’s dilatation is deter-mined as severe (over 7
mm in diameter), moderate (5-7 mm), and minimal (3-5 mm). Severe
dilatation was seen in 7 patients whose clinical grade was 2 in two
patients and 3 in five patients (Fig. 4).
A
Fig. 2. Multinlicity of the ISV and reno.spermatic shunt
B
Table 3. Occurrence of Anastomoses of the ISV (N = 26)
Location of Anastomosis
M 1 Ll M II LlI M III L III M IV LlV M V L V
No. 8 9 4 7 6 12 잉 5 2 7
% 31 35 15 27 23 46 12 19 8 27
Fig. 3. Circumaortic renal vein with reflux into the ISV. When
catheter was advancecl through preaortic superior limb , contast
injection into lower pole veins showecl preferential drainage into
cir-cumaortic renal vein . Note anastomosis between circumaortic
renal ve in and the ISV (arrows)
C
A. Two internal spermatic veins are shown. B. T wo ISVs with
reno-spermatic shunt (curved arrow). C. T wo ISVs are joined to
form single distal vein at cranial lumbar segment in Y.shape.
- 629 -
-
λ?:jUjj( n‘'*μ잭l}~ 션 ;w : q~23천 찌 4 싸 1987-
A B C
Fig. 4. Degree of the ISV ’s dilatation in selective venography
A. Minimal dilatation (3mm). B. Moderate dilatation (5mm) C. Severe
dilatation (9mm)
Concerning medial and lateral anastomo-ses, there was
prepollderance of MI, LI, and LII , LIII anastomoses , occurring in
27% 46% of cases (Fig. 5). Four cases of failed superselection were
excluded in this analysis about anastomotic sites.
Various forms of varicocele including dilated pampiniform plexus
only and dilated both pampiniform and cremasteric plexus and
mass-forming varicocele are demonstrated (Fig. 6).
In one patient of our series, crossover at the scrotallevel was
seen (Fig. 6(B)). Valves of the ISV were venographical1y detectable
in only 2 patients.
No major complications occurred in this series. Minimal
perivenous contrast extra-vasation around the ISV was observed in 2
in-stances almost invariably associated with guidewire and catheter
mainpulation in at-tempts to superselect the deep portion of the
ISV.
(3) Findings of left common iliac venography (Table 4)
Table 4. Finclings of Left COlll1110n l1 iac Venography
(N=30)
Findings No (%)
(37) Distal nutcracker phenomenon DNP with left to right shunt
DNP without left to right shunt
Suspicious DNP Both PNP and DNP
n 9
2
8
딩
(27)
(43)
menon (DNP) was observed. In 8 patients a similar but less
severe feature was seen with delayed persistent visualization of
the iliac viens (Fig. 7).
As a result of this phenomenon, col1ateral circulation has
developed from the left com-mon iliac system to the right side via
dilated pelvic veins in 9 cases. In 5 patients, left ascending
lumbar vein was shown. Both PNP and DNP were observed in 13
patients.
Spasm of the left external iliac vein occur-red in one patient.
T he spasm passed after a few minutes and left no clinical problem
(Fig. 8).
In 11 patients distal nutcracker pheno-
- 630-
-
- Seollng 011 Yang , et al.: Venographic Featllres of Va
ricocele-
CRANtAL Ll!M8 AR SU8 SEGI'!ENT
II CAUDAL LUPm AR S얘SEGI1ENT
r?1t、_eVI : INFRAIHGUINAL SEGMENT
A B C
D E F
Fig. 5. Sites of anast01l10ses A. Subdivision of the ISV into
subsegments. a = orifice of the ISV in left renal vein; b = pelvic
brim; c = deep in-guinal ring; d = superficial inguinal ring; e =
pampiniform plexus. B. Anastomosis at MI. C. Lll. D. ìVI III LllI
E. LlV. F. LV (see the text)
Discussion
A varicocele, the most common correctable cause of subfertiliy
in men, is present in 8% to 20% of the general male population,5.1
1. 12) and not all of those affected are infertile. However the
deleterious effect of the vari-cocele also has been well
established by Johnson and Pohl, who found a 70% incidence of
significantly abnormal semen characteris-
tics in 93 men with clinically asymptomatic varicoceles. 13 )
The most important implication of varicocele concerns its effect on
sper-matogenesis. It is speculated that reversed blood flow in the
ISV increases temperature and possibly increases pressure resulting
in decreased sperm counts, decreased motility, and increased number
of abnormal forms. And other hormonal or toxin theories had been
postulated. 14 ) For the time being, the patho-genesis of
subfertility associated with vari-
- 631 -
-
:J얘파}jX~‘t*~챔장‘f깐JE : 껴~23~ 짜 4 싸 1987-
A B C
Fig. 6. Various forms of varicocele
A
C
A. Usual shape of the dilated left pampiniform plexus. B.
Varicocele of pampiniform and cremasteric pexuses with crossover at
sacrallevel from left to right. External pudendal vein with patent
valve is noted (arrow). C. Peculiar round mass formation of the
dilated pampiniform plexus.
B
D
632 -
Fig. 7. Distal nutcracker phenome non. A . Left com mon iliac ve
nography shows focal compression of the left ex-ternal iliac vein
by cO l1ll1lon iliac artery without visible left to right pelvic
anasto l1losis. B & c. Ascen-ding lU l1lbar veins (arrows) and
left to rig ht pelvic anasto l1loses ‘ D. Multiple lU l1lbar colla
terals instead of filling in IVC
-
Seoung Oh Yang. et al.: Venographic Features of Varicocele-
A B C
Fig. 8. Spasm of left common and external iliac vein during
venography. A. Initial fi lm taken at 1 sec after injection of
contrast media shows initiation of spasm from above to below B.
Slit-like spasmodic peak at 4 sec. C. At 9 seconds. This spasm was
relieved after a few minutes
cocele has not been completely elucidated. Many diagnostic
methods including physic-
al examination, thermography, radioisotope imaging,15)
angiography, ultrasonography, and Doppler flow study are used to
evaluate varicocele . Ultrasonographic evaluation appears to have
the most success of the nonivasive imaging for defining subtle vari
cocele formation of the venous plexus. 16 ) Recently Sigmund and
associates compared the Doppler findings of varicocele and
veno-graphic features of flow pattern. 17 ) The stop-type
varicocele on the Doppler finding show-ed only retrograde blood
flow in the ISV and was small subclinical varicocele , whereas each
shunt-type varicocele showed both retrograde and orthograde venous
flow and that re-presented a kind of venous bypass. The shun ting
of venous blood appears to be a pre-condition for medium and large
varicoceles and might have some prognostic significance for
subfertility associated with varicoceles. To know these flow
patterns on venographic study , it is necessary to view the
spermatic
cord region intermittently with fluoroscopy for about 2 minutes
and to take spot images. We did not make efforts to depict these
draining veins in this study, but it should be searched afterward
.
Reflux due to anatomical causes include vascular inadequacy,
musculo-tendinous structures, anomalous renal and testicular
arteries, and anomalies of left renal vein.1B ) Hill and Green6 )
showed that venographic reflux into the ISV occured in 15 out of 26
cases (58%), but we demonstrated it in 29 out of 30 patients. In
the present investigation high grade varicocele was generally
associated with a higher degree of venographic reflux. 9 ) The
importance of the frequently occurring multi-plicity of the ISV and
vertical anastomoses lies in the fact that these venous tributaries
may lead to persistence or recurrence of varicocele 따ter treatment.
Connection between the ISV and other retroperitoneal veins were
noted in over half of the cases according to Morag et al. l9 ) The
most frequent connections were with the renal ιapsular , lumbar, or
internal iliac veins
633 -
-
太꾀1M‘r%씩까,~fr;ι{ ‘ 찌î23;하 짜 4 Wi 1987
as in this series. It is our impression that demonstration of
these connections is some-what dependent on the amount and pressure
of the contrast injection and the site at which it is delivered.
The deeper the catheter was placed into the ISV, the more likely
were venous connections to be demonstrated. So standardization of
the venographic technique is crucial for constant analysis of the
lesion
Ahlberg and associates1 ) showed that there was a significant
difference between the diameter of the left ISV in patients with a
varicocele and that in patients without a varicocele. The mean
diameter in these two groups were 6.8 and 4.3 mm respectively. This
also made it tenable that the diameter of the ISV is dependent on
the rate of reflux in-to this vesse l. Varicoceles usually are
con-sidered to result from absence of competent valves in the
proximal portion of the ISV. 20) Ahlberg2 ) showed in autopsy
material that the valves are absent in 40% of men and in 10% they
are incompetent. This finding raises the possibility of other
etiologies for the mechanism of varicocele. 2 1) In the concept of
the nutcracker phenomenon a central role is assigned to left renal
ve in compression. Several causes of this compression have been
postulated , including pressure exerted by the SMA, the ligament of
Treitz , the aberrant testicular artery or the retroaortic ve in
and stretching of the renal vein over the aorta. 19.10) Mali and
associates lO ) found a positive correla-tion between the
reno.caval pressure gradient and occurrrence of retrograde flow (r
= 0.67) and the size of the varicocele (r = 0.75) , by means of
pressure monitering and radioisotope study
Crossover at the scrotal level was seen in only 3 out of 140
patients according to Morag et al. 19) and we demonstrated one case
of crossover. And we experienced one case of circumaortic venous
ring. There are 3 main anatomic varients of the left renal vein:
preaortic, retroaortic , and circumaortic. Cir-
cumaortic left renal vein is potentially hazar-dous anomaly
inducing hemodynamic changes in kidney return circulation and may
be responsible for recurrent hematuria and pro-teinuria. 22.23)
With the usual transfemoral approach , right-sided
catheterization is often impossible. Morag et al. l9 ) showed the
success rate of superselction of the ISV by transfemoral ap-proach
as 93% in left and 62% in right. On the contrary, transjugular
approach succeeded in superselection as 92% in left side and 89% in
right side. So we think both approaches are equal for left-sided
lesion but for the sub-clinical varicocele with right-sided reflux
transjugular technique is indispensable. In addition , the
technique makes possible the safe, nonsurgical occlusion of both
ISV s more frequently. Nonsurgical varicocele occlusion can be
performed on an outpatient basis with reduced cost, no general
anesthesia, no postoperative sequelae such as hydrocele or
hematoma, and a lower recurrence rate. 24.1 9) Report of
percutaneous spring coil emboliza-tion of the ISV will be ensued.
For the time be-ing , we consider embolization warranted in
infertile patients with varicocele.
Venography is invasive and has some disad-vantage of requi,ring
an experienced angio-grapher, but it makes possible a detailed
study of the arrangement and function of the ISV s necessary in
planning treatment, and helps in the diagnosis of persistent or
recurrent varicoceles . Its reported morbidity is very low.4 )
Until noninvasive methods such as Dop-pler flow study have been
validated , veno-graphic features should be the criteria for the
diagnosis of the reflux including venous col-laterals and the tool
for the nonsurgical treatment.
Acknowledgement
We thank professor Jae Hyung Park , M.D. for providing valuable
advice about all these procedures.
- 634 -
-
Seoung Oh Yang, et al.: Venographic Features of Varicocele-
REFERENCES
1. Ahlberg NE, Bartley 0 , Chidelkel N: Right and left
gonadal veins. Acta Rad 4:593-601, 1966
2. Ah lberg NE, Bartley 0 , Chidelkel N: Phleoography in
varicocele scroti. Acta Rad 4:517-528, 1966
3. Brown j5, Dubin L, Becker M et al: Venography in the
subfertile man with varicocele. j Urol 98:388-392, 1967
4. jacobs jB: Selective gonadal venography. Radiology
92.885-888, 1969
5. Dubin L, Amerlar RD: Varicocele. UCNA, Vol. 5, No. 3,
563-572, 1978
6. Hill jT, Green NA: Varicocele - a review of radiological
and anatomical features in relation to surgical treatment
8r j Surg 64:747-752, 1977
7. Narayan P, Amplatz K, Gonzalez R: Varicocele and male
subfertility. Fertil 5teril 36:92-97, 1981
8. Charny CW, Baum 5: Varicocele and inferlility. jAMa
204:1165-1168, 7968
9. Marsman jW P: Clinical versus subc/inical va ricocele,
venographic findings and improvement of fertility after
embolization. Radiology 155:635-638, 1985
10. M ali WP, Oei HY, Arndt jW et al: Hemodynamics of the
varicocele. Part 1- 2. j Urol 135:483-493, 1986
11. Li pschultz 1.1 , Corriere jN: Progressive testicular
atrophy
in the varicocele patient. j UroI117:775, 1977
12. Clarke BG: Incidence of va ricocele in normal man and
amα19 men of different ages. jAMA 198:1121-1122,
1966
13. johnson DE, Pohl D, Ri vera CH: Varicocele-an in
nocuous cond ition? SOllth Med j 63:34, 1970
14. Comhaire F, Vermeuleu A: Varicocele sterilitκ cortisol
and ca techolamines. Fertil 5teril 25:88, 1974
15. Marmar jL, Zeiger LS, DeBenedictis Tj et al: Comprehen
sive scrotal flow and scan technique for detection of
varicocele. Urology 25:505-510, 1985
16. Yang 50, Kim Mj, Ro lW et al: The va lue of ultra-
sonography in varicocele evaluation. j of Korean Socie-
ty of ιled Ultrasound 5:126-132, 1986
17. 5igmund G, Gall H, Bähren W: Stop-type In Korean and
shunt-type varicoceles; venographic findings. Radiology
163: 105-110, 1987
18. Lerner MA, 5acks B, 5hapiro G: Retrograde flow in the
left gonadal vein at abdominal angiography. Urol Radiol
3:149-160, 1981
19. Morag B, Rubinstein ZY, Goldwasser B et al: Per
clltaneous venography and occ/usion in the manage-
ment of spermalÍc varicocele. AjR 143:635-640, 1984
20. Glezerman M , Rakowszczyk M, Lunenfeld B et al
Varicoceles in the oligospermic patients. j Urol 115:562,
1976
21. Coolsaet BLRA: The varicocele syndrome; venography
determining the optimallevel for surgical management
j Urol 124:833-838, 1980
22 . Beckmann CF, Abrams HL: Circllmaortic venolls ring; in-
cidence and significance. AjR 132:567-565, 1979
23 . Positano N, Nadal ini VF, Brutt ini GP: Hematuria due
to
circuma ortic left renal veil1. Urology 16:73-75, 7980
24. Berkman WA, Price RB, W heatley jE et al: Varicoceles,
a coaxial coil occ/usion system. Radiology 751:74-77,
1984
- 635-