Embed Size (px)
Citation preview

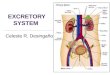
Urinary/Excretory System
Produces urine for elimination
Essential for homeostasis
normal blood composition
acid base (pH) balance
*Uremia poisoning from wastes build up toxic
2 Kidneys: clear blood of waste products from cell metab.
2 ureters: extend from kidneys & drain urine into to bladder
1 bladder: stores urine
1 urethra: extends from bladder & drains urine to void
Urinary Meatus: opening at end of urethra

Kidney Location: Above waist, towards back, under muscles
Behind Parietal Peritoneum (lines abdomen)
Encased in fat cushion (protects, anchors)
Renal Ptosis: kidney drops tubes kink obstructs urine
drainage
Floating Kidneys: Obese w/ rapid wt loss lose xs fat @
kidneys drift


Internal Kidney Structure
Cortex: outer
Medulla: Inner
Pyramids: ∆ shape division of medulla
Papilla: ∆ Narrow innermost end of pyramid
Pelvis: Expansion of upper end of ureter
Calyx: Division of renal pelvis w/ papilla of pyramid

Narrow part of pyramid
Renal pelvis w/ pyramid
Inner layer
Outer layer
Triangle shape in medulla
Drains urine from calyx
Expansion of upper end of ureter
Clean deO2
Dirty & O2

Microscopic Structure
Each kidney > 1 million Nephrons Basic unit of S&F of kidney


Nephron: 2 main parts * Renal Corpuscle: Bowman’s Capsule: cap of glomerulus Glomerulus: Capillary network in BC Afferent arteriole (lg) in Efferent arteriole (sm) out creates ↑ pressure for filtration of wastes
* Renal Tubule: Proximal Convoluted Tubule (PCT) (cortex) 1st segment closest to Bowman’s Capsule
Loop of Henle: extension of PCT (medulla)
Distal Convoluted Tubule (DCT) (cortex) Extensions of ascending Loop of Henle Collecting Tubule: drains several DCT’s cortex medulla


C
O
R
T
E
X
M
E
D
U
L
A

Urine from collecting tubules drain into collecting duct
papilla calyx renal pelvis
ureter bladder urethra
urinary meatus


3 Steps in Urine Formation in Nephrons
Filtration: continuous in renal corpusle
high glomerular pressure from A/E arteriole
pushes H2O & dissolved substances OUT of
glomerulus INTO BC
Ex. clean out desk remove most everything but most return thru “resorption”
If glomerular BP drops too low, (Ex. hemorrhage)
filtration stops kidney failure dialysis
Glomerular Filtration 125ml/min = 7500ml/hr = 180,000ml/day
180-190 qts!!!
But…most returns to blood thru peritubular capillary resorption!

Resorption: Mvmt of substances out of renal tubules
into peritubular capillaries
Substances resorbed: H2O, glucose, nutrients,
Na, Ions (based on intake)
Begins in PT, Loop of Henle, DT, CT
99% of H2O filtrate resorbed thru osmosis
& glucose absorbed into peritubular capillaries
thru AT in PT
K, H2O resorbed in DT
Diabetes Mellitus [blood glucose] ↑ so tubular filtrate contains more glucose than can be resorbed
Glucose in urine glycosuria

Secretion: Opposite of resorption
Substances move into urine in DT & CT from
capillaries @ tubules
Substances secreted: H+, K+, certain drugs (AT)
NH3 (diffusion)
Role in maintaining acid/base (pH) balance
& homeostasis



Control Of Urine Volume: Determined by amount of H2O & dissolved substances resorbed in PCT’s & DCT’s
ADH (Anti-Diuretic Hormone): “H2O retaining Hormone”
Made in hypothalamus
Stored in Posterior Pituitary Gland
↓’s amount of urine by making Distal/Collecting tubules
more permeable to H2O
↑ resorption, results in ↓ urine

More ADH = ↓ urine b/c tubules more permeable to H2O
Less ADH = ↑ urine b/c tubules less permeable to H2O
Caffeine & Alcohol: ↓ ADH ↑ urine ( dehydration) Nicotene: ↑ ADH ↓ urine

Aldosterone Hormone: “Salt & H2O retaining hormone”
Secreted by Adrenal Cortex
Stimulates tubules to resorb H2O & salt faster
Abnormal Urine Volume Excretion
* Anuria: no urine
* Oliguria: scant urine
* Polyuria: large amts of urine
Chilled vasoconstriction ↑ blood
flow to organs so
kidneys produce ↑ urine
Outer: adrenal cortexInner: adrenal medullaFx in tubule resorption

Ureters: Drain urine out of collecting tubules
into Renal Pelvis urinary bladder
Mucous Membranes line ureters & renal pelvis
Contraction of muscular coat peristaltic movement of
urine -> ureters bladder

Urinary Bladder: Empty, lies in pelvis
Full, projects up into lower abdominal cavity
Elastic fibers & Involuntary Muscle fx in expansion
Full: inner smooth
Empty: Rugae folds (like stomach)
Trigone:
Extends into urethra
*
males

Renal Colic: Pain from Kidney Stones (Renal Calculi)
Build up of Ca salts, uric acid, etc.
Avoid by ↑ H2O intake
Removal o kidney Stones:
Small, may pass
Large can obstruct urine flow or cause infection
Treat: Lithotripsy shock waves pulverize stones
in kidney, bladder, ureters, gall bladder too)
pass (Less invasive, faster recovery)
Surgery: Invasive, more complications, ? Infection & $$$$!

Urethra: Lower most part of urinary tract
Urine passes from bladder
↓urethra & out external
opening (Urinary Meatus)
***Same mucous membrane that lines renal pelvis, ureters, blaader, extends into urethra (so infections can spread up easily. 8” in males 1.5” in females

Urinary Catheteritization:
Insertion of catheter thru urethra into bladder
withdraw urine
(For sterile sample, surgery, urinary retention)
Requires asceptic technique to avoid infection,
cystitis (inflammation of bladder / infection)
UTI’s common nosocomial infection

Micturition: Urination / Voiding / Emptying Bladder
< 2 – 3yrs Reflex Action
>2 – 3yrs Voluntary Action
Internal Urethral Sphincter
@ bladder exit (Involuntary smooth muscle)
External Urethral Sphincter (compressor urethrae)
below bladder neck (Voluntary striated muscle)
Both contracted seal off bladder, urine accumulates & bladder stretches nerve impulses emptying reflex sphincters relax & contraction of bladder wall urine urethra void

Conditions
Urinary Retention: Kidneys produce urine but not voided
Urinary Suppression: Kidneys don’t produce urine but
bladder is able to empty
Incontinence: Void involuntarily
Elderly, stroke, spinal cord injury
lose muscle control affects emptying reflex
Cystitis: Bladder doesn’t empty completely
Residual urine chronic bladder infections
Polyuria: ↑ urine output
(hmm. ↓ levels of ADH, tubules less permeable don’t resorb as much H2O so it stays in urine))