Embed Size (px)
Citation preview

Upstream statin in ACS : Do we need to reload our patient?By
Ashraf Reda, MD, FESCProf and head of cardiology dep.-Menofiya university
President of EGYBACChairman of WGLVR

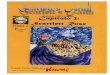
Effects of Statin Therapy on hs-CRP
when did the story begin?
-20
-15
-10
-5
0
5Placebo Statin
Per
cen
t C
han
ge
in M
edia
n C
RP
CAREPravastatin
5 yearsN = 472
AFCAPSLovastatin
1 yearN = 5719
BayerCerivastatin
8 weeksN = 785
4 SSimvastatin
4 monthsN = 249
PRINCEPravastatin12/24 weeks
N = 2400
Ridker PM. Eur Heart J. 2001;22:2135–2137.

CRP as Method to Target Statin Therapy in Primary Prevention:
AFCAPS/TexCAPS
Study Group Statin Placebo NNT
Low TC:HDL-C / low CRP 0.025 0.026 983
Low TC:HDL-C / high CRP 0.026 0.050 43
High TC:HDL-C / low CRP 0.022 0.051 35
High TC:HDL-C / high CRP 0.042 0.058 62
Median TC:HDL-C = 5.9 mg/dLMedian CRP = 0.16 mg/dL
Bermudez EA, Ridker PM. Prev Cardiol. 2002;5:42-46.

Atherosclerosis is an inflammatory disorder
“Inflammation is the reaction of the tissues to local injuries calling for protective and reparative measures; an imperfect pathologic adaptation often leading to consequences that per se are dangerous and defeat its purpose”
—LF Baker (1897)

No History of CADMen >55, Women > 65
LDL-C <130 mg/dL CRP >2 mg/L
Rosuvastatin 20 mg (n = 7500) MIStroke
Unstable Angina
CVD DeathCABG/PTCA
LDLCRPFHS
Lipidshs-CRP LFTs
Lipidshs-CRPHbA1C
JUPITER*: hitting the sweet spotRandomized Trial of Rosuvastatin 20 mg po qd in the Primary Prevention of Cardiovascular Events Among Individuals with Low Levels of LDL-C and Elevated
Levels of CRP
4 week Run-in
Screening Visit
Randomization Visit
Safety Visit
Bi-Annual Follow-Up Visits
End of Study Visit
Lipidshs-CRP LFTsHbA1C
Placebo (n = 7500)
*Justification for the Use of Statins in Primary Prevention:
an Intervention Trial Evaluating Rosuvastatin

AHA/CDC Scientific Statement
Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice
Impressive scientific and epidemiologic evidence that atherosclerosis is an inflammatory response
CRP risk cutpoints Low risk: 1.0 mg/L Average risk: 1.0–3.0 mg/L High risk: 3.0 mg/L
AHA/CDC Scientific Statement. Circulation. 2003;107:499-511

ACS from MIRACLE to PROVE-IT

ACS:PROVE-IT TIMI 224162 Pts With ACS
40mg Pravastatin 80mg Atorvastatin
Mean follow up:24 months
95 mg/dl (2.46 mmol/l) 62 mg/dl (1.6 mmol/l)LDL
26.3% 22.4%1ry end points
16%RRR (p0.005)

Treating to dual targets
Investigators also further stratified patients based on levels of CRP and LDL cholesterol:
LDL cholesterol >70 mg/dL and CRP >2.0 mg/L.
LDL cholesterol >70 mg/dL and CRP <2.0 mg/L. II LDL cholesterol <70 mg/dL and CRP >2.0 mg/L.
LDL cholesterol <70 mg/dL and CRP <2.0 mg/L.
"Even with the most aggressive statin that we have used to date, 56% of patients still did not make it to the dual target,"
56%
64%

The CRP continuum
The early Pravastatin trials
AF-CAPS, TEX-CAPS
PROVE-IT
JUPITER

Statin loading
ARMYDA: PCI in statin naïf
ARMYD-RECUPTURE: PCI in pts. on chronic
statin

ARMYDA-RECAPTURE (Atorvastatin for Reduction of MYocardial Damage during Angioplasty) trial
Prospective, multicenter, randomized, double blind trial investigating efficacy of atorvastatin reload
in patients on chronic statin therapy undergoing PCI
Principal Investigators: Giuseppe Patti, Vincenzo Pasceri, Achille Gaspardone, Giuseppe Colonna
Investigators: Andrea D’Ambrosio, Marco Miglionico, Annunziata Nusca, Rosetta Melfi, Laura Gatto, Elisabetta Ricottini, Gianluca Pendenza, Antonio Montinaro
Chairman: Germano Di Sciascio

Statin loading before PCI
Pts with chronic statin (NSTE- ACS or stable AP)
80 mg atorva 12 Hrs before and 40 mg 2 hrs after
30 day MACE Benefit more clear in ACS

Individual and Combined Outcome Measures of the Primary Endpoint at 30 days
8.69.1
P=0.045
ARMYDA-RECAPTURE: RESULTS
%
CompositePrimary End Point
3.4
0
3
6
9
12
Cardiac
death
MI TVR MACE
Atorvastatin
Placebo
0.5 0.5
3.4

0
3
6
9
12
15
Stable angina
%
0
3
6
9
12
15
ACS
%
4.3
5.3
2.4
13.8
P=0.97
P=0.016
ARMYDA-RECAPTURE Secondary endpoints
MACE according to clinical presentation (stable angina or ACS)
Test for Interaction: z=2.0; P=0.022
Atorvastatin Placebo

Loading and biomarkers
Significant CPK reduction
Significant troponin reduction
Non significant CRP production
LDL reduction????

Statin: the mechanism of benefit ?
LDL lowering
Pleotopic and anti-inflammatory
Molecule effect

ARMYDA-RECAPTURE
Reloading with high dose atorvastatin is associated with improved clinical outcome in patients on chronic statin therapy undergoing PCI
Acute atorvastatin bolus pre-PCI gives a 48% Relative Risk Reduction of 30-day MACE at MV analysis (NNT = 17)
The benefit is largely localized to patients who presented with ACS (87% Risk Reduction, NNT = 9)
Rapid LDL-independent cardioprotective effects may be responsible of this phenomenon