Embed Size (px)
Citation preview

Aggressive vs. Conventional Statin Therapy: Reduced Inflammation In Atherosclerosis ?
Provided by:
Christoph Bickel, M.D.Division of Cardiology
Central German Military Hospital, Koblenz, Germany
Editorial Slides VP Watch – November 6, 2002 - Volume 2, Issue 44

Although atherosclerosis was formerly considered to be a bland lipid storage disease, the importance of inflammation in atherosclerosis has been clearly demonstrated.1,2
Early in atherosclerosis endothelial cells express selective adhesion molecules - like vascular cell adhesion molecule-1 (VCAM-1) - that mediate adhesion and transmigration of leukocytes to the vascular endothelial wall and promote plaque growth and instability. In patients with CAD it has been shown that VCAM-1 levels predict independently future fatal cardiovascular events.3
Inflammation and Atherosclerosis
Interleukin (IL-18) plays a central role in orchestrating the cytokine cascade and accelerates atherosclerosis. Serum IL-18 levels were identified as a strong independent predictor of death from cardiovascular causes in patients with coronary artery disease.4
High-sensitivity C-reactive protein (hs-CRP) - a nonspecific marker of low-grade systemic inflammation - has received attention in atherogenesis. The cytokine cascade induces expression of hepatic genes encoding acute-phase reactants found in blood, including CRP.5
Inflammation and Atherosclerosis
hs-CRP levels have been demonstrated to identify increased risk of initial cardiovascular events in coronary heart disease patients and increased risk of recurrent cardiac events in patients with stable and unstable angina, patients with acute myocardial infarction, and patients undergoing elective coronary revascularization procedures.2,5-7.
Inflammation and Atherosclerosis
Nevertheless it has been shown that using a multimarker strategy (patients are categorized based on the number of elevated biomarkers including hs-CRP) seems to improve risk stratification in Non-ST elevation acute coronary syndromes to predict short- and long-term major cardiac events (death, myocardial infarction, congestive heart failure).8
Inflammation and Atherosclerosis

Beneath its lipid-lowering properties additional non-lipid effects of statin therapy9 on atherosclerosis are discussed:
In statin treated patients significantly lower levels of coagulation (von Willebrand factor), systemic inflammation (hs-CRP, interleukin-6) and soluble cell adhesion markers (p-selectin) were found.10
It has been shown that statin treatment influences the prediction of fatal coronary events by hs-CRP. Hs-CRP, which is a significant predictor of death from coronary artery disease, loses this prediction in statin-treated patients.11
Statin Therapy and Inflammation

Compared with patients receiving statin medication, patients without statins did not have increased cardiac mortality (even with elevated LDL-cholesterol levels) when hs-CRP levels were not elevated. In contrast, patients without statins and elevated hs-CRP had a 2.3-fold increase in risk for fatal coronary events, independent of LDL levels.11
Statin Therapy and Inflammation
In high-risk patients with coronary disease, other occlusive arterial disease, or diabetes it has been demonstrated that statin therapy is beneficial even when the initial LDL-cholesterol level is less than 100 mg/dl. The effect of statin therapy seems to be independent of the presenting cholesterol level.12
Statin Therapy and Inflammation
As reported in VP Watch of this week, van Wissen et al. show the results of the ASAP study (effects of atorvastatin vs. simvastatin on atherosclerosis progression) a 2 year, randomized double blinded study, to assess whether treatment with atorvastatin 80 mg or simvastatin 40 mg could retard atheroscleosis progression in patients with familial hypercholesterolaemia.13
ASAP-Study: hs-CRP reduction by statin therapyStudy-design

Baseline measurements of lipoprotein parameters, hs-CRP and carotid intima media thickness (IMT) were performed and repeated after 1 and 2 years.13,14
ASAP-Study: hs-CRP reduction by statin therapyStudy-design
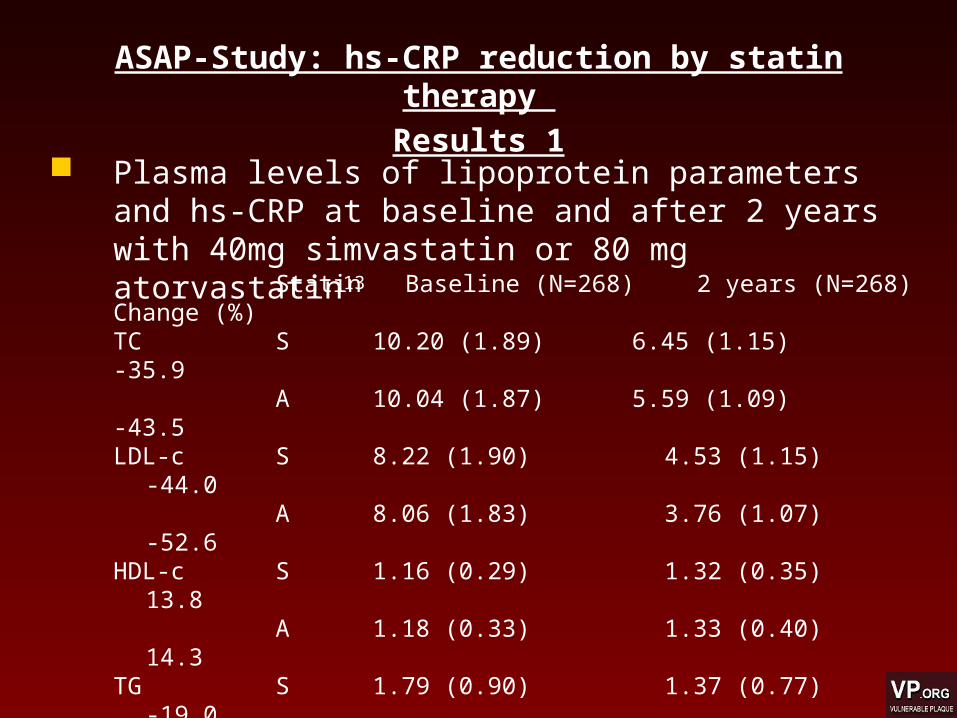
Plasma levels of lipoprotein parameters and hs-CRP at baseline and after 2 years with 40mg simvastatin or 80 mg atorvastatin13
ASAP-Study: hs-CRP reduction by statin therapy Results 1
Statin Baseline (N=268) 2 years (N=268) Change (%)TC S 10.20 (1.89) 6.45 (1.15) -35.9
A 10.04 (1.87) 5.59 (1.09) -43.5LDL-c S 8.22 (1.90) 4.53 (1.15) -44.0
A 8.06 (1.83) 3.76 (1.07) -52.6HDL-c S 1.16 (0.29) 1.32 (0.35) 13.8
A 1.18 (0.33) 1.33 (0.40) 14.3TG S 1.79 (0.90) 1.37 (0.77) -19.0
A 1.84 (1.07) 1.16 (0.64) -31.1hs-CRP S 2.0 (0.8 / 3.0) 1.5 (0.6 / 3.0) -19.7
A 2.1 (0.9 / 5.2) 1.1 (0.6 / 2.4) -40.1
Values are means (S.D.), except hs-CRP which is given as median (interquartile range); TC, total cholesterol; LDL-c, low density lipoprotein;HDL-c, high density lipoprotein; TG, triglcerides (all given in mmol/l); hs-CRP, high sensitive C-reactive protein (in mg/l); S = Simvastatin 40 mg;A = Atorvastatin 80 mg; % change: percentage change of median hs-CRP after 2 years of treatment;
In the atorvastatin 80 mg group 71.8% patients experienced a decrease of hs-CRP after 2 years of treatment, compared with 59.4 % in the simvastatin 40 mg group.13
However 1/3 of the patients developed an increase of hs-CRP after 2 years of treatment: in the atorvastatin 80 mg group 26.7% compared with 36.1 % in the simvastatin 40 mg group.13
1.5% of the patients in the atorvastatin and 4.5% of the patients in the simvastatin group had no change in hs-CRP level.13
ASAP-Study: hs-CRP reduction by statin therapy ASAP-Study: hs-CRP reduction by statin therapy Results 2
As published before the overall baseline IMT, combining the measurements of the common and internal carotid artery and the carotid bifurcation on both sides, was 0.93 mm (SD 0.22) and 0.92 mm (0.21) in the atorvastatin and simvastatin groups. 13,14
ASAP-Study: hs-CRP reduction by statin therapy Results 3
After treatment with atorvastatin for 2 years, IMT decreased (-0.031 mm [95% CI -0.007 to -0.055]; p=0.0017), whereas in the simvastatin group it increased (0.036 [0.014-0.058]; p=0.0005). The change in thickness differed significantly between the two groups (p=0.0001).13,14
ASAP-Study: hs-CRP reduction by statin therapy ASAP-Study: hs-CRP reduction by statin therapy Results 3

A significant correlation was found between the decrease of hs-CRP and the reduction of IMT, as seen in all patients combined (r = 0.13, P = 0.03).13
Patients in the highest tertile of CRP change (median hs-CRP reduction 3.28 mg/l; mean reduction IMT 0.016 mm/2 years), compared with the bottom tertile (median hs-CRP increase 0.57 mg/l; mean increase IMT 0.032 mm/2 years), exhibited a 2-fold greater reduction of mean carotid IMT.13
ASAP-Study: hs-CRP reduction by statin therapy Results 4
Conclusion: Aggressive statin therapy (80 mg
atorvastatin) reduces hs-CRP levels to a greater extent than conventional statin therapy (40mg simvastatin) in patients with familial hypercholesterolaemia.
Patients with the largest hs-CRP reduction showed a 2-fold greater reduction in IMT.
Conclusion: Aggressive statin therapy induces increased
reduction of inflammatory parameters like hs-CRP and seems to be associated with a decrease in progression rate of atherosclerosis especially in the prevention of premature atherosclerosis in high-risk patients with familial hypercholesterol-aemia
Questions:
• Is the difference in hs-CRP reduction between the both treatment groups a consequence of the different, non equivalent statin dosage or caused by the different agents independently from dosage ?
an increase in dosage of the same statin does not seem to cause an additional decrease of hs-CRP [in an randomized intervention study performed among 785 patients with primary hypercholesterolemia, Ridker observed highly significant reductions in plasma concentrations of CRP associated with both low-dose (0.4 mg) and high-dose (0.8 mg) cerivastatin given over an 8-week period. In contrast to LDL-C, he did not observe a significant dose-response effect for cerivastatin on CRP. Finally, there was no evidence that the change in LDL-C (or HDL-C) attributable to cerivastatin was related to the change in CRP that was also observed with the use of this agent]15.
Questions:• Why does about one third of the patients
show an increase of hs-CRP under statin treatment in this study ?
• Is this increase in hs-CRP really causally related to statin therapy or influenced by other circumstances that may affect hs-CRP, a non-specific marker of low-grade systemic inflammation e.g. infections ?
Questions:
• Should coadministration of statins in postmenopausal women with oral estrogens, which cause a hs-CRP increase16 with potential inflammatory and thrombotic consequences, be controlled by hs-CRP measurement to exclude an additional hs-CRP elevation and to verify that the combination of statins with estrogens may attenuate the potential harmful effects of estrogen therapy and reduce cardiovascular risk ?
References
1. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999;340:115-26.2. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105:1135-43.3. Blankenberg S, Rupprecht HJ, Bickel C, Peetz D, Hafner G, Tiret L, Meyer J. Circulating cell adhesion molecules and death
in patients with coronary artery disease. Circulation. 2001;104:1336-42.4. Blankenberg S, Tiret L, Bickel C, Peetz D, Cambien F, Meyer J, Rupprecht HJ. Interleukin-18 is a strong predictor of
cardiovascular death in stable and unstable angina. Circulation. 2002;106:24-30.5. Libby P, Ridker PM. Novel inflammatory markers of coronary risk: theory versus practice. Circulation. 1999;100:1148-50.6. Berk BC, Weintraub WS, Alexander RW. Elevation of C-reactive protein in "active" coronary artery disease. Am J Cardiol.
1990;65:168-72.7. Liuzzo G, Biasucci LM, Gallimore JR, Grillo RL, Rebuzzi AG, Pepys MB, Maseri A. The prognostic value of C-reactive
protein and serum amyloid a protein in severe unstable angina. N Engl J Med. 1994;331:417-24.8. Sabatine MS, Morrow DA, de Lemos JA, Gibson CM, Murphy SA, Rifai N, McCabe C, Antman EM, Cannon CP, Braunwald
E. Multimarker approach to risk stratification in non-ST elevation acute coronary syndromes: simultaneous assessment oftroponin I, C-reactive protein, and B-type natriuretic peptide. Circulation. 2002;105:1760-3.
9. Werner N, Nickenig G, Laufs U. Pleiotropic effects of HMG-CoA reductase inhibitors. Basic Res Cardiol. 2002;97:105-16.10. Bickel C, Rupprecht HJ, Blankenberg S, Espinola-Klein C, Rippin G, Hafner G, Lotz J, Prellwitz W, Meyer J. Influence of
HMG-CoA reductase inhibitors on markers of coagulation, systemic inflammation and soluble cell adhesion. Int J Cardiol.2002;82:25-31.
11. Bickel C, Rupprecht HJ, Blankenberg S, Espiniola-Klein C, Schlitt A, Rippin G, Hafner G, Treude R, Othman H, HofmannKP, Meyer J. Relation of markers of inflammation (C-reactive protein, fibrinogen, von Willebrand factor, and leukocyte count)and statin therapy to long-term mortality in patients with angiographically proven coronary artery disease. Am J Cardiol.2002;89:901-8.
12. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomisedplacebo-controlled trial. Lancet. 2002;360:7-22.
13. van Wissen S, Trip MD, Smilde TJ, de Graaf J, Stalenhoef AF, Kastelein JJ. Differential hs-CRP reduction in patients withfamilial hypercholesterolemia treated with aggressive or conventional statin therapy. Atherosclerosis. 2002;???:??-??
14. Smilde TJ, van Wissen S, Wollersheim H, Trip MD, Kastelein JJ, Stalenhoef AF. Effect of aggressive versus conventionallipid lowering on atherosclerosis progression in familial hypercholesterolaemia (ASAP): a prospective, randomised, double-blind trial. Lancet. 2001;357:577-81.
15. Ridker PM, Rifai N, Lowenthal SP. Rapid reduction in C-reactive protein with cerivastatin among 785 patients with primaryhypercholesterolemia. Circulation. 2001;103:1191-3.
16. Koh KK, Schenke WH, Waclawiw MA, Csako G, Cannon RO, 3rd. Statin attenuates increase in C-reactive protein duringestrogen replacement therapy in postmenopausal women. Circulation. 2002;105:1531-3.





























![Statin-Associated Muscle Disease: Advances in …...statin therapy because of side effects [12], making SAMS a serious public health problem. Patients stopping [13]oralter-ing their](https://img.dokumen.tips/doc/110x75/5f3496e8b771331bb838384a/statin-associated-muscle-disease-advances-in-statin-therapy-because-of-side.jpg)