Embed Size (px)
Citation preview

UPPER EXTREMITY ISCHEMIA IS SUPERIOR TO LOWEREXTREMITY ISCHEMIA FOR REMOTE ISCHEMIC CONDITIONINGOF ANTERO–LATERAL THIGH CUTANEOUS BLOOD FLOW
J. KOLBENSCHLAG,1* A. SOGORSKI,1 K. HARATI,1 A. DAIGELER,1 A. WIEBALCK,2 M. LEHNHARDT,1
N. KAPALSCHINSKI,1 and O. GOERTZ1
Remote ischemic conditioning (RIC) is known to improve microcirculation in various settings, but little is known about the impact of theamount of ischemic tissue mass or the limb itself. Since ischemia and subsequent necrosis of flaps is one of the most dreaded complica-tions in reconstructive surgery, adjuvant methods to improve microcirculation are desirable. We therefore performed a randomized trial tocompare the effect of arm versus leg ischemia for RIC of the cutaneous microcirculation of the antero–lateral thigh. Forty healthy volun-teers were randomized to undergo 5 min of ischemia of either the upper or lower extremity, followed by 10 min of reperfusion.Ischemiawas induced by a surgical tourniquet applied to the proximal limb, which was inflated to 250 mmHg for the upper and 300 mgHg for thelower extremity. This cycle was repeated a total of three times. Cutaneous microcirculation was assessed by combined laser dopplerspectrophotometry on the antero–lateral aspect of the thigh to measure cutaneous blood flow (BF), relative hemoglobin content (rHb), andoxygen saturation (StO2). Baseline measurements were performed for 10 min, after which the ischemia/reperfusion cycles were begun.Measurements were performed continuously and were afterwards pooled to obtain a mean value per minute. Both groups showed signifi-cant increases in all three measured parameters of cutaneous microcirculation after three cycles of ischemia/reperfusion when comparedto baseline (BF: 95.1% (P<0.001) and 27.9% (P 5 0.002); rHb: 9.4% (P<0.001) and 5.9% (P<0.001), StO2: 8.4% (P 5 0.045) and9.4% (P<0.001). When comparing both groups, BF was significantly higher in the arm group (P 5 0.019 after 11 min., P 5 0.009 after45 min). In conclusions, both ischemic conditioning of the upper and lower extremity is able to improve cutaneous BF on the ALT donorsite. However, RIC of the upper extremity seems to be a superior trigger for improvement of cutaneous BF. VC 2014 Wiley Periodicals, Inc.Microsurgery 00:000–000, 2014.
Tissue ischemia and the consecutive reperfusion injury
remain a major issue in medicine. Impaired tissue perfu-
sion can lead to necrosis and subsequent flap loss or
organ dysfunction, which can be further accentuated by
the so-called reperfusion injury.
Strategies to mitigate these effects have been
researched in various fields, most prominently in cardiol-
ogy. In 1986, Murry et al. showed that brief episodes of
coronary ischemia preceding an actual ischemic insult
were able to reduce the infarct size in a canine model.1
Seven years later, Przyklenk et al. found that ischemic
conditioning could also be applied at a remote vascular
bed to protect the myocardium.2 Thus, the term remote
ischemic conditioning (RIC) was coined and the way to
the clinical application of this technique was paved. In
addition to direct or remote ischemia, its timing in rela-
tion to the ischemia-reperfusion-injury lead to the con-
cepts of pre-, per-, and post-conditioning. The
mechanisms of these modalities are not yet fully under-
stood, but humoral factors like NO, TNF-a and reactive
oxygen species as well as neuronal factors seem to have
a great impact.3–5 The technique of RIC have found clin-
ical applications, most prominently in cardiac surgery,
percutaneous coronary interventions, and vascular
surgery.6–8
In reconstructive surgery, ischemia and reperfusion
injuries are the paramount problems associated with sur-
gical flaps in general and especially with free microvas-
cular transplants. While total flap loss rates are low and
are most often caused by technical issues or thrombosis
of the pedicle in coagulopathies, partial flap losses like
tip necrosis due to insufficient perfusion still pose a
major threat to the reconstructive outcome.9–11
There is a growing body of evidence that RIC can
improve the perfusion and therefore survival of surgical
flaps.3,12–17 However, studies considering the microcircula-
tion of flaps or potential flap donor sites in humans are
rare. To our knowledge, Kraemer et al. were the only
researchers to date to look into the effects of RIC on the
microcirculation of human skin at a potential flap donor
site.18 Also, while both upper and lower extremity were
used for RIC in various studies, their specific influence and
the impact of the amount of ischemic tissue on the effect
of RIC remains unclear.19,20 While a recent study found no
significant difference between the upper and lower extrem-
ity for remote ischemic postconditioning in patients under-
going percutaneous coronary intervention, the influence of
the extremity and therefore also the amount of ischemic tis-
sue on the cutaneous microcirculation remains unclear.21
1Department of Plastic Surgery, BG University Hospital Bergmannsheil,Hand Surgery, Burn Center, Ruhr University, Bochum, Germany2Department of Anesthesiology and Pain Therapy, Ruhrland Klinik, Univer-sity Hospital Essen, Essen, Germany.
*Correspondence to: Jonas Kolbenschlag, MD, BG University Hospital Berg-mannsheil, Department of Plastic Surgery, Burn Center, B€urkle-de-la-Camp-Platz 1, 44789 Bochum, Germany. E-mail: [email protected]. and A.S. contributed equally to this work.
Received 23 June 2014; Revision accepted 17 September 2014; Accepted22 September 2014
Published online 00 Month 2014 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/micr.22336
� 2014 Wiley Periodicals, Inc.

Therefore, we aimed to assess the influence of the
ischemic extremity and the ischemic tissue mass on the
acute RIC effects on the cutaneous microcirculation of a
common free flap donor site.
MATERIAL AND METHODS
After approval from the institutional ethics commit-
tee, healthy young volunteers were recruited. All subjects
were non-smokers without any history of known illnesses
or current medication. After screening for exclusion fac-
tors and obtaining the participants written informed con-
sent, a total of 40 volunteers were included in this study.
The demographic data for both groups is shown in Table
1, the included participants were between 19 and 40
years of age, with an BMI ranging from 18.8 to 30.9.
The participants were randomized into two groups:
one group underwent RIC of the leg, the other group of
the upper extremity.
Before measurements and conditioning, all partici-
pants were placed in a supine position in a temperature-
controlled room (21�C) without direct light exposure.
After resting for 15 min, blood pressure was measured
on the right upper arm. After this, baseline continuous
measurements were taken using the O2C device as
described below. These baseline measurements were per-
formed with the deflated tourniquet already attached to
the respective extremity to serve as an additional intrain-
dividual control for potential influences from the environ-
ment or the tourniquet itself. In both groups, RIC began
after those baseline measurements by occluding the blood
flow (BF) to either the upper or lower extremity for 5
min using surgical tourniquets. To achieve this occlusion,
250 mmHg, respectively 300 mmHg of pressure were
applied in the upper and lower extremity group. In all
participants, ischemia was verified by palpation and
doppler probe measurements of the dorsalis pedis artery
or the radial artery, respectively.
This phase of limb ischemia was then followed by a
reperfusion phase of 10 min before the next cycle was
applied, up to a total of three ischemia/reperfusion cycles
in both groups. Recordings were performed until the end
of the third reperfusion phase. All measurements were
performed by the same investigator.
In all cases, ischemia was applied to the extremity
contralateral to the leg on which the anterior lateral thigh
measurements were performed.
Ischemia was tolerated well by all but one partici-
pant. Because of increased discomfort during the second
leg ischemia, measurements had to be discontinued for
this volunteer. The data of this participant was removed
and replaced by measurements from an additional
participant.
Combined Laser Doppler Spectrophotometry
Continuous measurements of cutaneous blood flow
(BF in arbitrary units, AU), relative hemoglobin concen-
tration (rHb in AU) and oxygen saturation (StO2 in %)
were performed using the O2C device (LEA Medizin-
technik, Gießen, Germany).
This device applies combined laser doppler spectro-
photometry to simultaneously and continuously assess the
BF, the relative hemoglobin content (rHb) and the oxy-
gen saturation (StO2) in a depth of 2 mm, therefore rep-
resenting cutaneous microcirculation. The probe was
placed on the antero–lateral aspect of the thigh, at the
potential donor site of the antero–lateral thigh flap
(ALT). Its exact location was determined by drawing a
connecting line between the lateral patella and the ante-
rior superior iliac spine, with the probe being placed
halfway between the two anatomical landmarks. It was
taped to the leg in a standardized manner as proposed by
the manufacturer.
Measurements were performed continuously and were
afterwards pooled to obtain a mean value per minute to
correct for movement artifacts and other potential
influences.
Statistical Analysis
The extremity weight was calculated using the correc-
tion of the BMI formula for amputees as proposed by
Tzamaloukas et al.22 Statistical analysis was performed
using SPSS statistical package version 22.0 (IBM Corpo-
ration). The values for STO2 and rHb showed a normal
curve of distribution, therefore paired t-tests were used
for comparison to baseline and between groups. For BF,
data did not show a normal curve of distribution, there-
fore a nonparametric test was chosen to compare means
(Wilcoxon-rank-test) to baseline and between groups.
Results are displayed as mean 6 standard deviation (SD)
where applicable.
In addition to the absolute values, the relative
changes over the course of time are given as percentage
increase as compared to baseline (D%). An P-value of
<0.05 was considered to be statistically significant.
Table 1. Comparison of Demographic Data Between the Two
Groups
ARM LEG P
Age 26.25 6 4.76 23.95 6 2.65 0.069
Height 177.75 6 9.90 179.00 6 8.37 0.669
weight 72.70 6 14.02 77.70 6 12.85 0.247
BMI 22.80 6 2.67 24.00 6 2.79 0.162
Syst. BP 118.25 6 11.15 119.25 6 8.93 0.756
Dia. BP 76.75 6 4.94 75.00 6 7.43 0.386
Ext. Weight 4.82 6 0.92 14.55 6 2.40 <0.001
Male/female 14/6 6 0.47 15/5 6 0.44 0.731
BMI, body mass index, systl; BP, systolic blood pressure, dia; BP, diastolicblood pressure; ext. Weight, extremity weight.
2 Kolbenschlag et al.
Microsurgery DOI 10.1002/micr

RESULTS
There were no significant differences between the
two groups regarding age, BMI, blood pressure, or sex.
As expected, the calculated extremity weight was about
three times as high for the leg group, resulting in a sig-
nificant difference (P< 0.001, Table 1).
Blood Flow
Both groups started with a comparable BF without
significant differences. In the arm group, the BF was
already significantly improved after ten minutes when
compared to baseline (20.4% increase, P 5 0.048). It kept
rising throughout the ischemia/reperfusion cycles to end
up at a 95.1% increase after 45 min when compared to
baseline (P< 0.001). In the leg group, a significant
improvement in BF was first achieved after 25 min
(17.8% increase, P 5 0.006). It stayed significantly ele-
vated when compared to baseline, leading to a 27.9%
increase after 45 min (P 5 0.002). The first significant
difference between the two groups occurred at eleven
minutes, 6 min into the first reperfusion phase. Here, the
relative increase in flow for the arm group was 26.8%
and 10.7% for the leg group (P 5 0.019). After all three
ischemia/reperfusion cycles the difference between the
two groups became even more evident (95.1% increase
vs. 27.9%, P 5 0.009; Fig. 1, Table 2).
Relative Hemoglobin Content
There was no significant difference in the starting
values for both groups. Significant elevation of rHb was
found during the first reperfusion phase, at 7th min seven
in both groups (arm: 2.2% increase vs. baseline,
P 5 0.002; leg: 1.5% increase, P 5 0.009).
Over the course of time, rHb increased steadily in
both groups, resulting in a 9.4% increase for the arm and
5.9% increase and leg group after 45 min. Although
these increases were significant when compared to base-
lines (P< 0.001 for both), they did not differ signifi-
cantly between the two groups (Fig. 2, Table 3).
Oxygen Saturation
As for the parameters discussed above, the starting
values for both groups did not differ significantly. For
the leg group, a significant increase in SO2 when com-
pared to baseline was observed after 8 min (2.9%
increase, P 5 0.009). In the arm group, the first signifi-
cant increase of SO2 was seen only after 45 min (8.4%
increase, P 5 0.045). Although the increase in SO2
occurred earlier and more pronounced in the leg group,
there was no significant difference between the two
groups over the course of time (P 5 0.884) (Fig. 3, Table
4).
DISCUSSION
The combined laser doppler spectrophotometry uti-
lized in this study has been regularly used.18,23–28
As shown in previous works, RIC is capable of
improving the cutaneous microcirculation.18 This effect
was most pronounced for the BF, which was increased
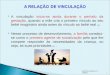
Figure 1. Course of cutaneous blood flow in AU over time for both
groups. The five minutes of ischemia are grayed out. Note the ear-
lier significant increase in flow for the arm group (P 5 0.048 after
10 min vs. P 5 0.006 after 25 min) and the significant higher blood
flow in the arm group when compared to the leg group after three
cycles of ischemia/reperfusion (*P 5 0.009 after 45 min).
(AU 5 arbitrary units).
Table 2. Comparison of the Cutaneous Blood Flow Over the Course of Time for Both Groups
Time
ARM LEG
P ARM vs. LEGAU D% P vs. BL AU D% P vs. BL
Baseline(BL) 21.30 6 12.58 – – 26.00 6 21.49 – – –
10 min 25.64 6 18.67 20.4 0.048* 28.50 6 26.96 9.6 0.099 0.071
11 min 27.01 6 19.11 26.8 0.006 28.77 6 26.61 10.7 0.062 0.019a
15 min 29.39 6 21.76 38.0 0.001 29.34 6 28.39 12.8 0.100 0.019
25 min 33.05 6 25.74 55.2 0.001 30.62 6 27.69 17.8 0.006a 0.014
30 min 35.76 6 25.96 67.9 < 0.001 31.47 6 28.36 21.0 0.006 0.005
45 min 41.56 6 34.17 95.1 < 0.001 33.26 6 27.89 27.9 0.002 0.009
AU, abitrary units; D%, is the percentage increase versus baseline measurements.aMarks the first point in time at which there was a significant increase versus baseline or a significant difference between groups.
RIC Extremity 3
Microsurgery DOI 10.1002/micr

nearly twofold in the arm group and about 1.3-fold in
the leg group. The increases seen in rHb and SO2 were
less prominent, but nonetheless statistically significant.
This matches the findings of Kraemer et al. except for
the rHb, which showed a significant reduction during the
second reperfusion phase, but no significant difference
after 50 min.18
The fact that BF was the most improved parameter
fits in with the previous findings that describe increased
flap survival, since an increased BF leads to a better
nutritional supply. Cutaneous BF is influenced by a num-
ber of elements such as the autonomous nervous system
and humoral factors and can therefore be controlled and
modulated in various ways.29 While cutaneous BF is sub-
jected to direct control, the changes in rHb and SO2
result from the interaction between the BF and the per-
fused tissue. After the increase of BF, the vascular bed
receives an additional inflow of hemoglobin and therefore
an increased oxygen supply. Since the measured parame-
ters primarily represent the venous system, these values
depict the nutritional state of the local tissue. As the met-
abolic demand of the local tissue was not significantly
altered in our study, the increased inflow of hemoglobin
resulted in a slight increase in SO2 and rHb. In tissue
with increased metabolic demand, the SO2 would be
reduced due to increased oxygen consumption. While the
SO2 was more than sufficient in the healthy volunteers
examined in this study, in a surgical pedicled or free flap
the distal part might already have a shortage of oxygen
supply due to the compromised vascular network, result-
ing in a lower SO2 and might therefore benefit from this
additional oxygen supply. Therefore, RIC might success-
fully be applied in flap surgery. However, one must take
into account that this study was conducted on a potential
donor site with an intact vascular bed.
By raising the flap and reducing its vascular supply
to the pedicle the tissue is depraved of its compensatory
mechanism. In addition, the flap itself is denervated in
the progress, since the nerve fibers from the surrounding
tissue are cut. In free flaps, even the innervation of the
vascular pedicle is severed. Therefore, in free flaps even
more than in pedicled flaps, direct neuronal modulation
of the perfusion might be hampered. However, based on
the existing data from animal models, humoral transmit-
ters, either released due to vascular stress, ischemia, or
as end effectors of neuronal regulation, seem to be
responsible for the regulation of BF and also the protec-
tive effects of RIC.12–16,30 Therefore, further research
concerning the possibly different reactions to an RIC
stimulus of pedicled and free-flaps as compared to local
skin seems warranted, especially in relation to the timing
of conditioning.
Considering the mechanisms of RIC, a variety of trig-
gers, mediators and end effectors are discussed.31 Among
those, NO and oxygen radicals seem to act as such
potential triggers.3,31,32 Because of the high oxygen con-
sumption of skeletal muscle, its ischemia tolerance is
limited, resulting in the accumulation of oxygen radicals
and endproducts of ischemic metabolism.33–35 During
reperfusion, these substances are washed out and together
with reactive leukocyte activation result in the so-called
reperfusion injury.12
In addition, the postocclusive reactive hyperemia
(PORH) leads to an increased vascular shear and stretch,
resulting in the release of NO.36
Since the magnitude of the release of the substances
aforementioned correlates with the amount of ischemic
Figure 2. Course of relative hemoglobin content in AU over time for
both groups. Note the early significant increase in rHb when com-
pared to baseline for both groups. The difference between groups
after 45 min showed a nonstatistically significant trend (P 5 0.074).
(AU 5 arbitrary units).
Figure 3. Course of oxygen saturation over time for both groups.
While both groups showed a significant increase when compared
to baseline, this effect was obtained earlier in the leg group. There
was no significant difference between the two groups.
(% 5 percentage of oxygen saturation).
4 Kolbenschlag et al.
Microsurgery DOI 10.1002/micr

tissue, one might hypothesize that a higher mass of
ischemic tissue could lead to an increase in the effect of
RIC. However, our results show that the opposite seems
to be the case, since the amount of ischemic tissue in the
leg group was about three times as high as in the arm
group. Therefore, one could hypothesize that there might
be a certain threshold that triggers an RIC stimulus and
after which further activation does not result in an
increased response.
Another possible explanation could be that the ische-
mia of the upper extremity acts as a more potent trigger
of the autonomous nervous system. Various works show
differences between the autonomic reactions of the upper
and lower extremity. Mental stress for example seems to
lead to a more pronounced vascular change in the fore-
arm when compared to the calf, although these results
seem to be modified by various factors, including gen-
der.37 This further contributes to the evidence that a
combination of neuronal and humoral factors seem to be
involved in RIC.38
The stress and relief from inflating and deflating the
tourniquet itself could also contribute to an autonomic
response, potentially influencing the perfusion by trigger-
ing a pain-induced “fight-or-flight-response.” Since the
ischemic cycling was tolerated well by all participants in
the arm group and by all but one volunteer in the leg
group, this stimulus seems to be distributed equally
between groups. If one would assume the leg ischemia to
be more painful based on this one drop-out, it should
lead to a more pronounced perfusion in the leg group,
which is not the case. However, additional research to
identify a potential correlation between a pain stimulus
and perfusion changes seem warranted.
Since we only measured the short-term response of
cutaneous microcirculation to RIC, the mid- and long-
term effects remains unclear. RIC is known to have an
early and a late window of effect, with the former being
primarily triggered by the immediate effects of humoral
and neuronal factors and the later being based on
changes in gene expressions that lead to a down-
regulation of proinflammatory genes and can also modify
neutrophil function. These effects were shown to last up
to ten days after RIC.38,39
Also, since we performed RIC of a potential flap
donor site, the effects seen in this study have to be
considered as “pre-conditioning.” Although various ani-
mal studies have shown positive effects of precondi-
tioning on flap survival, to our knowledge, none such
data exists for humans.13,14,40 In addition, in many
studies, “preconditioning” in relation to flap surgery
was defined as an RIC stimulus after flap elevation but
before flap ischemia, in contrast to the stimulus in our
study, which was applied to a healthy and intact vascu-
lar bed.14,40 In a rat muscle flap model, Carroll et al.
also found beneficial effects for acute ischemic condi-
tioning prior to flap elevation, therefore it seems appro-
priate to assume a positive effect of preconditioning in
a clinical setting.41
Table 4. Comparison of the Oxygen Saturation Between the Two Groups Over the Course of Time
Time
ARM LEG
P ARM vs. LEG% D% P vs. BL % D% P vs. BL
Baseline(BL) 51.90 6 8.78 – – 46.50 6 12.85 – – –
8 min 52.94 6 10.64 2.0 0.269 47.84 6 13.37 2.9 0.009a 0.554
15 min 53.29 6 9.54 2.7 0.337 49.19 6 13.20 5.8 <0.001 0.506
30 min 55.39 6 10.68 6.7 0.099 49.98 6 13.38 7.5 <0.001 0.839
45 min 56.27 6 11.16 8.4 0.045a 50.87 6 13.50 9.4 <0.001 0.884
%, percentage of oxygen saturation; D%, is the percentage increase versus baseline measurements.aMarks the first point in time at which there was a significant increase versus baseline.
Table 3. Comparison of the Relative Hemoglobin Content Over the Course of Time
Time
ARM LEG
P ARM vs. LEGAU D% P vs. BL AU D% P vs. BL
Baseline(BL) 65.50 6 6.77 – – 68.35 6 6.84 – – –
7 min 66.96 6 7.42 2.2 0.002a 69.37 6 6.94 1.5 0.009a 0.312
15 min 68.57 6 6.87 4.7 <0.001 70.67 6 7.01 3.4 <0.001 0.385
30 min 70.88 6 8.28 8.2 <0.001 71.75 6 7.19 5.0 <0.001 0.088
45 min 71.67 6 8.90 9.4 <0.001 72.36 6 7.23 5.9 <0.001 0.074
AU, arbitrary units; D%, is the percentage increase vs. baseline measurements.aMarks the first point in time at which there was a significant increase vs. baseline.
RIC Extremity 5
Microsurgery DOI 10.1002/micr

However, further studies need to look into the effect
of RIC and its timing (especially pre- and post-condition-
ing) on surgical flaps in a clinical setting. Especially, the
role of preoperative conditioning and late postcondition-
ing (after surgery) should be evaluated, since they can
easily applied in a clinical setting without prolonging the
duration of the surgery.
CONCLUSION
Ischemia of both the upper and lower extremity is
able to improve cutaneous microcirculation of the
antero–lateral thigh via RIC. The cutaneous BF improved
superior after ischemia of the arm when compared to
ischemia of the leg. Therefore, if possible, the upper
extremity should be used for RIC purposes. The amount
of ischemic tissue seems to have little impact on the
effect of RIC. This might suggest a certain role of neuro-
nal factors that warrants further research.
ACKNOWLEDGMENTS
The author thank the participants of this study for volun-
teering as well as Professor Hans Trampisch and Renate
Klaaßen-Mielke of the Department of Medical Infor-
matics, Biometry and Epidemiology, University of
Bochum for their help considering the statistical analysis.
REFERENCES
1. Murry CE, Jennings RB, Reimer KA. Preconditioning with ische-mia: A delay of lethal cell injury in ischemic myocardium. Circula-tion 1986;74:1124–1136.
2. Przyklenk K, Bauer B, Ovize M, Kloner RA, Whittaker P. Regionalischemic ’preconditioning’ protects remote virgin myocardium fromsubsequent sustained coronary occlusion. Circulation 1993;87:893–899.
3. Kuntscher MV, Kastell T, Altmann J, Menke H, Gebhard MM,Germann G. Acute remote ischemic preconditioning II: The role ofnitric oxide. Microsurgery 2002;22:227–231.
4. Donato M, Buchholz B, Rodriguez M, Perez V, Inserte J, Garcia-Dorado D, Gelpi RJ. Role of the parasympathetic nervous system incardioprotection by remote hindlimb ischaemic preconditioning. ExpPhysiol 2013;98:425–434.
5. Saxena P, Newman MA, Shehatha JS, Redington AN, KonstantinovIE. Remote ischemic conditioning: Evolution of the concept, mecha-nisms, and clinical application. J Card Surg 2010;25:127–134.
6. Ovize M, Thibault H, Przyklenk K. Myocardial conditioning: Oppor-tunities for clinical translation. Circ Res 2013;113:439–450.
7. Brevoord D, Kranke P, Kuijpers M, Weber N, Hollmann M, PreckelB. Remote ischemic conditioning to protect against ischemia-reperfusion injury: A systematic review and meta-analysis. PLoSOne 2012;7:e42179.
8. Yetgin T, Manintveld OC, Boersma E, Kappetein AP, van GeunsRJ, Zijlstra F, Duncker DJ, van der Giessen WJ. Remote ischemicconditioning in percutaneous coronary intervention and coronaryartery bypass grafting. Circ J 2012;76:2392–2404.
9. Kolbenschlag J, Daigeler A, Lauer S, Wittenberg G, Fischer S,Kapalschinski N, Lehnhardt M, Goertz O. Can rotational thromboe-lastometry predict thrombotic complications in reconstructive micro-surgery? Microsurgery 2014;34:253–260.
10. de Blacam C, Colakoglu S, Ogunleye AA, Nguyen JT, Ibrahim AM,Lin SJ, Kim PS, Lee BT. Risk factors associated with complicationsin lower-extremity reconstruction with the distally based sural flap:A systematic review and pooled analysis. J Plast Reconstr AesthetSurg 2014;67:607–616.
11. Yu P, Chang DW, Miller MJ, Reece G, Robb GL. Analysis of 49cases of flap compromise in 1310 free flaps for head and neckreconstruction. Head Neck 2009;31:45–51.
12. Kuntscher MV, Hartmann B, Germann G. Remote ischemic precon-ditioning of flaps: A review. Microsurgery 2005;25:346–352.
13. Kuntscher MV, Kastell T, Sauerbier M, Nobiling R, Gebhard MM,Germann G. Acute remote ischemic preconditioning on a rat cremas-teric muscle flap model. Microsurgery 2002;22:221–226.
14. Kuntscher MV, Schirmbeck EU, Menke H, Klar E, Gebhard MM,Germann G. Ischemic preconditioning by brief extremity ischemiabefore flap ischemia in a rat model. Plast Reconstr Surg 2002;109:2398–2404.
15. Moon JG, Lim HC, Gye MR, Oh JS, Park JW. Postconditioningattenuates ischemia-reperfusion injury in rat skin flap. Microsurgery2008;28:531–537.
16. Huang L. What happened if various kinds of postconditioning work-ing on the preconditioned ischemic skin flaps. PLoS One 2013;8:e72818.
17. Yan H, Zhang F, Kochevar AJ, Akdemir O, Gao W, Angel M. Theeffect of postconditioning on the muscle flap survival after ischemia-reperfusion injury in rats. J Invest Surg 2010;23:249–256.
18. Kraemer R, Lorenzen J, Kabbani M, Herold C, Busche M, VogtPM, Knobloch K. Acute effects of remote ischemic preconditioningon cutaneous microcirculation—A controlled prospective cohortstudy. BMC Surg 2011;11:32.
19. Crimi G, Pica S, Raineri C, Bramucci E, De Ferrari GM, Klersy C,Ferlini M, Marinoni B, Repetto A, Romeo M, Rosti V, Massa M,Raisaro A, Leonardi S, Rubartelli P, Oltrona Visconti L, Ferrario M.Remote ischemic post-conditioning of the lower limb during primarypercutaneous coronary intervention safely reduces enzymatic infarctsize in anterior myocardial infarction: A randomized controlled trial.JACC Cardiovasc Interv 2013;6:1055–1063.
20. Holmberg FE, Ottas KA, Andreasen C, Perko MJ, Moller CH,Engstrom T, Steinbruchel DA. Conditioning techniques and ischemicreperfusion injury in relation to on-pump cardiac surgery. ScandCardiovasc J 2014;48:241–248.
21. Lavi S, D’Alfonso S, Diamantouros P, Camuglia A, Garg P, TeefyP, Jablonsky G, Sridhar K, Lavi R. Remote ischemic postcondition-ing during percutaneous coronary interventions: Remote ischemicpostconditioning-percutaneous coronary intervention randomizedtrial. Circ Cardiovasc Interv 2014;7:225–232.
22. Tzamaloukas AH, Patron A, Malhotra D. Body mass index in ampu-tees. JPEN J Parenter Enteral Nutr 1994;18:355–358.
23. Kneser U, Beier JP, Schmitz M, Arkudas A, Dragu A, Schmidt VJ,Kremer T, Horch RE. Zonal perfusion patterns in pedicled free-styleperforator flaps. J Plast Reconstr Aesthet Surg 2014;67:e9–e17.
24. Rothenberger J, Amr A, Schiefer J, Schaller HE, Rahmanian-Schwarz A. A quantitative analysis of the venous outflow of thedeep inferior epigastric flap (DIEP) based on the perforator veinsand the efficiency of superficial inferior epigastric vein (SIEV)supercharging. J Plast Reconstr Aesthet Surg 2013;66:67–72.
25. Fox PM, Zeidler K, Carey J, Lee GK. White light spectroscopy forfree flap monitoring. Microsurgery 2013;33:198–202.
26. Mucke T, Rau A, Merezas A, Loeffelbein DJ, Wagenpfeil S,Mitchell DA, Wolff KD, Steiner T. Identification of perioperativerisk factor by laser-doppler spectroscopy after free flap perfusion inthe head and neck: A prospective clinical study. Microsurgery 2014;34:345–351.
27. Ozturk CN, Ozturk C, Ledinh W, Bozkurt M, Schwarz G, O’RourkeC, Djohan R. Variables affecting postoperative tissue perfusion mon-itoring in free flap breast reconstruction. Microsurgery 2014 doi:10.1002/micr.22276. [Epub ahead of print]
28. Rothenberger J, Amr A, Schaller HE, Rahmanian-Schwarz A. Evalu-ation of a non-invasive monitoring method for free flap breast recon-struction using laser doppler flowmetrie and tissuespectrophotometry. Microsurgery 2013;33:350–357.
6 Kolbenschlag et al.
Microsurgery DOI 10.1002/micr

29. Simmons GH, Wong BJ, Holowatz LA, Kenney WL. Changes inthe control of skin blood flow with exercise training: Where docutaneous vascular adaptations fit in? Exp Physiol 2011;96:822–828.
30. Loukogeorgakis SP, Williams R, Panagiotidou AT, Kolvekar SK,Donald A, Cole TJ, Yellon DM, Deanfield JE, MacAllister RJ. Tran-sient limb ischemia induces remote preconditioning and remote post-conditioning in humans by a K(ATP)-channel dependent mechanism.Circulation 2007;116:1386–1395.
31. Kaur S, Jaggi AS, Singh N. Molecular aspects of ischaemic postcon-ditioning. Fundam Clin Pharmacol 2009;23:521–536.
32. Baines CP, Goto M, Downey JM. Oxygen radicals released duringischemic preconditioning contribute to cardioprotection in the rabbitmyocardium. J Mol Cell Cardiol 1997;29:207–216.
33. Kloner RA, Jennings RB. Consequences of brief ischemia: stunning,preconditioning, and their clinical implications: Part 1. Circulation2001;104:2981–2989.
34. Defraigne JO, Pincemail J. Local and systemic consequences ofsevere ischemia and reperfusion of the skeletal muscle. Physiopa-thology and prevention. Acta Chir Belg 1998;98:176–186.
35. Schellong SM, Ockert D, Zimmermann T. Pathophysiology and clin-ical aspects of ischemia-reperfusion damage to skeletal muscles.Vasa 1998;27:207–215.
36. Birukov KG. Cyclic stretch, reactive oxygen species, and vascularremodeling. Antioxid Redox Signal 2009;11:1651–1667.
37. Yang H, Drummer TD, Carter JR. Sex differences in sympatheticneural and limb vascular reactivity to mental stress in humans. Am JPhysiol Heart Circ Physiol 2013;304:H436–H443.
38. Lim SY, Hausenloy DJ. Remote ischemic conditioning: from benchto bedside. Front Physiol 2012;3:27.
39. Shimizu M, Saxena P, Konstantinov IE, Cherepanov V, CheungMM, Wearden P, Zhangdong H, Schmidt M, Downey GP,Redington AN. Remote ischemic preconditioning decreases adhesionand selectively modifies functional responses of human neutrophils.J Surg Res 2010;158:155–161.
40. Adanali G, Ozer K, Siemionow M. Early and late effects of ische-mic preconditioning on microcirculation of skeletal muscle flaps.Plast Reconstr Surg 2002;109:1344–1351.
41. Carroll CM, Carroll SM, Overgoor ML, Tobin G, Barker JH. Acuteischemic preconditioning of skeletal muscle prior to flap elevationaugments muscle-flap survival. Plast Reconstr Surg 1997;100:58–65.
RIC Extremity 7
Microsurgery DOI 10.1002/micr