Embed Size (px)
Citation preview

TOWARDS HEALTHCARE PLANNING
ANDEVALUATION
Professor Michael ClarkeDept of Epidemiology &
Public Health

Are we doing the right thing? - evidence based medicine
To the right people? - appropriate care
Often enough - meeting needs

People have health care Needs
Health services are the responses to the
Needs
Good Quality Health services must be:
(i) effective
(ii) efficient
(iii)equitable
ie work for the lowest cost, and be
fairly distributed

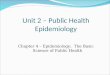
A Taxonomy of NeedNeeds: Items of service, or resources,
felt to be required, either by consumers or providers…………………
Demands: …………….. which are applied for …….
Met (demands) ……….. provided and utilised …… (admissions, consultations)
Unmet (demands) …… and the request is rejected or, (more usually) cannot be met at that time
(waiting lists)

CONSUMERDEFINEDNEED
NEEDNEEDNEED
DEMAND
MET
DEM.UNMET

NEEDNEEDNEED
DEMAND
MET
DEM.UNMET
NEEDNEEDNEED
DEMAND
METDEM.
UNMET(UTILISATION)
PROVIDER DEFINED NEED
CONSUMERDEFINEDNEED

NEEDNEEDNEED
DEMAND
MET
DEM.UNMET
NEEDDEM.UNMET
DEMANDMET
CONSUMERDEFINEDNEED
PROVIDER DEFINED NEED

NEEDNEEDNEED
DEMAND
MET
DEM.UNMET
NEEDNEEDNEED
DEMAND DEM.UNMET
CONSUMERDEFINEDNEED
PROVIDER DEFINED NEED
INAPPROPRIATE / INEFFECTIVE CARE
UTILISATION

Examples of Inappropriate Care
UK
Approximate %
50 Coronary angiography and bypass surgery
in Trent
60 Cholecystectomies in North West Thames
USA
66 Carotid endarterectomies – 65+
25 Gastrointestinal endoscopies
25 Coronary angiographies
25-66 Coronary artery bypass
ops Brook, R.H. Brit. Med. J. (1994) 308,
218-9

Factors which influence Quality of health care
STRUCTURES(RESOURCES)
Capital FacilitiesHospitalsDoctors
SurgeriesAmbulances
Trained Personnel

Factors which influence Quality of health care
STRUCTURES(RESOURCES)
Capital FacilitiesHospitalsDoctors
SurgeriesAmbulances
Trained Personnel
PROCESSES(USE OF
RESOURCES)
ConsultationsProcedures
Admissions etc(Ethical
RelevantEffective
Socially acceptable)

Factors which influence Quality of health care
STRUCTURES(RESOURCES)
Capital FacilitiesHospitalsDoctors
SurgeriesAmbulances
Trained Personnel
PROCESSES(USE OF
RESOURCES)
ConsultationsProcedures
Admissions etc(Ethical
RelevantEffective
Socially acceptable)
OUTCOMES
DeathDisease
DisabilityDiscomfort
DissatisfactionDebt

Factors which influence Quality of health care
STRUCTURES(RESOURCES)
Capital FacilitiesHospitalsDoctors
SurgeriesAmbulances
Trained Personnel
PROCESSES(USE OF
RESOURCES)
ConsultationsProcedures
Admissions etc(Ethical
RelevantEffective
Socially acceptable)
OUTCOMES
DeathDisease
DisabilityDiscomfort
DissatisfactionDebt
CASE-MIXAge, severity of illness, co-morbidity, culture/language
Derived from Donabedian, A. Evaluating the Quality of Medical Care. Milb. Mem. Fund Quart. 44(3) Part2:116-323,
July 1963.

Q How do we know what are the best structures or processes?
A (i) Judgemental method ‘human rights’
avoidable factors in care Consensus Conferences
(ii) Comparative approach confounders
case mix differences

Case Study of theComparative Method
Paediatric Intensive Care

Provision of intensive care for childrenA geographically integrated service may now be achieved
A study comparing illness adjusted mortality for children living in the ‘Trent’ region, where paediatric intensive care provision is fragmented among 19 centres, with that in the two paediatric intensive care units in Victoria, Australia – which has similar size of child population and similar rate of admission to paediatric intensive care – showed both an excess mortality and a greater length of stay in Trent
Jane Ratcliffe, Consultant Paediatric Intensivist, Alder Hey Childrens Hospital, Liverpool
BMJ Editorial Vol. 316, 1547, 23 May 1998

Should paediatric intensive care be centralised? Trent versus
Victoria
Lancet (1997), 349, 1213-17
Gale Pearson, Frank Shann, Peter Barry, Julian Vyas, David Thomas, Colin Powell,
David Field


Population 1994 1996Total<16 years
4,781,000 913,700
5,121,238 975,000
Deaths aged 1 month to <15 yearsNumberRate per 100,000 < 15 years (+/- 95% ci)
26829.3
(26.0–33.0)
31232.0
(28.6-35.7)
ONS Population Data for Trent 1994 &1996
• population increase due to boundary changes – 1996 includes Grimsby & Scunthorpe• 1994 – 28% deaths <15 years occur in PICU’s (74 deaths)

Trent Victoria
Population Total <16 yrsDeaths 1 month – 16 yrs Number Rate/100,000<16
4,2000,000 913,700
266 (100%) 29.1
4,500,000 1,011,000
257 (100%) 25.4
PICU Admissions No. per year Per 1000 <16 Deaths in ICU Deaths per 1000 ICU admissions
1014 1.22 74 (28%)
73
1194 1.18 60 (23%)
50

PICU Admissions No. per year per 1000 <16 Deaths in ICU Deaths per 1000 ICU admissions
1414 1.55 74 (28%) 52
1194 1.18 60(23%) 50
Trent Victoria
PICU Admissions No. per year Per 1000 <16 Deaths in ICU Deaths per 1000 ICU admissions
1014 1.22 74 (28%)
73
1194 1.18 60 (23%)
50

Next Steps
1. Undertake Prospective Study – as initial step in developing a continuing
evaluation of P.I.C.
2. Establish a simple Enquiry into all Paediatric
Mortality in Trent

When Comparing Health Care Systems
BEWARE !1. Population errors
2. Cases missed, not admitted (unmet need)
3. Differences in case definitions, admissions policies
4. Counting people or admissions
5. Differences in case mix

Q How do we know what are the best structures or processes?
A (i) Judgemental method ‘human rights’
avoidable factors in care consensus Conferences
(ii) Comparative approach confounders
case mix differences
(iii) Experimental (RCTs) Methods

Continuum of increasing evidence
Explore relevant theory to ensure best choice of intervention Strategic design issues
Pre-clinical
Theory

Continuum of increasing evidence
Explore relevant theory to ensure best choice of intervention Strategic design issues
Identify the intervention, and the underlying mechanisms by which they will influence outcomes.
Phase IPre-clinical
Theory
Modelling

Continuum of increasing evidence
Explore relevant theory to ensure best choice of intervention Strategic design issues
Identify the intervention, and the underlying mechanisms by which they will influence outcomes.
Phase IPre-clinical
Design a feasible protocol for comparing the intervention to an appropriate alternative
Phase II
Theory
Modelling
Exploratory Trial

Continuum of increasing evidence
Explore relevant theory to ensure best choice of intervention Strategic design issues
Identify the intervention, and the underlying mechanisms by which they will influence outcomes.
Phase IPre-clinical
Design a feasible protocol for comparing the intervention to an appropriate alternative
Phase II
Compare a fully defined intervention to an appropriate alternative that is an adequate control
Phase III
Theory
Modelling
Exploratory Trial
Definitive RCT

Continuum of increasing evidence
Explore relevant theory to ensure best choice of intervention Strategic design issues
Identify the intervention, and the underlying mechanisms by which they will influence outcomes.
Phase IPre-clinical
Design a feasible protocol for comparing the intervention to an appropriate alternative
Phase II
Compare a fully defined intervention to an appropriate alternative that is an adequate control
Determine whether others can reliably replicate your intervention and results in uncontrolledsettings over the long tern
Phase III Phase IV
Theory
Modelling
Exploratory Trial
Definitive RCT
Long-term Implementation

RCTs can be simple or complex
(i) a) drugs
b) appliances - simple
(ii) a) management e.g. length of stay
b) personnel e.g. nurse practitioner
(iii) Preventive services - complex
e.g. screening programmes

SUMMARY1. Evaluation is essential if we are to get the
best “bang for the buck”
2. Evaluation of health services needs the best quality clinical science
3. Best clinical science includes patient outcomes from a variety of perspectives, measured over the longer term

PHASE IV TRIALSPostmarketing surveillance-
Long term safetyThe yellow card system
Promotional activityChanging prescribing
behaviour
PROGRAMME EVALUATION
Long-term monitoringDissemination ofResearch findings
Health gain
PHARMACEUTICALRESEARCHPRECLINICAL
-pharmacology, animal toxicityPHASE 1 TRIALS
Clinical pharmacology and toxicityDrug metabolism and bioavailability
Healthy volunteers
HEALTH SERVICERESEARCH
BASIC LABORATORY SCIENCE
CLINICAL SCIENCEService Innovation
PHASE II TRIALSInitial treatment studies onsmall numbers of patients
PHASE III TRIALSLarge scale randomised trials
comparing a standard treatmentwith a new treatment
EXPLANATORY TRIALS
PRAGMATIC TRIALSEconomic assessment
Patient compliancePatient satisfaction