Embed Size (px)
Citation preview

American Journal of Medical Genetics Part C (Seminars in Medical Genetics) 175C:70–115 (2017)
R E S E A R C H R E V I E W
The Ehlers–Danlos Syndromes, Rare TypesANGELA F. BRADY, SERWET DEMIRDAS, SYLVIE FOURNEL-GIGLEUX, NEETI GHALI,CECILIA GIUNTA, INES KAPFERER-SEEBACHER, TOMOKI KOSHO,ROBERTO MENDOZA-LONDONO, MICHAEL F. POPE, MARIANNE ROHRBACH,TIM VAN DAMME, ANTHONY VANDERSTEEN, CAROLINE VAN MOURIK,NICOL VOERMANS, JOHANNES ZSCHOCKE, AND FRANSISKA MALFAIT *
Dr. Angela F. Brady, F.R.C.P., Ph.D., is a Consultant Clinical Geneticist at the North West Thames Regional Genetics Service, London and she has aspecialist interest in Ehlers–Danlos Syndrome. Shewas involved in setting up theUKNational EDSDiagnostic Servicewhichwas established in 2009 andshe has been working in the London part of the service since 2015.
Dr. Serwet Demirdas, M.D., Ph.D., is a clinical geneticist in training at the Erasmus Medical Center (Erasmus University in Rotterdam, theNetherlands), where she is involved in the clinical service and research into the TNX deficient type of EDS.
Prof. Sylvie Fournel-Gigleux, Pharm.D., Ph.D., is a basic researcher in biochemistry/pharmacology, Research Director at INSERM (Institut National dela Sant�e et de la RechercheM�edicale) and co-head of theMolCelTEG Research Team at UMR7561 CNRS-Universit�e de Lorraine. Her group is dedicatedto the pathobiology of connective tissue disorders, in particular the Ehlers–Danlos syndromes, and specializes on the molecular and structural basis ofglycosaminoglycan synthesis enzyme defects.
Dr. Neeti Ghali, M.R.C.P.C.H., M.D., is a Consultant Clinical Geneticist at the North West Thames Regional Genetics Service, London and she has aspecialist interest in Ehlers–Danlos Syndrome. She has been working in the London part of the UK National EDS Diagnostic Service since 2011.
Dr. Cecilia Giunta, Ph.D., is a molecular geneticist and established scientist working in the field of Ehlers–Danlos Syndrome and other heritableconnective tissue disorders (CTD) since 1995. Together with Dr. Marianne Rohrbach she runs the diagnostic and research activities of the ConnectiveTissue Unit as part of the Division of Metabolism at the University Children's Hospital, Zurich since September 2008. Her research focuses on theunderstanding of the Molecular Basis and Pathology of Connective Tissue Disorders, in particular the rare forms of EDS and osteogenesis imperfecta.She is currently a member of the medical and scientific board of the Ehlers–Danlos Society.
Dr. Ines Kapferer-Seebacher, D.M.D., is a periodontist with a clinical and research focus on dental and periodontal manifestations of rare diseases.She is an Associate Professor at the Department of Restorative and Operative Dentistry, Medical University Innsbruck, Austria.
Dr. Tomoki Kosho, M.D., Ph.D., is a pediatrician and clinical geneticist. He is an Associate Professor at the Center for Medical Genetics at ShinshuUniversity Hospital, where he directs clinical service for heritable connective tissue disorders and research especially on D4ST1-deficient EDS.
Dr. RobertoMendoza-Londono,M.D., is the Director of the EDS clinic at the Hospital for Sick Children (HSC) and University Health Network (UHN) inToronto and the interim head of the Division of Clinical of Metabolic Genetics at HSC/University of Toronto. He is a clinical geneticist with expertisein skeletal dysplasia's and connective tissue disorderswho has an interest in gene discovery and studies of natural history of disease. He has participatedin several collaborative projects that led to the identification and characterization of genes that regulate the formation and maintenance of bone andconnective tissue.
Prof. Michael F. Pope, M.B.B.Ch., F.R.C.P., M.D., is Consultant in Charge of the new NHS National Commissioning Group Complex EDS Service atthe Kennedy Galton Center, Northwick Park Hospital. He is especially interested in the classification, genetics, and diagnosis of Ehlers–Danlossyndrome, osteogenesis imperfecta, pseudoxanthoma elasticum, cutis laxa, Stickler syndrome, theMarfan syndrome, many of which overlap with thebenign hypermobility syndrome (BHS). His expertise lies in the differentiation, separation, and testing of these disorders from BHS.
Dr. Marianne Rohrbach, M.D., Ph.D. in molecular genetics, is a trained pediatrician and clinical geneticist. Together with Dr. Giunta, she leads thediagnostic and research activities of the Connective Tissue Unit at University Children's Hospital in Zurich, Switzerland. Dr. Rohrbach established amultidisciplinary Connective tissue clinic including clinical, biochemical, and molecular diagnosis, as well as patient management and counseling. Herresearch focus includes long-term follow up and natural history of all connective tissues diseases and the understanding of the Molecular Basis andPathology of Connective Tissue Disorders, in particular the rare forms of EDS and osteogenesis imperfecta.
Dr. Tim Van Damme is an M.D., Ph.D. student at the Center for Medical Genetics Ghent, Belgium, whose research involves the study of clinical,genetic and pathogenetic aspects of the Ehlers–Danlos syndromes and related disorders.
Dr. Anthony Vandersteen,M.A., Ph.D.,M.D., is amedical geneticist, assistant professor at IWKHealth Center and Dalhousie University, Nova Scotia,Canada. He has a special interest in EDS and previously worked in the UK National EDS Diagnostic Service.
Caroline van Mourik, B.Ed., M.Sc., Ph.D. (Biology and Geology), has been active in the Swedish patient-organization, previously as Chair but latermainly as the scientific editor. She even presented a paper at the first international symposium on EDS in Ghent, 2012 and frequently lectures aboutEDS, both for the medical field as well as laymen.
Nicol Voermans, M.D., Ph.D., is a neurologist specialized in neuromuscular disorders at the Radboud University Medical Center (Nijmegen, theNetherlands). She directs the clinical service for neurological and neuromuscular features of various types of EDS, and has a large experience with theTNX-deficient type EDS.
Prof. Johannes Zschocke,M.D., Ph.D., is Professor andChair of HumanGenetics at theMedical University Innsbruck, Austria, where he is also ActingDirector of the Department of Medical Genetics, Molecular and Clinical Pharmacology. As Head of the Center for Medical Genetics Innsbruck, he isresponsible for the provision of genetic services for theWestern Austria and beyond. His clinical and research focus is on inherited metabolic diseases,and he has been involved in the genetic characterization of several Ehlers–Danlos Syndrome subtypes.
Prof. FransiskaMalfait,M.D., Ph.D., is a rheumatologist and clinical geneticist. She is an Associate Professor at the Center forMedical Genetics at theGhent University Hospital, where she directs the research, clinical service, and laboratory facility for diagnosis and genetic testing for the Ehlers–Danlossyndrome and other heritable disorders of connective tissue. She is the current Chair of the medical and scientific board of the Ehlers–Danlos Society.
*Correspondence to: FransiskaMalfait,M.D., Ph.D., Center forMedical Genetics, Ghent University Hospital, De Pintelaan 185, Gent 9000, Belgium.E-mail: [email protected]
DOI 10.1002/ajmg.c.31550Article first published online in Wiley Online Library (wileyonlinelibrary.com).
� 2017 Wiley Periodicals, Inc.

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 71
The Ehlers–Danlos syndromes comprise a clinically and genetically heterogeneous group of heritable connectivetissue disorders, which are characterized by joint hypermobility, skin hyperextensibility, and tissue friability. In theVillefranche Nosology, six subtypes were recognized: The classical, hypermobile, vascular, kyphoscoliotic,arthrochalasis, and dermatosparaxis subtypes of EDS. Except for the hypermobile subtype, defects had beenidentified in fibrillar collagens or in collagen-modifying enzymes. Since 1997, a whole spectrum of novel, clinicallyoverlapping, rare EDS-variants have been delineated and genetic defects have been identified in an array of otherextracellular matrix genes. Advances in molecular testing have made it possible to now identify the causativemutation for many patients presenting these phenotypes. The aim of this literature review is to summarize thecurrent knowledgeon the rare EDS subtypes andhighlight areas for future research. ©2017Wiley Periodicals, Inc.
KEYWORDS: Ehlers–Danlos syndromes; heritable connective tissue disorders; collagen
How to cite this article: Brady AF, Demirdas S, Fournel-Gigleux S, Ghali N, Giunta C, Kapferer-Seebacher I,Kosho T, Mendoza-Londono R, Pope MF, Rohrbach M, Van Damme T, Vandersteen A, van Mourik C,Voermans N, Zschocke J, Malfait F. 2017. The Ehlers–Danlos syndromes, rare types. Am J Med Genet
Part C Semin Med Genet 175C:70–115.
INTRODUCTORYSTATEMENT
For each genetic EDS subtype, a sub-committee of authors performed a com-prehensive literature search. All articleswere reviewed for relevance and addi-tional articles were identified from theliterature. The articles were summarizedand divided into themes: (1) the historyofthe EDS subtype, (2) mechanisms ofdisease, (3) allelic heterogeneity, (4)clinical description, (5) genotype–phe-notype correlations and penetrance, (6)management, and (7) differential diagno-sis. The summary of these themes wascritically reviewed by all authors.
Subcommittees:
�
Classical EDS due to COL1A1p.(Arg312Cys) (cEDS-COL1A1):Fransiska Malfait�
Classical-like EDS due to Tenascin-Xdeficiency (clEDS): Serwet Demirdas,Nicol Voermans�
Cardiac-valvular EDS (cvEDS): Fran-siska Malfait�
Arthrochalasia EDS (aEDS): TomokiKosho, Cecilia Giunta, MarianneRohrbach, Fransiska Malfait�
Dermatosparaxis EDS (dEDS): TimVan Damme, Fransiska Malfait�
Kyphoscoliotic EDS (kEDS-PLOD1):Angela Brady, Neeti Ghali, CecilaGiunta, Marianne Rohrbach, TimVan Damme, Anthony Vandersteen�
Kyphoscoliotic EDS (kEDS-FKBP14):Cecila Giunta, Marianne Rohrbach,Tim Van Damme, Fransiska Malfait�
Brittle cornea syndrome (BCS): Ma-rianne Rohrbach, Tim Van Damme�
Spondylodysplastic EDS (spEDS-B4GALT7 and spEDS-B3GALT6):Sylvie Fournel-Gigleux, Tim VanDamme, Fransiska Malfait�
Spondylodysplastic EDS (spEDS-SLC39A13): Cecilia Giunta�
Musculocontractural (mcEDS): To-moki Kosho, Fransiska Malfait�
Myopathic EDS (mEDS): RobertoMendoza-Londono, Fransiska Malfait�
Periodontal EDS (pEDS): Ines Kapferer-Seebacher, Michael Pope, Anthony Van-dersteen, Johannes ZschockeCLASSICAL EDS DUE TOCOL1A1 p.(Arg312Cys)(COL1A1-cEDS)
Synonyms: Classic-like Ehlers–Danlossyndrome with propensity to arterialrupture, Vascular-like EDS
The History of Classical EDSdue to COL1A1 p.(Arg312Cys)(COL1A1-cEDS)
Nuytinck et al. [2000] reported twochildren with a classical EDS phenotype,including skin hyperextensibility, easybruising, atrophic scarring, and jointhypermobility, with a c.934C>T,p.(Arg312Cys) mutation. Malfait et al.[2007] identified the same mutation inan adult who suffered from a ruptureof medium-sized arteries, reminiscentof vascular EDS. In addition, twoother arginine-to-cysteine (Arg-to-Cys)
substitutions in the proa1(I) chain of typeI collagen, c.1720C>T, p.(Arg574Cys)and c.3277C>T, p.(Arg1093Cys°), wereidentified in two other adults withvascular rupture, but without EDS-signs[Malfait et al., 2007]. The p.(Arg312Cys)mutation has subsequently been identi-fied in two other individuals with EDSand complications of vascular fragility[Ritelli et al., 2013; Gaines et al., 2015].In view of the major clinical overlap ofthe p.(Arg312Cys)-associated phenotypewith classical EDS due to COL5A1 orCOL5A2 mutations, both conditionsare grouped within the same clinicalentity (“Classical EDS”) in the newEDS classification. Patients with thep.(Arg312Cys) mutation are particularlyat risk for vascular events, highlighting thebenefit of molecular confirmation inclassical EDS patients for managementpurposes.
In view of the major clinicaloverlap of the p.(Arg312Cys)-associated phenotype with
classical EDS due to COL5A1or COL5A2 mutations, bothconditions are grouped within
the same clinical entity(“Classical EDS”) in the new
EDS classification.

72 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
The prevalence of this condition isunknown.
Mechanism of Disease
Thepathogenetic basis for thephenotyperesulting from these specific Arg-to-Cyssubstitutions is currently not well under-stood. Ultrastructural studies of dermalcollagen fibrils have shown fibrilswith variable diameters, and slightlyirregular contour, and, in case of thep.(Arg312Cys), flower-like abnormali-ties [Malfait et al., 2007].
Several mechanisms have been sug-gested to be involved in the pathogenesis[Malfait et al., 2007], including localdestabilization of the triple helix due toloss of the stabilizing arginine residue;introduction of a cysteine residue, whichcan lead to disulfide-bonding withother collagenous or non-collagenousproteins, either intracellularly or in theextracellular matrix (ECM), therebydisturbing normal physiological interac-tions; interference with pericellularprocessing of the amino-propeptide ofprocollagen type I, and/or local unwind-ing of the region surrounding themutations, thereby disturbing specificinteractions with type I collagen ligands[Malfait et al., 2007].
Allelic Heterogeneity
Three different heterozygous COL1A1mutations, leading to a Arg-to-Cyssubstitution have been reported inassociation with vascular fragility:c.934C>T, p.(Arg312Cys); c.1720C>T,p.(Arg574Cys); and c.3277C>T, p.(Arg1093Cys).
Clinical Description
To date, six patients from five familieshave been reported with the p.(Arg312Cys) (Table S1). These includetwo females (respectively 5 and 43 yearsold) and five males (respectively 7, 16,39, and 53 years old). [Nuytinck et al.,2000; Malfait et al., 2007; Ritelli et al.,2013; Gaines et al., 2015].
The hallmark of this condition isthe “vascular fragility,” leading to spon-taneous dissection or rupture ofmedium-sized arteries, in combination
with other EDS signs. It is a rare, butimportant differential diagnosis of vas-cular EDS.
Reported clinical features for thep.(Arg312Cys) substitution
�
Reproductive, including pregnancyPremature preterm rupture of the fetalmembranes (PPROM) was reported inone patient. One patient was reportedto have neonatal hypotonia. No preg-nancy-related complications were re-ported (one known pregnancy in anaffected female).�
Craniofacial featuresNone of the patients had characteristicfeatures of vascular EDS. One patientwas reported to have redundant skinfolds on the eyelids and soft earlobes,reminiscent of classical EDS. Onepatient had blue sclerae, high palate,and hypoplastic uvula.�
Musculoskeletal systemGeneralized joint hypermobility wasreported in four patients. One patienthad congenital bilateral hip dislocationand a traumatic shoulder dislocation.Another patient was also reported tohave sporadic joint dislocations. Pectusexcavatum was reported twice. Twopatients complained from chronic jointpain. None of the patients had a historyof fractures; DEXAZ-score was normalin two patients.�
Skin and integumentSkin involvement included skin hyper-extensibility (n¼ 4); soft, doughy skin(n¼ 2); thin or translucent skin (n¼ 3);friable skin/skin splitting (n¼ 2); atro-phic scars (n¼ 4); delayed wound heal-ing (n¼ 1); unusual tenderness upontouch (hyperalgesia) (n¼ 1); piezogenicpapules (n¼ 1); molluscoid pseudotu-mors (n¼ 1); varicoseveins (n¼ 1). Easybruising was reported in all patients(n¼ 6). Finallyonepatient hadhiatal andabdominal and inguinal hernias.�
Ocular involvementBlue sclerae were observed on onepatient. One patient was operated forstrabismus.�
Cardiovascular systemAll three adults had severe cardiovascu-lar complications. The patient repo-rted by Malfait et al. [2007] had aspontaneous dissection of the right iliacartery at 43 years. Her affected 16-year-old son did not have complications ofvascular fragility, except for unusualbruising. The patient, reported byGaines et al. [2015] suffered from aspontaneous rupture of the commoniliac artery at 39 years. The patient,reported by Ritelli et al. [2013] hadmild mitral and aortic valve regurgita-tion, left ventricular wall thickening,aortic root dilatation, vertebral arterytortuosity, and a hepatic hemangioma at53 years. The two children reported byNuytinck et al. [2000] did not showsigns of vascular fragility at the time ofreport. Clinical follow-up is not avail-able for these patients.
Other Arg-to-Cys substitutions that lead tovascular fragilityEDS-like signs have only been observedin association with the p.(Arg312Cys)mutation. One patient harboring ap.(Arg574Cys) (male, 42 years) sufferedfrom a dissection of the left femoralartery and an aortic aneurysm. Onepatient harboring a p.(Arg1093Cys)(male, 40 years) had a left kidneyinfarction at age 34 years, and adissection of the infrarenal aorta andleft iliac artery, with aneurysm of the leftrenal artery at age 39 years. He also hadmitral valve bulging [Malfait et al.,2007].
Genotype–Phenotype Correlationand Penetrance
The Arg-to-Cys substitutions in the a1(I) collagen chain seem to be associatedwith specific phenotypes: Classical EDSwith vascular fragility for p.(Arg312Cys)and isolated vascular fragility forp.(Arg574Cys) and p.(Arg1093Cys).In addition, three other Arg-to-Cyssubstitutions have been reported forthis gene: c.3040C>T,p.(Arg1014Cys)is associated with autosomal dominantCaffey disease [Gensure et al., 2005],whereas c.3106C>T,p.(Arg1036Cys)and c.3196C>T,p.(Arg1066Cys) arereported in patients with an OI/EDSoverlap phenotype without signs ofvascular fragility [Cabral et al., 2007;

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 73
Lund et al., 2008]. The pathogenic basisfor theses specific clinical consequencesis unknown.
Penetrance is unknown.
Management
Key management guidelines focus onthe cardiovascular system.
Specific management guidelinesinclude:
–
Measurement of aortic root size andassessment of heart valves by echocar-diogram at the time of diagnosis or byage 5 years–
Echocardiogram at 5-year intervals,even if the initial echocardiogram isnormal–
Vigilant observation and control ofblood pressure can reduce the risk ofarterial rupture–
Further vascular surveillance ought tobe considered–
Consider bone densitometry evaluationGuidelines for management ofmusculoskeletal problems, skin in-volvement, ophthalmologic and dentalfollow-up, and pregnancy should fol-low those formulated for other formsof EDS (for reference: See “manage-ment guidelines for the classicalEhlers–Danlos syndrome,” by Bowenet al., this issue).
Differential Diagnosis
�
Vascular EDS � Classical EDS due to COL5A1 orCOL5A2 mutations�
OICLASSICAL-LIKE EDSDUE TO TENASCIN-XDEFICIENCY (clEDS)
The History of the Classical-LikeEDS
This type of EDS was first described byBurch et al. [1997]. The authorsdescribed a 26-year-old male patientwith congenital adrenal hyperplasia
(CAH) due to 21-hydroxylase defi-ciency as well as hyperextensible skin,hypermobile joints, easy bruising,and poor wound healing. Skin biopsyof this patient showed small collagenfibers of normal shape and a completeabsence of tenascin XB (TNX).Cultured dermal fibroblasts alsolacked TNX. PCR of the patientsDNA revealed a 30 kb deletion inchromosome 6 overlapping both theCYP21B gene and the TNXBgene. Subsequently, Schalkwijk et al.[2001] measured TNX in the serum of151 EDS patients (classical and vasculartype), 168 diseased controls (psoriasisand rheumatoid arthritis), and 21healthy controls. They detected acomplete TNX deficiency in fiveEDS patients and three affectedsiblings (one of which with the contig-uous gene syndrome). Mutation analy-ses revealed mostly homozygousmutations in the TNXB gene forthese patients. The authors concludedthat the TNX-deficient type is verysimilar to the classical type of EDS withtwo major differences: (1) No atrophicscarring was apparent, and (2) theinheritance pattern was autosomalrecessive.
The prevalence of this condition isunknown.
Mechanism of Disease
TNX is one of the three known largematricellular proteins of the tenascinfamily [Mao and Bristow, 2001;Valcourt et al., 2015]. Although theprecise function of TNX is unknown,it is known to play a role in the ECMas it is highly expressed in connectivetissue of muscle, around tendons,ligaments, and in skin [Mao andBristow, 2001]. The glycoprotein isencoded by the TNXB gene inhumans. Classical-like EDS is causedby a complete lack of TNX due tohomozygous or compound heterozy-gous TNXB mutations, that lead tononsense-mediated mRNA decay(NMD), or biallelic deletion ofTNXB. As a result, the TNX proteinis completely absent [Mao and Bris-tow, 2001].
Allelic Heterogeneity
A total of 24 patients with a completeTNX-deficiency without involvementof the CYP21B gene have beenreported. In 19 of these patients (15families), the molecular diagnosis isknown. Homozygous and compoundheterozygous mutations have been iden-tified. Mutations have been identifiedthroughout the TNXB gene, and in-clude missense, frameshift, and nonsensemutations.
There is a registry of reportedTNXB gene variants [Dalgleish, 1998].
In five out of the 24 reportedpatients, no genetic confirmation ofthe clinical diagnosis after TNX serummeasurement was performed.
Clinical Description
The clinical phenotype of the 24patients with a complete TNX-deficiency without involvement of theCYP21B gene was reviewed (Table S1)[Schalkwijk et al., 2001; Peeters et al.,2004; Lindor and Bristow, 2005; Voer-mans et al., 2007, 2009b; O’Connellet al., 2010; Hendriks et al., 2012,P�enisson-Besnier et al., 2013; Sakiyamaet al., 2015; Demirdas et al., 2016].
The absence of TNX throughoutthe body leads to a phenotype resem-bling the classical type of EDS. Thehallmarks of the disorders are GJH,hyperextensible, soft and/or velvetyskin, without the typical atrophic scar-ring seen in classical EDS, easy bruising,and an autosomal recessive inheritancepattern.
�
Reproductive, including pregnancyEgging et al. [2008] retrospectivelyinvestigated genitourinary and obstetriccomplications in seven women withclassical-like EDS, aged 38–57 years (sixfrom the cohort of Schalkwijk et al.[2001] and Patient 1 from the series ofLindor and Bristow [2005]). Thesewomen have had a total of 13 pregnan-cies and 12 deliveries. Twowomen (onewith CAH due to 21-hydroxylasedeficiency as a contiguous gene syn-drome; one with additional spina bifidawho decided to have no biological
74 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
children) did not have any pregnancies.One out of 13 pregnancies ended inintrauterine death of the fetus, and oneout of 12 deliveries was complicatedwith post-partum hemorrhage. Nopremature births or neonatal complica-tions were reported. No urinary incon-tinence was seen. Vaginal (n¼ 1),uterine (n¼ 2), and rectal (n¼ 1)prolapse were present. One undefinedprolapse was mentioned. Three out offive women had partus-related compli-cations (vaginal uterine extirpation afteruterine prolapse, post-partum hemor-rhage, intra-uterine death at 24 weekswith post-partum hemorrhage, andprecipitous second stage during atterm deliveries). The authors con-cluded that pregnancy is without majorcomplications in TNX-deficient pa-tients, apart from one incident ofpostpartum hemorrhage. However,uterine and vaginal prolapse regularlyoccurs in TNX-deficient women, evenat a young age, suggesting laxity of thegenitourinary tissues. Furthermore, nopremature births have been observed inthe offspring; however, some patientshad been born prematurely themselves.
Demirdas et al. [2016] described thegynecologic and obstetric history ofseven women in their cohort. Three ofthese women had previously beenincluded in the study by Egging et al.[2008]. The other four women reporteda total of 10 pregnancies, two of whichended in intrauterine demise of thefetus. Furthermore, four out of 10deliveries were complicated with post-partum hemorrhage, two women hadperineal rupture, and one pregnancywas complicated by PPROM. In thiscohort, another woman was reported tohave pelvic instability without everhaving been pregnant [Egging et al.,2008].
Obviously, some caution must betaken in making conclusions and ex-trapolating data from such a small groupof TNX-deficient patients (n¼ 11)[Egging et al., 2008].
�
Age of onsetSymptoms of patients with the TNX-deficiency have been described asstarting as early as 5 years of age in agirl byHendriks et al. [2012] and 7 yearsof age by O’Connell et al. [2010].Furthermore, in some adult cases, achildhood onset of hypermobility anddermatological symptomswas reported.Demirdas et al. [2016] reported that allpatients (n¼ 17) had a clinical onset inchildhood, ranging from the neonatalage to puberty. The most encounteredinitial symptoms in this group were(sub)luxations, hypermobility, and vel-vety/hyperextensible skin. Based on thedata we found, we conclude thatpatients already experience symptomssuch as skin hyperextensibility, a velvetyskin, easy bruising/spontaneous ecchy-mosis, subluxations, and joint hyper-mobility in childhood. Piezogenicpapules of the feet and pes planus arealso apparent at the pediatric age.
�
Craniofacial featuresCraniofacial features reported in thepatients included a slight asymmetry ofthe face (n¼ 1), lax skin of the cheeks(n¼ 1), and a narrow and/or higharched palate (n¼ 4).�
Musculoskeletal systemFrequently described musculoskeletalfeatures included joint and/or muscularpains. Furthermore, one paper reportedfrequently observed deformities of thehands and feet. Twelve out of 17included patients had pes planus andfour patients had short/broad feet withbrachydactyly of the toes. Four of thepatients had deformities of the fingersand acrogeric hands [Demirdas et al.,2016].�
Skin and integumentIt is noted that all reported patients hadhyperextensible skin, frequently de-scribed to be soft and velvety ofstructure. The atrophic scars typicalfor classical EDS were not observed.Bilateral inguinal hernia was describedin a male patient and unilaterally in afemale patient. An umbilical hernia wasdescribed in a 6-year-old male.�
Ocular involvementOcular involvement was infrequentlyreported in patients with TNX-defi-cient classical-like EDS. One patientwas described to have esotropia/ambly-opia [Lindor and Bristow, 2005], an-other to have astigmatism, and a thirdpatient was described to have bilateralconjunctivochalasis. Five out of 17patients from the cohort of Demirdaset al. [2016] were described to havefrequent subconjunctival hemorrhage.
�
Dental involvementRecurrent periodontitis was reported inone, and another patient was describedto have dental crowding due to a narrowpalate.�
Cardiovascular systemPeeters et al. [2004] investigated thecardiac features in seven TNX-deficientpatients (all from the cohort of Schalk-wijk et al. [2001]). They found a systolicmurmur at the apex in one patient.Three of the seven patients were foundto have mitral valve abnormalities(billowing of the mitral valve in twopatients of the same family and a severemitral valve prolapse (MVP) in anotherpatient). Although the number ofpatients was small and such abnormali-ties are not infrequent in the generalpopulation, the authors recommendedechocardiography at baseline and if acardiac murmur appears [Peeters et al.,2004]. Subsequently, Lindor and Bristow[2005] also described a patient who hadmitral valve surgery due to a MVP.Demirdas et al. [2016] also describedcardiologic features of their patients. Fourout of 17 of the patients had hypertensionand two patients (4/17 patients werepreviously included by Peeters et al.[2004]) had mitral valve abnormalities.One patient developed a post-partumcardiomyopathy [Demirdas et al., 2016].�
Gastrointestinal systemTwo patients reported by Lindor andBristow [2005] suffered from bleeding ofgastrointestinal structures, namely thesigmoid and duodenum, secondary todiverticulitis and as complications ofspontaneous ileus. Hendriks et al.[2012] reported a gastric hemorrhagedue to ulcers in a male patient initiallyreported by Schalkwijk et al. [2001]. Hedied at the age of 57 years due to a septicshock following elective mitral valvereplacement surgery, which was compli-cated by a sinuspiriformis perforation bya transesophageal ultrasound probe[Hendriks et al., 2012; Knuijt et al.,2014]. Sakiyama et al. [2015] also pre-sented a patient who had recurrentgastrointestinal perforation due to tissuefragility (diverticulitis, spontaneous ileus
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 75
and a subsequent perforation of theduodenum). Demirdas et al. [2016] didnot observe severe gastrointestinalproblems in their patients. However,one patient had a gastric ulcer at age 16and a bowel perforation due todiverticulitis at age 48 years [Demirdaset al., 2016].
�
Neuromuscular features and motordevelopmentA total of six articles describeresearch concerning muscular func-tion in patients with TNX-deficiencyor their muscle tissue [Voermanset al., 2007, 2009b; Ottenheijmet al., 2012; Gerrits et al., 2013;P�enisson-Besnier et al., 2013;Sakiyama et al., 2015]. All papersconclude that there is some degree ofmuscle weakness in patients withTNX-deficiency. Voermans et al.[2007] studied a cohort of 40 EDSpatients, among which 10 withTNX-deficiency (six of the cohortof Schalkwijk et al. [2001], and fouradditional patients). Muscle weakness,myalgia, and easy fatigability werereported by the majority of patients,whereas all patients were able to walkindependently without aids. Mild-to-moderate muscle weakness (80%) andreduction of vibration sense (60%)were common. Other findings wereaxonal polyneuropathy (40%) onnerve conduction studies and mildmyopathic features on muscle biopsy(20%). Patients with hypermobileEDS (hEDS) caused by TNXB hap-loinsufficiency were less affected[Voermans et al., 2009b]. This wasconfirmed in a quantitative study onisometric function of the thighmuscles in seven patients (four ofthe cohort of Schalkwijk et al.[2001] and three of the other patientsin the study of Voermans et al.[2009b] and Gerrits et al. [2013]).The results showed that muscleweakness in this type of EDS ismost likely due to increased compli-ance of the series-elastic componentof muscle tissue and failure of maxi-mal voluntary muscle activation. Fur-ther proof of this concept wasobtained in single fiber study ofmuscle tissue of four of these patients(one of the cohort of Schalkwijk et al.[2001] and three of the other patientsin the study of Voermans et al.[2009b] showing that in response tothe increased compliance of theextracellular matrix in muscle ofTNX-deficient EDS patients, amarked intracellular stiffening of thesarcomere protein titin occurs. Thestiffening of titin most likely com-pensates for the muscle weakness[Ottenheijm et al., 2012]. Thereport by P�enisson-Besnier et al.[2013] presented a 42-year-oldmale patient with proximal limbmuscle weakness, subclinical heartinvolvement, minimal skin hyperex-tensibility, no joint abnormalities,and a history of easy bruising. Hehad been asymptomatic until age 30but mentioned low performancesat upper bodybuilding exercises.Since then, he experienced graduallyworsening lower limb weakness, lead-ing to inability to run from age 40,frequent falls, and the recent need of abanister for stairs. He was initiallydiagnosed as having a primary myop-athy and only later diagnosedwith EDS [P�enisson-Besnier et al.,2013].
Motor development was not stud-ied in the included papers. We detectedno comments on delayed motor devel-opment other than mild to moderatemuscle weakness.
�
Neurological features and neuromotordevelopmentCognitive development was not studiedin the included papers. Intellectualdisability was not reported.�
OtherSevere edema of the ankles and/or feetwas described in four patients.�
Family historyDemirdas et al. [2016] asked theirpatients about family history and foundthat 4/11 mothers and 5/11 fatherscomplained of (sub)luxations (n¼ 4),pes planus (n¼ 2), easy bruising (n¼ 1),artralgia (n¼ 4), hyperextensible skin(n¼ 3), hypermobility (n¼ 1), andinguinal hernia (n¼ 1). Of the 17patient’s siblings, 11 out of 26 weretested and proven heterozygous car-riers. Three of these 11 carrier siblingsreported hypermobile joints [Demirdaset al., 2016].
Genotype–Phenotype Correlationsand Penetrance
No genotype–phenotype correlationsare reported within the group. Weassume that penetrance is high, but theresearch to support this assumption islacking. Family members with a hap-loinsufficient mutation in the TNXBgene have been described to havesymptoms of joint hypermobility in60% of the cases, but more research isneeded to confirm this [Zweers et al.,2003].
Management
No specific guidelines for managementof patients with classical-like EDS areavailable. Guidelines for managementof musculoskeletal problems, skin in-volvement, cardiovascular involve-ment, and pregnancy should followthose formulated for other forms ofEDS (for reference: See “managementguidelines for the classical Ehlers–Danlos syndrome,” by Bowen et al.,this issue).
Specific management guidelinesmay include:
�
MusculoskeletalIn case of operations, special attentionfor the effect of general anesthesia and ofadequate positioning and support isimportant to prevent pressure or stretchneuropathies [Voermans et al., 2006].Furthermore, intubation and endo-scopic studies should be performedcarefully in order to prevent rupture oftrachea or esophagus [Besselink-Loba-nova et al., 2010; Hendriks et al., 2012]�
PregnancyGynecological follow-up throughoutpregnancy is not warranted based onthe retrospective study in five patients[Egging et al., 2008]. However, thesevere complications that have beenreported during insertion of a tracheatube and a transesophageal ultrasoundprobe call for a very careful handlingof patients, especially in emergency
76 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
situations. Therefore, we advise a clini-cal delivery for all patients
Differential Diagnosis
�
Classical EDS � Congenital myopathies, including col-lagen VI- and collagen XII-relateddisordersTHE CONTIGUOUSGENE SYNDROME WITHCONGENITAL ADRENALHYPERPLASIA ANDTNX-DEFICIENCY
Burch et al. [1997] first described theTNX-deficient pheno- and genotype ina male patient (26 years old) withhyperextensible skin, hypermobilejoints, easy bruising and 21-hydroxylasedeficiency. A heterozygous 30 kb dele-tion was found on chromosome 6involving both the CYP21B gene andthe TNX gene as a causative explanationfor all symptoms. They also reportedthat TNX in serum, skin andmuscle wasmeasured and absent. The authorsconcluded that a small deletion ormissense mutation had probably re-mained undetected on the maternalallele [Burch et al., 1997].
The second patient with thisContinuous gene syndrome was in-cluded in the initial series of Schalk-wijk et al. [2001] (Patient 3) andsubsequent cohorts [Egging et al.,2008; Voermans et al., 2009b; Gerritset al., 2013]. She was homozygous forthe 30-kb deletion detected in theindex case reported by Bristow. Bothher parents and two siblings wereheterozygous for the deletion andwere clinically normal, providing evi-dence of recessive inheritance in thisfamily. This 32-year female patientwas described to have recurrent (sub)luxations, hypermobile joints, hyper-extensible, and velvety skin thateasily bruises, musculoskeletal pain,and CAH. Besselink-Lobanova et al.[2010] presented the follow-up of thiscase in order to draw attention tothe severe complications encountered
during intubation. During electivesurgery at the age of 41 years (becauseof a luxation of the left knee joint) atracheal rupture developed, despitethe initially uneventful intubation.The authors acknowledge that thepatient had other anatomic risk factorsfor a tracheal rupture (obesity andshort stature for example). However,the authors also state that TNX altersthe characteristics of the ECM andtherefore advise caution when intu-bating patients with TNX-deficiency,or even to refrain from intubatingentirely [Besselink-Lobanova et al.,2010].
TNXB Haploinsufficiency
Zweers et al. [2003] studied the 20heterozygous family members of theindex cases in Schalkwijk et al.[2001] regardless of clinical symptoms.In all of these individuals, significantlyreduced serum TNX levels weredetected, and in 17 of them, theyconfirmed heterozygosity for a trun-cating TNXB mutation. Clinical ex-amination in these family membersshowed generalized joint hypermobil-ity (GJH) in nine family members(45%; all female). Skin hyperextensi-bility and easy bruising, frequently seenin the individuals with complete TNXdeficiency, were absent. Subsequently,they measured serum TNX levels (byELISA) in an unselected cohort of 80patients with hEDS. Six of thesepatients (7.5%; all female) had serumTNX levels more than 2.5 SD belowthe mean for unaffected individuals.Clinically, patients with reduced TNXlevels showed hypermobile joints, of-ten associated with joint subluxationsand chronic musculoskeletal pain. Theauthors concluded that TNXB hap-loinsufficiency is associated with hEDS[Zweers et al., 2003].
Merke et al. [2013] investigated theprevalence of a Continuous gene syn-drome in a cohort of 192 consecutiveunrelated CAH patients. TNXB hap-loinsufficiency, here termed CAH-Xsyndrome, was present in 13 patients(and two sibs). Twelve of 91 patientscarrying a CYP21A2 deletion (13%)
carried a contiguous deletion thatextended into TNXB. One patientcarried a TNXB premature stop codon.Twelve of 13 patients with CAH-X hadEDS clinical features. Patients withCAH-X were more likely than age-matched controls to have joint hyper-mobility (P< 0.001), chronic joint pain(P¼ 0.003), multiple joint dislocations(P¼ 0.004), a structural cardiac valveabnormality by echocardiography(P¼0.02), and reduced TNX expres-sion by Western blot and immuno-staining. Piezogenic papules on the feetwere also observed. A subset of parentswas investigated (five mothers, twofathers), of which three had GJH witha Beighton score of 5 or more [Merkeet al., 2013].
Morissette et al. [2015] investigatedthe genetic background of this cohortin the same natural history study(n¼ 246). Seven families (10 patients)harbored a novel TNXB missensevariant c.12174C>G,p.(Cys4058Trp)and had a clinical phenotype consistentwith hEDS. Fourteen CAH probandscarried previously described TNXA/TNXB chimeras, resulting in a CAH-X prevalence of 8.5%. This highlyconserved pseudogene-derived variantin the TNX fibrinogen-like domain ispredicted to be deleterious and disul-fide-bonded, resulting in reduced der-mal elastin and fibrillin-1 staining andaltered TGF-1 binding, and representsa novel TNXA/TNXB chimera. TNXprotein expression was normal indermal fibroblasts, suggesting a domi-nant-negative effect. They concludedthat the CAH-X syndrome is com-monly found in CAH due to 21-hydroxylase deficiency and may resultfrom various etiological mechanisms[Morissette et al., 2015]. Patients in thiscohort were considered to be hetero-zygous for the TNXB deletion, andhad reduced but not absent TNX levelsin serum. Therefore, this phenotype islikely be more in line with what isreported by Zweers et al. [2003] inpatients with reduced serum levels ofTNX, and with the reported featuresin some of the sibs who are obligatecarriers of the mutation in theiraffected family member.

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 77
CARDIAC-VALVULAR EDS(cvEDS)
History of Cardiac-Valvular EDS
In 1987 and 1988, Sasaki et al. [1987],Kojima et al. [1988], and Hata et al.[1988] reported two Japanese patientswith complete absence of the proa2(I)collagen chains, both presenting EDS-like features, including joint hypermobil-ity, skin hyperextensibility, abnormalwound healing, but also cardiac-valvularproblems.Nicholls et al. [2001] reported atotal absence of a2(I) collagen chains in a9-year-old girl with phenotypic manifes-tations of both OI and EDS, but withoutcardiovascular anomalies. A homozygoussplice site mutation led to the introduc-tion of a premature termination codon(PTC). Schwarze et al. [2004] reportedfour patients from three independentfamilies (including the patient reportedby Kojima et al. [1988]) with a rare,recessively inherited form of EDS, char-acterized by joint hypermobility, skinhyperextensibility, and severe cardiac-valvular defects, resulting from biallelicCOL1A2mutations, leading to completeabsence of proa2(I)-chains. Because ofthe severe cardiac valve problems in mostof the adult patients, this phenotype wascalled “cardiac-valvular EDS” [Schwarzeet al., 2004]. One additional child withthis condition was subsequently reportedby Malfait et al. [2006].
The exact prevalence of this rarecondition is unknown.
Mechanism of Disease
The biallelic COL1A2 mutations resultin the complete absence of proa2(I)-chains. Cells from affected individualsproduce type I collagen molecules thatcontain only proa1(I) chains. ThemRNA from the mutant alleles isunstable and degraded so that no proteinis produced. Nicholls et al. [1984]reported a 5-year-old boy with severe,progressively deforming OI (OI typeIII). No cardiac abnormalities werereported in this patient [Nicholls et al.,1984]. A homozygous 4-nucleotideframe shift deletion within the carboxy(C)-terminal propeptide of pro-a2(I)collagen was identified. This mutation
escapes nonsense-mediated mRNA de-cay (NMD) and themRNA is stable, butthe proa2(I) chains fail to fold normallyand are degraded, which eventually alsoresults in the production of pro-a1(I)homotrimers [Pihlajaniemi et al., 1984].Given that proa(I) homotrimer forma-tion alone does not lead to OI, the OIphenotype in the latter patient suggeststhat the intracellular accumulation ofmutant proa2(I) chains and the cellularalterations, resulting from a high rate ofdegradation of these chains, contributesto the skeletal phenotype. In contrast,the EDS phenotype that results fromunstable mRNA and no proa2(I) chainsreflects what appears to be a morelimited response in the ECM.
Allelic Heterogeneity
Seven different mutations have beenreported in five independent cardiac-valvular EDS patients. These includeone homozygous nonsense mutation(c.213dupC,p.(Arg99�)), and six splicesite mutations (two homozygous(c.3105þ2T>C and c.3601G>T)) andtwo compound heterozygous(c.70þ717A>G; c.1404þ1G>A andc.540þ5G>A; c.1404G>C). The pa-tient reported by Sasaki et al. [1987] wasonly analyzed at the biochemical leveland no molecular data were reported.
Clinical Description
To date, six patients from five indepen-dent families have been reported(Table S1). Their age at diagnosis rangedfrom 6 to 65 years [Hata et al., 1988;Kojima et al., 1988; Nicholls et al.,2001; Schwarze et al., 2004; Malfaitet al., 2006].
The hallmark of the condition is thesevere cardiac-valvular disease, necessi-tating valve replacement surgery at adultage, in conjunction with variable skinhyperextensibility, atrophic scarring andjoint hypermobility, and autosomalrecessive inheritance.
�
Muscoloskeletal systemThree patients were reported to haveGJH, whereas in the other three thehypermobility was restricted to thesmall joints. One patient had shoulderdislocations, pectus excavatum, andmuscle and tendon tears. One patienthad recurrent patellar dislocations. Footdeformities were reported in threepatients: A 6-year-old boy displayedpes planus with valgus heels, halluxvalgus, and subluxations of the toes; a9-year-old girl had pedes palonvalgiwith secondary shortening of Achillestendon; and in an adult man pes planusand calcaneovalgus were reported. Onepatient had increased bone fragility.
�
Skin and integumentReported skin abnormalities included:Skin hyperextensibility (n¼ 4) (rangingfrom mild to severe), soft skin (n¼ 2),atrophic scar formation (classical EDS-like) (n¼ 2), easy bruising (n¼ 2)delayed wound healing (n¼ 1), thinskin (n¼ 1), striae (n¼ 1). Inguinalhernia was reported in two males,including congenital bilateral inguinalhernia in one.�
Ocular involvementMyopia and astigmatismwas reported inone patient; one patient was reported tohave blue sclerae.�
Cardiovascular systemAll four reported adults had severecardiac-valvular problems, resulting invalve replacement surgery. A 45-year-oldmale had severemitral valve regurgitationdue to MVP, resulting in left atrium andventricle dilatation and mild ventricularhypertrophy. He also had aortic valveinsufficiency, eventually necessitatingmitral and aortic valve replacement.Post-surgery, there was dehiscence ofthemitral annulus from the ventricle, andof the aortic valve from the atrioventric-ular groove. Finally, there was massiveleakage through the left ventricularmyocardium with disintegration of theentire left ventricle, from which thepatient died. A 65-year-old woman hadmitral valve insufficiency with uncom-plicated replacement surgery. A 30-year-old male had a secundum-type atrialseptum defect (ASD), MVP with regur-gitation, and aortic valve regurgitation.He underwent mitral and aortic valvereplacement with no complications. His25-year-old brother had aortic valvereplacement because of aortic insuffi-ciency [Schwarze et al., 2004].
78 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
The two reported children had nosevere cardiovascular features, althoughmitral valve bulging was noted in one[Nicholls et al., 2001; Malfait et al.,2006].
Genotype–Phenotype Correlationsand Penetrance
All mutations result in complete absenceof the proa2(I) chains. There are noreported genotype–phenotype correla-tions. Obligate carriers displayed noovert symptoms. Penetrance is presum-ably complete.
Management
Key management guidelines focus onthe cardiovascular system.
Specific management guidelinesinclude:
–
Measurement of aortic root size andassessment of heart valves by echocar-diogram at the time of diagnosis or byage 5 years–
Yearly echocardiogram, even if theinitial echocardiogram is normal–
Cardiac valve replacement surgery – Consider bone densitometry evaluationManagement guidelines for mus-culoskeletal problems, skin, ophthal-mologic and dental follow-up, andpregnancy should follow those formu-lated for other forms of EDS (forreference: See “management guide-lines for the classical Ehlers–Danlossyndrome,” by Bowen et al., thisissue).
Differential Diagnosis
�
Classical EDS � Hypermobile EDSARTHROCHALASIA EDS(aEDS)
Synonyms: Ehlers–Danlos syndrome,type VII (VIIA, VIIB); Arthrochalasismultiplex congenita
The History of EDS ArthrochalasiaType
Hass and Hass [1958] proposed pres-ence of a distinct entity of congenitalflaccidity of the joints, which theycalled “arthrochalasis multiplex con-genita” and which may or may notinvolve skin changes. In 1973, threepatients with the condition “EDS VII”were reported with accumulation ofprocollagen in their skin and tendon[Lichtenstein et al., 1973a]. The disor-der was therefore supposed to becaused by a defect in the conversionof procollagen to collagen, resemblingdermatosparaxis in cattle, and theactivity of the converting proteinasein the cultured fibroblasts from thesepatients was found to be reduced tobetween 10 and 40% of normal[Lichtenstein et al., 1973b]. However,Steinmann et al. [1980] demonstrated,through reinvestigation of the fibro-blasts from one of the patients, thepresence of mutant pNa2(I) collagenchains (precursor procollagen chainsin which the (C)- but not theN-propeptide is cleaved off) in colla-gen extracted from skin or producedby fibroblasts and the normal activityof procollagen N-proteinase in cellextracts. They concluded the conditionto be caused by a structural abnormal-ity in the portion of the pro-a2(I)chain that is normally cleaved byN-proteinase (and other proteinases)[Steinmann et al., 1980]. Subsequently,Cole et al. [1987] found mutantpNa1(I) in a patient with similarfeatures. EDS VII was, therefore,subdivided into types VIIA andtype VIIB, depending on whetherthe a1(I) or the a2(I) chain isaffected, respectively [Beighton et al.,1998].
Prevalence of this condition isunknown.
Mechanism of Disease
Arthrochalasia EDS is caused byheterozygous mutations in eitherCOL1A1 (previously EDS typeVIIA) or COL1A2 (previously EDStype VIIB). Heterozygous mutations
that lead to entire or partial loss ofexon 6 of either COL1A1 orCOL1A2 determines lack of the N-telopeptide linking the N-propeptideto the major triple helical domain ofthe a1(I) or the a2(I) chain. Deletionof the respective 24 and 18 amino acidresidues in the pro-a1(I) and the pro-a2(I) chain results in loss of the smallglobular region of the N-propeptide(present only in the pro-a1(I) chain),the procollagen N-proteinase cleavagesite (Pro-Gln and Ala-Gln at positions4–5, respectively), the cross-linkinglysine residue at position 13 and 9,respectively, of the N-telopeptideand the first triplet of the main helicalGly-X-Y domain [Giunta et al.,1999].
Allelic Heterogeneity
Most of the mutations are splice sitemutations leading to skipping of exon 6in COL1A1 (intron 5�2A>G/T; in-tron 5�1G>A/C/T; exon 6�1G>A/C) or COL1A2 (intron 5�2A>G;intron 5�1G>A/C; exon 6�1G>A;intron 6þ1G>A/T/C; intron6þ2T>C/G) [Steinmann et al., 2002].Genomic deletions of exon 6 [Byerset al., 1997] and exon 5þ6 [Nichollset al., 2000] were also reported.
There is a registry of reportedCOLI gene variants [Dalgleish, 1998].
Clinical Description
At present, 49 patients from 36families have been published (TableS1). The ages at the publicationranged from 2.5 months to 46 years(n¼ 35; Median age, 7.5 years of age)[Steinmann et al., 1980; Eyre et al.,1985; Cole et al., 1986; Viljoen et al.,1987; D’Alessio et al., 1991; Nichollset al., 1991; Vasan et al., 1991; Chiodoet al., 1992; Pope et al., 1992; Carret al., 1994; Ho et al., 1994; Lehmannet al., 1994; Byers et al., 1997; Giuntaet al., 1999; Hudgins et al., 1999;Nicholls et al., 2000; Whitaker et al.,2009; Giovannucci Uzielli et al.,2011; Klaassens et al., 2012; Giuntaand Steinmann, 2014; Hatamochiet al., 2014].

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 79
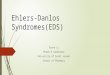
The hallmarks of the disorder aresevere generalized joint hypermobility,congenital bilateral hip dislocation, andrecurrent subluxations and dislocationsof both small and large joint[Steinmann et al., 2002] (Representative
Figure 1. Clinical photographs and radCOL1A2 and a mother and her two sons (H–bilateral hip dislocation and femoral and acerespectively. (D) An anterioposterior total boharness and bracing. (E) A left lateral total bodwith umbilical hernia, lordotic posture of thefirst son at age 14 years (I), and her second sonwith permission).
picture of the phenotype are given inFig. 1).
�
iolJ) wtabdyyspiat
Reproductive, including pregnancyAt least four affected women werereported to be pregnant, and to deliver
ogical images of patients with aEDS. A girl (Aith a c.279þ2T>C inCOL1A2. (A) X-rays of thular deformities. (B and C) Status of the hip disradiograph at age 11 years showing unsuccessfulradiograph at age 11 years showing lumbar lordosne, and foot deformities. Foot deformities of an aage 5 years (J) (Images A–G kindly provided by P
a total of 11 children, including sevenaffected ones. Pregnancy or delivery-related complications included breechpresentation (n¼ 4), PPROM (n¼ 2),polyhydramnios (n¼ 2), and decreasedfetal movement (n¼ 2).
–G) with a c.279þ1G> mutation ine hip at age 7 days showing congenitallocation at age 5 months and 3 years,treatment of the hip dislocation withis. (F and G) The patient at age 9 yearsffected mother at age 38 years (H), herrof. Maria Luisa Giovannucci-Uzielli,

80 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
Craniofacial characteristicsCharacteristic craniofacial features in-clude large fontanelle (n¼ 6), frontalbossing (n¼ 9), hypertelorism (n¼ 4),blue sclerae (n¼ 3), epicanthal folds(n¼ 3), depressed nasal bridge (n¼ 6),midfacial hypoplasia (n¼ 3), and mi-crognathia (n¼ 6).�
Musculoskeletal featuresCongenital bilateral hip dislocationwas described in all reported patients(n¼ 41). One unreported patient isknown to have had a unilateral congen-ital hip dislocation (Byers et al, personalcommunication). Joint hypermobility(n¼ 29) and recurrent dislocations orsubluxations affecting both large andsmall joints (n¼ 26) were frequent.Foot deformities (n¼ 15), includingpes equinovarus (n¼ 8), pes planus(n¼ 7), pes valgus (n¼ 2) and halluxvalgus (n¼ 6) (Fig. 1), and spinaldeformities (n¼ 13), including scoliosis(n¼ 9), kyphoscoliosis (n¼ 2), andlordosis (n¼ 3), were also frequent.Swan neck deformity of hands wasdescribed in several adults (n¼ 3).Pectus excavatum was observed insome (n¼ 3). Fractures (n¼ 9) andWormian bones on cranial radiographs(n¼ 5) suggested bone fragility, similarto patients to mild OI.�
Skin and integumentThe skin was often described to behyperextensible; hyperelastic or redun-dant (n¼ 26); soft, doughy, or velvety(n¼ 17); and/or fragile (n¼ 9). Easybruising (n¼ 12), atrophic scarring(n¼ 10), abnormal wound healing(n¼ 3), and crisscross patterning ofpalms/soles (n¼ 4) were also noted.Umbilical hernia was sometimes de-scribed (n¼ 8).�
Ocular involvementBlue sclerae (n¼ 3) and ectopia lentis(n¼ 1) were recorded.�
Dental involvementDentinogenesis imperfecta was re-corded in a few patients (n¼ 3).�
Neuromuscular features and motordevelopmentMotor developmental delay was re-corded in 16 patients, six of whomwerenot ambulatory at the time of publica-tion because of hypotonia and/or footdeformity.�
Neurological features and neuro-developmentMild learning disability was recorded ina patient with leptomeningocele andintracranial hemorrhage, presentingwith seizures, the 3rd cranial nervepalsy, left hemiparesis, and left homon-ymous hemianopsia.Genotype–Phenotype Correlationsand Penetrance
Interfamilial and intrafamilial variabilityseems to be slight [Steinmann et al.,2002]. Type I collagen consists of twoa1(I) and one a2(I) chains, thus threequarters of the collagen I molecules inaEDS due to COL1A1 mutationscontain one or two mutant pNa1(I)chains, whereas only half of the collagenI molecules in aEDS due to COL1A2mutations are affected [Steinmann et al.,2002; Giunta et al., 2008a]. Thisdifference in the stoichiometry suggeststhat COL1A1-associated aEDS mightbe more severe than COL1A2-assiatedaEDS. Because the number of patientswith a COL1A1 mutation is small, it isuncertain whether this correlation holdstrue [Giunta et al., 2008a]. Severephenotypes in patients with aCOL1A1 mutation have been de-scribed: A patient with a COL1A1“intron 5�1G>A” leading to completeloss of exon 6 presented with dermato-sparaxis EDS-like features [Nichollset al., 2000] and a patient with aCOL1A1 mutation “intron 5�2A>T”had multiple congenital dislocations anddermatosparaxis EDS-like skin features(doughty, redundant) [Giunta et al.,2008a].
Penetrance is complete.
Management
Key management guidelines focus onthe musculoskeletal system and the skin.
�
The advice to management of themusculoskeletal system is:– At diagnosis a whole body skeletalsurvey is recommended– Management of orthopedic problemsis the center of care for patients with
the disorder. Stable reductions ofcongenital hips dislocations were notachieved frequently through closedreductions with orthoses or hip spica.Anterolateral open reductions withcapsular plication were also ineffective.In contrast, open reductions with aniliac osteotomy, with or without femo-ral osteotomy, were favorable in somepatients. Appropriate surgical interven-tion is therefore difficult to plan but iscrucial for reducing the risk of recur-rence of hip dislocations, avascularnecrosis, and premature osteoarthritis[Giunta et al., 1999; Steinmann et al.,2002; Giunta and Steinmann, 2014]
– Recurrent and/or persistent disloca-tions and hypermobility of upperlimb joints are also disabling, butoperative intervention is rarely con-sidered because limited effectivenessof operative procedures is predicted[Giunta et al., 1999; Steinmann et al.,2002; Giunta and Steinmann, 2014]
– Orthotic management and earlyintervention, including physical andoccupational therapy are recom-mended to assist standing, walking,and activities of daily living [Giuntaet al., 1999; Steinmann et al., 2002;Giunta and Steinmann, 2014]
– Contact sports should be avoided toprevent dislocations
– Consider bonemineral density studies
�
The advice to management of the skin,cardiovascular, and ophthalmologicalfeatures is similar to that for patientswith classical EDS (see “managementguidelines for the classical Ehlers–Danlos syndrome,” by Bowen et al.,this issue)�
Pregnancy management– Follow-up throughout pregnancy iswarranted– Delivery should be performed in amedical center where intensive treat-ment could be given to an affectedpregnant woman and an affectedneonate
– Breech presentation is frequent if thefetus is affected. Though not de-scribed previously, affected pregnantwomen might be predisposed totearing of the perineal skin andto have postpartum extension of

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 81
episiotomy incisions as well as pro-lapse of the uterus and/or bladder, as
described in cEDSDifferential Diagnosis
�
Larsen syndrome � Classical EDS � Dermatosparaxis EDS � Kyphoscoliotic EDS � Musculocontractural EDS � Loeys–Dietz syndrome � PYCR1-related autosomal recessivecutis laxaDERMATOSPARAXIS EDS(dEDS)
Synonyms: Dermatosparaxis; Ehlers–Danlos dermatosparaxis type; EDS-VIIC; EDS7C
The History of DermatosparaxisEDS
Dermatosparaxis was first reported incattle [Lenaers et al., 1971; Hanset andLapiere, 1974] and subsequently insheep [Fjolstad and Helle, 1974], cats[Counts et al., 1980; Holbrook andByers, 1982] and dogs [Holbrook andByers, 1982]. Affected animals display aloose and extremely fragile skin (der-matosparaxis means “tearing of theskin”), resulting in large skin lacerationsduring delivery or early in life, withsubsequent infections and prematuredeath. Early ultrastructural studiesshowed alterations in the dermis ofthese animals, with loosely packed, thin,and twisted ribbon-like collagen fibrilsthat displayed a typical “hieroglyphicaspect” on cross sections, pointingtoward impaired collagen biosynthesisand fibrillogenesis. Subsequent bio-chemical studies performed on derma-tosparactic cattle revealed that theseabnormal collagen molecules werecomposed of incompletely processedtype I procollagen precursor molecules,in which the N-propeptide was insuffi-ciently cleaved [Lenaers et al., 1971].Deficient activity of the endopeptidasethat excises the N-propeptide of
procollagen chains was eventually dem-onstrated [Smith et al., 1992]. Althoughanimal dermatosparaxis was the firstrecognized collagen disorder, it tookmore than 20 years to confirm theexistence of a human counterpart forthe disorder. In 1992, three independentinfants were reported with clinical signsresembling dermatosparaxis [Nusgenset al., 1992; Smith et al., 1992].Ultrastructural studies of the dermisdemonstrated the same “hieroglyphic”pattern of the collagen fibrils as thoseobserved in dermatosparactic animals,and biochemical studies on culturedhuman fibroblasts confirmed deficientcleavage of the proa1(I) and proa2(I)N-propeptides. Seven additional pa-tients were identified subsequently, allof them displaying a severe phenotypewith an extremely fragile and lax skin,severe bruising, and a characteristicdysmorphic face, leading to a diagnosisusually within the first few months oflife. It lasted until 1999 to identify thefirst biallelic mutations in ADAMTS2,the gene encoding the procollagen I N-proteinase ADAMTS-2 (a disintegrinand metalloproteinase with thrombo-spondin motifs 2), in several patientswith the dermatosparaxis type of EDS aswell as in a strain of dermatosparacticcattle [Colige et al., 1999].
The exact prevalence of this rarecondition is unknown.
Mechanism of Disease
Dermatosparaxis EDS (dEDS) is causedby homozygous or compound hetero-zygous mutations in ADAMTS2, thegene that encodes ADAMTS-2.ADAMTS-2 is a metalloproteinase con-taining properdin repeats and a cysteine-rich domain with similarities to thedisintegrin domain of reprolysin. Thisenzyme is the main procollagen I N-proteinase, but it can also cleave the N-propeptides of type II and type IIIprocollagens [Colige et al., 2005]. Themutations result in decreased activity ofADAMTS-2, which leads to defects inprocessing of type I procollagen tomature type I collagen [Colige et al.,1999; Colige et al., 2004; Van Dammeet al., 2016]. There is an accumulation of
pN-collagen type I, resulting in poly-merization of abnormal collagen fibersthat appear thin, irregular, branched and“hieroglyphic” in cross-section.
Allelic Heterogeneity
Up till now eight biallelic mutations havebeen reported in 15 patients (14 indepen-dent families), including a recurrenthomozygous nonsense mutation p.(Gln225�) in six patients, a uniquehomozygous nonsense mutation p.(Trp795�), a homozygous in-frame skipof exons three to five a homozygous in-frame skip of exon 17 and compoundheterozygosity for an out-of-frame exon-skip of exon 3 and an in-frame skip ofexons 14–16, three homozygous loss-of-function mutations (c.2927_2928delCT,p.(Pro976Argfs�42); c.669-670dupG, p.(Pro224Argfs�41); c.2751-2A>T) andone compound heterozygous mutation(c.2T>C, p.? and c.888-891delTGAA, p.(Met295Thrfs25�)). All mutations resultin deficient activity of ADAMTS-2.
There is a registry of reportedADAMTS2 gene variants [Dalgleish, 1998]
Clinical Description
To date 15 patients from 14 independentfamilies have been reported. Threepatients were born to known consan-guineous parents (Table S1). Age atdiagnosis ranged from birth to 13 years.[Nusgens et al., 1992, Smith et al., 1992;Wertelecki et al., 1992; Reardon et al.,1995; Fujimoto et al., 1997; De Costeret al., 2003; Malfait et al., 2004; Bar-Yosef et al., 2008; Solomons et al., 2013;Van Damme et al., 2016]. Clinicalfollow-up into puberty and early adult-hood is reported for only two patients.
The hallmark of the disorder is theextreme skin fragility with redundant,almost lax skin, and the severe suscepti-bility of bruising.
�
Reproductive, including pregnancyPreterm birth was reported in ninepatients, and was preceded by PPROMin six. Mean gestational age was 34weeks and 4 days (n¼ 14, range: 28–41weeks). The umbilical cord was notedto be friable in two infants; one of them
82 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
also had a short umbilical cord thatruptured after clamping. Perinatal com-plications were reported in severalpatients. One patient died shortly afterbirth (39 weeks gestation) due to severehemorrhage and shock. A boy with agestational age of 33 weeks was bornwith multiple skull fractures and anextensive subgaleal hemorrhage. A duraltear at the site of the skull fracture led tothe development of a large cerebrospinalfluid collection, and he died due tosecondary infection at 145 days of age.Three other prematurely born infantswere admitted to a neonatal intensivecare unit for several weeks for a range ofcomplications, including cerebral hem-orrhage (n¼ 2); pneumothorax andrespiratory distress (n¼ 1); hydroneph-rosis (n¼ 1); and hypoglycemia, hypo-calcemia, and hypothyroidism (n¼ 1).No pregnancies have been reported inaffected individuals.
�
Craniofacial involvementMost patients were born with a severeand recognizable facial gestalt, includingprominent and protuberant eyes withpuffy, edematous eyelids and excessiveperiorbital skin, large fontanels and/orwide cranial sutures, a hypoplastic chinand bluish or greyish discoloration of thesclerae (n¼ 12). Less frequent findingsincluded gingival hyperplasia (n¼ 6),dental lamina cysts (n¼ 2), and general-ized hypertrichosis (n¼ 6). These pa-tients also presented extreme skin fragilitywith tearing of the skin, either at birth(n¼ 2) or within the first few years of life(n¼ 10). In addition, they had a lax andsagging skin with redundant skin folds,especially in the neck, and around wristsand ankles (n¼ 10). Together, thesefindings led to an early diagnosis in thesepatients. A number of patients displayed astrikingly milder phenotype, with ab-sence of obvious congenital facial dys-morphic features, skin fragility orredundancy. Mild dysmorphic features,skin fragility, and features of generalizedconnective tissue fragility however grad-ually became more apparent duringchildhood and adolescence.�
Musculoskeletal systemWhereas height, weight, and orofacialcircumference were usually withinnormal limits at birth, postnatal growthretardation was reported in all patients,except for those that died shortly afterbirth (n¼ 13). Eleven patients pre-sented with non-rhizomelic shorteningof the limbs and short, plump hands andfeet with stubby fingers and toes. Jointhypermobility was a consistent finding(n¼ 11), but often mild at birth.Follow-up data in older patients dem-onstrated that the joint hypermobilitybecomes more pronounced later on.Four patients had a history of fractures,including (congenital) skull fractures inthree. Several other skeletal abnormali-ties were reported, including delayedossification of the cranial vault (n¼ 3),Wormian bones (n¼ 2), delayed boneage (n¼ 2), and persistence of wovenbone in the ribs of one patient 15.Osteopenia was reported in only twopatients.
�
Skin and integumentFrequently occurring skin features,apart from the severe skin fragility(n¼ 14) and loose, lax, or hyperexten-sible skin (n¼ 15), included a soft anddoughy skin texture (n¼ 12), increasedpalmar wrinkling (n¼ 6), and atrophicscarring (n¼ 5). One of the mostconsistent clinical findings was anumbilical hernia at birth (n¼ 14).�
Ocular involvementOne patient had severe, congenitalmyopia, whereas several others pre-sented with early onset and progressivemyopia (n¼ 5). Three others hadastigmatism, and one patient developedsevere glaucoma at very young age.�
Dental involvementIn addition to gingival hyperplasia anddental lamina cysts, several other dentalabnormalities have been reported.These include microdontia (n¼ 6) oreven agenesis of several permanentteeth (n¼ 3), and tooth discoloration(n¼ 3). Abnormal morphology of themolars (n¼ 2) and severe enamel attri-tion of the deciduous teeth (n¼ 2) havebeen reported in a limited number ofpatients [De Coster et al., 2003; Malfaitet al., 2004].�
Cardiovascular systemEasy bruising was frequent (n¼ 11) andoften very severe with the formation oflarge subcutaneous hematomas. Bleed-ing problems were encountered inseven patients, ranging from severeepistaxis and gum bleeds to internaland (congenital) cerebral hemorrhages.Arterial rupture or aortic dilatation hasnot been reported so far.
�
Neuromuscular features and motordevelopmentA mild delay in gross motor develop-ment was reported in about half of thepatients (n¼ 8).�
Visceral complicationsA 9-year-old girl ruptured her dia-phragm due to postoperative vomiting.She subsequently developed a para-esopagheal hernia with incarceration ofthe stomach that was further compli-cated by the occurrence of a largeabdominal hematoma after reduction.Two patients had bladder diverticula,complicated by spontaneous bladderrupture, and two other patients devel-oped rectal prolapse with profuse analbleeding in puberty.Genotype–Phenotype Correlationsand Penetrance
The patients harboring thec.2927_2928delCT and the c.2751-2A>Tmutations have a relatively milderphenotype compared to the others.These mutations lead to introductionof a PTC. The milder phenotype couldbe due to the fact that NMD might beonly partially efficient for these allelesand some transcripts can escape NMD.As such, these alleles could producetruncated ADAMTS-2 enzymes lackingeither the last thrombospondin 1 (TSP1)domain and the PLAC (protease andlacunin) domain (c.2927_2928delCT),or the two most C-terminal TSP1domains and the PLAC domain(c.2751-2A>T) [Van Damme et al.,2016]. Interestingly, investigation ofthe N-endopeptidase activity of variousforms of recombinant ADAMTS-2 haspreviously shown that removal of one ortwo of the most C-terminal TSP1 andthe PLAC domain results in an enzymewhich is still significantly active [Coligeet al., 2005]. In addition, two othermembers of the ADAMTS family,ADAMTS-3 and ADAMTS-14, havebeen shown to possess procollagen

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 83
N-endopeptidase activity, and couldcompensate for the reduced activity ofADAMTS-2 [Fernandes et al., 2001;Colige et al., 2002; Le Goff et al., 2006].
Penetrance is presumably complete.
Management
No specific guidelines for managementof patients with dEDS are available.Management guidelines should followthose formulated for other forms of EDS(for reference: See “management guide-lines for the classical Ehlers–Danlossyndrome,” by Bowen et al., this issue).
Differential Diagnosis
�
Classical EDS � Cutis laxa syndromes � OI � Arthrochalasia EDS � RIN2 syndrome � AchondroplasiaKYPHOSCOLIOTIC EDS(kEDS) DUE TO LYSYLHYDROXYLASE 1DEFICIENCY (kEDS-PLOD1)
Synonyms: Kyphoscoliotic EDS; EDSType 6; EDS Type VIA; Ocular-scoliotic EDS; Nevo syndrome; Cutishyperelastica; Lysyl hydroxylase-deficient EDS
The History of KyphoscolioticEDS
Kyphoscoliotic EDS was the first inbornerror of human collagen metabolism tobe defined at the biochemical level, asearly as 1972. Based on a family study inwhich two sisters had marked muscularhypotonia, severe progressive scoliosisfrom birth, marked joint hypermobility,and recurrent joint dislocations [Kraneet al., 1972; Pinnell et al., 1972], theauthors found lysyl-hydroxylase defi-ciency in fibroblasts from the twosiblings that produced hydroxylysine-deficient collagen. Because the sistersalso presented microcornea, fragility ofocular tissues, and a distinct biochemical
defect, it was suggested that they beclassified as a new subtype, EDS VI, theocular type or the ocular-scoliotic type[McKusick, 1972]. Later, it was recog-nized that the ocular signs, thoughdramatic, were far less frequent thaninitially reported, prompting the Ville-franche Nosology to reclassify thedisorder as the kyphoscoliotic type ofEDS [Beighton et al., 1998]. At thattime it was recognized that in themajority of cases, the condition wascaused by the lysyl hydroxylase 1enzyme deficiency and specified as thekyphoscoliotic form of EDS (EDSVIA), whereas a rarer, clinically similarcondition with normal lysyl hydroxylaseactivity was designated EDS VIB [Stein-mann et al., 2002; Walker et al., 2004b].Thereafter, it was recognized that theNevo Syndrome, first reported in 1974,was an allelic condition to kEDS[Giunta et al., 2005a].
Recently, a number of rare autoso-mal recessive entities with distinct mo-lecular and biochemical abnormalitiesthat clinically overlap with kEDS havebeen described, and are discussed below:kEDS due to FKBP14 mutations,the Brittle cornea syndrome (BCS)(ZNF469 and PRDM5), the spondylo-dysplastic form of EDS caused bySLC39A13 mutations (previously calledspondylocheirodysplastic EDS), andmusculocontractural EDS (CHST14and DSE).
The exact prevalence of kEDS dueto lysylhydoxylase 1 deficiency isunknown.
Mechanism of Disease
kEDS-PLOD1 is caused by deficiency ofthe collagen-modifying enzyme procolla-gen-lysine, 2-oxoglutarate 5-dioxygenase1 (PLOD1 or LH1 [lysylhydroxylase1])due to homozygosity or compoundheterozygosity for mutated PLOD1 al-leles. Lysylhydroxylase 1 (LH1) plays animportant role as a post-translationalmodifying enzyme in collagen biosynthe-sis through (1) hydroxylation of helicallysyl residues in Xaa-Lys-Gly collagensequences to hydroxylysyl residueswhich serve as sites of attachment forcarbohydrate units (either galactose or
glucosyl-galactose), and (2) in the forma-tion of intra- and intermolecular collagencross-links. LH1 deficiency results inunderhydroxylation of lysyl residues andunderglycosylation of hydroxylysyl resi-dues in collagens and, hence, impairedcross-link formation with consequentmechanical instability of the affectedtissues [Rohrbach et al., 2011].
Allelic Heterogeneity
A total of 139mutations in PLOD1 havebeen identified in the 84 confirmedcases, of these there are 39 differentmutations. The 8.9 kb duplication of7 exons (exons 10–16; c.1067_1846dup) is the most common and has beenreported in 42/139 (30%) mutations (20individuals homozygotes; 2 patientscompound heterozygotes). Nine pa-tients from six families are homozygousfor the nonsensemutation p.Arg319�, allof Arab descent. The nonsense mutationp.Tyr511� has been identified in fivepatients, two of whom are homozygous.
There is a registry of reportedPLOD1 gene variants [Dalgleish, 1998].
Clinical Description
At present, 84 patients from 73 familieswith confirmed kEDS-PLOD1 (eitherby demonstration of biallelic PLOD1mutations or by urinary analysis) havebeen identified [Beighton, 1970b; Krieget al., 1979; Ihme et al., 1983; Dembureet al., 1984; Chamson et al., 1987;Wenstrup et al., 1989; Hyland et al.,1992; Hautala et al., 1993; Ha et al.,1994; Al-Gazali et al., 1997; Yeowell andWalker, 1997; Brinckmann et al., 1998;Heikkinen et al., 1999; Walker et al.,1999, 2004a, 2005; Yeowell et al., 2000a,b, 2005; Brunk et al., 2004; Giunta et al.,2005b; Yis et al., 2008; Esaka et al., 2009;Voermans et al., 2009a; Kariminejadet al., 2010; Rohrbach et al., 2011;Gok et al., 2012; Busch et al., 2014;Tosun et al., 2014; Abdalla et al., 2015].The ages at publication ranged from 5months to 54 years.Clinical featureswereadequately reported in 74 patients withkEDS-PLOD1 (either by demonstrationof biallelic PLOD1 mutations or byurinary analysis) (Table S1).

84 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
The hallmarks of the disorderinclude (congenital) kyphoscoliosis,muscle hypotonia, and joint hypermo-bility (Representative pictures of thephenotype are given in Fig. 2).
�
Reproductive, including pregnancyPregnancy of an affected fetus is usuallyuneventful although reduced fetalmovements have been reported(n¼ 7). PPROM was reported in threecases, four patients were known breechpresentation and there were threereports of oligohydramnios.Affected pregnant women may be atincreased risk for spontaneous abor-tions, premature rupture of mem-branes, and rupture of arteries. Thepatient reported by Esaka et al.[2009] experienced minor trauma at29 weeks gestation resulting in astillbirth and maternal death. Postmortem autopsy showed a spontane-ous rupture of the right iliac artery[Esaka et al., 2009]. Two affectedwomen had a total of seven pregnan-cies resulting in three miscarriages andfour healthy children, three of whomwere born vaginally at term and one ofwhom was born at 24 weeks; therewere no maternal complications[Steinmann, unpublished].Figure 2. Clinical findings in patients wmutations in PLOD1. (C) Severe kyphoscolioProf. Ebtesam Abdalla and Dr. Matthias Bau
�
ithsisma
Craniofacial featuresA number of dysmorphic features havebeen reported. However, individualcase series often report the samefeature in a number of patients. As aresult, the occurrence of certainfeatures may be over-represented.The most frequently observed featuresare high palate, epicanthal folds,down-slanting palpebral fissures, syn-ophrys and low-set ears.
�
Musculoskeletal systemKyphoscoliosis is present and usuallysevere and progressive. In most pa-tients, this is congenital (n¼ 55) butpostnatal kyphoscoliosis (n¼ 12) orscoliosis alone (n¼ 1) have beenreported. Almost all patients have jointhypermobility (n¼ 69). Joint disloca-tions/subluxations are common. Con-genital hip dislocations has beenreported in 15 patients and post-natalhip dislocation in an additional threepatients. Besides hip, shoulder(n¼ 12), knee (n¼ 5), and wrist(n¼ 2) were the most commonlynoted dislocations/subluxations. Gen-erally, recurrent dislocations werenoted in 18 patients. Hand deformitieswere noted in 13 patients. Footdeformities were also noted in 17,which included four cases of talipeskEDS: (A and B) Kyphoscoliosis in two unrelain a patient homozygous for a causative mutation inn, with permission).
equinovarus. Pes planus was reportedin 11 patients.
A marfanoid habitus has beenreported in 19/74 patients. Arach-nodactyly was reported in eightseparate patients. High palate wasrecorded in 11 patients, and inassociation with arachnodactyly infive, or with marfanoid habitus inthree patients. A pectus deformitywas observed, with pectus excavatumbeing more common (n¼ 12) thanpectus carinatum (n¼ 2). Osteopenia(n¼ 17) or osteoporosis (n¼ 2) wassometimes seen on X-ray; however,fractures were not reported in anypatients.
�
Skin and integumentSkin abnormalities are almost univer-sally described. Skin hyperextensibility(n¼ 48) and soft, doughy, or velvetyskin (n¼ 43) were most frequentlyobserved. Fragility was reported(n¼ 26) with easy bruising (n¼ 26);thin, translucent skin (n¼ 8); andabnormal wound healing (n¼ 17).Atrophic scarring was reported in 35patients. Criss-cross patterning of thepalms was only reported in one patient.Hernia was reported in 12 patientsincluding six umbilical and fiveinguinal.ted patients homozygous for causativen FKBP14 (Images kindly provided by

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 85
�
Ocular involvementOphthalmic features are variable andinclude bluish sclerae (n¼ 18), mi-crocornea (n¼ 16), and myopia(n¼ 16). Rupture of the eye globe,following minimal trauma has beenreported in five individuals includingone patient with both eyes affected[Beighton, 1970a; Pinnell et al.,1972; Ihme et al., 1983; Kariminejadet al., 2010].�
Cardiovascular systemMedium-sized vessel rupture has beenreported in several individual casereports. These events appear to bemore prevalent from teenage years andinto adulthood; however, there havebeen six cases of antenatal/neonatalbrain haemorrhage [Wenstrup et al.,1989; Yeowell and Walker, 1997;Yeowell et al., 2000a; Giunta et al.,2005b; Rohrbach et al., 2011; Tosunet al., 2014]. Arterial rupture has beenreported in various locations and duringpregnancy as mentioned above [Esakaet al., 2009].In one of the first reported siblings[Beighton, 1970b], the sister diedfrom a dissecting aortic aneurysm atthe age of 50 and the brother had acerebral bleed in the distribution of theright middle cerebral artery at theage of 19. Dembure et al. [1984]reported a patient, who was thenfollowed up by Ha et al. [1994] whohad a spontaneous arterial rupture intohis upper thigh at the age of 15. InWenstrup et al. [1989], one patienthad a rupture of a vertebral arteryand another patient had multipleruptures of the femoral artery andtwo episodes of spontaneous intra-thoracic arterial rupture. Brinckmannet al. [1998] reported two patientswith vascular complications; onesuffered a stroke at the age of 15 yearsand subsequently at age 30 years,he had spontaneous bleeding ofminor pancreatic arteries; and atage 32 years, he had spontaneousbleeding from branches of theright profundal femoral artery[Brinckmann et al., 1998; Buschet al., 2014]; another patient had ananeurysm of the mesenteric artery age12 years.
The patient reported by Yeowellet al. [2000a] had an intracranialhaemorrhage and brachial plexus inju-ries at birth; he had dextrocardia andmild aortic root dilatation with mildaortic insufficiency due to a biscuspidaortic valve and he died from arterialrupture age 14 years. Voermans et al.[2009a] followed-up patient 7 fromGiunta et al. [2005b] who had aruptured aneurysm of the left poplitealartery at the age of 15 years. Rohrbachet al. [2011] reported a 27-year-old manwith chest symptoms who duringcoronary angiography had a spontane-ous dissection of the ramus interven-tricularis anterior (RIVA) and maincoronary artery causing acute cardiacfailure. A Turkish boy presented with aleft brachial artery pseudo-aneurysm atthe age of 12 [Gok et al., 2012]. Therehas been one report of aortic stenosis[Ihme et al., 1983]. Another threepatients were reported to have MVP[Pinnell et al., 1972; Rohrbach et al.,2011].
�
Neuromuscular features and motordevelopmentOne of the key features of the conditionis congenital muscular hypotonia(n¼ 56), with associated feeding prob-lems (n¼ 17). Gross motor delay iscommon (n¼ 54) with varying severity,but with only one non-ambulatory case.�
Neurological features and neuro-developmentIntelligence is usually normal butlearning disabilities have been reportedin eight patients (two of thesepatients were reported to have antena-tal or perinatal intracranial bleeds)[Wenstrup et al., 1989; Rohrbachet al., 2011].Genotype–Phenotype Correlationand Penetrance
A range of clinical severity is observed inindividuals with kEDS-PLOD1 for eachof the systems discussed as detailed in theabove section [Steinmann et al., 2002;Rohrbach et al., 2011].No specific workhas been carried out looking at geno-type–phenotype correlations. There aretwo siblings with the same mutations
reported by Hyland et al. [1992]. Theyounger sibling appears be much lessseverely affected. Intrafamilial variationhas been observed.
Penetrance is complete.
Management
Key management guidelines focus onthe musculoskeletal system, skin, andthe cardiovascular system.
�
The advice to management of themusculoskeletal system is:– According to that for patients withclassical EDS (for reference: See“management guidelines for theclassical Ehlers–Danlos syndrome,”by Bowen et al., this issue)– Photographic and radiologic docu-mentation of the spine is recom-mended in view of the progressivekyphoscoliosis. Regular follow-upby an orthopedic surgeon for man-agement of kyphoscoliosis isappropriate
– Any surgery should be carried outwith caution due to the risk ofvascular complications
– Consider bone densitometry eval-uation
– Consider sleep study to assess fornocturnal hypoxemia, and night-time ventilation in case of severe
muscle hypotonia�
The advice to management of the skinis:– According to that for patients withclassical EDS (see “managementguidelines for the classical Ehlers–Danlos syndrome,” by Bowen et al.,this issue)– Routine examination for hernia and
surgical referral as necessary�
The advice for management of thecardiovascular system is:– Measurement of aortic root size andassessment of heart valves by echo-cardiogram at the time of diagnosis orby age 5 years– Echocardiogram at 5-year intervals,even if the initial echocardiogram isnormal
– Vigilant observation and control ofblood pressure can reduce the risk ofarterial rupture

86 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
– Further vascular surveillance ought
to be considered�
The advice for management of theophthalmologic system is:– Formal ophthalmologic evaluation atdiagnosis for myopia, astigmatism,and potential for retinal detachment– Routine ophthalmologic examina-tion for management of myopiaand early detection of ophthalmiccomplications
– Myopia and/or astigmatism may becorrected by glasses or contact lenses
– Laser treatment of the retina isindicated in case of imminent
detachment�
Pregnancy management– Follow-up throughout pregnancyand delivery should be performedin a specialized fetal medicine center– Measurement and monitoring ofaortic root size by echocardiogram
during pregnancyDifferential Diagnosis
�
Kyphoscoliotic EDS-FKBP14 � Brittle cornea syndrome � Spondylodysplastic EDS � Musculocontractural EDS � Classical EDS � Congenital myopathies, including col-lagen VI and collagen XII-associatedmyopathies (myopathic EDS)�
Metabolic disorders � Vascular EDS � Marfan syndrome � Loeys–Dietz syndromeKYPHOSCOLIOTIC EDS(kEDS) DUE TOFKBP22-DEFICIENCY(kEDS-FKBP14)
Synonyms: FKBP14-related EDS,FKBP22-deficient EDS
The History of KyphoscolioticEDS (kEDS) due to FKBP22-Deficiency (kEDS-FKBP14)
Baumann et al. [2012] reported fivefamilies with an autosomal recessive
variant of EDS, characterized by severecongenital muscle hypotonia, joint hy-permobility, skin hyperextensibility,progressive kyphoscoliosis, and sensori-neural hearing loss. The condition wasshown to be caused by biallelic muta-tions in FKBP14 [Baumann et al.,2012]. In view of the major clinicaloverlap of this phenotype with kEDS-PLOD1, both conditions are groupedwithin the same clinical entity (“Ky-phoscoliotic EDS” in the new EDSclassification).
Baumann et al. [2012]reported five families with anautosomal recessive variant ofEDS, characterized by severecongenital muscle hypotonia,joint hypermobility, skin
hyperextensibility, progressivekyphoscoliosis, and
sensorineural hearing loss.The condition was shown to
be caused by biallelicmutations in FKBP14.
The prevalence of kEDS-FKB14 isunknown.
The Mechanisms of Disease
FKBP14 encodes FKBP22, a member ofthe F506-binding family of peptidyl-prolyl cis–trans isomerases found in thelumen of the endoplasmic reticulum(ER), where it is thought to catalyzecis–trans-isomerization of peptidyl-prolylpeptide bonds and to accelerate proteinfolding, particularly of procollagens[Galat, 2003]. FKBP22 interacts withtypes III, VI, andX collagen, but does notshow direct binding to other types ofcollagen, such as type I or V collagen[Ishikawa and Bachinger, 2014]. Defi-ciency of FKBP22 was shown to result inenlargedERcisterns indermal fibroblasts,and an altered assembly of the ECM[Baumann et al., 2012].
Allelic Heterogeneity
Four different FKBP14 mutations havebeen identified to date [Baumann et al.,2012; Aldeeri et al., 2014; Murray et al.,2014; Dordoni et al., 2016]. Thec.362dup, p.(Glu122Argfs�7) has beenidentified in homozygous state in fiveindependent families. Furthermore, thismutation was twice identified in com-pound heterozygosity with anothermutation: One with a nonsense muta-tion (c.42_60del, p.(Thr15�)) and oncewith a 3-bp deletion (c.573_576del, p.(Gly191del)). A homozygous deletionof four amino acids was recentlyreported: c.197þ5_197þ8delGTAA[Alazami et al., 2016].
Clinical Description
To date, 10 patients with kEDS-FKBP14 from nine independent fami-lies have been described: Five pediatric(<12 years), three adolescents (16 years),and two adults (42- and 48-year-old)(Table S1) [Baumann et al., 2012,Aldeeri et al., 2014, Murray et al.,2014, Alazami et al., 2016, Dordoniet al., 2016]. Sufficient clinical data areavailable for nine patients.
The hallmarks of the disorder in-clude kyphoscoliosis (either progressiveor non-progressive), severe congenitalmuscle hypotonia with muscle atrophy,joint hypermobility, and congenital hear-ing loss (sensorineural, conductive, ormixed) (Representative pictures of thephenotype are given in Fig. 2).
�
Craniofacial featuresFacial dysmorphisms are not alwaysdescribed and a facial “gestalt” is notrecognizable. Some patients had epi-canthal folds (n¼ 3), micrognathia(n¼ 3), hypotelorism (n¼ 1), squarenasal root (n¼ 1), or long-narrow face(n¼ 1).�
MusculoskeletalKyphoscoliosis was noted at a mean ageof 12 months (range 2–18 months) andwas either non-progressive (n¼ 3) orprogressive (n¼ 7). Orthotic treat-ment seemed successful in case ofnon-progressive kyphoscoliosis, pro-gressive kyphoscoliosis required a
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 87
surgical approach. Atlantoaxial insta-bility was reported in one patient, theother patients presented uncompli-cated joint hypermobility withoutrecurrent dislocations/sprains orchronic pain (mean value of Beightonscore 7/9). Height was generallywithin the normal range, but at lowerlevel (10th–25th centile in 4 of 8), twopatients had short stature (lower thanthird centile).
�
Skin and integumentThe most distinctive cutaneous fea-tures in kEDS-FKBP14 are soft skin(n¼ 8), hyperextensible skin (n¼ 7)and hyperkeratosis follicularis(n¼ 5). Other skin features includeatrophic scarring, umbilical skin re-dundancy, and multiple mergingcomedones in a few patients. Fourpatients had a hernia, includingumbilical hernia in three and inguinalhernia in one.�
Ocular featuresOpthalmologic features include myo-pia, hypermetropia, and blue sclerae.�
HearingHearing impairment was noted inmost patients. It varied from sensori-neural (n¼ 6), to conductive (n¼ 2),or mixed. In one patient, becauseof the mixed origin of this sign,hearing improved after transtympanicdrains.�
Cardiovascular systemVascular complications were de-scribed in an adult patient, whopresented a celiac artery pseudoa-neurysm rupture at the age of 41years, and in the older likely affectedsister of a patient, likely affected butwithout molecular confirmation,who died due to unspecified aorticrupture at age 12 years. Celiac arterypseudoaneurysm rupture was ob-served in a child at age 6 years.�
Neuromuscular features and motordevelopmentMyopathic signs include muscle hy-potonia and atrophy, poor headcontrol in infancy, and delayed motordevelopment. Muscular weaknessseemed to regress with age and allof the subjects-but one-became ableto walk at the mean age of 33 months.The outcome was very variable andthe final ability to walk ranged frommyopathic gait, impossibility ofwalking without aids, to a motorself-sufficiency from 200m to 1 km.Muscle biopsy showed pathologicalresults in six patients, with myopathicchanges and/or fiber atrophy; creatinekinase was generally within the normalrange or slightly elevated and electro-myographic patterns were usually nor-mal at very young age, but sometimesmyopathic later on [Baumann et al.,2012].
�
Visceral complicationsLarge bladder diverticula (n¼ 3)or rectal prolapse (n¼ 1) werereported.Genotype–Phenotype Correlationand Penetrance
No genotype–phenotype correlationshave been described. Penetrance ispresumably complete.
Management
Key management guidelines focus onthe musculoskeletal, cardiovascular,and auditory systems. No specificguidelines for management of patientswith kEDS-FKBP14 are available.Guidelines for management ofmusculoskeletal problems, skin in-volvement, cardiovascular involve-ment, ophthalmologic and dentalfollow-up, and pregnancy shouldfollow those formulated for kEDS-PLOD1.
Specific management guidelinesshould also include hearing evaluationat initial diagnosis and annual hearingevaluation.
Differential Diagnosis
�
Kyphoscoliotic EDS-PLOD1 � Musculocontractural EDS � Spondylodysplastic EDS � Congenital myopathies, including col-lagen VI and collagen XII-associatedmyopathies (myopathic EDS)�
Vascular EDS � Classical EDS�
Marfan syndrome � Loeys–Dietz syndromeBRITTLE CORNEASYNDROME (BCS)
Synonyms: EDSVIB
History of Brittle CorneaSyndrome
Brittle cornea syndrome is a rare autosomalrecessive generalized HCTD, hallmarkedby a thin and fragile cornea that tends toperforate spontaneously or after minortrauma. It was originally described as aconstellation of brittle cornea, blue sclerae,and red hair [Ticho et al., 1980; Cameron,1993]. On the basis of overlapping clinicalfeatures, BCS and EDS kyphoscoliosistype were previously considered to repre-sent the same disorder [Cameron, 1993].Because of subtle clinical differences, thisclaim was later questioned and provenwrong on the basis of biochemical studies.In kEDS-PLOD1 there is deficient activ-ity of LH1 whereas in BCS the LH1-activity is normal [Royce et al., 1990; Al-Hussain et al., 2004].
Abu et al. [2008] first mapped theBCS gene to a 4.7Mb region onchromosome 16q24 and later identifiedrecessive mutations in ZNF469 (MIM612078). The single exon geneZNF469encodes a C2H2 zinc finger protein ofwhich the function is yet to fully beunderstood. Because not all BCS patientsharbored ZNF469 mutations, a secondlocus for BCS was suspected. This wasconfirmed by the discovery of mutationsin PRDM5 (MIM 614161) [BurkittWright et al., 2011]. PRDM5 encodesa C2H2 zinc finger protein of the PR/SET family of proteins. PRDM5was firstcharacterized as a potential tumor sup-pressor gene in the development ofseveral types of cancer [Watanabe et al.,2007, 2009; Cheng et al., 2010], but hasnow been shown to regulate transcrip-tion of collagen and several other ECMgenes in a mouse osteoblast cell line(MC3T3) [Galli et al., 2012]. In addition,expression profiling studies suggest thatboth PRDM5 and ZNF469 might bepart of a commonpathway regulating the

88 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
expression of ECM genes such asfibrillary collagens, and several studieshave suggested a role for ZNF469normal corneal development [Lu et al.,2010; Vitart et al., 2010; Vithana et al.,2011; Rohrbach et al., 2013].
The report of a single BCS familywith mutations in neither PRDM5 orZNF469 suggests the existence of athird genetics locus, but the largemajority of cases is probably attributableto mutations in ZNF469 or PRDM5[Rohrbach et al., 2013].
The exact prevalence of BCS isunknown.
Mechanism of Disease
ZNF469 encodes ZNF469, a zinc fingerprotein of unknown function, but lim-ited homology (�30%)with a number ofcollagens suggests that ZNF469 could beinvolved in collagen transcription andfibrillogenesis. Genome-wide associa-tion studies have consistently associatedsingle nucleotide polymorphisms (SNPs)in the vicinity of theZNF469 locus withcentral corneal thickness (CTT) [Luet al., 2010; Vitart et al., 2010; Vithanaet al., 2011; Hoehn et al., 2012; Ulmeret al., 2012], and pathogenic ZNF469alleles have been identified as the singlemost significant genetic risk factor in thedevelopment of keratoconus (relative riskof 12) [Lechner et al., 2014].
PRDM5 encodes a protein of thePR/SET protein family that lacks theintrinsic histon methyltransferase activityof other PR-domain containing proteins,but suppresses or activates the transcrip-tion of its target genes by recruiting thehistone methyltransferase G9a and class Ihistone deacetylases [Duan et al., 2007].In line with its role in BCS, PRDM5wasshown to regulate transcription of ECMgenes, including several collagen genesand small leucine-rich proteoglycans(SLRP) in pre-osteoblastic mouse cells.More specifically, it regulates collagentranscription and fibrillogenesis by bind-ing collagen genes andmaintainingRNApolymerase II occupancy [Galli et al.,2012].The role of PRDM5 does notappear to be limited to ECM develop-ment. Early studies focused on hyper-methylation of the PRDM5 promotor in
several types of cancer and its tumorsuppressor activity by modulating theWnt signaling pathway and expression ofoncogenes [Watanabe et al., 2007, 2009;Meani et al., 2009; Cheng et al., 2010]. Itsinvolvement invertebratedevelopmenthasbeen addressed in zebrafish studies; prdm5was shown to be essential for convergentextension movements through regulationof Wnt signaling [Meani et al., 2009].
Allelic Heterogeneity
The following ZNF469 mutations havebeen reported: 13 frameshift mutations:c.9611del, p. (Gln3206Argfs�23); c.9483delG, p.(His3162Thrfs�20); c.8901_8914dup, p.(Glu2972Glyfs�50); c.6647delA, p.(Gln2216Argfs�19); c.6444delG, p.(Gln2149Serfs�51); c.6638del,p.(Leu2210Trpfs�27); c.6027delA, p.(Gly2011Alafs�16); c.5787ins, p.(Gln1902Profs�13); c.5787delG, p.(Gln1902Argfs�6); c.3476del, p.(Gly1159Alafs�15); c.2234del, p.(Phe717Serfs�15);c.2150delT, p.(Phe717Serfs�15); andc.350dupC, p.(Gln118Thrfs�32), fivemissense mutations: c.10106G>C, p.(Arg3369Pro); c.10100G>A, p.(Cys3339Tyr); c.7508C>A, p.(Arg2478Glu); c.7424C>A, p.(Arg2478Glu);and c.5686C>G, p.(Pro1896Ala), andfour nonsensemutations: c.5353C>T, p.(Gln1785�); c.4258G>T, p.(Glu1420�);c.3304G>T, p.(Glu1109�); andc.2029G>T, p.(Gly677�).
The following PRDM5 mutationshave been reported: Three frameshiftmutations: c.1517_1527del11, p.(Val506Glufs�5); c.974delG, p.(Cy-s325Leufs�2); and c.711_714delTGTT,p.(Val238Alafs�35), one nonsensemutation (c.1768C>T, p.(Arg590�)),two missense mutations (c.320A>G,p.(Tyr107Cys) and c.17T>G, p.(Val6Gly)), one splice site mutation(c.93þ1G>A), and one multiple-exondeletion (exons 9–14) [Burkitt Wrightet al., 2011; Avgitidou et al., 2015a].
Clinical Description
To provide a comprehensive overview ofthe clinical phenotype of BCS, wereviewed the data on 51 patients(ZNF469: n¼ 32; PRDM5: n¼ 19)
(Table S1) [Al-Hussain et al., 2004; Abuet al., 2008; Christensen et al., 2010; Khanet al., 2010; Burkitt Wright et al., 2011;Al-Owain et al., 2012; Aldahmesh et al.,2012; Rohrbach et al., 2013; Ramappaet al., 2014; Avgitidou et al., 2015b; Porteret al., 2015]. Only those patients withindividual clinical andmolecular datawereincluded in the review. Their age rangedbetween 6 months and 48 years.
The hallmarks of the condition inthe thin, fragile cornea, with an in-creased risk for spontaneous cornealrupture (Representative pictures of thephenotype are given in Fig. 3).
�
Craniofacial involvementIn the experience of the authors, patientswith BCS present with a somewhatrecognizable facial gestalt, includingfrontal bossing, high palate, depressednasal bridge, and/or prominent chin.These features may however be mild.�
Musculoskeletal systemJoint hypermobilitywas a frequent finding(n¼ 40), and was sometimes complicatedby joint dislocations (n¼ 6), but appearedmostly limited to small joints. Otherfrequent features include developmentaldysplasia of the hip (DDH, n¼ 16),kyphoscoliosis (n¼ 22), foot deformities(n¼ 22) including pedes planovalgi andhallux valgus, and arachnodactyly (n¼ 6).Fractures (n¼ 5) and osteopenia/osteo-porosis (n¼ 2) have been reported in alimited number of patients.�
Skin and integumentPatients with BCS have a mild skinphenotype with soft, velvety (n¼ 16),and transparent (n¼ 11) skin. A hyper-extensible skin was noted in a minorityof patients (n¼ 3), and is often mild.Wound healing and easy bruising wassometimes delayed (n¼ 4), but atrophicscarring was absent.Soft connective tissue herniations werereported in five patients.�
OcularBCS is associated with a severe ocularphenotype. Its most striking feature is ahigh risk of corneal perforation(n¼ 36), either spontaneously or afterminor trauma, due to extreme cornealthinning (central corneal thicknessor CCT: 220–450mm, normal range520–560mm), and often leading to
Figure 3. Clinical findings of a 13 year old female BCS patient homozygous for acausativemutation in PRDM5: (A)Marfanoid habitus with heigth on P75 andweigth onP3; velvety skin, hematomas lower leg and hallux valgus bilaterally, pectus excavatum.Shoulder symmetrical, spine straight. Facial: depressed nasal bridge and/ prominentchin. (B) Blue sclerae. (C) Current protective spectacles after bilateral successful cornea-crosslinking (Images kindly provided by Dr. Marianne Rohrbach, with permission).
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 89
irreversible blindness. Ocular rupturefrequently occurred at young age, butseveral adults without ocular rupturehave been described. Prior to rupture,visual acuity in BCS patients was oftenaffected by keratoconus and/or kerato-globus (n¼ 27) and high myopia(n¼ 17). The most consistent ophthal-mic feature was blue sclerae (n¼ 49).Secondary glaucoma was reported inseveral patients (n¼ 5), particularly thosewith extensive corneal damage followingrupture. Retinal detachment and neo-vascularization were both reported once.Of note and in contrast to kEDS-PLOD1, microcornea was never ob-served. Megalocornea, on the otherhand, was reported in three cases. BCSusually presents as a generalized connec-tive tissue disorder with multi-tissueinvolvement, but one adult case withisolated ocular findings has been de-scribed [Khan et al., 2012]. This suggeststhat recessive mutations in ZNF469 andPRDM5 could be a rare cause of isolatedkeratoconus or corneal rupture. It shouldbe noted however that the majority ofBCS cases has been reported in ophthal-mological journals, and that extraocularfindings might be underestimated.
�
HearingHearing loss has been recognized as apredominant feature, but has not yetbeen comprehensively studied. Ap-proximately, one third was affectedwith hearing loss (n¼ 19). The mostfrequent type was mixed conductive/sensorineural hearing loss (n¼ 11) witha predominance of conductive hearingloss in childhood. Both inter- andintrafamilial variability with respect toage of onset and progression of deafnesswere observed. The combined hearingloss and decreased visual acuity often ledto severe sensorineural disability.
�
CardiovascularCardiovascular defects were uncom-mon, but mitral valve insufficiency hasbeen described (n¼ 3). Notably and incontrast to kEDS, vascular and visceralfragility has not been described in thecontext of BCS.Genotype–Phenotype Correlationand Prevalence
There is currently no evidence of a cleargenotype–phenotype correlation: Alltypes of mutations scattered acrossboth genes appear to cause indistin-guishable clinical phenotypes.
Penetrance is presumably complete.Individuals heterozygous for BCS-associated mutations have been reportedto have blue sclerae and small jointhypermobility. These are not always
present, and in particular may not bestriking in adult carriers. Heterozygouscarriers may have very mild cornealthinning (e.g., CCT around 500mm).Keratoconus has also been diagnosed in ayoung adult, heterozygous for a PRDM5mutation [Burkitt Wright et al., 2011].
Management
Early diagnosis (prior to ocular rupture)is possible and desirable to makeanticipatory management as effectiveas possible. The distinctive syndromicfeatures of BCS, such as DDH, kypho-scoliosis, blue sclerae, soft and/ortranslucent skin, and hypercomplianttympanic membranes, serve as impor-tant diagnostic clues in the early recog-nition of patients with this condition,particularly where they are the onlyaffected individual in their family.
Key management guidelines focuson the ocular system, with primaryprevention of corneal rupture by provi-sion of protective polycarbonate eye-glasses and careful screening of vision,but also hearing. An overview of clinicalmanagement strategies for BCS patientis given in Burkitt Wright et al. [2013].
Guidelines for management ofmusculoskeletal problems, skin involve-ment, cardiovascular problems, andpregnancy should follow those formu-lated for other forms of EDS (forreference: See “management guidelinesfor the classical Ehlers–Danlos syn-drome,” by Bowen et al., this issue).
Differential Diagnosis
�
Kyphoscoliotic EDS � Spondylodysplastic EDS � Musculocontractural EDS � OISPONDYLODYSPLASTICEDS DUE TOB4GALT7-DEFICIENCY(spEDS-B4GALT7)
Synonyms: EDS progeroid type, EDSprogeroid type 1, EDSwith short statureand limb anomalies

90 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
The History of SpondylodysplasticEDS due to b4GalT7-Deficiency(spEDS-B4GALT7)
Hernandez et al. [1979, 1981, 1986]reported five patients with EDS-featuresand features of early aging, includingwrinkled facies, significant growth failure,fine/curly hair, periodontitis, bilateralcryptorchidism, apparent intellectual def-icit. Kresse et al. [1987] reported a patientwith a similar phenotype, and showed itsskin fibroblasts converted only half ofthe core protein of the small dermatansulfate proteoglycan decorin to a matureglycosaminoglycan (GAG) bearing pro-teoglycan. This defective proteoglycanbiosynthesis was shown to result frombiallelic mutations in B4GALT7, encod-ing galactosyltransferase I [Quentin et al.,1990;Okajima et al., 1999]. Cartault et al.[2015] detected a homozygous missensemutation (c.808C>T, p.(Arg270Cys)) inB4GALT7 in a series of 22 patients withLarsen of Reunion Island syndrome(LRS), a skeletal dysplasia with clinicallyoverlaps with spEDS-B4GALT7.
In viewof the major clinical overlapof EDS caused by B4GALT7 mutationswith the phenotypes caused byB3GALT6 and by SLC39A13 muta-tions, these three conditions are nowgrouped within the same clinical entity(“Spondylodysplastic EDS”) in the newEDS classification.
In view of the major clinicaloverlap of EDS causedby B4GALT7 mutationswith the phenotypes caused
by B3GALT6 and bySLC39A13 mutations,these three conditions
are now grouped within thesame clinical entity
(“Spondylodysplastic EDS”)in the new EDSclassification.
The prevalence of spEDS-B4GALT7is unknown.
Mechanism of Disease
B4GALT7 encodes galactosyltransfer-ase I (b1,4-galactosyltransferase 7 orb4GALT7), a Golgi-resident enzyme,that is involved in synthesizing the GAGlinker region of proteoglycans. GAGsare long, unbranched polysaccharidescomposed of repeating disaccharideunits, which consist of alternatinguronic acids and amino sugars. MostGAGs are covalently attached to specificserine residues of core proteins via adefined linker region of xylose, twogalactoses and one glucuronic acid, thusassembling to proteoglycans (PG). Al-ternative addition of N-acetylglucos-amine or N-galactosylglucosamine tothe terminal glucuronic acid of thelinker region leads to the formation ofheparan sulfate (HS) or chondroitin/dermatan sulfate (CS/DS), respectively(Fig. 4). Cosynthetic modifications suchas epimerization and sulfation result inthe formation of diverse motifs in theGAG chains, that allow binding of avariety of ligands, thus regulatinggrowth factor signaling, cell adhesion,proliferation, differentiation, and motil-ity. The b1,4-galactosyltransferase 7 is aglycosyltransferase catalyzing the trans-fer of the first galactose onto the xyloseresidue of the PG core protein-GAGlinker region.
Seidler et al. [2006] studied fibro-blasts of a patient harboring the homozy-gous p.(Arg270Cys) substitution andshowed reduced b1,4-galactosyltransfer-ase 7 activity, reduced glycanation ofdecorin and biglycan, and reducedepimerization of the decorinGAG chain.In addition, morphological alterationsand intracellular accumulation of degra-dative vacuoles were seen in the patient’sfibroblasts. Analysis of the collagen fibrilsshowed that the b4GalT7-deficient cellshad an altered suprastructure, no bandedcollagen fibrils and an altered ratio of a1–a2 collagen chains. Finally theb4GalT7-deficient cells showed reduced prolifera-tion rates compared to controls. Gotteet al. [2008] analyzed structural alterationsin HS and their functional consequences
in fibroblasts harboring this mutation.They showed a reduced sulfation degreeof HS, delayed in vitrowound repair, andincreased fibronectin adhesion, impairedactin stress fiber formation, delayedcollagen gel extraction with reducedformation of pseudopodia and filopodia,and finally diminished formation ofcollagen suprastructures.
Bui et al. [2010] studied theability of mutant b4GalT7 harboringeither the homozygous p.(Arg186Asp),p.(Leu206Pro), and p.(Arg270Cys)substitution to prime GAG biosynthesisin recombinant cells. Whereas thep.(Arg185Asp) did not affect GAGbiosynthesis severely, the p.(Leu206Pro)mutation led to complete inhibition andthe p.(Arg270Cys) to significant reduc-tion of GAG biosynthesis. Molecularmodeling predicted that the p.(Leu206-Pro) mutation located in a conservedsecondary structure affected theoverall structure of the protein, whereasp.(Arg186Asp) is located in a lessstructural critical domain and the p.(Arg270Cys) in the vicinity of thesubstrate active site.
Allelic Heterogeneity
In total, seven missense and two frame-shift mutations have been reportedfor B4GALT7. The c.808C>T,p.(Arg270Cys) is most frequent. It hasonce been reported in homozygous state,once in compound heterozygosity withc.122T>C, p.(Leu41Pro), and once incompound heterozygous state withc.421C>T, p.(Arg141Trp). Further-more, the c.557C>A, p.(Ala186Asp)mutation was identified in compoundheterozygosity with the c.617T>G, p.(Leu206Pro) mutation, the c.641G>A,p.(Cys214Tyr) with c.277dup, p.(His93Profs�73) and finally a homozygousc.970T>A, p.(Cys324Ser) was reported.All mutations are localized in theluminal catalytic domain, except for thep.(Leu41Pro), which is localized inthe transmembrane domain.
Clinical Description
At present seven patients from sixfamilies with molecularly confirmed

Figure 4. Biosynthesis of theHS andCS/DSGAG chains is initiated by the attachment of a common tetrasaccharide linker region to aspecific serine residue of the core protein. This linker region is synthesized by the stepwise action of specific enzymes: Xylosyltransferase I/II (encoded byXYLT1 andXYLT2, respectively), galactosyltransferase I (b4GalT7, encoded by B4GALT7) and II (b3GalT6, encoded byB3GALT6), and glucuronyltransferase I (encoded by B3GAT3). Following completion of the linker region, the addition of the nextresidue determines whether HS or CS/DS is synthesized. CS is formed by the alternating addition of N-acetylgalactosamine (GalNAc) andglucuronic acid (GlcA) residues, which are subsequently modified by several sulfotransferases. The formation of DS requires theepimerisation of GlcA residues to iduronic acid (IdoA), an event catalyzed by dermatan sulfate epimerases I and II (DS-epi1 encoded byDSE and DS-epi2 encoded by DSEL, respectively), and subsequent 4-O-sulfation of the adjacent GalNAc residue by dermatan 4-O-sulfotransferase-1 (D4ST1, encoded by CHST14). Defects in the initiation and modification of the GAG chains are associated withdifferent EDS subtypes (indicated in black boxes). Defects in linker enzymes B4GALT7 and B3GALT6 lead to spEDS and affect theformation of both HS and CS/DS whereas alterations in DSE and CHST14 result in mcEDS and compromise the formation of DS.
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 91
spEDS-B4GALT7 have been identified(Table S1). The ages at publicationranged from 2 years to 33 years [Kresseet al., 1987, Faiyaz-Ul-Haque et al.,2004, Guo et al., 2013, Arunrut et al.,2016, Salter et al., 2016]. The clinicalfeatures reported in the patients withLRS are not included in this review.
The hallmarks of the disorderinclude short stature, muscle hypotonia,
radio-ulnar synostosis, and intellectualdisability.
�
Reproductive, including pregnancyAntenatal ultrasonography showedasymmetrical ventriculomegaly in onepatient and severe intrauterine growthretardation in another patient. Nopregnancies have been reported inaffected individuals.�
Craniofacial featuresThe most consistent craniofacial fea-tures include triangular face (n¼ 7),wide-spaced eyes (n¼ 6), proptosis(n¼ 6), narrow mouth (n¼ 5), low-set ears (n¼ 5), sparse scalp hair (n¼ 4),abnormal dentition (n¼ 4), flat face(n¼ 4), wide forehead (n¼ 4), bluesclerae (n¼ 3), cleft palate/bidif uvula(n¼ 2), high palate (n¼ 1), small jaw
92 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
(n¼ 1). Of note, none of the patientswas described to have progeroidfeatures.
�
Musculoskeletal featuresThe most consistent musculoskeletalfeatures include severe growth retarda-tion (n¼ 7), present at birth butprogressing later on, generalized jointhypermobility (n¼ 7), which wasnoted to be quite severe in severalpatients, bowing of limbs (n¼ 5), andfoot deformities (pes planus (n¼ 4), pesequinovarus (n¼ 1)). Other reportedsymptoms include dislocations/sublux-ations (n¼ 3), bilateral elbow contrac-tures or limited elbow movement(n¼ 3), syndactyly (n¼ 2), pectus car-inatum (n¼ 2), scoliosis (n¼ 1), longfingers (n¼ 4), thin fingers with bul-bous tips and broad thumbs (n¼ 1).One patient with low-impact rib andvertebral fractures in infancy receivedbisphosphonate treatment, with im-provement of bone pain and musclefunction [Salter et al., 2016].�
Skeletal X-ray imagingReported abnormalities include:Radio-ulnar synostosis (n¼ 6), meta-physeal flaring (n¼ 4), osteopenia(n¼ 4), radial head subluxation ordislocation (n¼ 3), short clavicles withbroad medial ends (n¼ 3), anteriorsplaying of ribs (n¼ 2), swedish keyfeature of the femur (n¼ 1), bulbousappearance of distal phalangeal tufts(n¼ 1), coxa valga (n¼ 1), reducedheight of vertebral bodies (n¼ 1).�
Skin and integumentHyperextensible (n¼ 6), single trans-verse palmar crease (n¼ 5), loose skin(n¼ 3), atrophic scarring (n¼ 3), softand doughy skin (n¼ 2), reducedsubcutaneous fat (n¼ 1), prominentscalp veins (n¼ 1), prominent venouspattern on chest (n¼ 1).�
Ocular featuresHypermetropia at very young age wasreported in 5/7 patients. In most ofthem, it was severe. One patient wasoperated at age 3 months for unilateralptosis. He also had astigmatism andintermittent exotropia. Small opticnerves (n¼ 1), and strabismus (n¼ 1)were reported. Arunrut et al.[2016] reported a patient with congen-ital cloudy cornea, bilateral highhypermetropia, pendular nystagmus,coloboma of iris and optic nerves, andposterior subcapsular cataracts.
�
Dental featuresYellowish teeth with defective enamelwas reported in one patient.�
HearingMild conductive hearing loss wasreported in one patient, likely relatedto cleft palate.�
Neuromuscular features and motordevelopmentMuscle hypotonia was reported in allpatients but ranged from mild to verysevere. Three patients were reported tobe “floppy” at birth, one had mildcongenital hypotonia, and the otherthree were reported to be mildlyhypotonic later in childhood. Delayedmotor development was reported in 6/7patients, but none of them remainednon-ambulatory. In none of the re-ported patients, a muscle biopsy wastaken.�
Neurological features and neuro-developmentFive patients were reported to havemildintellectual deficit. This includedspeech delay in three patients, mildlearning difficulties in one, and asomewhat more severe delay in onepatient.Genotype–Phenotype Correlationand Penetrance
Although marked differences in abilityto prime GAG biosynthesis havebeen described for different missensesubstitutions (see “Mechanism ofDisease” section), no genotype–phenotype correlations have emergedto date. It remains also unclear whythe p.(Arg270Cys) is associated witheither an EDS phenotype or withLRS. Cartault et al. [2015] hypothe-sized this could be due to the highlevels of homozygosity among theLRS population and modificationby interaction with other variantsin close linkage disequilibrium toB4GALT7.
Penetrance is presumably complete.Obligate carriers display no overt clini-cal symptoms.
Management
No specific guidelines for managementof patients with spEDS-B4GALT7 areavailable. Management guidelinesshould be tailored to the individual’sspecific problems and should followthose formulated for other forms ofEDS.
Specific management guidelinesmay include:
�
Musculoskeletal:– At diagnosis a whole body skeletalsurvey and bone densitometry studiesare recommended– In patients with recurrent fractures,bisphosphonate therapy should beconsidered, with treatment protocolsfollowing those formulated for pa-
tients with OIDifferential Diagnosis
�
Spondylodysplastic EDS-B3GALT6 � Spondylodysplastic EDS-SLC39A13 � Musculocontractural EDS � kEDS (PLOD1 and FKBP14) � ChondrodysplasiaSPONDYLODYSPLASTICEDS DUE TOB3GALT6-DEFICIENCY(spEDS-B3GALT6)
Synonyms: EDS progeroid type 2
The History of b3GalT6-DeficientEDS
In 2013, two independent researchstudies identified biallelic mutations inB3GALT6, encoding b3GalT6 (galacto-syltransferase II or b1,3-galactosyltrans-ferase 6), in two different conditions.Nakajima et al. [2013] identifiedB3GALT6 mutations in seven Japanesefamilies with spondyloepimetaphysealdysplasia with joint laxity type 1(SEMD-JL1 or SEMD-JL Beightontype) by whole exome sequencing. Inthree other families with a phenotyperesembling b4GalT7-deficient EDS,

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 93
targeted B3GALT6 sequencing subse-quently identified causal mutations in allof them. Coincidently, Malfait et al.[2013] identified B3GALT6 mutationsin three unrelated families with a pleio-tropic EDS-like connective tissue disor-der, characterized by severekyphoscoliosis, joint hypermobility andcontractures, multiple early-onset frac-tures, SEMD, skin fragility, and intellec-tual disability. Following theidentification of B3GALT6 as the causalgene for SEMD-JL1, Vorster et al.[2015] identified the same mutationsand a novel p.(Thr79Ala) mutations, alllocated in or in the vicinity of the stemregion, in eight prototype South Africanfamilies. A fewadditional patientswith anEDS/SEMDJL1 overlap phenotype havealso been reported [Sellars et al., 2014;Ritelli et al., 2015; Alazami et al., 2016].
In view of the major clinical overlapof EDS caused B3GALT6 mutations,with the phenotypes caused byB4GALT7 and by SLC39A13 muta-tions, these three conditions are groupedwithin the same clinical entity (“Spon-dylodysplastic EDS”) in the new EDSclassification.
The exact prevalence of spEDS-B3GALT6 is unknown.
Mechanisms of Disease
B3GALT6 encodes galactosyltransfer-ase II (b1,3-galactosyltransferase 6 orb3GalT6), a membrane Golgi-residentenzyme, that catalyzes the addition ofthe third galactose onto the secondgalactose of the GAG linker region (forintroduction, see also “Mechanism ofDisease for spEDS-B4GALT7” sec-tion). Malfait et al. [2013] showed, usingcultured dermal fibroblasts, that GAGsynthesis and activity was stronglyreduced by the homozygous or com-pound p.(Asp207His) mutation found intwo patients, as well as by the homozy-gous p.(Gly217Ser) mutation present inone of the patients. Expression of bothHS and CS GAG chains was affected inthese patients. This study also showedthat the GAG defects were associatedwith abnormal collagen structure anddelayed migration in a wound healingassay, emphasizing the role of GAG in
collagen fibril formation, as well as invarious physiological functions of con-nective tissue, such as cicatrisation.Nakajima et al. [2013] showed that arecombinant mutant, lacking the initia-tion codon (p.Met1) produced a trun-cated protein that was mislocalized tothe cytoplasm and nucleus, presumablyinactive. Also using recombinant pro-teins, they reported that both enzymemutants (p.(Ser65Gly), p.(Pro67Leu))were inactive, emphasizing the role ofthe conserved N-terminal end of thecatalytic domain in the functionalactivity of the enzyme. Other mutantsstudied, harboring mutations in thecentral or C-terminal part of thecatalytic domain, that is, p.(Asp156Asn)and p.(Cys300Ser), also exhibited se-verely impaired enzyme activity exceptfor p.(Glu174Asp) (50% loss in activity).Importantly, in the lymphoid cells ofthree SEMD-JL1 patients, the amountof HS was reduced whereas CS/DS wasincreased (2–5-fold). The molecularbasis of these observations remains tobe established. In two patients harboringa compound deletion and catalyticdomain mutation [Ritelli et al.,2015] showed by micro-array transcrip-tome and immunofluorescence analysesa reduced expression of cartilage oligo-meric matrix protein (COMP) andosteopontin (SPP1). Interestingly, theseauthors reported reduced expression anddisassembly of HS GAG chains and ofthe HS-matrix PG perlecan.
Allelic Heterogeneity
In total, 22 missense mutations, eightframeshift mutations, two in-frame dele-tions, two start codon mutations, onesplice site, and one in-frame duplicationhave been reported for B3GALT6.
Themost frequentmutation is the p.(Pro67Leu) substitution, which is fre-quent among South Africaner patients,but which was also reported in aVietnamese patient, followed by the p.(Thr79Ala) mutation, identified seventimes among South Africaner patients.Other recurrent substitutions include p.(Arg232Cys) (n¼ 4 families), p.(As-p207His) (n¼ 3 families), p.(Phe186-Leu) (n¼ 3 families), p.(Arg6Trp)
(n¼ 2 families), p.(Glu265Asp) (n¼ 2families), p.(Ser309Thr) (n¼ 2 families),and p.(Glu174Alafs�266) (n¼ 2 fami-lies). The p.(Met1?) was reported in fivefamilies.
Other reported missense mutationsinclude: p.(Val61Leu), p.(Ser65Gly), p.(Asp144Asn), p.(Asp156Asn), p.(Ser158-Tyr), p.Tyr182Cys, p.(Pro211Ser), p.(Gly217Ser), p.(Arg256Trp), p.(Ar-g261His), p.(Cys300Ser), p.(Tyr310Cys),and p.(Pro318Leu).
Other reported frameshift muta-tions are: p.(Ile76Thrfs�202), p.(Ala108Glyfs�163), p.(Asp118Alafs�160), p.(Met 139Ala141del), p.(Phe180Serfs�118), and p.(Arg197Alafs�81). Fi-nally, p.(Arg179_Arg180dup), and p.(Ala66_Arg84del) were each reportedonce.
Out of 36 families, 25 were com-pound heterozygous and 11were homo-zygous. Except for the homozygous p.(Arg179_Arg180dup), compound het-erozygosity always included a missensemutation on one of the two alleles.
Four highly deleterious mutationsare found outside the catalytic domain,one mutant lacking the initiation Metcodon (p.(Met1?), one mutant in thecytoplasmic tail (p.(Arg6Trp)), and twoin the stem region (p.(Ser65Gly) and p.(Pro67Leu)). Other mutations are lo-cated in the luminal catalytic domain.
Clinical Description
At present, 47 patients from 36 familieswith molecularly confirmed spEDS-B3GALT6 have been identified (TableS1). The ages at publication ranged frombirth to 33 years [Malfait et al., 2013;Nakajima et al., 2013; Sellars et al.,2014; Ritelli et al., 2015; Alazami et al.,2016; Honey, 2016, Van Damme et al.,unpublished]. Detailed clinical data areavailable for 36 patients. This overviewincludes the SEMD-JL1 patients re-ported by Nakajima et al. [2013], butnot those reported by Vorster et al.[2015], since detailed clinical data of thelatter patients were not available.
The hallmarks of the disorderinclude: (1) Characteristic craniofacialfeatures, (2) kyphoscoliosis, (3) jointhypermobility, mostly of distal joint,

94 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
(4) joint contractures, (5) short stature,(6) muscle hypotonia, (7) osteoporosiswith multiple fractures, (8) radiographicskeletal abnormalities compatible withSEMD, and (9) intellectual disability(Representative pictures of the pheno-type are given in Fig. 5).
�
Reproductive, including pregnancyAntenatal ultrasound abnormalitieswere reported in eight pregnancies.Reported abnormalities included pre-natal kyphoscoliosis (n¼ 2), shorteningof tubular bones (n¼ 2), contractures ofwrists and clubfeet (n¼ 1), oligohy-dramnios (n¼ 1); polyhydramnios(n¼ 1), decreased fetal movements(n¼ 1), and small cerebellum (n¼ 1).For two siblings, the pregnancy wasterminated around 22 weeks of gesta-tion because of “severe skeletaldysplasia.”Reported perinatal complications in-clude breech presentation (n¼ 3), con-genital kyphoscoliosis (n¼ 3),congenital bilateral hip dislocation(n¼ 1), bilateral clubfeet (n¼ 3), con-genital fractures (n¼ 1), cloudy cornea(n¼ 1), unilateral unilateral agnesis ofthe kidney (n¼ 1), open foramen ovale(n¼ 1), cleft palate (n¼ 3), Pierre–Robin sequence (n¼ 1), severe con-genital muscle hypotonia or floppyinfant (n¼ 2), and a cerebral hemor-rhage following vaginal delivery (n¼ 1)�
Craniofacial featuresCharacteristic craniofacial features in-clude blue sclerae (n¼ 24), frontalbossing (n¼ 21), midfacial hypoplasia(n¼ 20), downslanting palpebral fis-sures (n¼ 4), low-set, sometimes pos-teriorly rotated, ears (n¼ 19),prominent eyes/proptosis (n¼ 15),long philtrum (n¼ 15), micrognathia(n¼ 11), depressed nasal bridge (n¼ 9),small nose (n¼ 6), tooth discoloration(n¼ 5), hypoplastic teeth (n¼ 4), sparsehair (n¼ 4), high arched palate (n¼ 3),prominent chin (n¼ 2), cleft palate(n¼ 3), Pierre–Robin sequence(n¼ 1), asymmetrical skull (n¼ 2),large anterior fontanel (n¼ 1), shortneck with low hairline (n¼ 1)�
Musculoskeletal systemKyphoscoliosis is very frequent(n¼ 32), and may be congenital ordevelop during the first 24 months ofage, and is usually progressive. Severeshort stature was frequently reported(n¼ 26). While stature may be short atbirth, growth restriction usually evolvedpostnatally. Patients present joint hy-permobility (n¼ 27), either generalizedor restricted to distal joints, andsometimes complicated by dislocationsof large and small joints (n¼ 14). Jointcontractures were frequent (n¼ 21);they were either congenital, such astalipes equinovarus (n¼ 21), and/orevolved postnatally, and mostly affectedfingers (e.g., adducted thumbs, camp-todactyly), wrists, elbows, feet, andknees. Pectus deformities, either car-inatum or excavatum, were reported in8 patients. A total of 13 patients had ahistory of multiple spontaneous bonefractures and 12 had documentedgeneralized osteoporosis or osteopenia.Finger shapes were characteristicallydescribed as “slender,” “arachnodac-tyly,” or “tapering,” with “spatulate orbroad distal phalanges” (n¼ 13).
�
Skeletal X-ray imagingReported abnormalities include: Shortilia (n¼ 17), platyspondyly (n¼ 16)(described as becoming less conspicu-ous over time by Nakajima et al.[2013]), ovoid vertebra (n¼ 1), meta-physeal flaring (n¼ 13), osteopenia(n¼ 12), anterior beak of vertebralbody (n¼ 12), prominent lesser tro-chanter (n¼ 11), elbow malalignment(n¼ 10), epihyseal dysplasia femoralhead (n¼ 10), metacarpal shortening(n¼ 7), overtubulation (n¼ 6), radialhead dislocation (n¼ 5), advanced car-pal ossification (n¼ 5), bowing of longbones (n¼ 3), narrowing of long bones(n¼ 3), acetabular dysplasia (n¼ 2),vertebral listhesis (n¼ 2), radioulnarsynostosis (n¼ 1), craniosynostosis(n¼ 1), coxa valga (n¼ 1), coxa valga(n¼ 1), wedged vertebral bodies(n¼ 1), bony fusion of proximal endsof ulna and radius (n¼ 1), carpal fusion(n¼ 1). One patient had a severetorticollis at 12 months due to aposterior displacement of the vertebralcolumn, with atlanto-occipital andatlanto-axial dislocation. Two patientshad an invagination of the atlas intothe foramen magnum and anterioratlanto-axial subluxation. In two pa-tients, the cervical instability was asso-ciatedwith hydrocephalus [VanDammeet al., unpublished].
�
Skin and integumentThe skin was usually described ashyperextensible or loose (n¼ 19), softand doughy (n¼ 18), and/or thin ortranslucent (n¼ 8). In 10 patients,increased palmar wrinkling of the handswas reported. Atrophic scarring (n¼ 5)and easy bruising (n¼ 3) were rarelyreported. Other reported skin featuresinclude wrinkling of the skin on thedorsum of the hands (n¼ 1), and loose,redundant skin folds on wrists andankles (n¼ 1). Bilateral inguinal herniawas described in one patient.�
Ocular involvementRefractive errors were reported in fivepatients. Other ocular problems includemicrocornea (n¼ 1); intermittent glau-coma (n¼ 1); congenital corneal cloud-ing with sclerocornea (n¼ 1), andrepetitive retinal detachment (n¼ 1).One patient had optic nerve atrophy.�
Dental involvementDental involvement was reported in anumber of patients and includes toothdiscoloration (n¼ 5), hypoplastic teeth(n¼ 4), and early decay of teeth (n¼ 1).�
HearingHearing impairment with a conductivecomponent was described in one patient.�
Cardiovascular systemTwo patients had a dilation of theascending aorta in infancy, two patientshad a mitral valve prolapse, two patientshad an atrial septum defect, one patienthad a patent ductus arteriosus, and onepatient had a patent foramen ovale. Twopatients suffered from a cerebral hem-orrhage. One patient was reported withsevere bruising, spontaneous scalp he-matomas, and multiple hemorrhagicblisters.�
Gastro-intestinal systemConstipation was described in onepatient, and gastro-oesophageal refluxin another.�
Urogenital systemHydronephrosis was detected in onepatient, unilateral renal agenesis in one,dilatation of renal pelvis ureterocoele inone and bladder atonia in one. Onepatient developed a Wilms tumor.
Figure 5. Clinical characteristics of patients with spEDS-B3GALT6. Facial characteristics at 2 years of age (A), 6 years of age (B) and 2months of age (younger sister in panelC) include long facewithmildmicrognatia in infancy, proptotic eyeswith shalloworbits and blue tintto the sclerae. The palpebral fissures are downslanting. The nasal bridge is broad and there is a low nasal ridge. Chest showsmoderate pectusexcavatum. The limbs show significant hyperextensibility, reduced movement of distal joints that leads to absent creases of the distalinterphalangeal joints (D), increased creases of the skin of the palms (D) and club feet (E). There is muscle hypotonia, which iscompounded by the hyperextensibility of the joints and makes anti-gravitational movements difficult (F) (Images kindly provided by Dr.Roberto Mendoza-Londono, with permission).
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 95
�
Pulmonary involvementSeveral pulmonary problems werereported: Three patients were re-ported with restrictive lung disease;in one of them this was due to lunghypoplasia and a diaphragmatic her-nia. Respiratory distress due to lunghypoplasia was reported in anotherpatient. Other reports included mildrespiratory deficiency (n¼ 1), sleepapneu (n¼ 1), chronic aspiration andpneumonia (n¼ 1), and asthma(n¼ 1).�
Neuromuscular features and motordevelopmentMuscle hypotonia was reported in 16patients, and four of them had docu-mented muscle hypoplasia. Gross motordevelopmental delay, with a delay insitting and walking, was described inseven patients mainly because of musclehypotonia. The age at which unassistedwalking occurred in patients whoaccomplished ranged between 2 and7 years. Three patients remainednon-ambulatory during childhood. Inthree patients, feeding problems, due tomuscle hypotonia, were reported.
�
Neurological features and neuro-developmentTwo patients were reported with brainatrophy, and two patients had hydro-cephalus.Mild to moderate cognitive delay wassuggested in 11 patients.Genotype–Phenotype Correlationand Penetrance
No genotype–phenotype correlationshave been described.
Penetrance is complete. Obligatecarriers display no overt clinicalsymptoms.
Management
No specific guidelines for managementof patients with spEDS-B3GALT6
are available. Management guidelinesshould be tailored to the individual’sspecific problems and should followthose formulated for other forms ofEDS.
Specific management guidelinesmay include:
�
Musculoskeletal:– At diagnosis a whole body skeletalsurvey and bone densitometry studiesare recommended– In patients with recurrent fractures,bisphosphonate therapy should beconsidered, with treatment protocolsfollowing those formulated for pa-tients with OI
– Physical therapy for the contracturesand muscle hypotonia, and monitor-ing for any signs of feeding orrespiratory difficulties, in particularnocturnal hypoventilation. If thelatter is present then assisted non-interventional ventilation at night
may be indicated
96 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
Cardiovascular system:– Measurement of aortic root size andassessment of heart valves by echo-cardiogram at the time of diagnosis orby age 5 years.– Echocardiogram at 5-year intervals,even if the initial echocardiogram isnormal
– Further vascular surveillance ought
to be consideredDifferential Diagnosis
�
Spondylodysplastic EDS-B4GALT7 � Spondylodysplastic EDS-SLC39A13 � Kyphoscoliotic EDS (PLOD1 andFKBP14)�
Musculocontractural EDS � OI � Cutis laxa syndromes � Chondrodysplasia � Congenital myopathiesSPONDYLODYSPLASTICEDS DUE TOSLC39A13 MUTATIONS(spEDS-SLC39A13)
Synonyms: spondylocheirodysplasticEDS (SCD-EDS)
History of Spondylodysplastic EDSdue to SLC39A13 Mutations(spEDS-SLC39A13)
Giunta et al. [2008b] reported a “new”clinical entity caused by a mutation inthe zinc transporter gene SLC39A13.The clinical features of six patientsfrom two unrelated consanguineousfamilies were similar to those ofkEDS-PLOD1, but lack (kypho)scolio-sis and in addition presented distinctphenotypic components, includingplatyspondyly, osteopenia, short statureand widened metaphyses, tapered fin-gers, and a tendency to develop con-tractures of small joints. Because offeatures affecting mainly the spine(spondylo) and the hands (cheiro) thisvariant was termed the Spondylocheiro-dysplastic form of EDS (SCD-EDS)[Giunta et al., 2008b]. The six
patients presented with EDS-like fea-tures, short stature, finger contrac-tures, distinct radiological features,elevated ratios of lysyl pyridinolineto hydroxylysyl pyridinoline (LP/HP)(but to a lesser degree then in EDStype VIA), and underhydroxylatedcollagens in culture despite normalin vitro activities of lysyl hydroxylaseand prolyl 4-hydroxylase, respectively.The underhydroxylation was a gener-alized process which occurs along theentire molecule, and is not confined tospecific residues as shown by tandemmass spectrometry of the a1(I)- anda2(I)-chain derived peptides of colla-gen type I and involves at leastcollagen types I and II [Giunta et al.,2008a]. Subsequently, Fukada et al.[2008] reported a third family withtwo affected siblings presenting withsimilar clinical findings who werehomozygous for a missense mutationin SCL39A13 [Fukada et al., 2008].The authors furthermore generated aSlc39a13�/� knockout mouse thatrecapitulated defects observed in thepatients, thereby demonstrating thatmutations in SLC39A13 cause Spon-dylocheiro-dysplastic EDS [Fukadaet al., 2008].
In view of the clinical overlap ofEDS caused by SLC39A13 mutations,with the phenotypes caused byB3GALT6 and by B4GALT7 muta-tions, these three conditions are groupedwithin the same clinical entity (“Spon-dylodysplastic EDS”) in the new EDSclassification.
The exact prevalence of spEDS-SLC39A13 is unknown.
Mechanisms of Disease
SpEDS-SLC39A13 is caused by ho-mozygous loss-of-function mutationsin the zinc transporter geneSLC39A13. This gene encodes thehomodimeric transmembrane Zrt/irt-like protein 13 (ZIP13) protein, amember of the SLC39A/ZIP familythat regulates the influx of zinc (Znþþ)into the cytosol [Bin et al., 2011]. Thisprotein is a member of the LIV-1subfamily of ZIP zinc Transporters(LZT), a highly conserved group of
eight transmembrane domain proteinsknown to transport zinc and/or othermetal ions from the extracellular spaceor from the organellar lumen into thecytoplasm [Eide, 2006]. Mutant ZIP13proteins are easily degraded, anddisturb the intracellular Znþþ homeo-stasis [Bin et al., 2014a,b]. It has beenshown that ZIP13 loss-of-functionleads to a generalized disturbed hy-droxylation of lysyl and prolyl residuesin collagen a chains [Giunta et al.,2008b]. Since Znþþ was found to bean effective competitive inhibitor withrespect to iron (Feþþ) for prolyl4-hydroxylase and for lysyl hydroxy-lase, it was initially suggested that thegeneralized underhydroxylation of col-lagen was likely due to Znþþ overloadin the ER. Znþþ competes with Feþþ
for binding to lysyl hydroxylase,prolyl 4-hydroxylase, and prolyl 3-hydroxylase, thus impairing hydroxyl-ation of lysyl and prolyl residues[Giunta et al., 2008b]. Further studieshowever have disputed this hypothesis.One study proposed that trapping ofZnþþ in vesicular stores reduces theavailability of Zn in the ER and othercellular components and induces ERstress [Jeong et al., 2012]. Anotherstudy showed that ZIP13 is required forfull activation of BMP/TGF-b signal-ing via regulation of the intracellularlocalization of Smad proteins in con-nective tissue forming cells; this studyput forward the hypothesis that incom-plete activation of BMP/TGF-b sig-naling is responsible for the observedphenotype [Fukada et al., 2013].
Allelic Heterogeneity
Three mutations have been identified sofar in a total of eight patients from threeindependent families.
A homozygous 9-bp in-frame de-letion in exon 4, c.483_491del9 wasfound in two unrelated consanguineousfamilies originating from North-West-ern Iraq and the Southeastern part ofTurkey, respectively. At the proteinlevel, the c.483_491del9 mutation leadsto the deletion of the highly conservedamino acid residues Phe-Leu-Ala fromthe third transmembrane domain of

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 97
ZIP13 [Giunta et al., 2008b]. Thesecond mutation, a homozygous mis-sense variant c.221G>A, p.(Gly64Asp)[Bin et al., 2011] has been identified intwo siblings from Portugal [Fukadaet al., 2008]. It is localized in the secondtransmembrane domain of SLC39A13and is conserved through all vertebratespecies down to fish.
Clinical Description
To date, eight patients with spEDS-SLC39A13 from three independentfamilies have been described: Threepediatric (<12 years), two adolescents(12.5 and 14.5 years), and three adults(>20 years) (Table S1) [Fukada et al.,2008, Giunta et al., 2008b].
The hallmarks of the disorderinclude: (1) Moderate short stature; (2)hyperelastic, velvety, thin skin with aneasily visible venous pattern, and bruis-ability which leads to atrophic scars; (3)slender, tapering fingers,wrinkled palms,and considerable thenar (and hypothe-nar) atrophy; (4) distal joint hypermobil-ity which later results in contractures; (5)characteristic radiographic abnormali-ties; and (6) a ratio of urinary pyridino-lines, LP/HP, of �1.0 [Giunta et al.,2008b] (Representative pictures of thephenotype are given in Fig. 6).
�
Reproductive, including pregnancyAll affected individuals were born atterm from uncomplicated pregnancies.No pregnancies have been reported inthe affected individuals.�
Craniofacial featuresProtuberant eyes and down-slantingpalpebral fissures were described inthe majority of affected from the threefamilies.�
Musculoskeletal systemShort stature with height at the thirdcentile or below was reported for allpatients but one, whose height was atthe 10th centile at age 8.5 years. Theadult patients presented with mildlyshortened truck. Slender tapering fin-gers were also reported in the majorityof the affected.�
Skeletal X-ray imagingReported features include: platyspon-dyly, osteopenia of the axial skeleton,widening of the ends with relativenarrowing of the diaphyses and flatepiphyses of metacarpals and phalanges,small ileum, mildly flat proximal epiph-yses, and short and wide femoral necks.
�
Skin and integumentThe most distinctive cutaneous featureswere thin, velvety and fragile, easybruisable skin with atrophic, cigarettepaper-like scars. The skin of the palm ofthe hands was wrinkled in all affectedindividuals. In some individuals the skinwas translucent particularly on legs andfeet with easily visible veins.�
Ocular featuresOpthalmologic features included myo-pia, hyperopia, astigmatism, and bluesclerae.�
Dental featuresHypodontia of one or few teeth inpermanent dentition or abnormallyshaped teeth were described in allaffected individuals, but one.�
Cardiovascular systemVascular complications were describedin the male patient from Portugal whosuffered from a cerebral hemorrhageposteriorly to the left putamen at age 21years, from which he recoveredcompletely. The adult patients hadvenous varicosities on their feet andlegs in adulthood.�
Neuromuscular features and motordevelopmentThe most distinctive muscular featurewas atrophy of the thenar and thehypothenar and muscle weakness ofthe fingers. This feature was notreported in the two adult siblingsdescribed by Fukada et al. [2008].Motor development was normal.Genotype–Phenotype Correlationand Penetrance
No genotype–phenotype correlationshave been described. Penetrance ispresumably complete. Obligate carriershave no overt phenotype.
Management
No specific management guidelines havebeen reported. Guidelines for manage-ment of musculoskeletal problems, skin
involvement, cardiovascular problems,and pregnancy should follow thoseformulated for other forms of EDS (forreference: See “management guidelinesfor the classical Ehlers–Danlos syn-drome,” by Bowen et al., this issue).
MUSCULOCONTRACTURALEDS (mcEDS)
Synonyms: Adducted thumb, clubfoot,and progressive joint and skin laxitysyndrome; Adducted thumb-club footsyndrome (ATCS); D€undar syndrome;EDS Kosho type (EDS-KT); EDSmusculocontractural type 1 (EDS-MC); EDS type VIB, EDS6B; Distalarthrogtyposis with peculiar facies andhydronephrosis
The History ofMusculocontractural EDS
EDS caused by D4ST1 deficiency hasinitially been reported as three indepen-dent conditions: A rare type of arthrog-ryposis syndrome, “adducted thumb-clubfoot syndrome (ATCS)”; a specifictype of EDS, “EDS, Kosho Type(EDSKT)”; and a subset of kEDSwithout lysyl hydroxylase deficiency,“musculocontractural EDS (MCEDS),”all of which are now concluded to be asingle clinical entity [Kosho et al., 2005,Malfait et al., 2010, Janecke et al., 2011,Kosho et al., 2011, Shimizu et al., 2011].
EDS caused by D4ST1deficiency has initially beenreported as three independentconditions: A rare type ofarthrogryposis syndrome,“adducted thumb-clubfoot
syndrome (ATCS)”; a specifictype of EDS, “EDS, KoshoType (EDSKT)”; and a
subset of kEDS without lysylhydroxylase deficiency,
“musculocontractural EDS

Figure 6. Clinical and radiological findings in patients with spEDS-SLC39A13. (A) Appearance of the hand in a 10.1 years oldpatient. Excessively wrinkled palm, thenar and hypothenar atrophy, tapering fingers, and contracted thumb. (B and C) Abnormal scarformation in two patients. (D) Abnormal dentition and hypodontia. (E) Radiograph of the low thoracic and lumbar spine in a patient aged11.5 year with flattening, irregular endplates, and osteopenia of the vertebral bodies. (F) Radiograph of the hand of a 3.5 years old patientshowing alterations of shape and flat epiphyses of the short tubular bones. (G) Radiograph of the pelvis of a 10 years old patient showingsmall ilia, mild flattening of the proximal epiphyses, short and wide femoral necks (Images kindly provided by Prof. Beate Albrecht andProf. Nursel ElScioglu, with permission).
98 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
(mcEDS),” all of which arenow concluded to be a single
clinical entity.
The prevalence is unknown.
�
Adducted thumb-clubfoot syndromeD€undar et al. [1997] originally reportedon two cousins from consanguineousTurkish family, both having develop-mental delay, ocular abnormalities,characteristic facial features, generalizedjoint laxity, arachnodactyly, camptodac-tyly, and distal arthrogryposis withadducted thumbs and clubfeet. Theauthors named this condition adductedthumb-clubfoot syndrome (ATCS)[D€undar et al., 1997]. They subse-quently reported a similar patient fromanother consanguineous Turkish familywith three other similarly affectedsiblings who died of an unknownetiology in early infancy [D€undaret al., 2001]. The authors suggestedthat two brothers from a Japaneseconsanguineous family, manifestingmultiple distal arthrogryposis, charac-teristic facial features, cleft palate, shortstature, hydronephrosis, cryptorchi-dism, and normal intelligence, alsohad the syndrome [Sonoda and Kouno,2000]. Janecke et al. [2001] describedtwo affected brothers from anotherconsanguineous Austrian family, andconcluded that the syndrome wouldrepresent a new type of arthrogryposiswith central nervous system involve-ment, congenital heart defects, urogen-ital defects, myopathy, connective tissueinvolvement (GJH), and normal orsubnormal intellectual development[Janecke et al., 2001]. D€undar et al.[2009] reported that loss-of-functionmutations in CHST14 was causal for
the syndrome, through homozygositymapping using samples from previouslydescribed consanguineous families.They also described follow-up clinicalfindings of previously reported patients,including GJH, delayed wound healing,ecchymoses, hematomas, and osteope-nia/osteoporosis, from which the au-thors categorized the syndrome into ageneralized connective tissue disorder.
�
EDS, Kosho TypeIn 2000, Kosho and colleagues encoun-tered the first patient with a specific typeof EDS, and the second unrelatedpatient with parental consanguinity in2003. Both patients were Japanese girlswith characteristic craniofacial features,skeletal features (multiple congenitalcontractures, marfanoid habitus, pectusexcavatum, GJH recurrent dislocations,progressive talipes, and spinal defor-mity), cutaneous features (hyperexten-sibility, bruisability, and fragility with
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 99
atrophic scars), recurrent large subcuta-neous hematomas, and hypotonia withmild motor developmental delay[Kosho et al., 2005] which werestrikingly similar manifestations ob-served in Pakistani siblings classified ashaving a rare variant of kEDS withnormal lysyl hydroxylase activity (“EDStype VIB”) [Steinmann et al., 1975].Kosho et al. [2005] proposed that thesepatients represented a clinically recog-nizable subgroup of EDS, tentativelyclassified as EDS type VIB. Kosho et al.[2010] described four additional unre-lated Japanese patients with similarfeatures, including a patient with pa-rental consanguinity and a patientreported by Yasui et al. [2003]. Theyconcluded that these patients repre-sented a new clinically recognized formof EDS with distinct craniofacial fea-tures, multiple congenital contractures,and multisystem fragility-related man-ifestations [Kosho et al., 2010]. Thesyndrome was registered as “EDS,Kosho type” in the London Dysmor-phology Database (http://www.lmdatabases.com/index.html) and alsoin POSSUM (http://www.possum.net.au/). Miyake et al. [2010] identifiedCHST14 as the causal gene for thiscondition through homozygosity map-ping using the two consanguineousfamilies.
�
Musculocontractural EDSMalfait et al. [2010] found mutations inCHST14 through homozygosity map-ping in two Turkish sisters and an Indiangirl, both with parental consanguinity.The patients shared characteristic cra-niofacial features, joint contractures,and wrinkled palms in addition tocommon features of kEDS, includingkyphoscoliosis; joint hypermobility;muscular hypotonia; hyperextensible,thin, and bruisable skin with atrophicscarring; and ocular complications. Theauthors concluded that these patientsand those diagnosed with ATCS orEDS, Kosho type had a single clinicalcondition, which they termed “Mus-culocontractural EDS (MCEDS)”[Malfait et al., 2010].�
EDS caused by DSE deficiencyJanecke and colleagues identified ahomozygous loss-of-function DSEmutation, through positional candidategene approach, in a boy from aconsanguineous Indian family, whohad characteristic facial features, con-genital contractures of the thumbs andthe feet, joint hypermobility, muscleweakness, and atrophic scars and wasdiagnosed with MCEDS [M€uller et al.,2013]. Malfait and colleagues found amissense DSE mutation in two affectedsisters from a Spanish family, who sharedhyperextensible and fragile skin, recur-rent large hematomas, long slenderfingers, and clubfeet, but no adductedthumbs [Syxet al., 2015]. InOMIM, thesyndrome is termed as EDS, musculo-contractural type 2 (EDSMC2) to bedistinguished from EDS caused byD4ST1-deficiency termed as EDS,mus-culocontractural type 1 (EDSMC1).
Mechanisms of Disease
�
D4ST1 deficient EDSEDS caused by D4ST1-deficiency re-sults from recessive mutations in thecarbohydrate sulfotransferase 14 gene(CHST14), localized at 15q14.CHST14 is a single-exon gene encod-ing carbohydrate sulfotransferase 14 ordermatan 4-O-sulfotransferase 1 [Everset al., 2001]. D4ST1 is a Golgi-residentenzyme which is involved in thebiosynthesis of the GAG dermatansulfate, where it catalyzes 4-O-sulfationof N-acetylgalactosamine (GalNAc) inthe sequence “L-iduronic acid (IdoA)-GalNAc,” immediately after epimeriza-tion of D-glucuronic acid (GlcA) toIdoA by dermatan sulfate epimerase(DSE) [Evers et al., 2001].The sulfotransferase activity ofcos-7 cells transfected with CHST14containing p.(LysK69�), p.(Pro281Leu),p.(Cys289Ser), or p.(Tyr293Cys) muta-tions was decreased at almost the samelevel, suggesting that loss-of-functionmutations in CHST14 (i.e., D4ST1deficiency) are the basis of this disorder[Miyake et al., 2010].
Sulfotransferase activity toward DSin mutant skin fibroblasts was signifi-cantly decreased to 6.7% in a patientwiththe compound heterozygous mutation
p.(Pro281Leu)/p.(TyrY293Cys) and to14.5% in a patient with the homozygousmutation p.(Pro281Leu), comparedwith each age- and sex-matched control[Miyake et al., 2010]. Disaccharidecomposition analysis of CS/DS chainsisolated from the affected skin fibroblastsin these two patients showed a negligibleamount of DS and excess amount of CS,which was suggested to result fromimpaired 4-O-sulfation lock due toD4ST1 deficiency, followed by back-epimerization from IdoA to GlcA[D€undar et al., 2009; Miyake et al.,2010; Syx et al., 2015]. Decorin, a majorDS-PG in the skin, consists of a coreprotein and a singleGAGchain that playsan important role in assemblyof collagenfibrils, possibly through an electrostaticinteraction between decorin DS chainsand adjacent collagen fibrils. GAGchains of decorin from the affectedskin fibroblasts contained exclusivelyCS and noDS disaccharides, while thosefrom the controls contained mainly DSdisaccharides (approximately 95%)[Miyake et al., 2010; Syx et al., 2015].Light microscopy of the affected skinspecimens using hematoxylin and eosinstaining showed that fine collagen fiberswere predominantly present in thereticular to papillary dermiswithmarkedreduction of normally thick collagenbundles [Miyake et al., 2010]. Transmis-sion electron microscopy showed thatcollagen fibrils in the affected skinspecimenswere dispersed in the reticulardermis in contrast to the regularly andtightly assembled collagen fibrils ob-served in the controls and that eachcollagen fibril in affected skin specimenswas smooth and round, not varying insize and shape, similar to that in thecontrols [Miyake et al., 2010].
In view of these findings, skinfragility in patients with EDS causedby D4ST1 deficiency is postulated toresult from impaired assembly of colla-gen fibrils caused by the replacement ofa DS with a CS chain of decorinthrough alterations in the electrostaticbinding of decorin to collagen fibrilsfollowed by difference in the spatialrelationship between collagen fibrilsand decorin [Kosho, 2013; Koshoet al., 2014; Kosho, 2016].

100 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
DSE-deficient EDSEDS caused by DSE deficiency resultsfrom recessive mutations in the derma-tan sulfate epimerase gene (DSE). DSEis a Golgi-resident enzyme that cata-lyzes the epimerization of D-glucuronicacid (GlcA) toward iduronic acid(IdoA). This allows D4ST1 to catalyzethe 4-O-sulfation of the adjacentGalNAc, which then prevents back-epimerization of the IdoA to GlcA.Two homozygous missense muta-tions (p.(Arg267Gly); p.(Ser268Leu))have been detected [M€uller et al., 2013;Syx et al., 2015]. Heterologous expres-sion of mutant full-length and solublerecombinantDSE proteins harboring thep.(Ser268Leu) substitution showed a lossof activity towards partially desulfatedDS, and patient-derived fibroblastsalso showed a significant reduction inepimerase activity. The amount of DSdisaccharides was markedly decreased inthe conditionedmediumand cell fractionfrom cultured patient fibroblasts com-pared to control. No difference was seenin CS chains from the conditionedmedia, though the total amount of CSdisaccharides in the cell fraction from thepatient was increased approximately1.5-fold, consistent with increased syn-thesis or reduced conversionofCS chains[M€uller et al., 2013].
Syx et al. [2015] analyzed fibroblastsfrom a patient harboring the p.(Arg267-Gly) substitution and could show that aminor fraction of decorin DS waspresent, consisting of IdoA-containingdisaccharides, which could be attrib-uted to residual DSE activity, orcompensating DSE2 activity. In thispatient, no pronounced ultrastructuralabnormalities of dermal collagen fibrilswere noted, but immunofluorescentstainings of collagen types I, III, and Vand fibronectin showed evidence ofabnormal ECM assembly [Syx et al.,2015].
Allelic Heterogeneity
�
CHST14Mutations have been detected through-out the CHST14 gene. These include11 missense mutations, six frameshiftmutations, and two nonsense mutations.
The p.(Pro281Leu)wasmost frequent(n¼ 9), other recurrentmutations includep.(Val49�) (n¼ 3), p.(Arg213Pro) (n¼ 2),and p.(Tryr293Cys) (n¼ 4). All othermutations were reported once: p.(Arg29Gfs�113), p.(Lys69�), p.(Gln113Argfs�14), p.(Arg135Gly), p.(Leu137Gln),p.(Cys152Leufs�10), p.(Phe209Ser), p.(Arg218Ser), p.(Gly228Leufs�13), p.(Glu262Lys), p.(Arg274Pro), p.(Met280-Leu), p.(Cys289Ser), p.(Trp327Cfs�29),and p.(Glu334Glyfs�107).
�
DSETwo homozygous DSE1 missense mu-tations (p.(Arg267Gly) and p.(Ser268-Leu)) have been detected.A registry with CHST14 and DSEgene variants is available [Dalgleish,1998].
Clinical Description
At present, 39 patients (18 females, 21males) from 26 families have beenpublished with recessive CHST14mutations (Table S1). The ages ofpatients with CHST14 mutations atthe latest publication ranged from 0 dayto 59 years. [D€undar et al., 1997;Sonoda and Kouno, 2000; D€undaret al., 2001; Janecke et al., 2001; Yasuiet al., 2003; Kosho et al., 2005; Koshoet al., 2010; Malfait et al., 2010;Shimizu et al., 2011; Mendoza-Lon-dono et al., 2012; Winters et al., 2012;Voermans et al., 2012; Syx et al., 2015;Janecke et al., 2016; Mochida et al.,2016].
Three patients (one child, two adultwomen) from two families have beenpublished with recessive DSE1 muta-tions [M€uller et al., 2013; Syx et al.,2015].
The hallmarks of the disorderinclude: (1) Characteristic craniofacialfeatures, (2) congenital multiple contrac-tures, including adducted thumbs andtalipes equinovarus, (3) characteristiccutaneous features including fine palmarcreases, (4) peculiar finger shapes, (5)progressive spinal and foot deformities,(6) large subcutaneous hematomas, and(7) ophtalmological and urogenital
involvement (Representative pictures ofthe phenotype are given in Fig. 7).
�
Reproductive, including pregnancyPregnancy-related findings includehand/foot anomalies (n¼ 3), oligohy-dramnios (n¼ 2), and decreased fetalmovement (n¼ 2). No deliveries havebeen described in female patients withEDS caused by D4ST1 deficiency. Twodeliveries were described in a femalepatient with EDS caused by DSEdeficiency, followed by uterine andbladder prolapse [Syx et al., 2015].�
Craniofacial featuresCharacteristic craniofacial features in-clude a large fontanelle (n¼ 24), hyper-telorism (n¼ 36), downslantingpalpebral fissures (n¼ 35), blue sclerae(n¼ 28), short nose with hypoplasticcolumella (n¼ 17), ear deformities(n¼ 35) including low-set (n¼ 22) andposteriorly rotated (n¼ 14) ears, highpalate (n¼ 21), long philtrum and/orthin upper lip vermilion (n¼ 24), andsmall mouth and/or micro-retrognathia(n¼ 16) at birth to early childhood.Slender facial shapes with protrudingjaws (n¼ 11) and facial asymmetry(n¼ 8) are evident from adolescence.�
Musculoskeletal systemMild prenatal growth restriction wassuggested: Mean birth length �0.5 SDand median�0.6 SD (n¼ 9; range, from�1.6 to þ1.3 SD); mean birth weight�0.6 SD and median�0.67 SD (n¼ 11;range, from�2.0 toþ0.5 SD); andmeanbirthoccipital frontal circumference�0.2SD and median �0.5 SD (n¼ 8; range,from �1.0 to þ1.0 SD) [Shimizu et al.,2011]. Mild postnatal growth restrictionwas suggested with slenderness andrelative macrocephaly: Mean height�0.9 SD and median �0.6 SD (14 datapoints from 12 patients; range, from�3.9toþ1.2 SD); mean weight�1.5 SD andmedian �1.4 SD (11 data points from 9patients; range, from �2.4 to �0.4 SD);and mean occipital frontal circumference�0.2 SD and median 0.0 SD (10 datapoints from 8 patients; range, from �1.2to >2.0 SD) [Shimizu et al., 2011].Multiple congenital contractureswere cardinal features and typicallyincluded adduction-flexion contracturesof the thumbs (n¼ 32; no adducted

Figure 7. A female patient with mcEDS-CHST14. Facial characteristics at age 23days (A) and 24 years (B). (A and C) Congenital contractures of fingers includingadducted thumbs (A) and cylindrical fingers at age 24 years (C). (D) Characteristicwrinkling palmar creases. (E) Left talipes equinovarus. (F) progressive foot deformities atage 15 years. (G) A large subcutaneous hematoma at age 6 years (Images kindly providedby Dr. Tomoki Kosho, with permission. A and E, originally published in Kosho et al.[2010], in American Journal of Medical Genetics;G, originally published in Kosho et al.[2005], in American Journal of Medical Genetics).
RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 101
thumbs in seven and data not available intwo) and talipes equinovarus (n¼ 42).Finger shapes were characteristically de-scribed as “arachnodactyly,” “tapering,”“slender,” or “cylindrical” (n¼ 36). Pro-gressive talipes deformities (planus, valgus,or severer) (n¼ 27) and spinal deformities(decreased physiological curvature, scolio-sis, or kyphoscoliosis) (n¼ 23) wereobserved. Marfanoid habitus (n¼ 13);
recurrent, chronic or easy joint dislocations(n¼ 19), and pectus deformities (flat andthin, excavatum, or carinatum) (n¼ 18)were also noted.
�
Skin and integumentSkin hyperextensibility (from child-hood) and redundancy (from adoles-cence) (n¼ 24), bruisability (n¼ 22),and fragility with atrophic scars (n¼ 23)were common. Acrogeria-like finepalmar creases or wrinkles were char-acteristic and became evident withaging (n¼ 29). Hyperalgesia to pressurewas suggested (n¼ 8) because patientsdisliked being hugged in infancy ordisliked blood pressure measurement inthe upper arms. Recurrent subcutane-ous infections with fistula formationwere also observed (n¼ 8).
�
Ocular involvementRefractive errors, typically myopia(n¼ 12) followed by astigmatism(n¼ 5) and hyperopia (n¼ 4), weredescribed in 16 patients; strabismus in13 patients; microcornea in 13; glau-coma or elevated intraocular pressurein eight; and retinal detachment inseven. Progressive visual field loss wasdescribed in a 31-year-old female[Kosho et al., 2010], deterioration invision of the right eye because of thelacquer crack in Bruch’s membraneadjacent to right fovea in a 15-year-oldmale [Syx et al., 2015], and right-sidedblindness because of retinal detach-ment in a 45-year-old female [Janeckeet al., 2016].�
HearingHearing impairment was described innine patients (specified for high-pitchedsounds in five).�
Cardiovascular systemRecurrent large subcutaneous hema-tomas (skull, extremities, or hips) area serious complication that can, evenafter minor trauma, progress acutelyand massively to hemorrhagic shockrequiring intensive treatment (hos-pital admission, blood transfusion, orsurgical drainage) (n¼ 21). Intranasaladministration of 1-desamino-8-D-arginine vasopressin (DDAVP) aftertrauma effectively prevented largesubcutaneous hematomas in threepatients [Kosho et al., 2010; Janeckeet al., 2016]. Congenital heart de-fects, typically ASD, were detected inseven patients. Valve abnormalitiesand/or aortic root dilatation werealso detected in seven patients.Infectious endocarditis occurred intwo patients: One was successfullytreated with surgical resection of thevegetation [Kosho et al., 2010] andthe other expired [Janecke et al.,2016].
102 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
Gastro-intestinal systemConstipation was described in ninepatients. Two adults and one adolescentpatient had colonic diverticula perfora-tion, corrected surgically [Kosho et al.,2010; Kono et al., 2016]. One adoles-cent patient had a severe progressivegastric ulcer, treated with partialgastrectomy [Kosho et al., 2010].Complications associated with gastro-intestinal malformations included acommon mesentery, spontaneous vol-vulus of the small intestine associatedwith absent gastrocolic omentum[Janecke et al., 2001], and duodenalobstruction due to malrotation [Malfaitet al., 2010].�
Urogenital systemHydronephrosis was detected in eightpatients. It was caused by renal ptosis inone patient, who underwent laparo-scopic placement of a ureteral stent,complicated by severe hemorrhage dueto tissue fragility [Malfait et al., 2010].Another patient had a pelviuretericjunction obstruction requiring neph-rostomy in the neonatal period [Syxet al., 2015]. Nephrolithiasis or cysto-lithiasis was described in six patients,and recurrent urinary tract infection inthree. Cryptorchidism was observed inmost male patients. One patient whounderwent orchidopexy developed hy-pogonadism in adulthood.�
PulmonaryPneumothorax or pneumohemothoraxoccurred in three adult patients, whowere treated with chest tube drainage[Kosho et al., 2010].�
Neuromuscular features and motordevelopmentMuscle hypotonia or weakness wasdescribed in 17 patients. A myopathicprocess was suggested as the cause of themuscle weakness in a patient. Electro-myographic examination demonstratedmuscle action potentials with reducedamplitude but with a normal distallatency time and nerve conductionvelocity, and muscle biopsy revealedno histological abnormalities [D€undaret al., 1997]. In another patient,quantitative muscle ultrasonographyshowed increased echo intensity in theforearm extensors and anterior tibialmuscles aswell asmarkedbilateral atrophyof the forearm flexors, forearm extensors,and quadriceps. Nerve conduction stud-ies showed low compound muscle actionpotential amplitudes in the distal muscles.Needle electromyography showed anabnormal and mixed pattern of short-duration, low-amplitude, polyphasicmo-tor units, aswell as polyphasicmotor unitswith a longer duration and higheramplitude, reflecting an increase in fibersize diameter.Muscle biopsy showed fibertype 1 predominance without fiber typegrouping, increased variation in thediameter of both type 1 and type 2 fibers,and some type 1 fibers in close proximityto lobulated fibers. These findings werecompatible with a myopathy, similar toother EDS types [Voermans et al., 2012].Elevation of serum CK (creatine kinase)level was described in four patients (277,698, 1838, 3000 IU/L) [Janecke et al.,2016].Gross motor developmental delay wasdescribed in 23 patients mainly becauseof muscle hypotonia. The median age atwhich unassisted walking occurred inpatients who accomplished it was 2 years4 months (n¼ 10; range, from 1 year 5months to 4 years). One adult patientcould not walk unassisted because ofsevere foot deformities and leg muscleweakness [Kosho et al., 2010].
�
Neurological features and neuro-developmentVentricular enlargement was describedin six patients and asymmetry in threeon brain ultrasonography, computedtomography, or magnetic resonanceimaging. Additional minor findingswere also recorded: Absence of theleft septum pellucidum [Janecke et al.,2001], a short corpus callosumwith lackof an isthmus and well-defined rostrum,mild prominence of the Sylvian fissures,and a few small gray matter heterotopiasalong the lateral walls of the temporalhorns of the lateral ventricles [Men-doza-Londono et al., 2012], absence ofthe septum pellucidum, hypoplasia ofthe inferior vermis with a normallysized posterior fossa (Dandy–Walkervariant), hypoplasia of the hippocampiand splenium of the corpus callosum,and hypoplasia of the optic nerves(septo-optic dysplasia) [Winters et al.,2012] and mild cerebellar hypoplasia,hypoplasia of the cerebellar vermis(reminiscent of Dandy–Walker variant),and absence of the septum pellucidum[Syx et al., 2015]. Spinal cord tetheringwas noted in three patients, two ofwhom underwent corrective surgery.Mild intellectual delay was suggested inthree patients; one reportedly hadglobal psychomotor delay in infancy,but his IQ was around 90 at the age of7 years 2 months [D€undar et al., 1997;Janecke et al., 2011].
�
OtherPoor breast development was noted inseven female patients beyondadolescence.Genotype–Phenotype Correlationand Penetrance
Penetrance is complete, whereas differ-ences in phenotypic severity amongaffected siblings have been suggested.No apparent genotype–phenotype cor-relations have been described amongpatients with EDS caused by D4ST1deficiency. Phenotypic features in threepatients with EDS caused by DSEdeficiency seemed to be milder thanthose in patients with EDS caused byD4ST1 deficiency, presumably associ-ated with the glycobiological findingthat some DS moieties were present inthe decorin GAG in the fibroblastsderived from patients with EDS causedby DSE deficiency, whereas DS wascompletely replaced by CS in thefibroblasts derived from patients withEDS caused by CHST14/D4ST1 defi-ciency [Syx et al., 2015].
Management
Management should be comprehensiveespecially focusing on musculoskeletal,cutaneous, cardiovascular, visceral, andocular complications [Shimizu et al.,2011; Kosho, 2016]. No specific guide-lines for management of patients withD4ST1/DSE-deficient EDS are avail-able. Guidelines for management ofmusculoskeletal problems, skin involve-ment, cardiovascular involvement, oph-thalmologic and dental follow-up, andpregnancy should follow those formu-lated for other forms of EDS (for

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 103
reference: See “management guidelinesfor the classical Ehlers–Danlos syn-drome,” by Bowen et al., this issue).
Specific management guidelinesmay include:
�
At diagnosis:– Screening for congenital heart defectsthrough a cardiac ultrasonography– Screening for ocular malformationsthrough an examination by a pediat-ric ophthalmologist
– Screening for malformations in therenal system through a renalultrasonography
– Screening for hearing impairment byan automated auditory brainstemresponse (aABR) as well as an
examination of a pediatric otologist�
Musculoskeletal:– Orthopedic intervention (e.g., serialplaster casts or surgery) for talipesequinovarus and physical therapy formotor developmental delay as thecenter of care for patients with thedisorder– After walking independently, specialattention to progressive foot defor-mities and trauma that could causeskin lacerations, joint dislocations, orlarge subcutaneous hematomas
– Assessment of spinal deformities
(scoliosis, kyphoscoliosis)�
Skin: Awrist-type sphygmomanometerfor patients with hyperalgesia topressure�
Ophtalmological: Regular check-upsfor strabismus, refractive errors,glaucoma�
ORL:Regular check-up forotitismediawith effusion, hearing impairment�
Urological: Regular check-up for uri-nation problems, bladder enlargement.Surgical fixation for cryptorchidism inmales�
Cardiovascular: Regular check-up forvalve abnormalities, aortic root dilation�
Gastro-intestinal: Regular check-up forconstipation and evaluation for need oflaxatives and/or enemas�
Assessment of secondary sex character-istics (breast development in femalesand gonadal function in males)�
Emergent treatment for pneumothoraxorpneumohemothorax, large subcutaneoushematomas, and diverticular perforationDifferential Diagnosis
�
Spndylodysplastic EDS � KyphoscolioticEDS (PLOD1,FKBP14) � Freeman–Sheldon syndrome � Loeys–Dietz syndromeMYOPATHIC EDS (mEDS)
Synonyms: EDS/Myopathy overlapsyndrome
The History of Myopathic EDS(mEDS)
The spectrum of diseases characterizedby muscle weakness, hypotonia, myop-athy, and connective tissue symptomswasfirst associated with mutations in thegenes that code for collagen type VI.These conditions have a wide spectrumof severity that ranges from the mostsevere Ullrich congenital muscular dys-trophy to the milder Bethlem myopathy.Zou et al. [2014] and Hicks et al.[2014] investigated groups of patientsthat had some symptoms of thesemyopathies but presented with a distinc-tive phenotype and did not have muta-tions affecting typeVI collagen.Throughthese studies they identified eight patientsin four families that presented withautosomal recessive (two patients, onefamily) and dominant (six patients, threefamilies) forms of EDS/myopathy. Sincethen, one additional patient has beendescribed [Punetha et al., 2016]. Preva-lence of this condition is unknown.
Mechanism of Disease
Collagen XII is synthesized as a homo-trimer made up of three a1 collagenchains coded by COL12A1. It is foundalong the surfaces of the fibers ofcollagen type I in tissues that expressthat collagen, and it is presumed to act asa bridge between the collagen I fibersand other extracellular componentsincluding decorin, fibromodulin, andTNX [Zou et al., 2014]. Deficiency ofthis collagen results in lax tissues due to amechanical problem with the ECM.Because collagen XII is expressed in the
muscle ECM, its absence results indisorganized patterning, abnormal forcetransmission, and other biomechanicalalterations resulting in myopathy. Itsabsence in skin and tendonswould explainthe overlapping EDS manifestations.
Allelic Heterogeneity
To date, nine patients from five familieswith myopathic EDS have been reported[Hicks et al., 2014; Zou et al., 2014;Punetha et al., 2016]. The mutationsinclude four heterozygous missense muta-tions that have an autosomal dominantmode of inheritance: c.7167 T>C, p.(Ile2334Thr), c.C5893T, p.(Arg1965Cys),8329G>C, p.(Gly2777Arg), and c.G8357A, p.(Gly2786Asp), and one ho-mozygous frameshift mutation, introduc-ing a PTC, associated with autosomalrecessive inheritance (c.8006þ1 G>A, p.(2567Asp>Phefs�2).
Clinical Description
At present, nine patients from fivefamilies have been reported (Table S1).Their age at publication ranged frombirth to 48 years (Table S1) [Hicks et al.,2014; Zou et al., 2014; Punetha et al.,2016]. The severity ranges from a severeautosomal recessive neonatal form thatwas described in two boys born to aconsanguineous couple, to a milderautosomal dominant form that presentsin childhood with muscle weakness,large joint contractures, and variabledegrees of joint hypermobility andhypertrophic scarring. The phenotypemay not be fully understood as there areso few reported cases.
The hallmark of the disorder ismuscle weakness that is present in infancyor childhood and is associated withproximal large joint contractures and distaljoint hypermobility. Characteristically,the muscle weakness tends to get betterwith age until young adulthood withsome deterioration in the 4th decade.
�
Reproductive, including pregnancyOne patient was born after a selectivecaesarian section because of oligohy-dramnios, intrauterine growth restric-tion, and breech presentation.
104 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
Craniofacial featuresOne patient displayed facial asymmetrywith skull flattening at birth, and milddysmorphic facial features, includingmicrognathia, high palate, short nose,big dysplastic ears. High arched palatewas reported in two other patients.�
MusculoskeletalCongenital proximal joint contracturesin combination with distal joint hyper-mobility were reported in three pa-tients. One patient was reported to haveproximal contractures at birth withoutmentioning of distal join hypermobility.At age 7 years, contractures haddisappeared but she had joint hypermo-bility in childhood. All patients tendedto have congenital kyphosis, in con-junction with torticollis in one, andsome developed scoliosis. The patientsreported by Hicks et al. [2014] (n¼ 5)developed long finger flexions (n¼ 4),rigid spine (n¼ 2), flexion contracturesof knee (n¼ 2), elbow (n¼ 1), andwrist (n¼ 1). Hip dislocation or sub-luxation was reported in two patients.One patient had a pectus excavatum.�
Skin and integumentReported skin features include hyper-trophic scars (n¼ 3), atrophic scars(n¼ 2), hyperkeratosis pilaris (n¼ 1).�
Neuromuscular features and motordevelopmentThe siblings reported by Zou et al.[2014] (homozygous mutation) had themost severe phenotype with profoundmuscle hypotonia at birth, poor feedingand swallowing, and night-time hypo-ventilation, with need for tube feedingand non-invasive night-time ventilation.They had a severe delay in motordevelopment, and they eventually wereable to reach a sitting position, but werenever able to stand or walk [Zou et al.,2014]. All other patients had congenitalmuscle hypotonia, with delayed grossmotor development, but symptomsseemed to improve over time. None ofthese patients remained non-ambulatory.Inone adult,muscle strengthwas reportedto deteriorate again in his late 30s.Reported abnormalities on musclebiopsy include myopathy with variabil-ity in fiber diameter, without overt sinsof degeneration or regeneration. In oneinstance, there was decreased laminin
B1. CK was elevated in several, but notall patients (of note: It was normal in thesiblings with the most severe, autosomalrecessive form).
Genotype–Phenotype Correlationand Penetrance
There appears to be a clear genotype–phenotype correlation. In general, fromthe fivemutations described so far it seemsthat missense mutations that affect criticalresidues in themolecule have a dominant-negative effect and result in variabledegrees of severity. There are no docu-mented instances of non-penetrance.There is significant variability, withinand between families, with individualscarrying the same mutation presentingwith different degrees of severity.
The one family with the autosomalrecessive condition harbors a homozy-gous loss of function mutation. Theaffected siblings have a more severe formof the condition. Reportedly carrierparents walked late (almost at 2 years ofage); therefore there appears to be a mildphenotype (dominant) in the carriersand a severe phenotype (recessive) in theindividuals that are homozygous [Zouet al., 2014].
Penetrance is unknown.
Management
There are no described treatments forthis group of disorders. Anticipatoryguidance should focus on preventingcomplications and improving the pre-senting symptoms. This may includephysical therapy for the contractures(since they tend to resolve over time),and monitoring for any signs of feedingor respiratory difficulties, in particularnocturnal hypoventilation. If the latter ispresent, then assisted non-interventionalventilation at night may be indicated.
Differential Diagnosis
�
Bethlem and Ullrich myopathies (Col-lagen type VI-related disorders)�
Kyphoscoliotic EDS � Hypermobile EDS�
Classical EDS � Classical-like EDSPERIODONTAL EDS (pEDS)
Synonyms: EDS type VIII, Ehlers–Danlos Syndrome periodontitis type,Ehlers–Danlos Syndrome periodontosistype.
The History of Periodontal EDS
McKusick [1972] described a “uniquecondition” in a patient with EDS-likefeatures, that is, lesions on the shins, slow-healing breaks in the skin, atrophic scars,and absorptive periodontitis with earlyloss of the teeth. Five years later, Stewartet al. [1977] published a similar case andclassified this new variant as EDS VIII.Since then, pEDS has been reported in32 case reports and seven pedigreeanalyses. Extensive periodontal destruc-tion with early onset is a core finding ofperiodontal EDS, mostly in combinationwith striking pre-tibial plaques and tissuefragility. There is greater variability inother clinical features.
In the past, the delineation of pEDSas a specific phenotype was hampered bythe relatively high prevalence of chronicperiodontitis, with an estimated rangefrom 19 to 83% depending on age andseverity [Demmer et al., 2010]. There-fore, periodontal disease in vascular andother EDS types could be a coincidenceof two unrelated diseases. These histori-cal overlaps between pEDS and otherEDS subtypes have confused the phe-notype. While the majority of pEDSpatients had vEDS excluded throughcollagen protein analysis, this does notcompletely exclude a COL3A1 variantbeing causative in some of the oldercases.
Also, joint hypermobility is a com-mon feature in the general population,which complicates accurately ascertain-ing co-segregation of these two traits.The Villefranche EDS nosology groupnoted these difficulties in distinguishingthis rare disorder from other hereditarydisorders of connective tissue [Beightonet al., 1998]. In 2003, pEDSwas mappedto a 7 cM (5.8MB) interval on

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 105
chromosome 12p13 in three families[Rahman et al., 2003], but no candidategene was identified. In 2016, an interna-tional consortium published 19 indepen-dent families comprising 107 individualswith pEDS to identify the genetic locus[Kapferer-Seebacher et al., 2016]. In-cluded were samples of eight previouscase reports and pedigree studies [Stewartet al., 1977, Hartsfield and Kousseff,1990, Rahman et al., 2003, Reinsteinet al., 2011, Reinstein et al., 2012,Reinstein et al., 2013, Cıkla et al.,2014, George et al., 2016]. In 17 ofthese families, heterozygous missense orin-frame insertion/deletionmutations inC1R (15 families) or C1S (two families)were identified. C1R and C1S arecontiguous genes in the previouslyreported linkage region on chromosome12p13, and encode subunits C1r andC1sof the first component of the classicalcomplement pathway.
The prevalence of pEDS is unknown.
Figure 8. (A) Gingival tissues of a child affected with pEDS. The keratinizedgingiva is missing; the oral mucosa extends to the free gingival margin and the interdentalpapillae and is very fragile. (B) Gingival tissues of a non-affected child. The gingiva iskeratinized and is tightly bound to the underlying periostum via collagen structures, andperforms a protective function during mastication. The border between gingiva andalveolar mucosa is the mucogingival junction (dotted line). The oral mucosa is non-keratinized and only loosely connected to the periostum; therefore, it is more fragile. (C)Dental radiograph of an affacted individual, at aged 29. Notice severe periodontal boneloss (asteriks). (D) Clinical picture of the same individual, at age 30. Premolars in the leftmandible have been lost in the meantime without periodontal pocketing and despitegood oral hygiene. Notice the lack of keratinized gingiva and gingival recessions(receeding gums) (Images kindly provided by Dr. Ines Kapferer-Seebacher, withpermission).
The Mechanisms of Disease
Complement is a major element ofantimicrobial host defense through itsability to recognize pathogens and limitinfection in the early phase after expo-sure to microorganisms. The classicalpathway of complement is triggered byC1, a complex comprising a recognitionsubunit C1q and two modular serineproteases (SPs) C1r and C1s [Budayova-Spano et al., 2002]. C1r and C1s areassembled into a Ca(2þ)-dependentC1s─C1r─C1r─C1s tetramer whichassociates with the recognition proteinC1q [Gaboriaud et al., 2014;Rossi et al.,2014]. After C1 binding to immunecomplexes, C1r auto-activates and thencleaves C1s which in turn cleaves C4(into C4a and C4b) and C2 (into C2aand C2b) to form the classical pathwayC3 convertase (C4b2a) [Patrick et al.,1970; Thielens et al., 1982; Amanoet al., 2008].
One attractive hypothesis for thepathomechanism of pEDS is alteredbinding of the C1r─C1s tetramer orprematurely cleaved fragments to C1qor soluble procollagens. This couldaffect C1 function or interfere withprocollagen processing within the ER.
Moderate enlargement of the ERcisterns documented in vitro in dermalfibroblasts may reflect retention ofmalprocessed molecules but could alsoreflect boosted expression/productionof collagen as a feed-back response todecreased deposition of mature collageninto the matrix. The exact pathome-chanism of pEDS remains to be clarified.
Allelic Heterogeneity
Heterozygous missense or in-frameinsertion/deletion variants in C1Rwere detected in 15 families (comprising76 affected individuals), and heterozy-gous missense or in-frame insertion/deletion variants in C1S were detectedin two families (comprising 16 affectedindividuals). These variants involve theC1r/C1s, C1r/C1r, or C1r/C1q inter-faces or the hinges between interactionand catalytic domains of C1r and C1s.Variants never involved the catalyticdomain of C1r or C1s [Kapferer-Seebacher et al., 2016].
Clinical Description
In the review on clinical features, wedistinguished between individuals withconfirmed mutations in C1R or C1Sand other case reports. See Table S1 forthe prevalence of clinical features in themolecularly confirmed patients (Repre-sentative pictures of the phenotype aregiven in Fig. 8).
�
Craniofacial featuresStewart et al. [1977] included a photo-graph of the reported patient with an“aesthenic build.” Dysmorphic facialfeatures were not described by Rahmanet al. [2003]. In the dysmorphologyliterature, Cunniff and Williamson-Kruse [1995] described a triangularface, prominent eyes, long nose, andshort philtrum. Biesecker described apaucity of subcutaneous fat with prom-inent nose and larynx [Biesecker et al.,1991]. Hartsfield noted the phenotypicoverlap with vEDS [Hartsfield andKousseff, 1990].
106 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
�
Musculoskeletal systemIn 93 individuals with C1R or C1Smutations reported by Kapferer-See-bacher et al. [2016] joint hypermobilitywas reported in 56% of patients, mostlyaffecting the fingers (30%), the elbows(19%), knees (11%), hips, wrist, andankle (3%). Marfanoid habitus, scolio-sis, osteoarthritis, flat feet, and herniawere not consistent features [Kapferer-Seebacher et al., 2016].�
Skin and integumentPretibial plaques with or withouthaemosiderosis are a consistent featurein most reports. Clinically, the lesionsresemble necrobiosis lipoidica, butgenerally differ histologically. Fibrosisand haemosiderin deposits were re-ported, as opposed to interstitial andpalisade granulomas and/or microangi-opathy 19. Buckel and Zaenglein[2007] confirmed similar findings.Easy bruising, skin fragility, and (mild)hyperelasticity of the skin have beenreported in the majority of cases. Thereis a single report of an associatedvasculitis in the absence of pretibiallesions [Hoffman et al., 1991]. In 93individuals withC1R orC1Smutationsreported by Kapferer-Seebacher et al.[2016], consistent cutaneous findingswere pretibial discolorations (83%),easy bruising (96%), skin fragility(83%), and (mild) hyperelasticity ofthe skin (73%). Atrophic scars werepresent in 50% of cases [Kapferer-Seebacher et al., 2016].�
Cardiovascular involvementUntil recent, pEDS has not beenassociated with catastrophic vascularcomplications or hollow visceral rup-ture that arise in vEDS. It is of note thatthe father of the case reported byStewart et al. [1977] had duodenalrupture and subsequent collagen pro-tein analysis showed a normal collagen(I:III) ratio. Recently, a 42-year-oldwoman was reported with pEDS and aruptured “blood blister” shaped aneu-rysm of her left middle cerebral artery[Cıkla et al., 2014].Kapferer-Seebacher et al. [2016]reported a prevalence of 16% forvascular complications (cerebral aneur-isms or aortic dissection), and oneindividual with three events of organrupture (once duodenum, twice lung).As pEDS patients are not routinelychecked for aneurisms, there might bealso unrecorded cases. Additionally,many of the reports describe pediatricpatients and there is a great need forlongterm follow-up.
�
Dental involvementEarly-onset periodontitis with exten-sive periodontal destruction and loss ofteeth, starting in childhood or adoles-cence, is one of the defining hallmarksof pEDS, and was present in all reportedcases and in 99% of individuals withconfirmed C1R/C1S mutations. Aclear demarcation to the diagnosis ofchronic or aggressive periodontitis isessential. Typically, periodontal de-struction in pEDS is not accompaniedby periodontal pocket formation but byreceding gums (personal observationIK). Prior to periodontitis, affectedindividuals may present with extensivegingival inflammation in response tomild dental plaque accumulation. Acharacteristic recently described featureis a striking lack of attached gingivacausing oral tissue fragility (Fig. 1)[Kapferer-Seebacher et al., 2016].�
Additional laboratory findings– Biochemistry:Biochemical analysis of collagen incultured skin fibroblasts did not showabnormalities in the production andsecretion of type I, III, andV collagensin several case reports and also in eightindividuals with confirmed mutationsin C1S/C1R [Biesecker et al., 1991;Cunniff andWilliamson-Kruse, 1995;Kapferer-Seebacher et al., 2016]. Incontrast, Mataix et al. [2008] reporteda reduced rate of collagen (I) andcollagen (III) synthesis compared tocontrol samples. Lapiere and Nusgens[1981] initially reported a family withpEDS and reduced collagen III pro-tein from skin, but later reported that arepeat analysis had not been able toreplicate this.– Skin histology and ultrastructure:It is of note that there is variation incollagen ultrastructure depending onthe site of biopsy in the generalpopulation (Pope and Vandersteen,personal observations). Many pa-tients with pEDS in the literature
had biopsy from pre-tibial lesions,others at the standard site. Therewereno consistent findings, but evidenceof collagen fibril size, packing, mor-phology, and ER dilatation are allreported.Electron microscopy examination ofskin reported in seven individualswith C1R/C1S mutations showeddecreased collagen content, abnor-mal variation in collagen fibrildiameter and some abnormallyshaped fibrils [Rahman et al.,2003; Reinstein et al., 2012, 2013;Kapferer-Seebacher et al., 2016],which is in line with further reports[Kobayasi, 2004; Mataix et al.,2008]. Dermal collagen fibersshowed some variability in thedensity of the packing and afew areas of kinking. The sizeuniformity does not supportvEDS, while the kinking is non-specific. Additionally, patients’fibroblasts showed an increasedproportion of dilated rough ER(RER) cisternae [Reinstein et al.,2012; Kapferer-Seebacher et al.,2016].Dyne et al. [1993] reported collagendepletion and a larger number ofsmall elastin fibrils; ultrastructureshowed occasional serrated collagenfibrils, with normal fibril diameter.
– Immunology:Hoffman et al. [1991] reported apatient with severe periodontitis,valvular heart disease, osteocondylarand phalangeal osteolysis in theabsence of pretibial hyperpigmenta-tion. This patient had intractablevasculitis and had a T cell responseto type I collagen. Other patientshave not had evidence of vasculitis.The case has some similarities topatients described with SingletonMerton syndrome, (premature dentalloss, aortic calcification, and osteo-porosis, OMIM 182250). It is doubt-ful whether this patient had truepEDS.
Kapferer-Seebacher et al. [2016]reported a prevalence of 40% forrecurrent infections like otitis media,herpes zoster, bladder infections,empyema, kidney infections, or

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 107
pneumonia. There were single pa-tients with autoimmunologic disor-ders like Sj€ogren syndrome, rosacea,and Crohn’s disease [Kapferer-Seebacher et al., 2016].
Management
There is no curative treatment for thisdisorder. A recent review of the dentalmanagement of EDS recommendedspecial care regarding mucosal fragil-ity, bleeding, temporomandibularjoint hypermobility, and local anaes-thetic resistance [Tulika and Kiran,2015]. Management of periodontaldisease requires lifelong biofilm man-agement including intense oral hy-giene instructions and nonsurgicaldebridement about every 3 months.Systemic antibiotics may be indicated.Conservative surgical management isrecommended because of difficultieswith fragile periosteal skin flaps andsuture tears.
Differential Diagnosis
�
Vascular EDS � Classical EDS � Hypermobile EDS � Periodontal diseasesPeriodontal diseases range frommild and reversible gingivitis to irre-versible loss of periodontal attachmentresulting in tooth loss. “(Plaque-in-duced) gingivitis” is an inflammationsolely of the gums in response tobacterial biofilms, and is characterizedby bleeding on probing. “Periodontitis”is characterized by inflammation of thegingiva and destruction of the peri-odontal tissues, which are the gingiva,the cementum, the periodontal liga-ment, and the alveolar bone. Periodon-tal bone loss is diagnosed radiologicallyor clinically with a periodontal probe.“Gingival recession” (receding gums) ingeneral is the exposure of the toothroots. It might be an accompanyingfeature of periodontitis, and in thiscase the tooth root is exposed also
interdentally. Gingival recession mightalso present only on the buccal orlingual aspects of the tooth. In thiscase, it can, for example, be associatedwith a thin gingival biotype andintencse tooth brushing, but notwith periodontitis.
“Chronic periodontitis” prevalenceestimates ranged from 19 to 83%depending on age and severity[Demmer et al., 2010]. Severe peri-odontitis with a mean prevalence of11.2% is the sixth-most prevalent con-dition in the world [Kassebaum et al.,2014]. The typical patient is over30 years of age, and the amount ofbone destruction is consistent withthe presence of plaque and calculus[Armitage, 2004]. In general, thedisease progresses slowly but theremay be bursts of destruction. Inaddition, the rate of disease progressioncan be modified by local factors,systemic diseases, and extrinsicfactors such as smoking or emotionalstress.
“Aggressive periodontitis” preva-lence estimates range from 0.1% inCaucasians residing in north and midEurope to 5% in African populations[Albandar, 2014]. The primaryfeatures are rapid attachment loss inotherwise healthy individuals andfamilial aggregation, usually affectingpersons under 30 years of age [Alban-dar, 2014]. Some types of aggressiveperiodontitis seem to be inheritedin a Mendelian manner, and bothautosomal modes and X-linkedtransmission have been proposed[Meng et al., 2011]. However, reviewof pedigree analysis, linkage andlinkage disequilibrium studies have sofar been inconclusive [Meng et al.,2011].
There are several “monogenic syn-dromes with significant periodontitis” aspart of the clinical phenotype. Themajority of syndromes with severeperiodontal destruction in childhoodare inherited as autosomal recessive orX-linked traits and are associated withneutrophil dysfunction, for example,congenital and cyclic neutropenia(OMIM 202700), Chediak–Higashisyndrome (OMIM 214500), leukocyte
adhesion deficiencies types I, II, and III(OMIM 116920; OMIM 266265;OMIM 612840), WHIM (OMIM193670), Cohen Syndrome (OMIM216550), and agranulocytosis (OMIM610738).
Conditions with more complexdermatological phenotypes includeKindler syndrome (hereditary acroker-atotic poikiloderma OMIM 173650),Papillon–Lefevre syndrome and cathep-sin C associated phenotypes (�602635),hypotrichosis osteolysis periodontitis(OMIM 607658). Multiple loci associ-ated with an aggressive periodontitishave been reported (OMIM 170650)[Hart and Atkinson, 2007]. TheSingleton–Merten syndrome (OMIM182250) with periodontal destructionand aortic calcification has recently beenshown to result from dominant muta-tions in the IF1H1 gene [Rutsch et al.,2015].
Hypophosphatasia (OMIM146300) is a highly variable autosomaldominant disorder associated withenamel hypoplasia, early loss of primarydentition, bowed long bones, andosteopenia. Odontohypophosphatasiais the least severe form of hypophos-phatasia, characterized by prematureexfoliation of primary and/or perma-nent teeth in the absence of skeletalsystem abnormalities. It is associatedwith a low circulating alkalinephosphatase.
FUTURE RESEARCH ANDGAPS
During the last decade, there has beenan explosion of diverse but overlap-ping novel EDS or EDS-like pheno-types for which molecular defects havebeen identified in an array of newgenes, as illustrated above. The geno-mic era promises to shed additionallight on unsolved forms of Ehlers–Danlos syndrome. However, while ourknowledge of the molecular basis ofEDS has greatly progressed since theVillefranche Nosology, our under-standing of the pathophysiologicalmechanisms underlying these condi-tions remains very limited, and eluci-dation of the genetic basis has not

108 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
translated to improved clinical man-agement strategies.
However, while ourknowledge of the molecularbasis of EDS has greatly
progressed since theVillefranche Nosology, our
understanding of thepathophysiological
mechanisms underlying theseconditions remains very
limited, and elucidation of thegenetic basis has not
translated to improved clinicalmanagement strategies.
Future research could focus ondifferent aspects, including:
�
Natural history studies � Quality of life studies � The creation of an international patientregister, with prospective collection ofdetailed information regarding geno-type and phenotype. This informationshould, among others, help addressquestions regarding:– genotype–phenotype correlations– prevalence– clinical variability (inter- andintrafamilial)– age-dependent organ-system in-volvement outcomes
– risk related to pregnancy and delivery
�
Development of surveillance, and man-agement and care guidelines, includingpain management�
Collection of tissue samples for thestudy of the pathogenetic basis of disease�
Development of animal models forstudy of pathogenetic mechanisms andfor preclinical studies�
Identification of biomarkers to followevolution of disease�
With the advent of next-generationsequencing techniques, many variantsof unknown significance are being iden-tified. As such there is a need for thedevelopment of functional tests to studythe pathogenic nature of these variants
�
Identification of therapeutic targetsACKNOWLEDGEMENTS
We are very grateful for the cooperationof many patients and their families allover the world. We also wish toacknowledge the invaluable discussionswith many professionals and lay persons.We would like to thank our generoussponsors including, but not limited to,The Ehlers–Danlos National Founda-tion, the Ehlers–Danlos Support UK,and the Ehlers–Danlos Society. Fran-siska Malfait is Senior Clinical Investi-gator at the Fund for Scientific ResearchFlanders.
REFERENCES
Abdalla EM, Rohrbach M, Burer C, Kraenzlin M,El-Tayeby H, Elbelbesy MF, Nabil A, GiuntaC. 2015.Kyphoscoliotic typeof Ehlers–Danlossyndrome (EDS VIA) in six Egyptian patientspresenting with a homogeneous clinicalphenotype. Eur J Pediatr 174:105–112.
Abu A, Frydman M, Marek D, Pras E, Nir U,Reznik-Wolf H, Pras E. 2008. Deleteriousmutations in the Zinc-Finger 469 gene causebrittle cornea syndrome. Am J Hum Genet82:1217–1222.
Al-Gazali LI, Bakalinova D, Varady E, Scorer J,Nork M. 1997. Further delineation of Nevosyndrome. J Med Genet 34:366–370.
Al-Hussain H, Zeisberger SM, Huber PR, GiuntaC, Steinmann B. 2004. Brittle corneasyndrome and its delineation from thekyphoscoliotic type of Ehlers–Danlos syn-drome (EDS VI): Report on 23 patients andreview of the literature. Am J Med GenetPart A 124A:28–34.
Al-Owain M, Al-Dosari MS, Sunker A, Shuaib T,Alkuraya FS. 2012. Identification of anovel ZNF469 mutation in a large familywith Ehlers–Danlos phenotype. Gene511:447–450.
Alazami AM, Al-Qattan SM, Faqeih E, AlhashemA, Alshammari M, Alzahrani F, Al-DosariMS, Patel N, Alsagheir A, Binabbas B,Alzaidan H, Alsiddiky A, Alharbi N,Alfadhel M, Kentab A, Daza RM, KircherM, Shendure J, Hashem M, Alshahrani S,Rahbeeni Z, Khalifa O, Shaheen R,Alkuraya FS. 2016. Expanding the clinicaland genetic heterogeneity of hereditarydisorders of connective tissue. Hum Genet135:525–540.
Albandar JM. 2014. Aggressive periodontitis: Casedefinition and diagnostic criteria. Periodon-tol 2000 65:13–26.
AldahmeshMA,Mohamed JY, Alkuraya FS. 2012.A novel mutation in PRDM5 in brittlecornea syndrome. Clin Genet 81:198–199.
Aldeeri AA, Alazami AM, Hijazi H, Alzahrani F,Alkuraya FS. 2014. Excessively redundantumbilical skin as a potential early clinicalfeature of Morquio syndrome and FKBP14-related Ehlers–Danlos syndrome. ClinGenet 86:469–472.
Amano MT, Ferriani VP, Florido MP, Reis ES,Delcolli MI, Azzolini AE, Assis-PandochiAI, Sj€oholm AG, Farah CS, Jensenius JC,Isaac L. 2008. Genetic analysis of comple-ment C1s deficiency associated with sys-temic lupus erythematosus highlightsalternative splicing of normal C1s gene.Mol Immunol 45:1693–1702.
Armitage GC. 2004. Periodontal diagnoses andclassification of periodontal diseases. Perio-dontol 2000 34:9–21.
Arunrut T, Sabbadini M, Jain M, Machol K,Scaglia F, Slavotinek A. 2016. Cornealclouding, cataract, and colobomas with anovel missense mutation in B4GALT7—Areview of eye anomalies in the linkeropathysyndromes. Am J Med Genet Part A170A:2711–2718.
Avgitidou G, Siebelmann S, Bachmann B,Kohlhase J, Heindl LM, Cursiefen C.2015a. Brittle cornea syndrome: Case reportwith novel mutation in the PRDM5 geneand review of the literature. Case RepOphthalmol Med 2015:5.
Avgitidou G, Siebelmann S, Bachmann B,Kohlhase J, Heindl LM, Cursiefen C.2015b. Brittle cornea syndrome: Case reportwith novel mutation in the PRDM5 geneand review of the literature. Case RepOphthalmol Med 2015:637084.
Bar-Yosef O, Polak-Charcon S, Hoffman C,Feldman ZP, Frydman M, Kuint J. 2008.Multiple congenital skull fractures as apresentation of Ehlers–Danlos syndrometype VIIC. Am J Med Genet Part A146A:3054–3057.
Baumann M, Giunta C, Krabichler B, Ruschen-dorf F, Zoppi N, Colombi M, Bittner RE,Quijano-Roy S, Muntoni F, Cirak S,Schreiber G, Zou Y, Hu Y, Romero NB,Carlier RY, Amberger A, Deutschmann A,Straub V, Rohrbach M, Steinmann B,Rostasy K, Karall D, Bonnemann CG,Zschocke J, Fauth C. 2012. Mutations inFKBP14 cause a variant of Ehlers–Danlossyndrome with progressive kyphoscoliosis,myopathy, and hearing loss. Am J HumGenet 90:201–216.
Beighton P. 1970a. Ehlers–Danlos syndrome. AnnRheum Dis 29:332–333.
Beighton P. 1970b. Serious ophthalmologicalcomplications in the Ehlers–Danlos syn-drome. Br J Ophthalmol 54:263–268.
Beighton P, De Paepe A, Steinmann B, TsipourasP, Wenstrup RJ. 1998. Ehlers–Danlos syn-dromes: Revised nosology, Villefranche,1997. Ehlers–Danlos National Foundation(USA) and Ehlers–Danlos Support Group(UK). Am J Med Genet 77:31–37.
Besselink-Lobanova A, Maandag NJ, Voer-mans NC, van der Heijden HF, van derHoeven JG, Heunks LM. 2010. Trachearupture in tenascin-X-deficient typeEhlers–Danlos syndrome. Anesthesiology113:746–749.

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 109
Biesecker LG, Erickson RP, Glover TW, BonadioJ. 1991. Molecular and cytologic studies ofEhlers–Danlos syndrome type VIII. Am JMed Genet 41:284–288.
Bin BH, Fukada T, Hosaka T, Yamasaki S, OhashiW, Hojyo S, Miyai T, Nishida K, YokoyamaS, Hirano T. 2011. Biochemical characteri-zation of human ZIP13 protein: A homo-dimerized zinc transporter involved in thespondylocheiro dysplastic Ehlers–Danlossyndrome. J Biol Chem 286:40255–40265.
Bin BH, Hojyo S, Hosaka T, Bhin J, Kano H,Miyai T, Ikeda M, Kimura-Someya T,Shirouzu M, Cho EG, Fukue K, KambeT, Ohashi W, Kim KH, Seo J, Choi DH,Nam YJ, Hwang D, Fukunaka A, Fujitani Y,Yokoyama S, Superti-Furga A, Ikegawa S,Lee TR, Fukada T. 2014a. Molecularpathogenesis of spondylocheirodysplasticEhlers–Danlos syndrome caused by mutantZIP13 proteins. EMBO Mol Med6:1028–1042.
Bin BH, Hojyo S, Ryong Lee T, Fukada T. 2014b.Spondylocheirodysplastic Ehlers–Danlossyndrome (SCD-EDS) and the mutantzinc transporter ZIP13. RareDis 2:e974982.
Brinckmann J, Acil Y, Feshchenko S, Katzer E,Brenner R, Kulozik A, Kugler S. 1998.Ehlers–Danlos syndrome type VI: Lysylhydroxylase deficiency due to a novel pointmutation (W612C). Arch Dermatol Res290:181–186.
Brunk I, Stover B, Ikonomidou C, Brinckmann J,Neumann LM. 2004. Ehlers–Danlos syn-drome type VI with cystic malformations ofthe meninges in a 7-year-old girl. Eur JPediatr 163:214–217.
Buckel T, Zaenglein AL. 2007. What syndrome isthis? Ehlers–Danlos syndrome type VIII.Pediatr Dermatol 24:189–191.
Budayova-Spano M, Lacroix M, Thielens NM,Arlaud GJ, Fontecilla-Camps JC, GaboriaudC. 2002. The crystal structure of thezymogen catalytic domain of complementprotease C1r reveals that a disruptivemechanical stress is required to triggeractivation of the C1 complex. EMBO J21:231–239.
Bui C, Talhaoui I, Chabel M, Mulliert G,Coughtrie MW, Ouzzine M, Fournel-Gigleux S. 2010. Molecular characterizationof b1,4-galactosyltransferase 7 genetic mu-tations linked to the progeroid form ofEhlers–Danlos syndrome (EDS). FEBS Lett584:3962–3968.
Burch GH, Gong Y, Liu W, Dettman RW, CurryCJ, Smith L, Miller WL, Bristow J. 1997.Tenascin-X deficiency is associated withEhlers–Danlos syndrome. Nature Genet17:104–108.
Burkitt Wright EM, Porter LF, Spencer HL,Clayton-Smith J, Au L, Munier FL, Smith-son S, Suri M, Rohrbach M, Manson FD,Black GC. 2013. Brittle cornea syndrome:Recognition, molecular diagnosis and man-agement. Orphanet J Rare Dis 8:6.
Burkitt Wright EM, Spencer HL, Daly SB,Manson FD, Zeef LA, Urquhart J, ZoppiN, Bonshek R, Tosounidis I, Mohan M,Madden C, Dodds A, Chandler KE, BankaS, Au L, Clayton-Smith J, Khan N,Biesecker LG, Wilson M, Rohrbach M,Colombi M, Giunta C, Black GC. 2011.Mutations in PRDM5 in brittle cornea
syndrome identify a pathway regulatingextracellular matrix development and main-tenance. Am J Hum Genet 88:767–777.
Busch A, Suellner J, Anger F, Meir M, Kickuth R,LorenzU,WildenauerR. 2014. Critical careof kyphoscoliotic type Ehlers–Danlos syn-drome with recurrent vascular emergencies.Vasa 43:216–221.
Byers PH, Duvic M, Atkinson M, Robinow M,Smith LT, Krane SM, Greally MT, LudmanM, Matalon R, Pauker S, Quanbeck D,Schwarze U. 1997. Ehlers–Danlos syndrometype VIIA and VIIB result from splice-junction mutations or genomic deletionsthat involve exon 6 in the COL1A1 andCOL1A2 genes of type I collagen. Am JMed Genet 72:94–105.
Cabral WA, Makareeva E, Letocha AD, ScribanuN, Fertala A, Steplewski A, Keene DR,Persikov AV, Leikin S, Marini JC. 2007. Y-position cysteine substitution in type Icollagen (alpha1(I) R888C/p.R1066C) isassociated with osteogenesis imperfecta/Ehlers–Danlos syndrome phenotype. HumMutat 28:396–405.
Cameron JA. 1993. Corneal abnormalities inEhlers–Danlos syndrome type VI. Cornea12:54–59.
Carr AJ, Chiodo AA, Hilton JM, Chow CW,Hockey A, Cole WG. 1994. The clinicalfeatures of Ehlers–Danlos syndrome typeVIIB resulting from a base substitution at thesplice acceptor site of intron 5 of theCOL1A2 gene. J Med Genet 31:306–311.
Cartault F, Munier P, Jacquemont ML, Vellayou-dom J, Doray B, Payet C, Randrianaivo H,Laville JM, Munnich A, Cormier-Daire V.2015. Expanding the clinical spectrum ofB4GALT7 deficiency: Homozygous p.R270C mutation with founder effect causesLarsen of Reunion Island syndrome. Eur JHum Genet 23:49–53.
Chamson A, Berbis P, Fabre JF, Privat Y, Frey J.1987. Collagen biosynthesis and isomor-phism in a case of Ehlers–Danlos syn-drome type VI. Arch Dermatol Res 279:303–307.
Cheng HY, Chen XW, Cheng L, Liu YD, Lou G.2010. DNA methylation and carcinogenesisof PRDM5 in cervical cancer. J Cancer ResClin Oncol 136:1821–1825.
Chiodo AA, Hockey A, Cole WG. 1992. A basesubstitution at the splice acceptor site ofintron 5 of the COL1A2 gene activates acryptic splice site within exon 6 andgenerates abnormal type I procollagen in apatient with Ehlers–Danlos syndrome typeVII. J Biol Chem 267:6361–6369.
Christensen AE, Knappskog PM, Midtbø M,Gjesdal CG, Mengel-From J, Morling N,Rødahl E, Boman HI. 2010. Brittle corneasyndrome associated with a missense muta-tion in the zinc-finger 469 gene. InvestOphthalmol Vis Sci 51:47–52.
Cıkla U, Sadighi A, Bauer A, BaSskaya MK. 2014.Fatal ruptured blood blister-like aneurysm ofmiddle cerebral artery associated withEhlers–Danlos syndrome type VIII (peri-odontitis type). J Neurol Surg Rep 75:e210–e213.
Cole WG, Chan D, Chambers GW, Walker ID,Bateman JF. 1986. Deletion of 24amino acids from the pro-alpha 1(I) chainof type I procollagen in a patient with the
Ehlers–Danlos syndrome type VII. J BiolChem 261:5496–5503.
Cole WG, Evans R, Sillence DO. 1987. Theclinical features of Ehlers–Danlos syndrometype VII due to a deletion of 24 amino acidsfrom the pro alpha 1(I) chain of type Iprocollagen. J Med Genet 24:698–701.
Colige A, Nuytinck L, Hausser I, van Essen AJ,Thiry M, Herens C, Ades LC, Malfait F,Paepe AD, Franck P, Wolff G, OosterwijkJC, Smitt JH, Lapiere CM, Nusgens BV.2004. Novel types of mutation responsiblefor the dermatosparactic type of Ehlers–Danlos syndrome (Type VIIC) and commonpolymorphisms in the ADAMTS2 gene.J Invest Dermatol 123:656–663.
Colige A, Ruggiero F, Vandenberghe I, Dubail J,Kesteloot F, Van Beeumen J, Beschin A, BrysL, Lapiere CM, Nusgens B. 2005. Domainsand maturation processes that regulate theactivity of ADAMTS-2, a metalloproteinasecleaving the aminopropeptide of fibrillarprocollagens types I–III and V. J Biol Chem280:34397–34408.
Colige A, Sieron AL, Li SW, Schwarze U, PettyEM,WerteleckiW,WilcoxWR, KrakowD,Cohn DH, Reardon W, Byers PH, Lapi�ereCM, Prockop DJ, Nusgens BV. 1999.Human Ehlers–Danlos syndrome type VIIC and bovine dermatosparaxis are caused bymutations in the procollagen I N-proteinasegene. Am J Hum Genet 65:308–317.
Colige A, Vandenberghe I, ThiryM, Lambert CA,Van Beeumen J, Li SW, Prockop DJ, LapiereCM, Nusgens BV. 2002. Cloning andcharacterization of ADAMTS-14, a novelADAMTS displaying high homology withADAMTS-2 and ADAMTS-3. J Biol Chem277:5756–5766.
Counts DF, Byers PH, Holbrook KA, HegrebergGA. 1980. Dermatosparaxis in a Himalayancat: I. Biochemical studies of dermal colla-gen. J Invest Dermatol 74:96–99.
Cunniff C, Williamson-Kruse L. 1995. Ehlers–Danlos syndrome, type VIII presenting withperiodontitis and prolonged bleeding time.Clin Dysmorphol 4:145–149.
D’Alessio M, Ramirez F, Blumberg B, Wirtz M,Rao V, Godfrey M, Hollister D. 1991.Characterization of a COL1A1 splicingdefect in a case of Ehlers-Danlos syndrometype VII: Further evidence of molecularhomogeneity. Am J Hum Genet49:400–406.
Dalgleish R. 1998. The human collagen mutationdatabase 1998. Nucleic Acids Res26:253–255.
De Coster PJ, Malfait F, Martens LC, De Paepe A.2003. Unusual oral findings in dermatospar-axis (Ehlers–Danlos syndrome type VIIC).J Oral Pathol Med 32:568–570.
Dembure PP, Priest JH, Snoddy SC, Elsas LJ.1984. Genotyping and prenatal assessment ofcollagen lysyl hydroxylase deficiency in afamily with Ehlers–Danlos syndrome typeVI. Am J Hum Genet 36:783–790.
Demirdas S, Dulfer E, Robert L, Kempers M, vanBeek D, Micha D, van Engelen BG, HamelB, Schalkwijk J, Loeys B, Maugeri A,Voermans NC. 2016. Recognizing thetenascin-X deficient type of Ehlers–Danlossyndrome: A cross-sectional study in 17patients. Clin Genet. doi: 10.1111/cge.12853 [Epub ahead of print].

110 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
Demmer RT, Papapanou PN, Jacobs DR, Jr.,Desvarieux M. 2010. Evaluating clinicalperiodontal measures as surrogates forbacterial exposure: The oral infections andvascular disease epidemiology study (IN-VEST). BMC Med Res Methodol 10:2.
Dordoni C, Ciaccio C, Venturini M, Calzavara-Pinton P, Ritelli M, Colombi M. 2016.Further delineation of FKBP14-relatedEhlers–Danlos syndrome: A patient withearly vascular complications and non-pro-gressive kyphoscoliosis, and literature re-view. Am J Med Genet Part A170A:2031–2038.
D€undar M, Demiryilmaz F, Demiryilmaz I,Kumandas S, Erkilic K, Kendirch M, TuncelM, Ozyazgan I, Tolmie JL. 1997. Anautosomal recessive adducted thumb-clubfoot syndrome observed in Turkish cousins.Clin Genet 51:61–64.
D€undar M, Kurtoglu S, Elmas B, Demiryilmaz F,Candemir Z, Ozkul Y, Durak AC. 2001.A case with adducted thumb and club footsyndrome. Clin Dysmorphol 10:291–293.
D€undar M, M€uller T, Zhang Q, Pan J, SteinmannB, Vodopiutz J, Gruber R, Sonoda T,Krabichler B, Utermann G, Baenziger JU,Zhang L, Janecke AR. 2009. Loss ofdermatan-4-sulfotransferase 1 function re-sults in adducted thumb-clubfoot syndrome.Am J Hum Genet 85:873–882.
Duan Z, PersonRE, LeeHH,Huang S, DonadieuJ, Badolato R, Grimes HL, Papayannopou-lou T, Horwitz MS. 2007. Epigeneticregulation of protein-coding and micro-RNA genes by the Gfi1-interacting tumorsuppressor PRDM5. Mol Cell Biol27:6889–6902.
Dyne KM, Vitellaro-Zuccarello L, Bacchella L,Lanzi G, Cetta G. 1993. Ehlers–Danlossyndrome type VIII: Biochemical, stereo-logical, and immunocytochemical studies ondermis from a child with clinical signs ofEhlers–Danlos syndrome and a familyhistory of premature loss of permanentteeth. Br J Dermatol 128:458–463.
Egging DF, van Vlijmen-Willems I, Choi J,Peeters AC, van Rens D, Veit G, Koch M,Davis EC, Schalkwijk J. 2008. Analysis ofobstetric complications and uterine connec-tive tissue in tenascin-X-deficient humansand mice. Cell Tissue Res 332:523–532.
Eide DJ. 2006. Zinc transporters and the cellulartrafficking of zinc. Biochim Biophys Acta1763:711–722.
Esaka EJ, Golde SH, Stever MR, Thomas RL.2009. A maternal and perinatal mortality inpregnancy complicated by the kyphoscoli-otic form of Ehlers–Danlos syndrome.Obstet Gynecol 113:515–518.
Evers MR, Xia G, Kang HG, Schachner M,Baeziger JU. 2001. Molecular cloning andcharacterization of a dermatan-specific N-acetylgalactosamine 4-O-sulfotransferase.J Biol Chem 276:344–353.
Eyre DR, Shapiro FD, Aldridge JF. 1985.A heterozygous collagen defect in a variantof the Ehlers–Danlos syndrome type VII.Evidence for a deleted amino-telopeptidedomain in the pro-alpha 2(I) chain. J BiolChem 260:11322–11329.
Faiyaz-Ul-Haque M, Zaidi SH, Al-Ali M, Al-MureikhiMS, Kennedy S, Al-Thani G, TsuiLC, Teebi AS. 2004. A novel missense
mutation in the galactosyltransferase-I(B4GALT7) gene in a family exhibitingfacioskeletal anomalies and Ehlers–Danlossyndrome resembling the progeroid type.Am J Med Genet Part A 128A:39–45.
Fernandes RJ, Hirohata S, Engle JM, Colige A,Cohn DH, Eyre DR, Apte SS. 2001.Procollagen II amino propeptide processingby ADAMTS-3. Insights on dermatospar-axis. J Biol Chem 276:31502–31509.
Fjolstad M, Helle O. 1974. A hereditary dysplasiaof collagen tissues in sheep. J Pathol112:183–188.
Fujimoto A, Wilcox WR, Cohn DH. 1997.Clinical, morphological, and biochemicalphenotype of a new case of Ehlers–Danlossyndrome type VIIC. Am J Med Genet68:25–28.
Fukada T, Civic N, Furuichi T, Shimoda S,Mishima K, Higashiyama H, Idaira Y, AsadaY, Kitamura H, Yamasaki S, Hojyo S,Nakayama M, Ohara O, Koseki H, DosSantos HG, Bonafe L, Ha-Vinh R, Zankl A,Unger S, Kraenzlin ME, Beckmann JS, SaitoI, Rivolta C, Ikegawa S, Superti-Furga A,Hirano T. 2008. The zinc transporterSLC39A13/ZIP13 is required for connec-tive tissue development; its involvement inBMP/TGF-beta signaling pathways. PLoSONE 3:e3642.
Fukada T, Hojyo S, Furuichi T. 2013. Zinc signal:A new player in osteobiology. J Bone MinerMetab 31:129–135.
Gaboriaud C, Ling WL, Thielens NM, Bally I,Rossi V. 2014. Deciphering the fine detailsof c1 assembly and activation mechanisms:“Mission impossible”? Front Immunol5:565.
Gaines R, Tinkle BT, Halandras PM, Al-Nouri O,Crisostomo P, Cho JS. 2015. Spontaneousruptured dissection of the right commoniliac artery in a patient with classic Ehlers–Danlos syndrome phenotype. Ann Vasc Surg29:595;e511–e594.
Galat A. 2003. Peptidylprolyl cis/trans isomerases(immunophilins): Biological diversity–tar-gets–functions. Curr Top Med Chem3:1315–1347.
Galli GG, Honnens de Lichtenberg K, Carrara M,Hans W, Wuelling M, Mentz B, MulthauptHA, Fog CK, Jensen KT, Rappsilber J,Vortkamp A, Coulton L, Fuchs H, Gailus-Durner V, Hrab�e de Angelis M, CalogeroRA, Couchman JR, Lund AH. 2012.Prdm5 regulates collagen gene transcriptionby association with RNA polymerase II indeveloping bone. PLoS Genet 8:e1002711.
Gensure RC, Makitie O, Barclay C, Chan C,Depalma SR, Bastepe M, Abuzahra H,Couper R, Mundlos S, Sillence D, AlaKokko L, Seidman JG, Cole WG, JuppnerH. 2005. A novel COL1A1 mutation ininfantile cortical hyperostosis (Caffey dis-ease) expands the spectrum of collagen-related disorders. J Clin Invest115:1250–1257.
George SM, Vandersteen A, Nigar E, FergusonDJ, Topham EJ, Pope FM. 2016. TwoEhlers–Danlos syndrome type VIII patietswith unexpected hoarseness. Clin ExpDermatol 41:771–774.
Gerrits KH, Voermans NC, de Haan A, vanEngelen BG. 2013. Neuromuscular proper-ties of the thigh muscles in patients with
Ehlers–Danlos syndrome. Muscle Nerve47:96–104.
Giovannucci Uzielli ML, Giunta C, Scarselli G,DayanN, lapi E, DiMedio L. 2011. A 7 yearsfollow-up of a new case of Ehelrs–Danlossyndrome type VIIB: Major problems arerepresented by bilateral, extremely severe hipdislocation. in 12th International Congressof Human Genetics/61st Annual Meeting ofthe American Society of Human Genetics.Montreal, Canada.
Giunta C, Chambaz C, PedemonteM, Scapolan S,Steinmann B. 2008a. The arthrochalasia typeof Ehlers–Danlos syndrome (EDS VIIA andVIIB): The diagnostic value of collagen fibrilultrastructure. Am J Med Genet Part A146A:1341–1346.
Giunta C, ElScioglu NH, Albrecht B, Eich G,Chambaz C, Janecke AR, Yeowell H, WeisM, Eyre DR, Kraenzlin M, Steinmann B.2008b. Spondylocheiro dysplastic form ofthe Ehlers–Danlos syndrome—An autoso-mal-recessive entity caused by mutations inthe zinc transporter gene SLC39A13. Am JHum Genet 82:1290–1305.
Giunta C, Randolph A, Al-Gazali LI, BrunnerHG, Kraenzlin ME, Steinmann B. 2005a.Nevo syndrome is allelic to the kyphoscoli-otic type of the Ehlers–Danlos syndrome(EDS VIA). Am J Med Genet Part A133A:158–164.
Giunta C, Randolph A, Steinmann B. 2005b.Mutation analysis of the PLOD1 gene: Anefficient multistep approach to themoleculardiagnosis of the kyphoscoliotic type ofEhlers–Danlos syndrome (EDS VIA). MolGenet Metab 86:269–276.
Giunta C, Steinmann B. 2014. Arthrochalasis typeof Ehlers–Danlos syndrome (EDS typesVIIA and VIIB) and related disorders. In:Shapiro JR, Byers PH, Glorieux FH,Sponseller PD, editors. Osteogenesis imper-fect: A translational approach to brittle bonedisease. Amsterdam: Elsevier Inc. pp217–228.
Giunta C, Superti-Furga A, Spranger S, ColeWG,Steinmann B. 1999. Ehlers–Danlos syn-drome type VII: Clinical features andmolecular defects. J Bone Joint Surg Am81:225–238.
Gok E, Goksel OS, Alpagut U, Dayioglu E. 2012.Spontaneous brachial pseudo-aneurysm in a12-year-old with kyphoscoliosis-type Eh-lers–Danlos Syndrome. Eur J Vasc EndovascSurg 44:482–484.
Gotte M, Spillmann D, Yip GW, Versteeg E,Echtermeyer FG, van Kuppevelt TH, KieselL. 2008. Changes in heparan sulfate areassociated with delayed wound repair,altered cell migration, adhesion and con-tractility in the galactosyltransferase I (be-ta4GalT-7) deficient form of Ehlers–Danlossyndrome. Hum Mol Genet 17:996–1009.
Guo MH, Stoler J, Lui J, Nilsson O, Bianchi DW,Hirschhorn JN, Dauber A. 2013. Redefin-ing the progeroid form of Ehlers–Danlossyndrome: Report of the fourth patient withB4GALT7 deficiency and review of theliterature. Am J Med Genet Part A161A:2519–2527.
Ha VT, Marshall MK, Elsas LJ, Pinnell SR,Yeowell HN. 1994. A patient with Ehlers–Danlos syndrome type VI is a compoundheterozygote for mutations in the lysyl

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 111
hydroxylase gene. J Clin Invest93:1716–1721.
Hanset R, Lapiere CM. 1974. Inheritance ofdermatosparaxis in the calf. A genetic defectof connective tissues. J Hered 65:356–358.
Hart TC, Atkinson JC. 2007. Mendelian forms ofperiodontitis. Periodontol 2000 45:95–112.
Hartsfield JK, Jr., Kousseff BG. 1990. Phenotypicoverlap of Ehlers–Danlos syndrome types IVand VIII. Am J Med Genet 37:465–470.
Hass J, Hass R. 1958. Arthrochalasis multiplexcongenita; congenital flaccidity of the joints.J Bone Joint Surg Am 40A:663–674.
Hata R, Kurata S, Shinkai H. 1988. Existence ofmalfunctioning pro alpha2(I) collagen genesin a patient with a pro alpha 2(I)-chain-defective variant of Ehlers–Danlos syn-drome. Eur J Biochem 174:231–237.
Hatamochi A, Hamada T, Yoshino M, HashimotoT. 2014. The first Japanese case of thearthrochalasia type of Ehlers–Danlos syn-drome with COL1A2 gene mutation. Gene538:199–203.
Hautala T, Heikkinen J, Kivirikko KI, Myllyla R.1993. A large duplication in the gene forlysyl hydroxylase accounts for the type VIvariant of Ehlers–Danlos syndrome in twosiblings. Genomics 15:399–404.
Heikkinen J, Pousi B, Pope M, Myllyla R. 1999.A null-mutated lysyl hydroxylase gene in acompound heterozygote British patientwith Ehlers–Danlos syndrome type VI.Hum Mutat 14:351.
Hendriks AG, Voermans NC, Schalkwijk J,Hamel BC, van Rossum MM. 2012. Well-defined clinical presentation of Ehlers–Danlos syndrome in patients with tenascin-X deficiency: A report of four cases. ClinDysmorphol 21:15–18.
Hernandez A, Aguirre-Negrete MG, Gonzalez-Flores S, Reynoso-Luna MC, Fragoso R,Nazara Z, Tapia-Arizmendi G, Cantu JM.1986. Ehlers–Danlos features with progeroidfacies and mild mental retardation. Furtherdelineation of the syndrome. Clin Genet30:456–461.
Hernandez A, Aguirre-Negrete MG, Liparoli JC,Cantu JM. 1981. Third case of a distinctvariant of the Ehlers-Danlos Syndrome(EDS). Clin Genet 20:222–224.
Hernandez A, Aguirre-Negrete MG, Ramirez-Soltero S, Gonzalez-Mendoza A,Martinez yMartinez R, Velazquez-Cabrera A, CantuJM. 1979. A distinct variant of the Ehlers–Danlos syndrome. Clin Genet 16:335–339.
Hicks D, Farsani GT, Laval S, Collins J, Sarkozy A,Martoni E, Shah A, Zou Y, Koch M,Bonnemann CG, Roberts M, LochmullerH, Bushby K, Straub V. 2014. Mutations inthe collagen XII gene define a new form ofextracellular matrix-related myopathy. HumMol Genet 23:2353–2363.
Ho KK, Kong RY, Kuffner T, Hsu LH, Ma L,Cheah KS. 1994. Further evidence that thefailure to cleave the aminopropeptide oftype I procollagen is the cause of Ehlers–Danlos syndrome type VII. Hum Mutat3:358–364.
Hoehn R, Zeller T, Verhoeven VJ, Grus F, AdlerM, Wolfs RC, Uitterlinden AG, CastagneR, Schillert A, Klaver CC, Pfeiffer N,Mirshahi A. 2012. Population-based meta-analysis in Caucasians confirms associationwith COL5A1 and ZNF469 but not
COL8A2 with central corneal thickness.Hum Genet 131:1783–1793.
Hoffman GS, Filie JD, Schumacher HR, Jr.,Ortiz-Bravo E, TsokosMG,Marini JC, KerrGS, Ling QH, Trentham DE. 1991. Intrac-table vasculitis, resorptive osteolysis, andimmunity to type I collagen in type VIIIEhlers–Danlos syndrome. Arthritis Rheum34:1466–1475.
Holbrook KA, Byers PH. 1982. Structuralabnormalities in the dermal collagen andelastic matrix from the skin of patients withinherited connective tissue disorders. J InvestDermatol 79:7s–16s.
Honey EM. 2016. Spondyloepimetaphyseal dys-plasia with joint laxity (Beighton type): Aunique South African disorder. S Afr Med J106:S54–S56.
Hudgins LCC, Drummond-Borg LM, AtkinsonM, Schwarze U, Byers PH. 1999. Clinicaland molecular findings in Ehlers–Danlossyndrome type VIIA. Am J Hum Genet 65.
Hyland J, Ala-Kokko L, Royce P, Steinmann B,Kivirikko KI, Myllyla R. 1992.A homozygous stop codon in the lysylhydroxylase gene in two siblings withEhlers–Danlos syndrome type VI. NatGenet 2:228–231.
Ihme A, Risteli L, Krieg T, Risteli J, Feldmann U,Kruse K, Muller PK. 1983. Biochemicalcharacterization of variants of the Ehlers–Danlos syndrome type VI. Eur J Clin Invest13:357–362.
Ishikawa Y, Bachinger HP. 2014. A substratepreference for the rough endoplasmicreticulum resident protein FKBP22 duringcollagen biosynthesis. J Biol Chem289:18189–18201.
Janecke AR, Baenziger JU, M€uller T, D€undar M.2011. Loss of dermatan-4-sulfotransferase 1(D4ST1/CHST14) function represents thefirst dermatan sulfate biosynthesis defect,“dermatan sulfate-deficient adductedthumb-clubfoot syndrome”. Hum Mutat32:484–485.
Janecke AR, Li B, Boehm M, Krabichler B,Rohrbach M, M€uller T, Fuchs I, Golas G,Katagiri Y, Ziegler SG, Gahl WA, Wilnai Y,Zoppi N, Geller HM, Giunta C, SlavotinekA, Steinmann B. 2016. The phenotype ofthe musculocontractural type of Ehlers–Danlos syndrome due to CHST14 muta-tions. Am J Med Genet Part A170A:103–115.
Janecke AR, Unsinn K, Kreczy A, Baldissera I,Gassner I, Neu N, Utermann G, M€uller T.2001. Adducted thumb-club foot syndromein sibs of a consanguineous Austrian family.J Med Genet 38:265–269.
Jeong J, Walker JM, Wang F, Park JG, Palmer AE,Giunta C, Rohrbach M, Steinmann B, EideDJ. 2012. Promotion of vesicular zinc effluxby ZIP13 and its implications for spondy-locheiro dysplastic Ehlers–Danlos syndrome.Proc Natl Acad Sci USA 109:E3530–E3538.
Kapferer-Seebacher I, Pepin M, Werner R,Aitman TJ, Nordgren A, Stoiber H, Thie-lens N, Gaboriaud C, Amberger A, SchossigA, Gruber R, Giunta C, BamshadM, Bj€orckE, Chen C, Chitayat D, Dorschner M,Schmitt-Egenolf M, Hale C, Hanna D,Hennies H, Heiss-Kisielewsky I, LindstrandA, Lundberg P, Mitchell AL, Nickerson DA,Reinstein E, Rohrbach M, Romani N,
Schmuth M, Silver R, Taylan F, VandersteenA, Vandrovcova J, Weerakkody R, Yang M,Pope F, Byers PH, Zschocke J; MolecularBasis of Periodontal EDS Consortium.2016. Periodontal Ehlers–Danlos syndromeis caused by mutations in C1R and C1S,which encode subcomponents C1r and C1sof complement. Am J Hum Genet99:1005–1014.
Kariminejad A, Bozorgmehr B, Khatami A,Kariminejad MH, Giunta C, Steinmann B.2010. Ehlers–Danlos syndrome type VI in a17-year-old Iranian boy with severe muscu-lar weakness—A diagnostic challenge? Iran JPediatr 20:358–362.
KassebaumNJ, Bernab�e E, DahiyaM, Bhandari B,Murray CJ, Marcenes W. 2014. Globalburden of severe periodontitis in 1990–2010: A systematic review and meta-regres-sion. J Dent Res 93:1045–1053.
Khan AO, Aldahmesh MA, Alkuraya FS. 2010.Brittle cornea without clinically-evidentextraocular findings in an adult harboring anovel homozygous ZNF469 mutation.Ophthalmic Genet 33:257–259.
Khan AO, Aldahmesh MA, Mohamed JN,Alkuraya FS. 2012. Blue sclera with andwithout corneal fragility (brittle corneasyndrome) in a consanguineous familyharboring ZNF469 mutation (p.E1392X).Arch Ophthalmol 128:1376–1379.
Klaassens M, Reinstein E, Hilhorst-Hofstee Y,Schrander JJ, Malfait F, Staal H, ten HaveLC, Blaauw J, Roggeveen HC, Krakow D,De Paepe A, van Steensel MA, Pals G,Graham JM, Jr., Schrander-Stumpel CT.2012. Ehlers–Danlos arthrochalasia type(VIIA-B)—expanding the phenotype:From prenatal life through adulthood. ClinGenet 82:121–130.
Knuijt S, Kalf JG, de Swart BJ, Drost G, HendricksHT, Geurts AC, van Engelen BG. 2014.Dysarthria and dysphagia are highly preva-lent among various types of neuromusculardiseases. Disabil Rehabil 36:1285–1289.
Kobayasi T. 2004. Abnormality of dermal collagenfibrils in Ehlers–Danlos syndrome. Antici-pation of the abnormality for the inheritedhypermobile disorders. Eur J Dermatol14:221–229.
Kojima T, Shinkai H, Fujita M, Morita E,Okamoto S. 1988. Case report and studyof collagen metabolism in Ehlers–Danlossyndrome type II. J Dermatol 15:155–160.
KonoM,Hasegawa-Murakami Y, Sugiura K,OnoM, Toriyama K, Miyake N, Hatamochim A,Kamei Y, Kosho T, AkiyamaM. 2016. A 45-year-old woman with Ehlers–Danlos syn-drome caused by dermatan 4-O-sulfotrans-ferase-1 deficiency: Implications for earlyageing. Acta Derm Venereol 96:830–831.
Kosho T. 2013. Discovery and delineation ofdermatan 4-O-sulfotransferase-1 (D4ST1)-deficient Ehlers–Danlos syndrome. Croatia:InTech.
Kosho T. 2016. Dermatan 4-O-sulfotransferase 1-deficiency: A new form of Ehlers–Danlossyndrome characterized by various malfor-mations and progressive multisystem fragil-ity-related manifestations. Pediatr Int58:88–99.
Kosho T, Miyake N, Hatamochi A, Takahashi J,Kato H, Miyahara T, Igawa Y, Yasui H,Ishida T, Ono K, Kosuda T, Inoue A,

112 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
Kohyama M, Hattori T, Ohashi H, Nishi-mura G, KawamuraR,Wakui K, FukushimaY, Matsumoto N. 2010. A new Ehlers–Danlos syndrome with craniofacial charac-teristics, multiple congenital contractures,progressive joint and skin laxity, and multi-system fragility-related manifestations. Am JMed Genet Part A 152A:1333–1346.
Kosho T, Miyake N, Mizumoto S, Hatamochi A,Fukushima Y, Yamada S, Sugahara K,Matsumoto N. 2011. A response to: Lossof dermatan-4-sulfotransferase 1 (D4ST1/CHST14) function represents the firstdermatan sulfate biosynthesis defect, “der-matan sulfate-deficient adducted thumb-clubfoot syndrome”. Which name is appro-priate, “adducted thumb-clubfoot syn-drome” or “Ehlers-Danlos syndrome”?Hum Mutat 32:1507–1509.
Kosho T, Mizumoto S, Sugahara K. 2014.Carbohydrate (N-acetylgalactosamine 4-O)sulfotransferase 14 (CHST14). In: TaniguchiN, Honke K, Fukuda M, Narimatsu H,Yamaguchi Y, Angata T, editors. Handbookof glycosyltransferases and related genes.Berlin: Springer. pp 1135–1148.
Kosho T, Takahashi J, Ohashi H, Nishimura G,Kato H, Fukushima Y. 2005. Ehlers–Danlossyndrome type VIB with characteristicfacies, decreased curvatures of the spinalcolumn, and joint contractures in twounrelated girls. Am J Med Genet Part A138A:282–287.
Krane SM, Pinnell SR, Erbe RW. 1972. Lysyl-protocollagen hydroxylase deficiency infibroblasts from siblings with hydroxyly-sine-deficient collagen. Proc Natl Acad SciUSA 69:2899–2903.
Kresse H, Rosthoj S, Quentin E, Hollmann J,Glossl J, Okada S, Tonnesen T. 1987.Glycosaminoglycan-free small proteoglycancore protein is secreted by fibroblasts from apatient with a syndrome resembling proge-roid. Am J Hum Genet 41:436–453.
Krieg T, Feldmann U, Kessler W, Muller PK.1979. Biochemical characteristics of Ehlers–Danlos syndrome type VI in a family withone affected infant. Hum Genet 46:41–49.
Lapiere CM, Nusgens BV. 1981. Ehlers–Danlos(Ed) type-VIII skin has a reduced proportionof collagen type-III. J Invest Dermatol76:422–422.
Le Goff C, Somerville RP, Kesteloot F, Powell K,Birk DE, Colige AC, Apte SS. 2006.Regulation of procollagen amino-propep-tide processing duringmouse embryogenesisby specialization of homologous ADAMTSproteases: Insights on collagen biosynthesisand dermatosparaxis. Development133:1587–1596.
Lechner J, Porter LF, Rice A, Vitart V, ArmstrongDJ, Schorderet DF, Munier FL, Wright AF,Inglehearn CF, Black GC, Simpson DA,Manson F, Willoughby CE. 2014. Enrich-ment of pathogenic alleles in the brittlecornea gene, ZNF469, in keratoconus.Hum Mol Genet 23:5527–5535.
Lehmann HW, Mundlos S, Winterpacht A,Brenner RE, Zabel B, Muller PK. 1994.Ehlers–Danlos syndrome type VII: Pheno-type and genotype. Arch Dermatol Res286:425–428.
Lenaers A, Ansay M, Nusgens BV, Lapiere CM.1971. Collagen made of extended—chains,
procollagen, in genetically-defective derma-tosparaxic calves. Eur J Biochem23:533–543.
Lichtenstein JR, Kohn LD, Martin GR, Byers P,McKusick VA. 1973a. Procollagen peptidasedeficiency in a form of the Ehlers–Danlossyndrome. Trans Assoc Am Physicians86:333–339.
Lichtenstein JR,Martin GR, Kohn LD, Byers PH,McKusick VA. 1973b. Defect in conversionof procollagen to collagen in a form ofEhlers–Danlos syndrome. Science182:298–300.
Lindor NM, Bristow J. 2005. Tenascin-X defi-ciency in autosomal recessive Ehlers–Danlossyndrome. Am J Med Genet Part A135A:75–80.
Lu Y, Dimasi DP, Hysi PG, Hewitt AW, BurdonKP, Toh T, Ruddle JB, Li YJ, Mitchell P,Healey PR, Montgomery GW, Hansell N,Spector TD, Martin NG, Young TL,Hammond CJ, Macgregor S, Craig JE,Mackey DA. 2010. Common genetic var-iants near the Brittle Cornea Syndromelocus ZNF469 influence the blinding diseaserisk factor central corneal thickness. PLoSGen 13;6:e1000947.
Lund A, Joensen F, Christensen E, Duno M,Skovby F, Schwartz M. 2008. A novelarginine-to-cysteine substitution in thetriple helical region of the alpha1(I) collagenchain in a family with an osteogenesisimperfecta/Ehlers–Danlos phenotype. ClinGenet 73:97–101.
Malfait F, De Coster P, Hausser I, van Essen AJ,Franck P, Colige A, Nusgens B, Martens L,De Paepe A. 2004. The natural history,including orofacial features of three patientswith Ehlers–Danlos syndrome, dermato-sparaxis type (EDS type VIIC). Am J MedGenet Part A 131A:18–28.
Malfait F, Kariminejad A, Van Damme T, GaucheC, Syx D, Merhi-Soussi F, Gulberti S,Symoens S, Vanhauwaert S, Willaert A,Bozorgmehr B, Kariminejad MH, Ebrahi-miadibN,Hausser I, Huysseune A, Fournel-Gigleux S, De Paepe A. 2013. Defectiveinitiation of glycosaminoglycan synthesisdue to B3GALT6 mutations causes apleiotropic Ehlers–Danlos-syndrome-likeconnective tissue disorder. Am J HumGenet92:935–945.
Malfait F, Symoens S, Coucke P, Nunes L, DeAlmeida S, De Paepe A. 2006. Total absenceof the alpha2(I) chain of collagen type Icauses a rare form of Ehlers–Danlos syn-dromewith hypermobility and propensity tocardiac valvular problems. J Med Genet 43:e36.
Malfait F, Symoens S, De Backer J, Hermanns-LeT, Sakalihasan N, Lapiere CM, Coucke P,De Paepe A. 2007. Three arginine tocysteine substitutions in the pro-alpha (I)-collagen chain cause Ehlers–Danlos syn-drome with a propensity to arterial rupturein early adulthood. Hum Mutat28:387–395.
Malfait F, Syx D, Vlummens P, Symoens S,Nampoothiri S, Hermanns-Le T, Van LaerL, De Paepe A. 2010. MusculocontracturalEhlers–Danlos syndrome (former EDStype VIB) and adducted thumb clubfootsyndrome (ATCS) represent a singleclinical entity caused by mutations in the
dermatan-4-sulfotransferase 1 encodingCHST14 gene. Hum Mutat 31:1233–1239.
Mao JR, Bristow J. 2001. The Ehlers–Danlossyndrome: On beyond collagens. J ClinInvest 107:1063–1069.
Mataix J, Ba~nuls J, Mu~noz C, Bermejo A, ClimentJM. 2008. Periodontal Ehlers–Danlos syn-drome associated with type III and I collagendeficiencies. Br J Dermatol 158:825–830.
McKusick VA. 1972. Heritable disorders ofconnective tissue. St. Louis: MosbyCompany.
Meani N, Pezzimenti F, Deflorian G, Mione M,Alcalay M. 2009. The tumor suppressorPRDM5 regulates Wnt signaling at earlystages of zebrafish development. PLoS ONE4:e4273.
Mendoza-Londono R, Chitayat D, Kahr WH,Hinek A, Blaser S, Dupuis L, Goh E, Badilla-Porras R, Howard A, Mittaz L, Superti-Furga A, Unger S, Nishimura G, Bonafe L.2012. Extracellular matrix and plateletfunction in patients with musculocontrac-tural Ehlers–Danlos syndrome caused bymutations in the CHST14 gene. Am J MedGenet Part A 158A:1344–1354.
Meng H, Ren X, Tian Y, Feng X, Xu L, Zhang L,Lu R, Shi D, Chen ZJ. 2011. Genetic studyof families affected with aggressive peri-odontitis. Periodontol 2000 56:87–101.
Merke DP, Chen W, Morissette R, Xu Z, VanRyzin C, Sachdev V, Hannoush H, Shanb-hag SM, Acevedo AT, Nishitani M, Arai AE,McDonnell NB. 2013. Tenascin-X haploin-sufficiency associated with Ehlers–Danlossyndrome in patients with congenital adrenalhyperplasia. J Clin Endocrinol Metab 98:E379–E387.
Miyake N, Kosho T, Mizumoto S, Furuichi T,Hatamochi A, Nagashima Y, Arai E,Takahashi K, Kawamura R, Wakui K,Takahashi J, Kato H, Yasui H, Ishida T,Ohashi H,Nishimura G, ShiinaM, Saitsu H,Tsurusaki Y, Doi H, Fukushima Y, IkegawaS, Yamada S, Sugahara K, Matsumoto N.2010. Loss-of-function mutations ofCHST14 in a new type of Ehles–Danlossyndrome. Hum Mutat 31:966–974.
Mochida K, AmanoM,Miyake N,Matsumoto N,Hatamochi A, Kosho T. 2016. Dermatan 4-O-sulfotransferase 1-deficient Ehlers–Dan-los syndrome complicated by a large subcu-taneous hematoma on the back. J Dermatol43:832–833.
Morissette R, Chen W, Perritt AF, Dreiling JL,Arai AE, Sachdev V, Hannoush H, MallappaA, Xu Z, McDonnell NB, Quezado M,Merke DP. 2015. Broadening the spectrumof Ehlers–Danlos syndrome in patients withcongenital adrenal hyperplasia. J Clin En-docrinol Metab 100:E1143–E1152.
M€uller T, Mizumoto S, Suresh I, Komatsu Y,Vodopiutz J, Dundar M, Straub V, LingenhelA, Melmer A, Lechner S, Zschocke J,Sugahara K, Janecke AR. 2013. Loss ofdermatan sulfate epimerase (DSE) functionresults in musculocontractural Ehlers–Dan-los syndrome. Hum Mol Genet22:3761–3772.
Murray ML, Yang M, Fauth C, Byers PH. 2014.FKBP14-related Ehlers–Danlos syndrome:Expansion of the phenotype to includevascular complications. Am J Med GenetPart A 164A:1750–1755.

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 113
NakajimaM,Mizumoto S, Miyake N, Kogawa R,Iida A, Ito H, Kitoh H, Hirayama A,Mitsubuchi H, Miyazaki O, Kosaki R,Horikawa R, Lai A, Mendoza-LondonoR, Dupuis L, Chitayat D, Howard A, LealGF, Cavalcanti D, Tsurusaki Y, Saitsu H,Watanabe S, Lausch E, Unger S, Bonafe L,Ohashi H, Superti-Furga A, Matsumoto N,Sugahara K, Nishimura G, Ikegawa S. 2013.Mutations in B3GALT6, which encodes aglycosaminoglycan linker region enzyme,cause a spectrum of skeletal and connectivetissue disorders. Am J Hum Genet92:927–934.
Nicholls AC, Oliver J, Renouf DV, McPheat J,Palan A, Pope FM. 1991. Ehlers–Danlossyndrome type VII: A single base change thatcauses exon skipping in the type I collagenalpha 2(I) chain. Hum Genet 87:193–198.
Nicholls AC, Osse G, Schloon HG, Lenard HG,Deak S, Myers JC, Prockop DJ,WeigelWR,Fryer P, Pope FM. 1984. The clinical featuresof homozygous alpha 2(I) collagen deficientosteogenesis imperfecta. J Med Genet21:257–262.
Nicholls AC, Sher JL, Wright MJ, Oley C,Mueller RF, Pope FM. 2000. Clinicalphenotypes and molecular characterizationof three patients with Ehlers–Danlos syn-drome type VII. J Med Genet 37:E33.
Nicholls AC, Valler D, Wallis S, Pope FM. 2001.Homozygosity for a splice site mutation ofthe COL1A2 gene yields a non-functionalpro(alpha)2(I) chain and an EDS/OI clinicalphenotype. J Med Genet 38:132–136.
Nusgens BV, Verellen-Dumoulin C, Hermanns-Le T, De Paepe A, Nuytinck L, Pierard GE,Lapiere CM. 1992. Evidence for a relation-ship between Ehlers–Danlos type VII C inhumans and bovine dermatosparaxis. NatGenet 1:214–217.
Nuytinck L, Freund M, Lagae L, Pierard GE,Hermanns-Le T, De Paepe A. 2000. Classi-cal Ehlers–Danlos syndrome caused by amutation in type I collagen. Am J HumGenet 66:1398–1402.
O’Connell M, Burrows NP, van Vlijmen-WillemsMJ, Clark SM, Schalkwijk J. 2010. Tenascin-X deficiency and Ehlers–Danlos syndrome:A case report and review of the literature. BrJ Dermatol 163:1340–1345.
Okajima T, Fukumoto S, Furukawa K, Urano T.1999. Molecular basis for the progeroidvariant of Ehlers–Danlos syndrome. Identi-fication and characterization of two muta-tions in galactosyltransferase I gene. J BiolChem 274:28841–28844.
Ottenheijm CA, Voermans NC, Hudson BD,Irving T, Stienen GJ, van Engelen BG,Granzier H. 2012. Titin-based stiffening ofmuscle fibers in Ehlers–Danlos syndrome.J Appl Physiol (1985) 112:1157–1165.
Patrick RA, Taubman SB, Lepow IH. 1970.Cleavage of the fourth component of humancomplement (C4) by activated Cls. Immu-nochemistry 7:217–225.
P�enisson-Besnier I, Allamand V, Beurrier P,Martin L, Schalkwijk J, van Vlijmen-Willems I, Gartioux C, Malfait F, Syx D,Macchi L, Marcorelles P, Arbeille B, CroueA, De Paepe A, Dubas F. 2013. Compoundheterozygous mutations of the TNXB genecause primary myopathy. NeuromusculDisord 23:664–669.
Peeters AC, Kucharekova M, Timmermans J, vanden Berkmortel FW, Boers GH, Nov�akov�aIR, Egging D, den Heijer M, Schalkwijk J.2004. A clinical and cardiovascular survey ofEhlers–Danlos syndrome patients with com-plete deficiency of tenascin-X. Neth J Med62:160–162.
Pihlajaniemi T, Dickson LA, Pope FM, KorhonenVR, Nicholls A, Prockop DJ, Myers JC.1984. Osteogenesis imperfecta: Cloning of apro-alpha 2(I) collagen gene with a frame-shift mutation. J Biol Chem259:12941–12944.
Pinnell SR, Krane SM, Kenzora JE, Glimcher MJ.1972. A heritable disorder of connectivetissue. Hydroxylysine-deficient collagen dis-ease. N Engl J Med 286:1013–1020.
Pope FM, Nicholls AC, Palan A, Kwee ML, DeGroot WP, Hausmann R. 1992. Clinicalfeatures of an affected father and daughterwith Ehlers–Danlos syndrome type VIIB. BrJ Dermatol 126:77–82.
Porter LF, Galli GG,Williamson S, Selley J, KnightD, Elcioglu N, Aydin A, Elcioglu M,Venselaar H, Lund AH, Bonshek R, BlackGC, Manson FD. 2015. A role for repressivecomplexes and H3K9 di-methylation inPRDM5-associated brittle cornea syn-drome. Hum Mol Genet 24:6565–6579.
Punetha J, Kesari A, Hoffman EP, Gos M,Kaminska A, Kostera-Pruszczyk A, Haus-manowa-Petrusewicz I, Hu Y, Zou Y,Bonnemann CG, JEdrzejowska M. 2016.Novel Col12A1 variant expands the clinicalpicture of congenital myopathies withextracellular matrix defects. Muscle Nerve55:277–281.
Quentin E, Gladen A, Roden L, Kresse H. 1990.A genetic defect in the biosynthesis ofdermatan sulfate proteoglycan: Galactosyl-transferase I deficiency in fibroblasts from apatient with a progeroid syndrome. ProcNatl Acad Sci USA 87:1342–1346.
Rahman N, Dunstan M, Teare MD, Hanks S,Douglas J, Coleman K, Bottomly WE,Campbell ME, Berglund B, Nordenskj€oldM, Forssell B, Burrows N, Lunt P, YoungID, Williams N, Bignell G, Futreal PA,Pope FM. 2003. Ehlers–Danlos syndromewith severe early-onset periodontal disease(EDS-VIII) is a distinct, heterogeneousdisorder with one predisposition gene atchromosome 12p13. Am J Hum Genet73:198–204.
Ramappa M, Wilson ME, Rogers RC, TrivediRH. 2014. Brittle cornea syndrome: A casereport and comparison with Ehlers–Danlossyndrome. J AAPOS 18:509–511.
Reardon W, Winter RM, Smith LT, Lake BD,Rossiter M, Baraitser M. 1995. The naturalhistory of human dermatosparaxis (Ehlers–Danlos syndrome type VIIC). Clin Dys-morphol 4:1–11.
Reinstein E, DeLozier CD, Simon Z, Bannykh S,Rimoin DL, Curry CJ. 2013. Ehlers–Danlossyndrome type VIII is clinically heteroge-neous disorder associated primarily withperiodontal disease, and variable connectivetissue features. Eur J Hum Genet21:233–236.
Reinstein E, Pariani M, Lachman RS, Nemec S,Rimoin DL. 2012. Early-onset osteoarthri-tis in Ehlers–Danlos syndrome type VIII.Am J Med Genet Part A 158A:938–941.
Reinstein E, Wang RY, Zhan L, Rimoin DL,Wilcox WR. 2011. Ehlers–Danlos typeVIII, periodontitis-type: Further delineationof the syndrome in a four-generationpedigree. Am J Med Genet Part A155A:742–747.
Ritelli M, Chiarelli N, Zoppi N, Dordoni C,Quinzani S, Traversa M, Venturini M,Calzavara-Pinton P, Colombi M. 2015.Insights in the etiopathology of galactosyl-transferase II (GalT-II) deficiency fromtranscriptome-wide expression profiling ofskin fibroblasts of two sisters with compoundheterozygosity for two novel B3GALT6mutations. Mol Genet Metab Rep 2:1–15.
Ritelli M, Dordoni C, Venturini M, Chiarelli N,Quinzani S, TraversaM, Zoppi N, VascellaroA, Wischmeijer A, Manfredini E, GaravelliL, Calzavara-Pinton P, Colombi M. 2013.Clinical and molecular characterization of40 patients with classic Ehlers–Danlossyndrome: Identification of 18 COL5A1and 2 COL5A2 novel mutations. Orphanet JRare Dis 8:58.
Rohrbach M, Spencer HL, Porter LF, Burkitt-Wright EM, B€urer C, Janecke A, Bakshi M,Sillence D, Al-Hussain H, Baumgartner M,Steinmann B, Black GC, Manson FD,Giunta C. 2013. ZNF469 frequently mu-tated in the brittle cornea syndrome (BCS) isa single exon gene possibly regulating theexpression of several extracellular matrixcomponents. Mol Genet Metab109:289–295.
RohrbachM,Vandersteen A, YisU, SerdarogluG,Ataman E, Chopra M, Garcia S, Jones K,Kariminejad A, Kraenzlin M, Marcelis C,Baumgartner M, Giunta C. 2011. Pheno-typic variability of the kyphoscoliotic type ofEhlers–Danlos syndrome (EDS VIA): Clini-cal, molecular, and biochemical delineation.Orphanet J Rare Dis 6:46.
Rossi V, Bally I, Lacroix M, Arlaud GJ, ThielensNM. 2014. Classical complement pathwaycomponents C1r and C1s: Purification fromhuman serum and in recombinant form andfunctional characterization. Methods MolBiol 1100:43–60.
Royce PM, Steinmann B, Vogel A, SteinhorstU, Kohlschuetter A. 1990. Brittle corneasyndrome: An heritable connective tissuedisorder distinct from Ehlers–Danlos syn-drome type VI and fragilitas oculi, withspontaneous perforations of the eye,blue sclerae, red hair, and normalcollagen lysyl hydroxylation. Eur J Pediatr149:465–469.
Rutsch F, MacDougall M, Lu C, Buers I,MamaevaO,NitschkeY,RiceGI, ErlandsenH, Kehl HG, Thiele H, N€urnberg P, H€ohneW, Crow YJ, Feigenbaum A, HennekamRC. 2015. A specific IFIH1 gain-of-function mutation causes Singleton–Mertensyndrome. Am J Hum Genet 96:275–282.
Sakiyama T, Kubo A, Sasaki T, Yamada T, Yabe N,Matsumoto K, Futei Y. 2015. Recurrentgastrointestinal perforation in a patient withEhlers–Danlos syndrome due to tenascin-Xdeficiency. J Dermatol 42:511–514.
Salter CG, Davies JH, Moon RJ, Fairhurst J,Bunyan D, Study DDD, Foulds N. 2016.Further defining the phenotypic spectrum ofB4GALT7 mutations. Am J Med Genet PartA 170A:1556–1563.

114 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) RESEARCH REVIEW
Sasaki T, Arai K, Ono M, Yamaguchi T, Furuta S,Nagai Y. 1987. Ehlers–Danlos syndrome. Avariant characterized by the deficiency of proalpha 2 chain of type I procollagen. ArchDermatol 123:76–79.
Schalkwijk J, ZweersMC, Steijlen PM,DeanWB,Taylor G, van Vlijmen IM, van Haren B,Miller WL, Bristow J. 2001. A recessiveform of the Ehlers–Danlos syndrome causedby tenascin-X deficiency. N Engl J Med345:1167–1175.
Schwarze U, Hata R, McKusick VA, Shinkai H,Hoyme HE, Pyeritz RE, Byers PH. 2004.Rare autosomal recessive cardiac valvularform of Ehlers–Danlos syndrome resultsfrom mutations in the COL1A2 gene thatactivate the nonsense-mediated RNA decaypathway. Am J Hum Genet 74:917–930.
Seidler DG, Faiyaz-Ul-Haque M, Hansen U, YipGW, Zaidi SH, Teebi AS, Kiesel L, Gotte M.2006. Defective glycosylation of decorin andbiglycan, altered collagen structure, andabnormal phenotype of the skin fibroblastsof an Ehlers–Danlos syndrome patientcarrying the novel Arg270Cys substitutionin galactosyltransferase I (beta4GalT-7).J Mol Med (Berl) 84:583–594.
Sellars EA, Bosanko KA, Lepard T, Garnica A,Schaefer GB. 2014. A newborn withcomplex skeletal abnormalities, joint con-tractures, and bilateral corneal clouding withsclerocornea. Semin Pediatr Neurol21:84–87.
Shimizu K, Okamoto N, Miyake N, Taira K, SatoY, Matsuda K, Akimaru N, Ohashi H,Wakui K, Fukushima Y, Matsumoto N,Kosho T. 2011. Delineation of dermatan 4-O-sulfotransferase 1 deficient Ehlers-Danlossyndrome: Observation of two additionalpatients and comprehensive review of 20reported patients. Am J Med Genet Part A155A:1949–1958.
Smith LT, Wertelecki W, Milstone LM, Petty EM,Seashore MR, Braverman IM, Jenkins TG,Byers PH. 1992. Human dermatosparaxis: Aform of Ehlers–Danlos syndrome that resultsfrom failure to remove the amino-terminalpropeptide of type I procollagen. Am J HumGenet 51:235–244.
Solomons J, Coucke P, Symoens S, Cohen MC,Pope FM, Wagner BE, Sobey G, Black R,Cilliers D. 2013. Dermatosparaxis (Ehlers-Danlos type VIIC): Prenatal diagnosisfollowing a previous pregnancy with unex-pected skull fractures at delivery. Am J MedGenet Part A 161A:1122–1125.
Sonoda T, Kouno K. 2000. Two brothers withdistal arthrogryposis, peculiar facial appear-ance, cleft palate, short stature, hydroneph-rosis, retentio testis, and normal intelligence:A new type of distal arthrogryposis? Am JMed Genet 91:280–285.
Steinmann B, Gitzelmann R, Vogel A, Grant ME,Harwood R, Sear CH. 1975. Ehlers–Danlossyndrome in two siblings with deficient lysylhydroxylase activity in cultured skin fibro-blasts but only mild hydroxylysine deficit inskin. Helv Paediatr Acta 30:255–274.
Steinmann B, Royce PM, Superti-Furga A. 2002.The Ehlers–Danlos syndrome. New York:Wiley-Liss.
Steinmann B, Tuderman L, Peltonen L, MartinGR, McKusick VA, Prockop DJ. 1980.Evidence for a structural mutation of
procollagen type I in a patient with theEhlers–Danlos syndrome type VII. J BiolChem 255:8887–8893.
Stewart RE, Hollister DW, Rimoin DL. 1977.A new variant of Ehlers–Danlos syndrome:An autosomal dominant disorder of fragileskin, abnormal scarring, and generalizedperiodontitis. Birth Defects Orig Artic Ser13:85–93.
Syx D, Van Damme T, Symoens S, Maiburg MC,van de Laar I, Morton J, Suri M, Del CampoM, Hausser I, Hermanns-Le T, De Paepe A,Malfait F. 2015. Genetic heterogeneity andclinical variability in musculocontracturalEhlers–Danlos syndrome caused by impaireddermatan sulfate biosynthesis. Hum Mutat36:535–547.
Thielens NM, Villiers MB,Reboul A, Villiers CL,Colomb MG. 1982. Human complementsubcomponent C2: Purification and proteo-lytic cleavage in fluid phase by C1s, C1r2-C1s2, and C1. FEBS Lett 141:19–24.
Ticho U, Ivry M, Merin S. 1980. Brittle cornea,blue sclera, and red hair syndrome (thebrittle cornea syndrome). Br J Ophthalmol64:175–177.
Tosun A, Kurtgoz S, Dursun S, Bozkurt G. 2014.A case of Ehlers–Danlos syndrome type VIAwith a novel PLOD1 gene mutation. PediatrNeurol 51:566–569.
Tulika W, Kiran A. 2015. Ehlers-Danlos syn-drome. J Dent Res Rev 2:42–46.
Ulmer M, Li J, Yaspan BL, Ozel AB, Richards JE,Moroi SE, Hawthorne F, Budenz DL,Friedman DS, Gaasterland D, Haines J,Kang JH, Lee R, Lichter P, Liu Y, PasqualeLR, Pericak-Vance M, Realini A, SchumanJS, Singh K, Vollrath D, Weinreb R,Wollstein G, Zack DJ, Zhang K, Young T,Allingham RR, Wiggs JL, Ashley-Koch A,HauserMA. 2012. Genome-wide analysis ofcentral corneal thickness in primary open-angle glaucoma cases in the NEIGHBORand GLAUGEN consortia. Invest Ophthal-mol Vis Sci 53:4468–4474.
Valcourt U, Alcaraz LB, Exposito JY, Lethias C,Bartholin L. 2015. Tenascin-X: Beyond thearchitectural function. Cell Adh Migr9:154–165.
Van Damme T, Colige A, Syx D, Giunta C,Lindert U, Rohrbach M, Aryani O, AlanayY, Simsek-Kiper PO, Kroes HY, DevriendtK, Thiry M, Symoens S, De Paepe A,Malfait F. 2016. Expanding the clinical andmutational spectrum of the Ehlers–Danlossyndrome, dermatosparaxis type. GenetMed 18:882–891.
Vasan NS, Kuivaniemi H, Vogel BE, Minor RR,Wootton JA, Tromp G, Weksberg R,Prockop DJ. 1991. A mutation in the proalpha 2(I) gene (COL1A2) for type Iprocollagen in Ehlers–Danlos syndrometype VII: Evidence suggesting that skippingof exon 6 in RNA splicing may be acommon cause of the phenotype. Am JHumGenet 48:305–317.
Viljoen D, Goldblatt J, Thompson D, Beighton P.1987. Ehlers–Danlos syndrome: Yet anothertype? Clin Genet 32:196–201.
Vitart V, Benci�c G, Hayward C, Skunca Herman J,Huffman J, Campbell S, Bu�can K,Navarro P,Gunjaca G, Marin J, Zgaga L, Kolci�c I,Polasek O, Kirin M, Hastie ND, Wilson JF,Rudan I, Campbell H, Vatavuk Z, Fleck B,
Wright A. 2010. New loci associated withcentral cornea thickness include COL5A1,AKAP13, and AVGR8. Hum Mol Genet19:4304–4311.
Vithana EN, Aung T, Khor CC, Cornes BK, TayWT, Sim X, Lavanya R, Wu R, Zheng Y,Hibberd ML, Chia KS, Seielstad M, GohLK, Saw SM, Tai ES, Wong TY. 2011.Collagen-related genes influence the glau-coma risk factor, central corneal thickness.Hum Mol Genet 20:649–658.
Voermans NC, Altenburg TM, Hamel BC, deHaan A, van Engelen BG. 2007. Reducedquantitative muscle function in tenascin-Xdeficient Ehlers–Danlos patients. Neuro-muscular Disord 17:597–602.
Voermans NC, Bonnemann CG, Lammens M,van Engelen BG, Hamel BC. 2009a.Myopathy and polyneuropathy in an adoles-cent with the kyphoscoliotic type of Ehlers–Danlos syndrome. Am J Med Genet Part A149A:2311–2316.
VoermansNC,Drost G, van Kampen A,Gabreëls-Festen AA, Lammens M, Hamel BC,Schalkwijk J, van Engelen BG. 2006.Recurrent neuropathy associated with Eh-lers–Danlos syndrome. J Neurol253:670–671.
Voermans NC, Kempers M, Lammens M, vanAlfen N, Janssen MC, B€onnemann C, vanEngelen BG, Hamel BC. 2012.Myopathy ina 20-year-old female patient with D4ST-1deficient Ehlers–Danlos syndrome due to ahomozygous CHST14 mutation. Am J MedGenet Part A 158A:850–855.
Voermans NC, van Alfen N, Pillen S, LammensM, Schalkwijk J, Zwarts MJ, van Rooij IA,Hamel BC, van Engelen BG. 2009b.Neuromuscular involvement in varioustypes of Ehlers–Danlos syndrome. AnnNeurol 65:687–697.
Vorster AA, Beighton P, Ramesar RS. 2015.Spondyloepimetaphyseal dysplasiawith jointlaxity (Beighton type); mutation analysis ineight affected South African families. ClinGenet 87:492–495.
Walker LC, Marini JC, Grange DK, Filie J,Yeowell HN. 1999. A patient with Ehlers–Danlos syndrome type VI is homozygous fora premature termination codon in exon 14of the lysyl hydroxylase 1 gene. Mol GenetMetab 67:74–82.
Walker LC, Overstreet MA, Siddiqui A, De PaepeA, Ceylaner G, Malfait F, Symoens S,Atsawasuwan P, Yamauchi M, Ceylaner S,Bank RA, Yeowell HN. 2005. A novelmutation in the lysyl hydroxylase 1 genecauses decreased lysyl hydroxylase activity inan Ehlers–Danlos VIA patient. J InvestDermatol 124:914–918.
Walker LC, Overstreet MA, Willing MC, MariniJC, Cabral WA, Pals G, Bristow J, Atsawa-suwan P, Yamauchi M, Yeowell HN. 2004a.Heterogeneous basis of the type VIB form ofEhlers–Danlos syndrome (EDS VIB) that isunrelated to decreased collagen lysyl hy-droxylation. Am J Med Genet Part A131A:155–162.
Walker LC, Teebi AS, Marini JC, De Paepe A,Malfait F, Atsawasuwan P, Yamauchi M,Yeowell HN. 2004b. Decreased expressionof lysyl hydroxylase 2 (LH2) in skinfibroblasts from three Ehlers–Danlos pa-tients does not result from mutations in

RESEARCH REVIEW AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 115
either the coding or proximal promoterregion of the LH2 gene. Mol Genet Metab83:312–321.
Watanabe Y, Kim HS, Castoro RJ, Chung W,Estecio MR, Kondo K, Guo Y, Ahmed SS,Toyota M, Itoh F, Suk KT, ChoMY, Shen L,Jelinek J, Issa JP. 2009. Sensitive and specificdetection of early gastric cancer with DNAmethylation analysis of gastric washes.Gastroenterology 136:2149–2158.
Watanabe Y, Toyota M, Kondo Y, Suzuki H, ImaiT, Ohe-Toyota M, Maruyama R, NojimaM, Sasaki Y, Sekido Y, Hiratsuka H,Shinomura Y, Imai K, Itoh F, Tokino T.2007. PRDM5 identified as a target ofepigenetic silencing in colorectal and gastriccancer. Clin Cancer Res 13:4786–4794.
Wenstrup RJ, Murad S, Pinnell SR. 1989. Ehlers-Danlos syndrome type VI: Clinical mani-festations of collagen lysyl hydroxylasedeficiency. J Pediatr 115:405–409.
Wertelecki W, Smith LT, Byers P. 1992. Initialobservations of human dermatosparaxis:Ehlers–Danlos syndrome type VIIC.J Pediatr 121:558–564.
Whitaker IS, Rozen WM, Cairns SA, Howes J,Pope FM, Hamish Laing J. 2009. Moleculargenetic and clinical review of Ehlers–DanlosType VIIA: Implications for management bythe plastic surgeon in a multidisciplinarysetting. J Plast Reconstr Aesthet Surg62:589–594.
Winters KA, Jiang Z, Xu W, Li S, AmmousZ, Jayakar P, Wierenga KJ. 2012. Re-assigned diagnosis of D4ST1-deficient Eh-lers–Danlos syndrome (adducted thumb-clubfoot syndrome) after initial diagnosisof Marden–Walker syndrome. Am J MedGenet Part A 158A:2935–2940.
Yasui H, Adachi Y, Minami T, Ishida T, Kato Y,Imai K. 2003. Combination therapy ofDDAVP and conjugated estrogens for arecurrent large subcutaneous hematoma inEhlers–Danlos syndrome. Am J Hematol72:71–72.
Yeowell HN, Allen JD, Walker LC, OverstreetMA, Murad S, Thai SF. 2000a. Deletion ofcysteine 369 in lysyl hydroxylase 1 eliminatesenzyme activity and causes Ehlers–Danlossyndrome type VI. Matrix Biol 19:37–46.
Yeowell HN, Walker LC. 1997. Ehlers–Danlossyndrome type VI results from a nonsensemutation and a splice site-mediated exon-skipping mutation in the lysyl hydroxylasegene. Proc Assoc Am Physicians109:383–396.
Yeowell HN, Walker LC, Farmer B, Heikkinen J,Myllyla R. 2000b. Mutational analysis of thelysyl hydroxylase 1 gene (PLOD) in sixunrelated patients with Ehlers–Danlos syn-drome type VI: Prenatal exclusion of thisdisorder in one family. Hum Mutat 16:90.
Yeowell HN, Walker LC, Neumann LM. 2005.An Ehlers–Danlos syndrome type VIA
patient with cystic malformations of themeninges. Eur J Dermatol 15:353–358.
Yis U, Dirik E, Chambaz C, Steinmann B, GiuntaC. 2008. Differential diagnosis of muscularhypotonia in infants: The kyphoscoliotictype of Ehlers–Danlos syndrome (EDS VI).Neuromuscul Disord 18:210–214.
Zou Y, Zwolanek D, Izu Y, Gandhy S, SchreiberG, Brockmann K, Devoto M, Tian Z, Hu Y,Veit G,MeierM, Stetefeld J, Hicks D, StraubV, Voermans NC, Birk DE, Barton ER,Koch M, Bonnemann CG. 2014. Recessiveand dominant mutations in COL12A1 causea novel EDS/myopathy overlap syndrome inhumans and mice. Hum Mol Genet23:2339–2352.
Zweers MC, Bristow J, Steijlen PM, Dean WB,Hamel BC, Otero M, Kucharekova M,Boezeman JB, Schalkwijk J. 2003. Hap-loinsufficiency of TNXB is associatedwith hypermobility type of Ehlers–Danlossyndrome. Am J Hum Genet 73:214–217.
SUPPORTINGINFORMATION
Additional supporting information maybe found in the online version of thisarticle at the publisher’s web-site.