Embed Size (px)
Citation preview

The Distally Based Sural Artery Flap forAnkle and Foot Coverage
Tahseen A. Cheema, MD,1 Ehab S. Saleh, MD,2 and Alex F. De Carvalho, MD3
The sural artery flap is a distally based fasciocutaneous flap that has many advantages to offer forcoverage in the foot and ankle area. It has the largest arc of rotation of all the regional flaps and does notrequire sacrifice of any major artery, and moderate-to-large-sized defects can be covered adequately.The dissection technique is simple, and donor site morbidity is minimal. We report our experience with17 cases. Age range was from 13 to 56 years. Ten (59%) defects were posttraumatic, 3 (17%) wererelated to reconstructive surgery of the foot or tendon Achilles’, 2 (11%) resulted from tumor resection,and 1 each were from infection and gunshot wound. The smallest flap was 6 � 4 cm and the largest was15 � 12 cm, with the average size being 11 � 7.5 cm. In 5 cases, the donor site was closed primarily,and in other cases, split-thickness skin graft was needed. The short saphenous vein was included in thepedicle in all cases. There was no incidence of complete flap necrosis. Follow-up ranged from 3 to 30months. Two cases (12%) developed partial superficial necrosis. In 1 case, there was partial wounddehiscence that needed debridement and repair. Another case had postoperative discharge, whichsubsided after removal of the calcaneal plate. None of the patients complained of any functional problemrelated to loss of sensation along the lateral border of the foot. The sural island flap is a reliable, safe, andeasy method of providing soft tissue coverage in the area of the foot and ankle. (The Journal of Foot &Ankle Surgery 46(1):40–47, 2007)
Key words: skin coverage, ankle, foot, sural artery flap
Coverage of soft tissue defects of the lower one third ofthe leg and foot remains a challenging yet common recon-structive problem. These areas are easily susceptible totrauma and are sites of numerous trophic problems, likepressure sores and chronic ulcers. Also, the unique weight-bearing requirement adds to the difficulty (1–3). The con-cept of the reconstructive ladder provides a useful algorithmfor consideration of different options for providing skincoverage. Upon climbing this ladder, the surgeon encoun-ters methods ranging from allowing the wound to heal bysecondary intension, direct closure, local flaps, and distalflaps to more sophisticated and complex methods like freetissue transfer (4). It emphasizes the use of simpler methodsfor wound closure whenever possible, with minimal focus
Address correspondence to: Tahseen A. Cheema, MD, Associate Pro-fessor, Department of Orthopaedics, MSC 10 5600, 1 University of NewMexico, Albuquerque, NM 87131-0001 E-mail: [email protected].
1Associate Professor, Department of Orthopaedics, University of NewMexico, Albuquerque, NM.
2Hand Surgery Fellow, Department of Orthopaedics and Rehabilitationat University of New Mexico, Albuquerque, NM.
3Hand Surgery Fellow, Department of Orthopaedics and Rehabilitationat University of New Mexico, Albuquerque, NM.
ACFAS Level of Clinical Evidence: Case series, level IVNo financial support was used for this study, which was approved by the
institutional review board.Copyright © 2007 by the American College of Foot and Ankle Surgeons
1067-2516/07/4601-0007$32.00/0doi:10.1053/j.jfas.2006.10.00140 THE JOURNAL OF FOOT & ANKLE SURGERY
on functional outcome. With a better understanding of anat-omy and vascularity, and improvement of technique andfunctional outcome of many methods on the higher rung ofthe ladder, Gottlieb and Krieger proposed a complimentaryconcept of the reconstructive elevator, which suggestedbypassing steps in the ladder to rise to a higher point if amore complex, reconstructive method offered more advan-tage (5). Among the options of dealing with skin loss aroundthe ankle and the foot, direct closure and skin grafting arenot applicable in many situations. A traditional cross-legflap was a multiple-staged procedure, fraught with manycomplications and an ordeal for the patient. Cutaneous localflaps afford coverage of only smaller wounds. Distallybased musculocutaneous flaps are frequently unreliable.With the development of microsurgery, many excellentcoverage solutions have become available, but they aretime-consuming and require microvascular expertise, whichis not always available. Major anatomic investigations andsystematization of the blood supply of skin have resulted inthe description of several fasciocutaneous flaps, includingthose based on the major vascular territories of the lowerlimb (for example, the anterior tibial artery, posterior tibialartery, and peroneal artery and its perforators) (6, 7). Mas-quelet et al studied the role of the vascular axis that accom-panies sensitive superficial nerves in skin vascularizationand described the concept of neurocutaneous arteries andflaps (8). The distally based superficial sural artery flap is
one of these neurocutaneous flaps, and its circulation de-
pends on anastomosis of perisural vasculature with distalperforators of the peroneal artery near the lateral malleolus.This flap is very useful for soft-tissue coverage in the distalthird of the leg and foot, is easy and fast to execute, andprovides durable coverage of the defect; also, its pedicle isfrequently preserved in most instances of superimposedvascular disorders and trauma (9, 10). Because of its orig-inal description by Masquelet et al, significant experiencehas accumulated to define application, limitations, and as-sociated complications of the reverse-flow sural artery flap(2, 11–14).
The purpose of this article is to report our experience withthis flap in the coverage of cutaneous defects in the foot andankle. This study also explores the safe limits of the largestdimensions of the sural artery flap and the role of the shortsaphenous vein in making this flap more reliable.
Materials and Methods
Seventeen consecutive patients were treated with distallybased superficial sural flaps in our institution from January2003 to June 2005. Institutional approval for this study wasobtained. Eleven patients were men, and 6 were women.The average age of patients was 30 years, ranging from 13to 56 years. In 10 patients, skin defects were posttraumatic,in 3, they were from complications of ankle or foot surgery,and in 2, they were from resection of tumors. One defectwas from a gunshot wound, and 1 resulted from infection.Patients with diabetes and evidence of ischemia, like coldand pulseless feet and thin, shiny skin without hair, wereexcluded. A complication rate 5 to 6 times higher has beenreported in literature for patients with any of these comor-bidities (13). Presence of diabetes with no evidence ofperipheral vascular deficiency was not considered a contra-indication, but patients with diabetic foot ulcers were ex-cluded. Patients with an active infection or osteomyelitiswere also not treated with the sural artery flap, because webelieved this flap would not provide adequate perfusion forsupportive treatment of osteomyelitis and also would not fillthe space after debridement as a muscle flap would. Injuryon the lateral side of ankle in the area of peroneal perfora-tors was also taken as a contraindication for the sural arteryflap. Preoperative evaluation included clinical evaluation ofperipheral pulses and perfusion of skin. Presence of 1 ormore peroneal perforators in the area posterior and proximalto the lateral malleolus was confirmed with Doppler ultra-sound in all cases.
The reconstructed areas were the weight-bearing heel in 4patients, the lateral side of the ankle in 4, the dorsum of thefoot in 3, the Achilles’ tendon area in 3, the lateral aspect ofthe foot in 2, and the anterior aspect of the ankle in 1.
All the flaps were fasciocutaneous, and short saphenous
vein was included in the pedicle in all cases. None of theVOLUME
flaps were delayed or staged in this series. The size variedfrom 6 � 4 cm to 15 � 12 cm. The average size was 11 �7.5 cm. The donor area was covered with a split-thicknessskin graft in 12 patients and was directly closed in theremaining 5 patients. Postoperatively, the foot was elevatedwith the help of an external fixator previously applied forthe primary problem, or pillows if there was no externalfixator in place. If the flap was applied directly on the heel,the arrangement was made to relieve the pressure from theheel. Non–weight-bearing ambulation was permitted on thefifth day if the patient’s general condition and injuriesallowed for it. Weight-bearing was generally determined bythe healing status of other injuries in traumatic cases. Ifthere was no contraindication, protected weight-bearing wasallowed between 4 and 6 weeks. Associated clinical prob-lems included diabetes mellitus in 4 patients, mild periph-eral vascular disease in 2, hepatitis B in 2, and neuropathicfoot in 1.
The average follow-up was 12 months, ranging from 3months to 30 months. All patients were available for thefinal assessment. The patients were evaluated for the pres-ence of flap necrosis, infection, recurrent ulceration, andneuroma at the donor site, loss of sensation along the lateralborder of the foot, ambulatory status, and pain. The clinicaloutcome was considered good, fair, or poor on the followingbasis: good, if the flap healed primarily with no necrosis orcomplication requiring further surgery related to coverage;fair, where partial necrosis or other complications necessi-tated further surgical intervention; poor, where the flap wascompletely lost.
Anatomy of the Superficial Sural Artery
The anatomy of the superficial sural artery and its rela-tionship to the sural nerve have been well studied by severalauthors (8, 15, 16) and will be briefly reviewed here (Fig 1).The sural nerve descends between the 2 heads of the gas-trocnemius and pierces the deep fascia in the middle third ofthe leg. The superficial sural artery arises from the poplitealartery in 65% of the cases, from the medial sural artery in20%, and from the lateral sural artery in 8.3% (15). Then itreaches the sural nerve after 2 to 3 cm and gives off a furtherbranch to the skin that supplies the upper part of the calf,which corresponds to the subfascial course of the nerve andits artery. The artery gives off small branches to the skinonly in the lower two thirds of the leg, corresponding to thesuprafascial course. In 65% of the cases, this artery de-scends to the lateral malleolus, and in 35%, the artery fadesdistally into a vascular network at the distal third of the leg.Regardless of the termination, the artery has a constantdistal anastomosis with septocutaneous perforators from theperoneal artery, which will supply a reverse-flow flap. The
venous drainage of this flap has been a matter of debate.46, NUMBER 1, JANUARY/FEBRUARY 2007 41

Imanishi et al demonstrated that there is a small-calibernetwork of veins alongside the sural nerve that plays animportant role in venous drainage of the flap, thus bypassingthe valves of the small saphenous vein (17).
Surgical Technique
The procedures were performed while patients were un-der general or regional block anesthesia. The patient ispositioned in a lateral decubitus position. Before inflatingthe tourniquet, a sterile Doppler is used to spot the peronealartery perforators at the lateral malleolus. The wound is thendebrided and irrigated. A pattern of the recipient site is usedto determine the dimensions and design of the flap. The flapis designed in the area of the upper and middle thirds ofthe posterior calf, depending on the size of the wound to becovered. Where a large size flap is needed, one third of thediameter of the calf is taken as the extreme limit for thebreadth of the flap. The format of the flap is an ellipse;however, the distal part of the flap is tailored into a teardropconfiguration to facilitate closure of the skin over the pedi-cle without tension (Fig 2, A). The pivot point of the flap isabout 3 to 5 cm above the lateral malleolus, proximal to themost distal perforators from the peroneal artery. The dis-
FIGURE 1 Anatomy of the sural nerve and accompanying super-ficial sural artery. The superficial sural artery takes origin from thepopliteal artery and travels in close approximation of the sural nerve.The sural nerve is subfacial in the proximal third of the calf andbecomes suprafascial in the middle of the calf.
section of the flap is started proximally down to the subfas-
42 THE JOURNAL OF FOOT & ANKLE SURGERY
cial plane. The sural nerve, superficial sural artery, and shortsaphenous vein are included in the flap (Fig 2, B). Thosestructures are ligated proximally to the flap. Once the skin
FIGURE 2 (A) Design of the flap. Addition of the teardrop at thedistal end of the flap helps to cover the pedicle of the flap withouttension at the time of setting it in. (B) Elevation of the fasciocuta-neous flap and preservation of the neurovascular pedicle within theadipofascial sleeve.
and fascia are elevated as a unit, dissection is carried out

distally until the pivot point is reached. This part of thedissection is above the fascia. The pedicle of the flap isabout a 2-cm-wide strip of tissue comprising of fascia andsubcutaneous adipose tissue and containing the sural nervewith its accompanying vessels and short saphenous vein.We do not attempt to individualize the components of thepedicle, which are raised as a unit. A skin incision isopened, thus communicating the area just above the pivotpoint to the proximal aspect of the wound to be covered.The tourniquet is deflated, and the circulation in the flap ischecked. The flap is then transposed distally and sutured tothe receptor site. The opened skin bridge is partially coveredwith the tear-shaped extension of the flap, thus decreasingpressure over the pedicle. The donor area is either primarilyclosed or skin grafted, depending on the dimensions. Awell-padded dressing and splint are applied to keep theankle in the neutral position.
Results
Fifteen (88%) flaps survived completely, and 2 (12%)developed partial necrosis. One of these patients was man-aged successfully with wound care and debridement, andthe other required split-thickness skin graft for wound clo-sure. The necrosis was not related to the size of the flap. Onepatient (6%) developed partial wound dehiscence thathealed after excision of wound margins and repair (Fig 3,A-E). One patient (6%) had drainage that cleared afterremoval of the calcaneal plate.
All patients were able to bear weight on the operatedextremity at follow-up. Thirteen (76%) patients were painfree during activity, and 4 (24%) had mild discomfort thatwas not related to flap coverage. No recurrent ulcerationwas found in either weight-bearing flaps or non–weight-bearing flaps. The patients with flaps over weight-bearingareas were prescribed with orthotics to decrease pressureover the flap during the early period of weight-bearing.Finally, all patients except 2 were able to use regular foot-wear. Two patients used custom-made shoes because ofskeletal problems. All patients were ambulatory on finalassessment, but the ambulatory level was determined byother injuries. None of the patients developed symptomaticneuromas. Loss of sensation along the lateral border of thefoot was universal, but it was not considered functionallyrestrictive by any of the patients. The donor site healedadequately in all patients. One patient who had direct clo-sure of the donor site without skin grafting expressed con-cern about depression at the donor site. At the final assess-ment, 13 (76%) patients were rated as good and 4 (24%) as
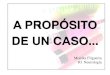
fair. The data are summarized in Table 1.VOLUME
Discussion
Great progress has been made in concepts of skin cover-age during the last 4 decades. With the work of Ian McGre-gor, a new era of understanding of blood supply of the skinwas initiated, and many axial pattern flaps were identified(18). Combined with the advent of microsurgery, this ledthe way for free vascularized flaps, which became the stan-dard tool in the hands of reconstructive surgeons. Thisimproved the whole field of skin coverage tremendously,but significant limitations included lengthy and technicallydemanding procedures, a need for special training in micro-surgery, and a risk of failure of vascular anastomosis. Pon-ten identified fasciocutaneous perforators of peripheral ar-teries and their cutaneous territories, which became thebasis for fasciocutaneous flaps in the extremities (6). Thatmade many nonmicrosurgical flaps feasible around the dif-ficult areas of the distal leg and the ankle. Most of theseflaps had a short arc of rotation, thus limiting their applica-tion in the ankle and the foot. Masquelet et al studied therole of arteries accompanying the superficial sensory nervesin skin vascularization and identified flaps based on vascularaxes of the saphenous nerve, the superficial peroneal nerve,and the sural nerve (8). Because of its long arc of rotation,ease of dissection, and reliable blood supply, the sural arteryflap was rapidly accepted as an important option for skincoverage of the distal leg, ankle, and foot, and many clinicalseries appeared in the literature further defining limitationsand advantages of this flap (9, 11–14, 19–21).
Inclusion of the short saphenous vein in the flap not onlyimproves the venous outflow, but also improves the circu-lation of the flap and allows cranial extension of the flapover the proximal third of the calf. Nakajima et al describedaccompanying arteries of the short saphenous vein and suralnerve that give venocutaneous and neurocutaneous perfora-tors that nourish the skin from the calf down to the ankle(16). Neurocutaneous perforators from the accompanyingartery of the sural nerve are the dominant source of bloodsupply in this flap when the flap is raised from the distal halfof the leg. At the level of the proximal third of the calf, thesural nerve becomes infrafascial, but the short saphenousvein remains suprafascial and venocutaneous perforatorsfrom its accompanying artery significantly contribute to thecutaneous circulation. These findings have been confirmedby other authors also (22). Based on this concept, Nakajimaet al have raised flaps based on only the circulation from theaccompanying artery of the short saphenous vein, thus pre-serving the sural nerve and the sensation along the lateralborder of the foot. We have not attempted that because weconsider adequate blood supply and survival of the flapmore important, and the loss of sensation along the lateralborder of the foot has not been a significant clinical problemin our patients. We have included the short saphenous vein
in all our flaps, thus allowing us to raise some flaps from the46, NUMBER 1, JANUARY/FEBRUARY 2007 43

proximal third of the calf. One third of the diameter of thecalf has proved to be a safe limit of the breadth of the flapin this group of patients.
FIGURE 3 (A) Skin defect in a 42-year-old male patient after exadipofascial pedicle containing the sural nerve, superficial sural arteartery flap, and the donor site was skin grafted. (D) The patient devewound margins and repair.
The venous drainage of reverse fasciocutaneous flaps has
44 THE JOURNAL OF FOOT & ANKLE SURGERY
been vigorously debated in the literature (17, 23–25). Re-verse venous outflow is established as the valves are by-passed by communicating and collateral branches of venae
of the synovial sarcoma. (B) The sural artery flap is raised withd short saphenous vein. (C) The defect was covered with the sural
d partial wound dehiscence. (E) The wound healed after revision of
cisionry, anlope
comitantes. This is also aided by denervation of venae
comitantes during the process of raising the flap and thebuild-up of pressure in the veins, which make the valvesincompetent (25). The small, long veins that run along thelesser saphenous vein and are considered to be venae co-mitantes of the accompanying artery of the lesser saphenousvein are other channels for venous drainage. Although thereis adequate venous flow in most of the cases, occasionallyvenous congestion may be a problem. This might havecontributed to partial necrosis in 2 of our flaps. Comorbidi-ties like diabetes mellitus, peripheral vascular disease, orvenous insufficiency have been recognized as risk factors byBaumeister et al, which increases risk of flap necrosis 5 to6 times (13). Although none of these conditions is anabsolute contraindication, we have avoided using the suralartery flap in diabetic patients with peripheral vasculardisease or venous insufficiency, thus avoiding high-risksituations. If no suitable alternate solution is available inthese situations, then one should consider modification ofthe technique to enhance the vascularity of the sural arteryflap. Al-Qattan has described a gastrocnemius muscle cufftechnique that improves the survival rate of this flap even inpatients with diabetes (26). Recently, a sural artery delayprocedure has been advocated in patients with risk factors
TABLE 1 Summary of patients’ data
Patient Age Gender Mechanism of Skin Loss Defect Site F
1 45 Male Resection of synovioma Heel
2 25 Male Trauma TendonAchilles’
3 28 Male Trauma Lateral side ofthe ankle
4 42 Male Trauma Heel5 56 Female Resection of melanoma Heel6 14 Female Trauma Heel7 39 Male Trauma Lateral side of
the ankle8 40 Female Breakdown of skin after
plating of calcaneumLateral side of
the ankle
9 21 Male Trauma Lateral side ofthe foot
10 22 Male Trauma Dorsal side ofthe foot
11 14 Female Triple arthrodesis in a severeplanovalgus foot
Lateral side ofthe foot
12 25 Male Trauma Heel andtendonAchilles’
13 38 Female Skin necrosis after repair oftendon Achilles’
TendonAchilles’
14 18 Male Trauma Dorsal side ofthe foot
15 15 Male Gunshot wound Anterior side ofthe ankle
16 52 Male Infection Lateral side ofthe ankle
17 13 Female Trauma Dorsal side ofthe foot
such as age over 40 years, peripheral vascular disease,
VOLUME
venous insufficiency, and diabetes (27, 28). One of ourpatients with partial necrosis had diabetes without any ev-idence of peripheral vascular insufficiency, and, in otherpatient, no particular cause or risk factor could be identified.In the present study, most of the patients’ injuries weretrauma related and had minimal risk factors. Avoiding theuse of this flap in patients with multiple risk factors helps toimprove the success rate.
Jeng et al have described a sensate version of the suralisland flap by inclusion of the lateral sural nerve and coapt-ing it to recipient nerves (20). This provided protectivesensation in 4 of their cases. We have not found it necessarybecause all of our patients who had weight-bearing areas oftheir feet covered with this flap were able to manage withproper shoe fitting and instructions about the care of theirfeet. None of them developed trophic ulcers and, with time,developed some pressure sensation from deep structures.
Compared with other fasciocutaneous flaps that are usedto cover the ankle and foot region, the sural artery flap hasmany advantages. The medial plantar flap provides sensatevolar skin and can be used advantageously for the weight-bearing areas of the heel, but extent of the skin available israther limited and is technically more tedious and time-
ize (cm) Comorbidities Complications Outcome
� 8 None Partial wounddehiscence
Fair
� 7 Hepatitis B Good
� 6 None Good
12 None Good7 Diabetes Good10 Good5 Loss of hair and skin
discolorationGood
4 Diabetes Drainage that subsidedafter removal ofcalcaneal plate
Fair
9 Good
11 Good
4 Diabetes Good
7 Partial necrosis Fair
7 Diabetes Partial necrosis Fair
8 Good
6 Good
5 Peripheral vascular disease;neuropathic foot
Good
12 Good
lap S
11
12
13
15 �8 �
13 �6 �
7 �
12 �
15 �
6 �
12 �
11 �
12 �
10 �
10 �
15 �
consuming (29). The lateral supramalleolar flap, which of-
46, NUMBER 1, JANUARY/FEBRUARY 2007 45

fers a range of coverage similar to that of the sural arteryflap, is also more difficult to perform and has a much higherrate of failure (3).
Conclusion
Although this study is limited by a relatively small num-ber of patients and the absence of a comparison group, weconclude that the sural artery reverse-flow flap provides aneasy and reliable method of skin coverage in the region ofthe foot and the ankle. The success rate in this study (88%complete survival) is comparable with other series in theliterature (2, 3, 11, 14, 30). There is minimal risk of failurebecause of the reliable source of blood supply. One third ofthe calf seems to be the safe limit of breadth of the flap, andwith inclusion of the short saphenous vein, the territory ofthe flap can be extended to the proximal third of the calf. It
FIGURE 4 (A) 26-year-old patient with posttraumatic skin lossover the heel. (B) This large area of skin loss was covered with asural artery flap measuring 15 � 12 cm.
allows coverage of extensive defects in a traditionally dif-
46 THE JOURNAL OF FOOT & ANKLE SURGERY
ficult area and has limited aesthetic and functional sequalae(Fig 4, A-B). In patients with multiple risk factors likeperipheral arterial disease, venous insufficiency, and diabe-tes, one should consider alternate solutions.
References
1. Jeng SF, Wei FC, Kuo YR. Salvage of the distal foot using the distallybased sural island flap. Ann Plast Surg 43:499–505, 1999.
2. Fraccalvieri M, Verna G, Dolcet M, Fava R, Rivarossa A, Robotti E,Bruschi S. The distally based superficial sural flap: our experience inreconstructing the lower leg and foot. Ann Plast Surg 45:132–139, 2000.
3. Touam C, Rostoucher P, Bhatia A, Oberlin C. Comparative study oftwo series of distally based fasciocutaneous flaps for coverage of thelower one-fourth of the leg, the ankle, and the foot. Plast Reconstr Surg107:383–392, 2001.
4. Mathes SJ, Nahai F. Reconstructive Surgery: Principles, Anatomy, andTechnique, London, Churchill Livingstone, 1997.
5. Gottlieb LJ, Krieger LM. From the reconstructive ladder to the recon-structive elevator. Plast Reconstr Surg 93:1503–1504, 1994.
6. Ponten B. The fasciocutaneous flap: its use in soft tissue defects of thelower leg. Br J Plast Surg 34:215–220, 1981.
7. Taylor GI, Pan WR. Angiosomes of the leg: anatomic study andclinical implications. Plast Reconstr Surg 102:599–616; discussion617–618, 1998.
8. Masquelet AC, Romana MC, Wolf G. Skin island flaps supplied by thevascular axis of the sensitive superficial nerves: anatomic study andclinical experience in the leg. Plast Reconstr Surg 89:1115–1121,1992.
9. Costa-Ferreira A, Reis J, Pinho C, Martins A, Amarante J. The distallybased island superficial sural artery flap: clinical experience with 36flaps. Ann Plast Surg 46:308–313, 2001.
10. Isenberg JS. When less is more: revascularization and sural arteryfasciocutaneous flaps in ischemic limb salvage. J Reconstr Microsurg19:235–240, 2003.
11. Hasegawa M, Torii S, Katoh H, Esaki S. The distally based superficialsural artery flap. Plast Reconstr Surg 93:1012–1020, 1994.
12. Jeng SF, Hsieh CH, Kuo YR, Lin TS, Wei FC. Distally based suralisland flap. Plast Reconstr Surg 111:840–841, 2003.
13. Baumeister SP, Spierer R, Erdmann D, Sweis R, Levin LS, GermannGK. A realistic complication analysis of 70 sural artery flaps in amultimorbid patient group. Plast Reconstr Surg 112:129–140; discus-sion 141–142, 2003.
14. Rajacic N, Darweesh M, Jayakrishnan K, Gang RK, Jojic S. Thedistally based superficial sural flap for reconstruction of the lower legand foot. Br J Plast Surg 49:383–389, 1996.
15. Fachinelli A, Masquelet A, Restrepo J, Gilbert A. The vascularized suralnerve: anatomy and surgical approach. Int J Microsurgery 3:57, 1981.
16. Nakajima H, Imanishi N, Fukuzumi S, Minabe T, Fukui Y, MiyasakaT, Kodama T, Aiso S, Fujino T. Accompanying arteries of the lessersaphenous vein and sural nerve: anatomic study and its clinical appli-cations. Plast Reconstr Surg 103:104–120, 1999.
17. Imanishi N, Nakajima H, Fukuzumi S, Aiso S. Venous drainage of thedistally based lesser saphenous sural veno-neuroadipofascial pedicledfasciocutaneous flap: a radiographic perfusion study. Plast ReconstrSurg 103:494–498, 1999.
18. Smith PJ, Foley B, McGregor IA, Jackson IT. The anatomical basis ofthe groin flap. Plast Reconstr Surg 49:41–47, 1972.
19. Raveendran SS, Perera D, Happuharachchi T, Yoganathan V. Super-ficial sural artery flap—a study in 40 cases. Br J Plast Surg 57:266–269, 2004.
20. Jeng SF, Wei FC. Distally based sural island flap for foot and ankle
reconstruction. Plast Reconstr Surg 99:744–750, 1997.
21. Singh S, Naasan A. Use of distally based superficial sural island arteryflaps in acute open fractures of the lower leg. Ann Plast Surg 47:505–510, 2001.
22. Rajendra Prasad JS, Cunha-Gomes D, Chaudhari C, Bhathena HM,Desai S, Kavarana NM. The venoneuroadipofascial pedicled distallybased sural island myofasciocutaneous and muscle flaps: anatomicalbasis of a new concept. Br J Plast Surg 55:203–209, 2002.
23. Al-Qattan MM. A modified technique for harvesting the reverse suralartery flap from the upper part of the leg: inclusion of a gastrocnemiusmuscle “cuff” around the sural pedicle. Ann Plast Surg 47:269–274,discussion 274–278, 2001.
24. Lin SD LC, Cin CC. Venous drainage in the reverse forearm flap. PlastReconstr Surg 74:508–512, 1984.
25. Timmons M. The vascular basis of the radial forearm flap. Plast
Reconstr Surg 77:80–92, 1986.VOLUME
26. Al-Qattan MM. Lower-limb reconstruction utilizing the reverse suralartery flap-gastrocnemius muscle cuff technique. Ann Plast Surg 55:174–178, 2005.
27. Erdmann D, Gottlieb N, Humphrey JS, Le TC, Bruno W, Levin LS.Sural flap delay procedure: a preliminary report. Ann Plast Surg54:562–565, 2005.
28. Tosun Z, Ozkan A, Karacor Z, Savaci N. Delaying the reverse suralflap provides predictable results for complicated wounds in diabeticfoot. Ann Plast Surg 55:169–173, 2005.
29. Rashid M, Hussain SS, Aslam R, Illahi I. A comparison of twofasciocutaneous flaps in the reconstruction of defects of the weight-bearing heel. J Coll Physicians Surg Pak 13:216–218, 2003.
30. Yilmaz M, Karatas O, Barutcu A. The distally based superficial suralartery island flap: clinical experiences and modifications. Plast Recon-
str Surg 102:2358–2367, 1998.46, NUMBER 1, JANUARY/FEBRUARY 2007 47

![Hyperbaric oxygen therapy and surgical delay …the dorsum of the foot, the medial and lateral arches, and all regions of the heel. The reverse sural flap [3,4] is raised from the](https://img.dokumen.tips/doc/110x75/5f7b32540d8f777e9871b889/hyperbaric-oxygen-therapy-and-surgical-delay-the-dorsum-of-the-foot-the-medial.jpg)