Embed Size (px)
Citation preview

Susceptibility to Multiple Air Pollutants in Cardiovascular Disease
Substantial research links ambient air pollution to cardiovascular disease (CVD), theleading cause of death in the US (Brook et al 2009; Kaufman et al 2016), potentially withstronger impacts in lower-socioeconomic position (SEP) communities (Clark et al 2014;
Krewski et al, 2003) The causal factors underlying this susceptibility, however, have notbeen identified (US EPA 2008; Matthews & Gallo 2011).
Evidence suggests that susceptibility by SEP may be mediated, in part, by chronicstressors (e.g., violence, job insecurity) (Clougherty et al 2014; Shankardass et al 2009) -
interactions particularly relevant to CVD (Hicken et al 2014), as both are linked toinflammation, metabolic function, oxidative stress, hypertension, and atherosclerosis(Everson-Rose 2014; Kubzansky et al 2007). Elucidating these susceptibilities will help toidentify susceptible populations, better target interventions, and strengthen cost-benefit and accountability analyses. We hypothesize that:
(1) Combined exposures to multiple pollutants and chronic SEP/ stressor exposuresshape community CVD event rates.
(2) Associations between spatio-temporal variation in multiple pollutants and CVDrisk will be greater in communities of lower SEP and/ or higher stressor exposures.
Jane E. Clougherty1, Jamie L. Humphrey1, Laura D. Kubzansky2, Colleen Reid3, Ellen Kinnee4, Lucy Robinson1, Leslie McClure1, David Q. Rich5, Fernando Holguin6
1 Drexel University Dornsife School of Public Health, Philadelphia PA, 2Harvard T.H. Chan School of Public Health, Boston MA, 3University of Colorado at Boulder, 4 University of Pittsburgh Graduate School of Public Health; 5University of Rochester School of Medicine and Dentistry, 6 University of Colorado at Denver School of Medicine
We will quantify relationships among chronic stressors and multiple pollutants inNYC, and test whether pollutant-CVD relationships vary by SEP/ stressor exposures.
Aim 1: In ecologic cross-sectional analyses, test whether exposures to annual-average chronic stressor rates and annual-average pollutant exposures, separatelyand together, predict community age-adjusted CVD event rates.
Aim 2: Use case-crossover models to quantify associations between CVD events andday- and residence-specific exposures to PM2.5, NO2, and O3, across 0 - 6 lag days.
Aim 3: Examine whether SEP/ stressors exacerbate pollution effects on CVD, usingindicators of community SEP/ stressor exposures in case-crossover models.
Anselin L. Exploring Spatial Data with GeoDa. Urbana-Champaign, IL: Center for Spatially Integrated Social Science; 2005.Brook, R.D., et al. Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans.Hypertension 2009. 54(3):659-67.Clougherty JE, et al. Intra-urban spatial variability in wintertime street-level concentrations of multiple combustion-related air pollutants. JESEE. 2013. 23(3):232-40.Clougherty JE, et al. The role of non-chemical stressors in mediating socioeconomic susceptibility to environmental chemicals. Curr Env H Reports. 2014: 1(4): 302-13.Everson-Rose SA, et al. Chronic stress, depressive symptoms, anger, hostility, and risk of stroke and transient ischemic attack in the multi-ethnic study ofatherosclerosis. Stroke 2014: 45(8): 2318-23Hicken MT, et al. 2014. Fine particulate matter air pollution and blood pressure: the modifying role of psychosocial stress. Environ Res, 133, 195-203.Kaufman JD, et al. 2016. Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the Multi-Ethnic Study ofAtherosclerosis and Air Pollution): a longitudinal cohort study. Lancet.Kubzansky LD, et al. Prospective Study of Posttraumatic Stress Disorder Symptoms and Coronary Heart Disease in the Normative Aging Study. 2007. Arch GenPsychiatry. 2007a;64(1):109-116.Matte T, et al. Monitoring intra-urban spatial patterns of multiple combustion air pollutants in New York City: Design and Implementation. J Expos Sci EnvironEpidemiol. 2013 23(3):223-31.Messer LC, et al. Effects of socioeconomic and racial residential segregation on preterm birth: a cautionary tale of structural confounding. Am J Epidemiol2010;171:664–73.Ross Z, et al. Spatial and temporal interpolation of air pollutants in New York City: exposure assignment for use in a birth outcomes study. Environmental Health.2013; 12 (51).Shankardass K, et al. 2009. Parental stress increases the effect of traffic-related air pollution on childhood asthma incidence. Proc Natl Acad Sci 106(30):12406-11.Shmool JL, et al. Area-level socioeconomic deprivation, nitrogen dioxide exposure, and term birth weight in New York City. Environ Res 2015; 142: 624-632.
Preliminary Results
Specific Aims
Introduction and Background
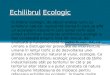
Figure 1: Socioeconomic Deprivation Index
References
Methods: Datasets Cont’d
Methods: Datasets
(1) Hospital CVD data: Data on all in- and out-patient unscheduled cardiovascularevents (ICD-9 codes 390-459) at NYC hospitals 2005-11 (n = 1,136,838) from NYState Dept. of Health Statewide Planning and Research Cooperative System(SPARCS). We use "emergent" and “urgent” admissions, indicating acute events.
(2) Citywide air pollution data: The NYC Community Air Survey (NYCCAS) wasestablished by NYC Dept. of Health & Mental Hygiene (DOHMH) to inform policyand air quality initiatives. Monitoring was performed year-round at 155 sitescitywide for two years (Matte et al 2013). Land Use Regression was used to modelspatial variation in fine particles (PM2.5), nitrogen dioxide (NO2), sulfur dioxide(SO2), and summer ozone (O3) (Clougherty et al 2013).
(3) Daily EPA data: We use daily averages from all NYC Air Quality System (AQS)stations for 2005-11. We examined data completeness, imputed missing values,and averaged daily values into one citywide trend (Sheffield et al., 2015), which wecombine with NYCCAS surfaces to create day- and residence-specific ‘spatio-temporal’ estimates (Ross et al 2013; Shmool et al 2015).
(4) GIS-based area-level susceptibility indicators: We examine effects of community-level susceptibility using 3 types of SEP/ stressor indicators:
4a) Key stressors: Community assault rate, percent of households < 200% ofpoverty level: Using focus groups and surveys to ‘validate’ stressors, these twomost strongly predicted perceived disorder and mental health (perceived stress,anxiety, depression), and thus are examined individually.
4b) Socioeconomic deprivation index (SDI): Wecaptured material deprivation using spatially-stratifiedprincipal components analysis (PCA) (Messer et al2006) on 20 indicators [education, employment,occupation, housing, poverty, racial/ethniccomposition) from American Communities Survey(ACS) 2005-09, at census tract, retaining all variablesloading > |0.4| in 2+ boroughs. The final SDI of 7variables explained 56% of variance. (Figure 1).
Methods: Analysis
Aim 1: Because social stressor data is aggregated to community annual means, weconducted ecologic cross-sectional analyses to compare associations for pollution andstressors against age-adjusted annual-mean community CVD rates [ICD-9 codes 390-459,and key diagnoses (i.e., acute myocardial infarction, heart failure). We tested modificationby median-dichotomized stressors using OLS Regression. In sensitivity analyses, weadjusted for autocorrelation using Simultaneous Autoregression (SAR) with severalweights matrices, and Moran’s I to test autocorrelation in OLS residuals (Anselin 2005).
Aim 2: We are testing daily PM2.5, NO2, SO2, and O3 vs. 1,136,838 CVD events usingconditional logistic regression in case-crossover, with time-stratified referent sampling tocontrol for day of week and time-invariant confounders (e.g., age, race), adjusting fortemperature, relative humidity, and co-pollutants. We are estimating risks per 10-unitpollutant increase on lag days 0-6 with Bonferroni adjustment for multiple comparisons.
Aim 3: We will test modification in associations between spatio-temporal exposures andrisk of CVD event, using the models described above, in interaction with categoricalstressor modifiers and Bonferroni adjustment for multiple comparisons.
4c) Factors of spatially-correlated stressors: We used unconstrained factor analysis, withand without spatial autocorrelation adjustment, to examine 27 stressor indicators fromadministrative data in 6 categories [crime & violence, physical disorder, healthcare access,noise disruption, school-related stressors, SEP indicators]. We required citywide coverage,conceptual comparability with validated measures in our citywide stress survey, andexcluded indicators with substantial under-reporting/ reporting bias (e.g., felony rape)(Shmool et al 2014). The factors identified were characterized by: (1) crime and violence,(2) housing violations and material deprivation, (3) noise, air pollution complaints.
Table 1: Preliminary case-crossover (conditional logistic regression) results for associations between daily PM2.5, NO2, SO2, and O3 vs. 1,136,838 CVD events (expect O3, summer-only) across lag days 0-6.
Ecologic Analysis: To compare associations with CVD for social stressors and pollutants,we used mutually-adjusted OLS models of community (n=34 UHF areas) annual meanpollutant concentrations and social stressors vs. annual-mean age-adjusted in-patientCVD events. All estimates were scaled to a 1-IQR unit change in stressor prevalence orpollutant concentration.
In cross-sectional ecologic models, all social stressors except Factor 3 (‘noise/ air pollutioncomplaints’) were significantly associated with CVD risk. Associations between stressorsand annual-mean CVD rates were substantially stronger than for PM2.5, NO2, SO2, and O3.
We found some evidence of effect modification; associations between SO2 and CVD weresomewhat modified by Factor 2. We are, however, underpowered to detect effectmodification in Aim 1, due to the small sample size (n = 34) of the ecologic analysis.
Case-crossover analysis: In preliminary case-crossover models, we found moderateassociations between some pollutants (i.e., PM2.5, NO2, SO2) and a subset of CVDoutcomes (i.e., all CVD, heart failure, IHD).
Items for Discussion
Next Steps: (1) Examine effect modification by the social stressors [3 spatially-correlatedstressors, SDI, Poverty, Assault] in case-crossover models. (2) Adjust for co-pollutants. (3)Examine sensitivity to alternative missing data correction in AQS time-series.
Referent sampling method. Using time-stratified referent sampling with 6 lag days, we lose~225,000 cases (first days of each month). Would we benefit from symmetric bi-directionalreferent sampling?
Key diagnoses. We selected seven key diagnoses from the literature. To reduce multiple-comparison problems, would it be prudent to drop some diagnoses (and, if so, which?)?
Future Directions: Examine effect modification by: (1) noise [perceived and objective], (2) co-morbid conditions (e.g., diabetes), (3) spatially- and temporally-refined violence exposures.
Figure 2: Percent excess risk of emergency department event for CVD, heart failure, or ischemic heart disease (IHD), per 10-unit increase in PM2.5, NO2, SO2, or summer O3.
Preliminary Results
Legend: ‘+’ indicates positive association, ‘-’ negative association, ‘ns’ no association. Shading indicates statistical significance after Bonferroni correction.