Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Reverse pedicle-based greater saphenous neuro-veno-fasciocutaneous flap for reconstruction of lower leg and foot
Sandeep Kansal • Pradeep Goil • Vijay Agarwal •
Swarnima Agarwal • Shashank Mishra •
Deepak Agarwal • Pranay Singh
Received: 7 June 2012 / Accepted: 8 December 2012
� Springer-Verlag France 2013
Abstract
Introduction Paucity of soft tissue available locally for
reconstruction of defects in leg and foot presents a chal-
lenge for reconstructive surgeon. The use of reverse pedi-
cle-based greater saphenous neuro-veno-fasciocutaneous
flap in reconstruction of lower leg and foot presents a viable
alternative to free flap and cross-leg flap reconstruction. The
vascular axis of the flap is formed by the vessels accom-
panying the saphenous nerve and the greater saphenous
vein. We present here our experience with reverse saphe-
nous neurocutaneous flap which provides a stable cover
without the need to sacrifice any important vessel of leg.
Patients and methods The study is conducted from March
2003 through Dec 2009 and included a total of 96 patients
with defects in lower two-thirds of leg and foot. There are
74 males and 22 females. Distal pivot point was kept
approximately 5–6 cm from tip of medial malleolus, thus
preserving the distal most perforator, and the flap is turned
and inserted into the defect. Donor site is covered with a
split thickness skin graft. Postoperative follow-up period
was 6 weeks to 6 months.
Result The procedure is uneventful in 77 cases. Infection
is observed in 14 cases. Partial flap necrosis occurs in 2
cases. Total flap necrosis is noted in 3 cases.
Conclusion Reverse pedicle saphenous flap can be used
to reconstruct defects of lower one-third leg and foot with a
reliable blood supply with a large arc of rotation while
having minimal donor site morbidity.
Keywords Lower leg � Foot � Reverse saphenous flap �Great saphenous vein � Saphenous nerve
Introduction
Paucity of soft tissue available locally for reconstruction
of defects in leg and foot presents a challenge for recon-
structive surgeon. Reconstruction with free flap provides
healthy tissue for reconstruction, but many a times leads to
sacrifice of one of the major vessels of leg. Similarly,
peroneal flap [1], posterior tibial artery flap [2] and ante-
rior tibial artery flap [3] also lead to sacrifice of a vessel.
The use of reverse pedicle-based greater saphenous neuro-
veno-fasciocutaneous flap in reconstruction of lower leg
and foot presents a viable alternative to free flap and
cross-leg flap. The vascular axis of the flap is formed by
the vessels accompanying the saphenous nerve and the
greater saphenous vein. The flap can be raised up to the
knee, has minimal morbidity and can reach up to the distal
part of foot. We present here our experience with reverse
saphenous neurocutaneous flap which provides a stable
cover without the need to sacrifice any important vessel
of leg.
Patients and methods
The study was conducted from March 2003 through Dec
2009 in our hospital and included a total of 96 patients with
defects in lower two-thirds of leg and foot. There were 74
males and 22 females. Injury due to road traffic accident
was the main aetiology of the defect. Patients with defect
encroaching upon the territory of the saphenous nerve, vein
and the medial malleolus were excluded.
S. Kansal (&) � P. Goil � V. Agarwal � S. Agarwal �S. Mishra � D. Agarwal � P. Singh
A-27, Alok Park, Modinagar 201204, Ghaziabad, UP, India
e-mail: [email protected]
123
Eur J Orthop Surg Traumatol
DOI 10.1007/s00590-012-1150-5
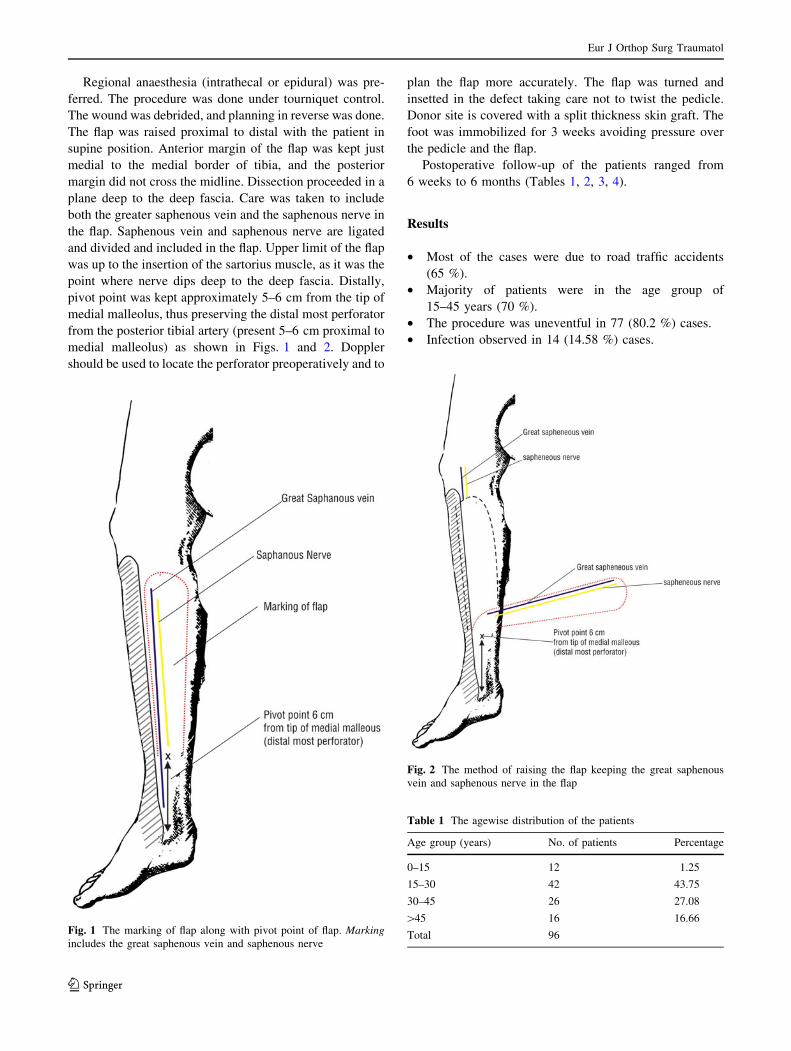
Regional anaesthesia (intrathecal or epidural) was pre-
ferred. The procedure was done under tourniquet control.
The wound was debrided, and planning in reverse was done.
The flap was raised proximal to distal with the patient in
supine position. Anterior margin of the flap was kept just
medial to the medial border of tibia, and the posterior
margin did not cross the midline. Dissection proceeded in a
plane deep to the deep fascia. Care was taken to include
both the greater saphenous vein and the saphenous nerve in
the flap. Saphenous vein and saphenous nerve are ligated
and divided and included in the flap. Upper limit of the flap
was up to the insertion of the sartorius muscle, as it was the
point where nerve dips deep to the deep fascia. Distally,
pivot point was kept approximately 5–6 cm from the tip of
medial malleolus, thus preserving the distal most perforator
from the posterior tibial artery (present 5–6 cm proximal to
medial malleolus) as shown in Figs. 1 and 2. Doppler
should be used to locate the perforator preoperatively and to
plan the flap more accurately. The flap was turned and
insetted in the defect taking care not to twist the pedicle.
Donor site is covered with a split thickness skin graft. The
foot was immobilized for 3 weeks avoiding pressure over
the pedicle and the flap.
Postoperative follow-up of the patients ranged from
6 weeks to 6 months (Tables 1, 2, 3, 4).
Results
• Most of the cases were due to road traffic accidents
(65 %).
• Majority of patients were in the age group of
15–45 years (70 %).
• The procedure was uneventful in 77 (80.2 %) cases.
• Infection observed in 14 (14.58 %) cases.
Fig. 1 The marking of flap along with pivot point of flap. Markingincludes the great saphenous vein and saphenous nerve
Table 1 The agewise distribution of the patients
Age group (years) No. of patients Percentage
0–15 12 1.25
15–30 42 43.75
30–45 26 27.08
[45 16 16.66
Total 96
Fig. 2 The method of raising the flap keeping the great saphenous
vein and saphenous nerve in the flap
Eur J Orthop Surg Traumatol
123

• Partial flap necrosis occurs in 2 (2.1 %) cases, with
resulting need for complimentary minor surgery
(debridement and split thickness graft).
• Total flap necrosis noted in 3 (3.1 %) cases.
Discussion
Soft tissue defects of lower one-third tibia and foot used to
be enigma of orthopaedic and even plastic and recon-
structive surgeon. Trauma due to road traffic accidents
account for most of the cases. Various techniques have
been developed for the reconstruction of these defects.
Split skin graft remains the best option to cover superficial
defects over dorsum of foot due to its faster take and early
neurotization.
The coverage of wounds of the lower third of the leg is
usually best treated using microvascular free-tissue trans-
fer. These flaps provide reliable single-stage coverage of
these wounds. There are certain disadvantages of free flaps.
These are the need for a remote donor site, increased
operative time, use of a major vessel of the leg and the need
for micro vascular expertise (Figs. 3, 4, 5, 6, 7, 8, 9, 10).
Inferiorly based muscle flaps continue to be plagued by
a high failure rate [3]. The donor defect and bulk and
morbidity also added the disadvantage of this flap [4].
Fasciocutaneous flaps first introduced by Ponten in 1981
[5, 6] are in the use for the reconstruction of soft tissue
defects of lower one-third leg and foot. Reversed island
flap, for example, peroneal artery flap [1], anterior tibial
artery flap [7–9] and posterior tibial artery flap can be
transferred to the ankle or foot [2]. However, it needs
sacrifice of a major artery which constitutes a potentially
serious disadvantage. Masquelet et al. [10] in 1992 first
described distally based sural artery flap based on vascular
plexus around the sural nerve.
Saphenous nerve is the largest branch of the femoral
nerve and enters the leg between sartorius and tendon of
Fig. 3 Pre-operative photograph of patient 1 showing defect over
anteromedial aspect of foot
Fig. 4 Pre-operative photograph of patient 1 showing incision of the
marked reverse saphenous flap
Table 2 Aetiology of patients
Aetiology No. of patients Percentage
RTA 62 64.58
Nonhealing ulcer 12 12.5
Unstable area 13 13.54
Others (exposed pin, plates, etc.) 9 9.4
Table 3 The site of defect
Site of defect No. of patients Percentage
Ankle 21 21.9
Lower one-third leg 42 43.75
Foot 27 28.1
Heel 6 6.25
Table 4 The postop. results in study group
Postop. result No. of patients Percentage (%)
Uneventful 77 80.2
Discharge/infection 14 14.58
Partial flap necrosis 2 2.1
Total flap necrosis 3 3.1
Eur J Orthop Surg Traumatol
123

gracilis. It remains deep to the deep fascia proximally and
become suprafascial distal to insertion of sartorius muscle.
It accompanies the great saphenous vein in the leg and foot
and ends in the skin of medial side of leg. According to
Masquelet et al. [10], a rich network of vessels is formed
around the nerve by the saphenous artery. Distally this
plexus has numerous anastomoses with perforators from
posterior tibial artery. The distal most of these anastomoses
is 5–6 cm proximal to medial malleolus.
The hemodynamic role of the large subcutaneous veins
in distally based flaps has been extensively discussed.
Timmons [11] suggested that flow could be reversed
against the denerved valves to drain the flaps. Torri et al.
[12] reported that the valves of the greater saphenous vein
become independent only with venous pressures of more
than 90 mmHg; therefore, it seems very unlikely that flow
reversal could occur in clinical situation. Imanshi et al. [13]
suggested that superficial vein included in the flap usually
get thrombosed in postoperative period. Chang [14]
observed that, when the large veins draining from the limb
were included in a reversed flap, they became extremely
Fig. 6 Post-operative photograph of patient 1 after reverse saphenous
flap insetting over the defect
Fig. 5 Pre-operative photograph of patient 1 showing raised reverse
saphenous flap
Fig. 7 Photograph of patient 2 showing defect over medial malleolus
and raised reverse saphenous flap
Fig. 8 Post-operative photograph of patient 2 after reverse saphenous
flap insetting over the defect
Fig. 9 Pre-operative photograph of patient 3 showing pressure ulcer
over heel
Eur J Orthop Surg Traumatol
123

engorged and the venous pressure inside the veins increased
to 42 mmHg, which was much higher than the capillary
pressure. Venous hypertension thus propagates and hinders
normal venous pressure through valveless small veins within
the flap. Cavadas [15] advocated to routinely ligated and
divide the vein at the base of the flap and taking care not to
disrupt other vascular structures. This significantly reduces
postoperative flap congestion and partial flap loss. In our
series, we have not ligated the saphenous vein at the base of
the flap and found no problem of engorgement of flap due to
venous hypertension.
Carriquiry et al. [4] reported their detailed anatomical
study of the septocutaneous vessels of the leg. They
reported that the lower leg perforator is 9–12 cm above the
tip of the medial malleolus. However, Amarante et al.
suggested that the lowest perforator of the posterior tibial
vessels is about 4 and 6.5 cm above the medial malleolus.
In all our cases, we found the lowest perforator 5–6 cm
from the medial malleolus.
Nayak et al. [16] in their study of the microneurovas-
cular structure of greater saphenous vein reported that the
vein is surrounded by a rich mixed vascular network from
ankle to knee.
Based on these networks, a flap can be raised over the
anteromedial aspect of the leg. Using only the neurocuta-
neous component restricts the length of the flap up to the
insertion of sartorius, that is, to a point where the nerve
dips deeper to the deep fascia. Inclusion of the vein enables
extension of the flap beyond this point.
Based on the vein, the pivot point of the flap can be
placed just proximal to the medial malleolus, but preser-
vation of the tibial perforator ensures better nourishment to
the flap.
Thus, inclusion of both the nerve and the vein enabled
raising of a long flap while ensuring its viability.
Amarante et al. [17] described a medial distally based
fasciocutaneous flap with a narrow pedicle and reported
four successful cases.
Cavadas [15] reported his experience of 5 cases of
reverse flow neurocutaneous saphenous flap with low
complication rate.
Shalby et al. [18] reported their experience of 7 cases of
distally based medial island septocutaneous flap for repair
of soft tissue defect of lower leg.
Rajacic et al. [19] reported their experience of using
distally based saphenous island flap in 14 patients. Nine
flaps survived completely. Two had marginal flap necrosis
while one flap lost completely.
Flap is indicated in defect of lower one-third leg, mid
foot and defect of heel. However, it is contraindicated in
venous disease of leg and in suspected trauma of perforator
and in peripheral arterial disease of leg. This flap has many
advantages. It can be raised with the patient in supine
position, does not require sacrifice of any major artery of
the leg and can be used to cover areas like tendo achilles.
The flap has wide arc of rotation, and it can reach up to
lower one-third leg, ankle and midfoot level. Moreover, it
is easy to execute and transpose. The donor site morbidity
is also minimal compared with the reverse sural flap, and
tendo achilles is not exposed. And also saphenous nerve
sacrifice has not been a problem, since most of the defect to
be reconstructed involved the area supplied by the nerve.
The elevation of large retrograde flow flap in the
saphenous region inevitably implies the elevation of pre-
tibial skin. We have modified the technique by elevating
the flap at the medial border of the shin preserving the
pretibial skin and taking care to include the great saphe-
nous vein in the flap. As the flap did not encroach upon the
subcutaneous part of tibia, the donor site defect required
only a split skin graft for coverage.
Any venous pathology like varicose vein and venous
thrombosis should be ruled out, as with sacrificing the
superficial veins venous congestion occurs.
Other options for reconstruction of lower leg and foot
include microvascular flaps, cross-leg flaps and reverse
flow island flaps. Microvascular flaps introduce healthy
tissue with its blood supply in the area. However, they
require sophisticated instruments and availability of a
microvascular team. Moreover, long-standing infection and
oedema alter the physical characteristics of the recipient
vessels and increase the possibility of anastomotic prob-
lems. Cross-leg flaps though feasible require the patient to
maintain an uncomfortable position for a long time. Thus, a
reverse saphenous flap scores over the other modalities of
treatment available for management of the leg and foot
defects.
The distally based medial septocutaneous flap, based on
one vascular pedicle with a very wide arc of rotation, can
Fig. 10 Post-operative photograph of patient 3 showing reverse saphe-
nous flap coverage over heel defect
Eur J Orthop Surg Traumatol
123

be transposed 90� or 180� to cover the defects of the lower
third of the leg successfully. There is no bulk or pedicle
kink of the flap. However, this flap is not recommended in
cases of venous ulcers or stasis because this might com-
prise the venous drainage of the flap.
In our series, we have used both pedicle as well as island
flap to cover the defect. Procedure is carried out in two
stages, first being flap elevation and coverage of defect.
Second stage is being flap detachment and insetting. Donor
site scar and loss of sensation at medial aspect of leg and two-
stage procedure are the main disadvantages. Our series shows
that majority of patients are males and got injured due to road
traffic accident, implicating that usually males are going out
for earning their living. Our series shows the complications
like discharge and infection, which may be due to inadequate
debridement or cross-infection and is controlled by antibi-
otics and dressing. Our series shows that partial flap necrosis
that may be due to kinking of pedicle or pressure over flap
due to improper position and controlled by giving proper
position and relieving the kinking or tension at the suture line
by removing sutures. Later the flap resettled. In our series 3,
patient showed total flap necrosis, which may be due to
pressure over pedicle for a prolong period and secondary
procedure like free flap have to be done to cover the defect.
Conclusion
Reverse pedicled saphenous flap is a versatile flap which
can be used to reconstruct defects of lower one-third leg
and foot with a reliable blood supply, easy elevation and
long vascular pedicle with a large arc of rotation can be
transposed up to base of the toes. Also, it preserves the
major arteries of the leg and also dispenses off with the
need of executing a free-tissue transfer while having min-
imal donor site morbidity.
Conflict of interest None.
References
1. Yoshimora M, Imura S, Shimamura K, Yamauchi S, Nomura S
(1984) Peroneal flap for reconstruction in the extremity. Plast
Reconstr Surg 74:402
2. Hong G, Steffens K, Wang FB (1989) Reconstruction of the
lower leg and foot with the reverse pedicled posterior tibial fas-
ciocutaneous flap. Br J Plast Surg 42:512
3. Townsend PLG (1978) An inferiorly based soleus muscle flap.
Br J Plast Surg 31:210
4. Carriquiry C, Costa M, Vasconez LO (1985) An anatomic study
of the septocutaneous vessels of the leg. Plast Reconstr Surg
76:354
5. Bhandari PS, Bath AS, Sadhotra LP (2005) Management of soft
tissue defects of the ankle and foot. Med J Armed Forces India
61:253–255
6. Ponten B (1981) The fasciocutaneous flap: its use in soft tissue
defects of the lower leg. Br J Plast Surg 34:215–220
7. Wee JTK (1986) Reconstruction of the lower leg and foot with
the reverse pedicled anterior tibial flap: preliminary report of a
new fasciocutaneous flap. Br J Plast Surg 39:327
8. Morrison WA, Shen TY (1987) Anterior tibial artery flap: anat-
omy and case report. Br J Plast Surg 40:230
9. Satoh K, Yoshikawa A, Hayasi M (1988) Reverse-flow anterior
tibial flap type III. Br J Plast Surg 43:634
10. Masquelet AC, Ramana MC, Wolf G (1992) Skin island flaps
supplied by the vascular axis of the sensitive superficial nerves.
Anatomic study and clinical experience in the leg. Plast Reconstr
Surg 89:1115
11. Timmons MJ (1984) Reverse flow through valves of forearm
veins. Lancet 2:394
12. Torri S, Namiki Y, Mori R (1987) Reverse flow island flap:
clinical report and venous drainage. Plast Reconstr Surg 79:600
13. Imanshi N, Nakajima H, Fukuzuni S (1999) Venous drainage of
the distally based lesser saphenous-sural veno-neuroadipofascial
pedicled fasciocutaneous flap: a radiographic perfusion study.
Plast Reconstr Surg 103:494
14. Chang SM (2000) Role of large superficial veins in distally based
flaps of the extremities. Plast Reconstr Surg 106:230
15. Cavadas PC (2003) Reversed saphenous neurocutaneous island
flap: clinical experience and evolution to the posterior tibial
perforator-saphenous subcutaneous flap. Plast Reconstr Surg 111(2):
837–839
16. Nayak BB, Thatte RL, Thatte MR, Baliarsing AS, Jagannathan
M, Pandit SP (2000) A microneurovascular study of great
saphenous vein in man and the possible implications for survival
of flaps. Br J Plast Surg 53:230–233
17. Amarante J, Costa H, Reis J (1986) A new distally based fas-
ciocutaneous flap of the leg. Br J Plast Surg 39:338
18. Shalby HA, Higazi M, Mandour S (1991) Distally based medial
Island septocutaneous flap for repair of soft tissue defect of the
lower leg. Br J Plast Surg 44:175–178
19. Rajacic N, Gang RK, Krishnan J, Kojic S (2001) Lower leg
reconstruction using distally based saphenous island flap. Euro J
Plast Surg 24:7–11
Eur J Orthop Surg Traumatol
123





























