Embed Size (px)
Citation preview

RECONSTRUCTION OF EXTENSIVE ABDOMINAL WALL DEFECTUSING AN ECCENTRIC PERFORATOR-BASED PEDICLEDANTEROLATERAL THIGH FLAP: A CASE REPORT
JOONCHUL JANG, M.D., SEONG-HO JEONG, M.D., Ph.D.,* SEUNG-KYU HAN, M.D., Ph.D., and WOO-KYUNG KIM, M.D., Ph.D.
Reconstruction of extensive abdominal wall defects is a challenge for reconstructive surgeons. In this report, a case of reconstruction of alarge abdominal wall defect using an eccentric perforator-based pedicled anterolateral thigh (ALT) flap is presented. A 30-year-old manpresented with recurrent desmoid-type fibromatosis in the abdominal wall. The recurrent tumor was radically excised, and the en blocexcision resulted in a full-thickness, large abdominal wall defect (25 cm 3 20 cm). An eccentric perforator-based pedicled ALT flap, includ-ing wide fascial extension, was transferred to the abdominal defect; fascial portions were sutured to the remnant abdominal fascia. Plica-tion of the fascia along the sutured portion was performed to relieve the skin tension between the flap and the marginal skin of theabdominal defect. Eight months after surgery, the reconstructed abdomen had an acceptable esthetic appearance without tumor recur-rence or hernia. The use of an eccentric perforator-based pedicled ALT flap may be an alternative method for the reconstruction of exten-sive abdominal wall defects. VC 2013 Wiley Periodicals, Inc. Microsurgery 33:482-486, 2013.
Reconstruction of extensive abdominal wall defects is a
challenge for reconstructive surgeons. Various approaches
to this type of reconstruction based on the use of skin
grafts and skin flaps, with or without concomitant incor-
poration of prosthetic materials, have been advocated in
the past. In recent years, the anterolateral thigh (ALT)
flap has been used extensively for the reconstruction of
various soft tissue defects.1 It is a versatile flap that has
gained popularity because of its ease of dissection, vari-
able composition and volume availability, long vascular
pedicle, and durable skin paddle.2 Since the introduction
of the ALT flap by Song et al.,3 the flap has evolved,
and the pedicled-type ALT flap has been used in the
reconstruction of defects in the groin and lower abdo-
men.2–5 Free ALT/fascia lata composite flaps have been
described as the ideal surgical option for various poston-
cological resection defects in the abdominal and thora-
coabdominal regions.4,5 These flaps have been used for
the reconstruction of defects that are not amenable to
direct primary repair or when stable reconstruction of the
fascial layer, adequate skin coverage, and restoration of
the contour of the abdominal wall are required.6 How-
ever, the pedicled ALT flap could be the option of
choice in certain cases such as the presence of recipient
vessel damage resulting from a primary operation or
other procedures and the presence of a high potential for
tumor recurrence that could lead to large abdominal wall
defects. Here, we report a case of reconstruction of an
extensive abdominal wall defect using the eccentric per-
forator-based pedicled ALT flap with an extended
fascial cuff.
CASE REPORT
A 30-year-old man presented with a recurrent palpa-
ble mass in the abdominal wall. Radical resection of the
abdominal mass and reconstruction using a local
advancement flap and umbilicoplasty had been performed
2 years earlier (Fig. 1A). The patient was histologically
diagnosed with desmoid-type fibromatosis after the previ-
ous surgery. Physical examination revealed a huge, solid,
indolent, recurrent mass within the infraumbilical rectus
abdominis muscle (Figs. 1B and 1C). Magnetic resonance
imaging showed a huge, lobulated, partially infiltrating,
local, recurrent mass extending into the entire lower ab-
dominal wall; the mass was mainly intramuscular in the
bilateral rectus abdominis (Fig. 2).
An en bloc resection with a wide curative margin
was performed, which resulted in a full-thickness abdom-
inal wall defect of 25 cm 3 20 cm. Before reconstruc-
tion of the abdominal wall defect, an intraoperative
frozen section was obtained for margin evaluation, and
histologically clear margins were confirmed. The abdomi-
nal fascia was repaired using a synthetic Marlex net
(Phillips Petroleum Company, Bartlesville, OK) (Fig. 3),
and a fasciocutaneous pedicled ALT perforator flap (20
cm 3 15 cm) was designed for the closure of the defect.
The perforator was located using a 5-MHz hand-held
Doppler probe. To maximize the rotation arc, the flap
was raised subfascially on the basis of two very distal
eccentric septocutaneous perforators (diameter, 1.5 mm);
the more proximal perforator was cut to obtain a maxi-
mal length pedicle (Fig. 4A). The flap with a 20 cm 3
15 cm skin paddle was raised, and a large piece of
Department of Plastic Surgery, Korea University Guro Hospital, Guro-Gu,Seoul, Korea
*Correspondence to: Seong-Ho Jeong, M.D., Ph.D., Department of PlasticSurgery, Korea University Guro Hospital, 97 Guro-Dong, Guro-Gu, Seoul152–703, Korea. E-mail: [email protected]
Received 11 December 2012; Revision accepted 27 February 2013;Accepted 4 March 2013
Published online 9 July 2013 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/micr.22117
� 2013 Wiley Periodicals, Inc.

vascularized fascial extension was included. Extended
fascial harvesting was performed by excavating �5 cm
beyond the cutaneous perimeter of the flap and then
incising around the larger area of fascia. During the har-
vest, the fascial margin showed good bleeding from its
subfascial and prefascial vascular plexus. The pedicle
was dissected to the level of its origin from the profunda
femoris with a division of the transverse branch. The
pedicled ALT perforator flap was then elevated and
delivered into the abdominal defect through the tunnel
beneath the rectus femoris and sartorius muscle (Fig.
4B). The deep fascia of the flap was sutured onto the
deep fascia of the abdomen. Then these fasciae were pli-
cated together to reduce skin tension. Release of the ten-
sion between the flap and the margin of the defect
facilitated suturing of the skin (Fig. 5).The donor site
was closed by sutures and a split-skin graft. Congestion
developed at the distal tip of the flap, which was
resolved after 5 days by the application of medical
leeches. Partial necrosis of fat tissues at the distal flap
portion and wound dehiscence (length, 4 cm) occurred.
However, the dehiscence healed well by secondary inten-
tion 1 month after the operation using conservative dress-
ings. Eight months after the surgery, the reconstructed
abdominal wall was stable without herniation of the in-
traperitoneal organs, and the esthetic result was good
(Fig. 6). The patient reported transient numbness within
the distribution of the lateral femoral cutaneous nerve.
However, there were no reports of donor-site complica-
tions, such as wound dehiscence, bulging, or herniation
of the thigh.
DISCUSSION
In the past, large, full-thickness abdominal wall
defects required staged repairs.4 The abdominal organs
were first covered with a synthetic mesh, and granulation
tissue was induced. Skin grafts were then performed.7
However, this technique of abdominal wall reconstruction
did not provide durable results. To overcome this draw-
back, pedicled or free flaps (sometimes accompanied by
prosthetic reinforcement) have been used for abdominal
reconstruction.8,9 In particular, the ALT perforator flap is
considered as a useful option. The free ALT perforator
flap (alone or in combination with a vascularized fascia
lata flap) has been used for the reconstruction of large
abdominal wall defects; however, the pedicled ALT per-
forator flap has not been used for this purpose because of
the limited rotation arc and relatively small dimension of
the skin paddle.6 Posch et al.10 showed that the combina-
tion of the skin paddle and the vastus lateralis muscle is
useful for reconstruction with an ALT flap and can be
used in cases of extensive defects. Sasaki et al.11
described the use of a combination of the tensor fasciae
Figure 1. Clinical aspects of a 30-year-old man with a solid mass
in the lower abdominal wall: (A) initial preoperative mass; (B) sec-
ond preoperative mass (anterior view); and (C) second preopera-
tive mass (lateral view). [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
Figure 2. Contrast-enhanced magnetic resonance imaging scan showing a huge (15 cm 3 15 cm 3 9.2 cm) lobulated, partially infiltrating,
local recurrent mass extending to almost the entire lower abdominal wall; the mass is mainly intramuscular in the bilateral rectus abdomi-
nis: (A) coronal view and (B) transverse view.
Treatment of Abdominal Wall Defect Using ALT Flap 483
Microsurgery DOI 10.1002/micr
lata musculocutaneous flap and the ALT flap for the
reconstruction of a large abdominal wall defect.
Recent reports have described the use of the pedicled
ALT perforator flap for the reconstruction of various
defects despite some limitations such as a limited rota-
tion arc and the relatively small dimensions of the skin
paddle.1,2,12–14 The pedicled ALT perforator flap can
have a long pedicle and can reach 8 cm above the umbil-
icus. Moreover, the pedicled ALT flap is associated with
a shorter operation time than the free ALT flap. Kayano
et al. found no significant differences between free and
pedicled ALT flaps in the rate of flap complications. The
only significant difference was a significantly longer
reconstructive time for free ALT flaps because of the
time required for microvascular anastomosis.15 Therefore,
we selected the pedicled ALT perforator flap attached to
the fascia lata and used perforators to reconstruct the ab-
dominal wall.
In this case, the reconstruction of the large abdominal
wall defect was limited by the size of the ALT skin flap.
We solved this problem by using an eccentric perforator
and placating the extended fascia. The careful selection
of perforators allows the flap to reach the subcostal area;
however, if the selection is not appropriate, it may be a
limiting factor in pedicle extension.14 The entire length
of the vascular pedicle and consequently the radius of
the rotation arc increases when the perforator is distally
Figure 3. Desmoid-type fibromatosis resection with wide margins
that resulted in a full-thickness defect (25 cm 3 20 cm). Defect
coverage was performed using a synthetic Marlex mesh for fascial
stabilization. [Color figure can be viewed in the online issue, which
is available at wileyonlinelibrary.com.]
484 Jang et al.
Microsurgery DOI 10.1002/micr
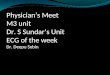
Figure 4. A (from the lateral side): A pedicled ALT perforator flap was elevated on the basis of two very distal perforators (black arrows).
The more proximal perforator was cut to maximize the arc of rotation. The lateral circumflex femoral artery is indicated with an orange
arrow. B: The flap was delivered to the abdominal defects through the submuscular and subcutaneous tunnels. Attached fascia (black
arrow). C: Eccentric perforator (black arrow) is shown. D: Schematic of the arc of rotation, and pedicle (dotted lines) are shown. [Color fig-
ure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
located in the case of a proximally based flap. Gravvanis
et al.1 showed that a pedicled ALT flap could be trans-
ferred proximally or distally from the umbilicus to the tib-
ial tuberosity. We used the distal eccentric perforator,
which improved the distal reach of the flap. The absence
of distal perforator pedicles in flap elevation procedures
prevents the transfer of the flap to the subcostal area. In
this case, the pedicled ALT flap might be transferred to a
free ALT flap.5 Potential recipient vessels are the superfi-
cial circumflex iliac artery or the deep circumflex iliac ar-
tery. Another possible method is plication of the extended
fascia. Using this method, the skin paddle of the flap in
the remaining abdominal wall can be approximated.
Therefore, the size of the defect can be reduced as much
as possible and skin repair between the remaining abdomi-
nal wall and skin-flap paddle can be performed with ease.
In this case, we achieved excellent functional and es-
thetic results using this method. Functionally, we pre-
vented herniation by plicating the extended fascia, which
resulted in a tight abdominal wall. Esthetically, the color
and thickness of the flap and those of the abdomen were
satisfactory. In addition, a very important advantage of
this method is that the opposite thigh can be saved for
managing a recurrent tumor. Salas et al.16 described three
unfavorable prognostic factors of desmoid-type fibroma-
tosis: age< 37 years, tumor size> 7 cm, and extra-ab-
dominal tumor location. In the current case, age and
tumor size were relevant as unfavorable prognostic fac-
tors. With regard to tumor recurrence, the saved opposite
thigh can provide useful tissue for the reconstruction of
abdominal defects. However, before the adoption of this
method, several disadvantages should be considered. Do-
nor-site issues such as pain, weakness, wound dehis-
cence, and scarring can develop because the deep fascia
is sacrificed.17 The method may not be performed
because of the anatomic variations of perforators. More-
over, congestion at the distal portion of the flap may de-
velop because of insufficient venous drainage. To test if
the distal part of flap gets enough perfusion, it can be
helpful to clamp the more proximal perforator before
complete flap elevation. If the distal perfusion is found
poor after clamping the proximal perforator, we suggest
two possible options. Supercharging procedure can be
considered as one choice.18 In other words, anastomosis
between proximal perforator vein and the superficial cir-
cumflex iliac vein may be possible. Free ALT flap could
be another option in case of failure in supercharging.5
Other methods to overcome the flap-size limitation
for the reconstruction of large defects have been
reported. Kulahci et al.19 used a pre-expanded pedicled
flap to reconstruct a large defect. Fujiwara et al.20
reported the use of a free flap in combination with a
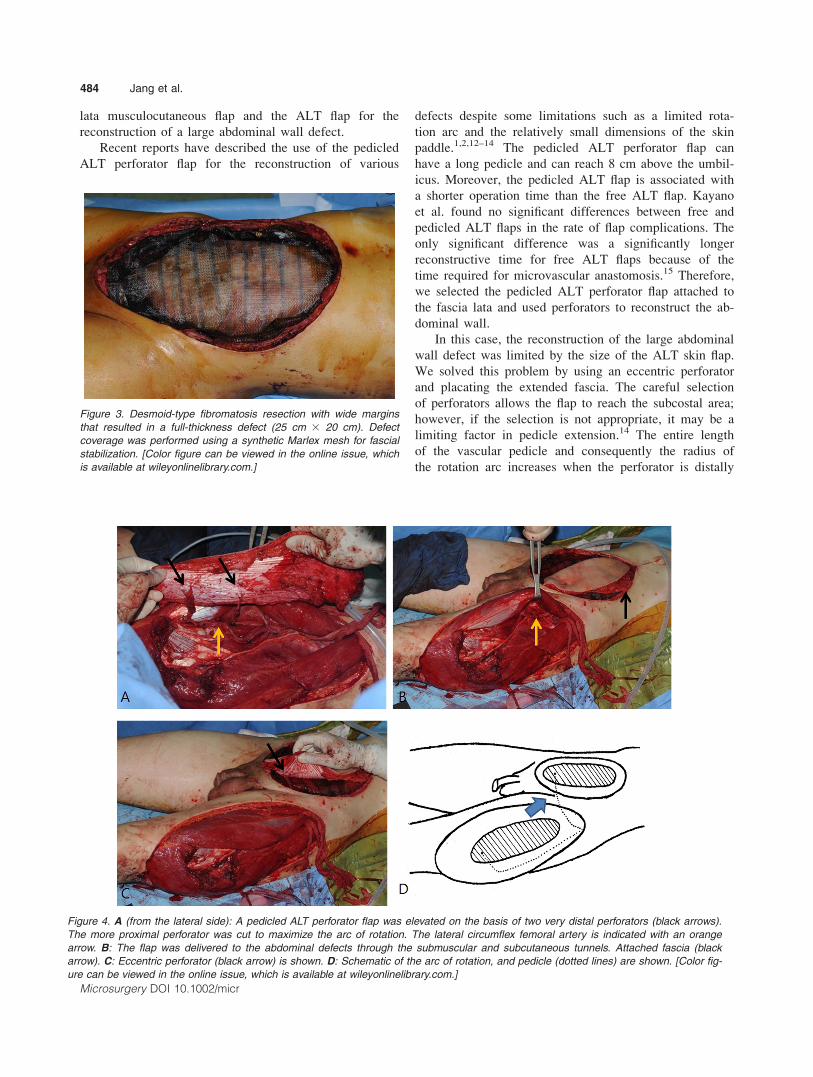
Figure 5. A: Schematic of the pedicle ALT flap set into the abdominal defect. B: Schematic horizontal section of dotted lines: (a) fascial
suture, (b) plication of fascia, and (c) skin suture. [Color figure can be viewed in the online issue, which is available at
wileyonlinelibrary.com.]
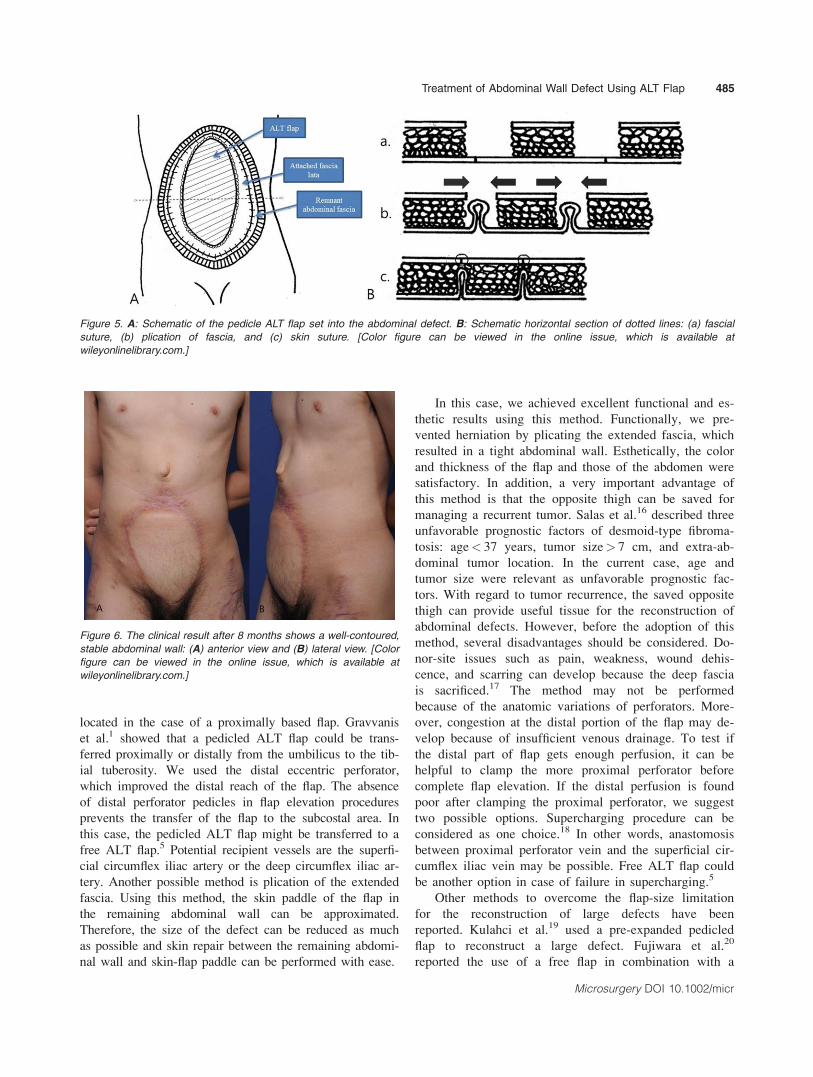
Figure 6. The clinical result after 8 months shows a well-contoured,
stable abdominal wall: (A) anterior view and (B) lateral view. [Color
figure can be viewed in the online issue, which is available at
wileyonlinelibrary.com.]
Treatment of Abdominal Wall Defect Using ALT Flap 485
Microsurgery DOI 10.1002/micr

delayed procedure. The use of a tissue expander or
delayed reconstruction could be applied to our technique.
Further research is necessary to evaluate pre-expanded
pedicled ALT flaps and an eccentric perforator-based
pedicled ALT flap in delayed reconstruction. This will be
the focus of our future investigations.
Despite some drawbacks, we believe that the eccen-
tric perforator-based pedicled ALT flap with an extended
fascial cuff can be a very useful alternative for recon-
structing extensive abdominal wall defects.
REFERENCES
1. Gravvanis AI, Tsoutsos DA, Karakitsos D, Panayotou P, IconomouT, Zografos G, Karabinis A, Papadopoulos O. Application of thepedicled anterolateral thigh flap to defects from the pelvis to theknee. Microsurgery 2006;26:432–438.
2. Ting J, Trotter D, Grinsell D. A pedicled anterolateral thigh (ALT)flap for reconstruction of the epigastrium. Case report. J PlastReconstr Aesthet Surg 2010;63:e65–e67.
3. Song YG, Chen GZ, Song YL. The free thigh flap: A new free flapconcept based on the septocutaneous artery. Br J Plast Surg1984;37:149–159.
4. Mathes SJ, Steinwald PM, Foster RD, Hoffman WY, Anthony JP.Complex abdominal wall reconstruction: A comparison of flap andmesh closure. Ann Surg 2000;232:586–596.
5. Wong CH, Lin CH, Fu B, Fang JF. Reconstruction of complex ab-dominal wall defects with free flaps: Indications and clinical out-come. Plast Reconstr Surg 2009;124:500–509.
6. Kuo YR, Kuo MH, Lutz BS, Huang YC, Liu YT, Wu SC, HsiehKC, Hsien CH, Jeng SF. One-stage reconstruction of large midlineabdominal wall defects using a composite free anterolateral thighflap with vascularized fascia lata. Ann Surg 2004;239:352–358.
7. Millard DR, Pigott R, Zies P. Free skin grafting of full-thicknessdefects of abdominal wall. Plast Reconstr Surg 1969;43:569–582.
8. Yang F. Radical tumor excision and immediate abdominal wallreconstruction in patients with aggressive neoplasm compromisedfull-thickness lower abdominal wall. Am J Surg 2013;205:15–21.
9. Williams JK, Carlson GW, deChalain T, Howell R, Coleman JJ.Role of tensor fasciae latae in abdominal wall reconstruction. PlastReconstr Surg 1998;101:713–718.
10. Posch NA, Mureau MA, Flood SJ, Hofer SO. The combined freepartial vastus lateralis with anterolateral thigh perforator flap recon-struction of extensive composite defects. Br J Plast Surg2005;58:1095–1103.
11. Sasaki K, Nozaki M, Nakazawa H, Kikuchi Y, Huang T. Recon-struction of a large abdominal wall defect using combined free ten-sor fasciae latae musculocutaneous flap and anterolateral thigh flap.Plast Reconstr Surg 1998;102:2244–2252.
12. Lannon DA, Ross GL, Addison PD, Novak CB, Lipa JE, NeliganPC. Versatility of the proximally pedicled anterolateral thigh flapand its use in complex abdominal and pelvic reconstruction. PlastReconstr Surg 2011;127:677–688.
13. Neligan PC, Lannon DA. Versatility of the pedicled anterolateralthigh flap. Clin Plast Surg 2010;37:677–681, vii.
14. Maxhimer JB, Hui-Chou HG, Rodriguez ED. Clinical applicationsof the pedicled anterolateral thigh flap in complex abdominal-pelvicreconstruction. Ann Plast Surg 2011;66:285–291.
15. Kayano S, Sakuraba M, Miyamoto S, Nagamatsu S, Taji M, Ume-zawa H, Kimata Y. Comparison of pedicled and free anterolateralthigh flaps for reconstruction of complex defects of the abdominalwall: Review of 20 consecutive cases. J Plast Reconstr Aesthet Surg2012;65:1525–1529.
16. Salas S, Dufresne A, Bui B, Blay JY, Terrier P, Ranchere-Vince D,Bonvalot S, Stoeckle E, Guillou L, Le Cesne A, Oberlin O, BrousteV, Coindre JM. Prognostic factors influencing progression-free sur-vival determined from a series of sporadic desmoid tumors: A wait-and-see policy according to tumor presentation. J Clin Oncol2011;29:3553–3558.
17. Lipa JE, Novak CB, Binhammer PA. Patient-reported donor-sitemorbidity following anterolateral thigh free flaps. J Reconstr Micro-surg 2005;21:365–370.
18. Kawai K, Imanishi N, Nakajima H, Aiso S, Kakibuchi M, HosokawaK. Vascular anatomy of the anterolateral thigh flap. Plast ReconstrSurg 2004;114:1108–1117.
19. Kulahci Y, Sever C, Uygur F, Oksuz S, Sahin C, Duman H. Pre-expanded pedicled thoracodorsal artery perforator flap for postburnaxillary contracture reconstruction. Microsurgery 2011;31:26–31.
20. Fujiwara M, Nagata T, Matsushita Y, Fukamizu H. Free hemibackflap with surgical delay for reconstruction of extensive soft tissuedefect: A case report. Microsurgery 2013;33:152–155.
486 Jang et al.
Microsurgery DOI 10.1002/micr