-
Central JSM Ophthalmology
Cite this article: Kalikivayi L, Salim R, Jacob SC, Kalikivayi V
(2020) Effectiveness of Unilateral or Alternating Methods Employed
to Measure Phoria When Targets Get Deviated From Midline among
School Children. JSM Ophthalmol 7(1): 1072.
*Corresponding authorLavanya Kalikivayi, Asst.Professor, Ahalia
School of Optometry, Palakkad, Kerala, 678557, India, Email:
[email protected]
Submitted: 08 August 2020
Accepted: 20 August 2020
Published: 22 August 2020
ISSN: 2333-6447
Copyright© 2020 Kalikivayi L, et al.
OPEN ACCESS
Research Article
Effectiveness of Unilateral or Alternating Methods Employed to
Measure Phoria When Targets Get Deviated From Midline among School
ChildrenLavanya Kalikivayi, Ruksana Salim, Sajeev Cherian Jacob,
and Venkataramana KalikivayiAhalia School of Optometry, Palakkad,
IndiaAhalia Foundation Eye Hospital, Palakkad, Kerala, India
INTRODUCTIONBinocular single vision is defined as the perception
of
simultaneous vision with coordinated use of both eyes to produce
a single vision when an individual’s attention is on an object of
regard. Proper development of motor and sensory mechanism along
with a proper mental process is essential. Additionally, to
maintain a clear vision in a dynamic environment, it involves both
accommodative facility and vergence facility. Accommodation helps
in focusing the objects at various distances and the vergence
system helps in aligning the eye accordingly [1]. Unlike infants,
as a child grows, blur is not the only stimulus for accommodation.
It involves all the different types of accommodations along with
fusional convergence in variable proportions depending on the
viewing environment [2].
Another factor that requires consideration is, for a given
stimulus at a particular distance, the amount of accommodative and
associated vergence is asymmetrical between the eyes. When a target
is moved nearer, it gets displaced off the midline,
and the resultant adduction will be asymmetrical with dynamic
properties of slow vergence and abnormalities of this vergence may
contribute to non-strabismic anomalies in childhood [3].
Apart from non-strabismic anomalies, this asymmetry can cause
physiological heterophoria. This heterophoria may lead to altered
stereo acuity. The literature states that distance stereo acuity is
achieved to adult levels by approximately 5 years [4]. In spite of
stereo acuity development completion, children with heterophoria
exhibit altered stereo acuity, more with esophoria than with
exophoria [5,6].
Earlier studies revealed that a proper visual function and motor
integration are important factors for good academic performance in
a child [7]. It is an established fact that prevalence of non-
strabismic anomalies of binocular vision are high among school
children and hence screening of these along with refractive errors
are important [8,9]. Another study stated that a significant
increase in myopia occurs owing to the presence of head tilt in
children while writing. This asymmetrical viewing
Keywords•Heterophoria•Motor and Sensory
mechanism•Vergence•Accommodation
Abstract
To maintain a clear vision in dynamic environment, both
accommodative and vergence facilities are imperative, though they
are asymmetrical between the eyes. This asymmetrical vergence leads
to non strabismic anomalies in children. The position of the
targets while measuring these phoria and the method of measurement
employed plays an important role in concluding the amount of
heterophoria present. The influence of this asymmetry and
consequently the interactions between the motor and sensory
mechanism in producing heterophoria were measured by alternate
cover test (ACT), with reference to the amount of phoria measured
independently in each eye through cover/uncover test (PBCT), and
modified thorington test (MTT), in children. The results revealed a
statistically significant difference in the measurement of
heterophoria for distance between ACT, PBCT and by MTT both between
the groups and within the groups with a p < 0.00. A
statistically significant difference was found between ACT and PBCT
with prism in front of the right eye for near with p = 0.025 and
between ACT and MTT with Maddox rod in front of right eye for a
near target with p = 0.004. Similarly, a statistically significant
difference was found between ACT and PBCT with prism in front of
the left eye for near with p = 0.018 and between ACT and MTT with
Maddox rod in front of left eye for a near target with p = 0.009.
This study emphasizes to measure heterophoria through cover/uncover
test which is more pertinent with the dynamic spatial environment
than ACT during school screening programs.
mailto:[email protected]
-
Central
Kalikivayi L, et al. (2020)
JSM Ophthalmol 7(1): 1072 (2020) 2/5
angle between eyes lead to asymmetrical vergence and induced
hyperopic defocus between the eyes [10].
All these led to the thought that the total phoria measured are
not equally distributed between the eyes. Hence the aim of the
study is to find out the impact of targets deviated from midline
while measuring phoria among school children.
MATERIALS & METHODSA cross-sectional study with 349 subjects
between 7 and 18
years were enrolled in the study, of which 180 were girls and
169 were boys. All the subjects were selected by simple random
sampling from a school in Kerala.
Subjects without symptoms, with a best corrected visual acuity
of < 0.2 logMAR (6/9), for distance and N6 for near in both the
eyes, normal ocular motility, and no manifest deviation were
included in the study. Subjects with ocular pathology, previous
ocular surgeries, nystagmus, amblyopia, and contact lens wear were
excluded from the study.
The study followed the tenets of the Declaration of Helsinki and
got approved by the Institutional ethics committee. Informed
consent was obtained from the school authorities and acceptance
from the parents. Each child was explained before the commencement
of procedures. All the procedures were executed by the same
examiner who was well experienced as per optometric practice.
Vision assessment, objective and subjective refraction, ocular
motility, the amplitude of accommodation using RAF ruler, and the
near point of convergence were measured [11-14], Following these
procedures, ocular deviation, and stereo acuity were measured as
explained below.
A standard cover/uncover and alternate cover tests were
performed followed by prism bar cover test (PBCT). The PBCT was
performed for each eye separately and also together. The subject
was given a target at 3 meters to fixate which was not precisely at
midline. Initially, with the left eye fixating on the target, PBCT
through cover/uncover test with an occlusion time of 2 seconds was
done on the right eye and the strength of the prism with which no
recovery movement of the eye undercover was noted. This was noted
as the amount of phoria in the right eye. The same procedure was
repeated in the left eye and recorded. Similarly, the entire
procedure for both right and left eye was done for a near target at
40 cm [15], following which, the alternate cover test (ACT), with
prisms was performed for both distance and near in a conventional
way [16]. The occlusion time of 2 seconds was maintained while
performing ACT too.
As PBCT was an objective method, Modified Thorington test (MTT),
was performed for a subjective measurement which is more reliable
than other subjective methods [17].
Similar to PBCT, MTT was also performed for each eye separately.
A Maddox rod was placed in front of the right eye with horizontal
orientation. Penlight was shone from behind the hole of the MTT
card at 3 meters which was also not positioned exactly at midline.
The subject was asked to report if the straight line produced by
the Maddox rod was to the right or left to the spot. This value was
recorded as the phoria of the right eye [18].
The same procedure was repeated with Maddox rod in front of the
left eye and recorded as phoria of the left eye, and the whole
procedure was executed for near at 40 cm too.
The stereo acuity was measured using a TNO random test as the
measurement is devoid of monocular cues, and a more critical judge
than other methods employed in stereo acuity measurements [19].
Descriptive statistics were computed for all the parameters. As
a conventional practice, exophoria was expressed with a negative
sign and esophoria with a positive sign. The limits of agreement
(LOA), between the two different methods of heterophoria
measurement (PBCT-objectively and MTT-subjectively) were found
using Bland Altman plots, which defined LOA = mean difference ±
1.96 x standard deviation of the differences between two methods.
MedCalc was used to fit the data and graphical representation.
ANNOVA test for comparing the means of equal variance was used to
compare the difference in phoria measured by ACT, PBCT, and MTT,
for distance and near (SPSS16.0). Simple linear regression was
performed to analyze the effect of heterophoria on stereo
acuity.
RESULTSOut of 349 children between 7 and 18 years, 51.5% (180),
were
girls and 48.5% (169), were boys. The mean age of the sample was
11.5 ± 3.01 years. The distributions of refractive errors were 3.44
% of hyperopia with a mean spherical equivalent of + 1.02 D ± 0.77,
15.76 % of myopia with a mean spherical equivalent of – 1.64 D ±
1.37 and 80.80 % of emmetropia.
The prevalence of heterophoria for distance was found in 92
subjects (26.36%), and that for near was in 174 subjects (49.86%).
Out of this 92 and 174 subjects, the heterophoria measured through
cover/uncover test with PBCT showed varied responses between the
eyes. The distribution of these are represented in Tables 1 and 2
for distance and near respectively.
The agreement between PBCT and MTT for right and left eye
separately was performed using Bland Altman analysis. The mean
difference between the two methods for distance was found to be
-0.4 (CI 6.5, -7.3), and -0.4 (CI 3.1,-3.9), in the right and left
eye respectively. Likewise, the mean difference between the two
methods for near was found to be 0.1 (CI 2.55, -2.35), and 0.1 (CI
2.2, -2.0), in the right and left eye respectively. This states
that both methods were agreeable to each other and can be used to
measure alternatively.
The mean phoria exhibited by ACT was 1.60∆ ± 0.51 exophoria for
distance and for near was 1.69∆ ± 0.51 exophoria. The mean phoria
measured through cover/uncover test with prisms in front of the
right eye for distance was 0.56∆ ± 4.10 esophoria and that for near
was 1.13∆ ± 3.53 exophoria. Similarly, the mean phoria measured
through cover/uncover test with prisms in front of the left eye for
distance was 0.87∆ ± 3.89 esophoria and for near was 1.05∆ ± 3.76
exophoria. The mean phoria measured by MTT with Maddox rod in front
of the right eye for a distance target was 0.20∆ ± 3.73 esophoria
and for a near target was 0.99∆ ± 3.41 exophoria. Concurrently the
mean phoria measured by MTT with Maddox rod in front of the left
eye for a distance target was 0.47∆ ± 3.73 esophoria and for a near
target was 0.99∆ ± 3.70
-
Central
Kalikivayi L, et al. (2020)
JSM Ophthalmol 7(1): 1072 (2020) 3/5
Table 1: Distribution of heterophoria in each eye with prism bar
cover test (PBCT) and modified thorington test (MTT) for 3m
distance.
Heterophoria PBCT Right Eye PBCT Left Eye MTT Right Eye MTT Left
Eye
Number Percentage Number Percentage Number Percentage Number
Percentage
Orthophoria 35.00 38.04 7.00 7.61 35.00 38.04 16.00 4.98
Exophoria 25.00 27.17 39.00 42.39 25.00 27.17 35.00 10.90
Esophoria 32.00 34.78 46.00 50.00 32.00 34.78 41.00 12.77
Table 2: Distribution of heterophoria in each eye with prism bar
cover test (PBCT) and modified thorington test (MTT) for 40cm.
Heterophoria PBCT Right Eye PBCT Left Eye MTT Right Eye MTT Left
Eye
Number Percentage Number Percentage Number Percentage Number
Percentage
Orthophoria 17.00 9.77 45.00 25.86 29.00 4.78 54.00 8.89
Exophoria 104.00 59.77 82.00 47.13 97.00 15.97 78.00 12.84
Esophoria 53.00 30.46 47.00 27.01 48.00 7.90 42.00 6.92
exophoria. The mean heterophoria measured through different
methods for both distance and near is presented in Table 3.
The mean heterophoria measured by ACT, PBCT with prism in front
of the right eye for distance and MTT with Maddox rod in front of
the right eye for distance were compared by ANNOVA and was found to
be statistically significant both between the groups and within the
groups with p < 0.00. Similarly, an ANNOVA was performed between
ACT, PBCT with prism in front of the left eye for a distance target
and MTT with the Maddox rod placed in front of the left eye with a
target at distance revealed a statistically significant difference
both between the groups and within the groups with a p <
0.00.
On the contrary, the mean heterophoria measured by ACT, PBCT
with prism in front of the right eye for near and MTT with Maddox
rod in front of right eye for a near target when compared by ANNOVA
was not statistically significant between the groups but was found
to be statistically significant within the groups. A statistically
significant difference of p = 0.025 was found between ACT and PBCT,
and a statistically significant difference of p = 0.004 was found
between ACT and MTT. There was no statistically significant
difference between PBCT and MTT.
Comparably, an ANNOVA when performed between ACT, PBCT with
prism in front of the left eye for a near target and MTT with the
Maddox rod placed in front of the left eye with a target at near
revealed no statistically significant difference between the groups
whereas a significant difference was found within the groups with a
p = 0.018 between ACT and PBCT, and a p = 0.009
between ACT and MTT. No statistical significance was found
between PBCT and MTT.
The influence of heterophoria on stereo acuity was analyzed with
a simple linear regression and was not statistically significant
(R2 = 0.04).
DISCUSSIONThe study revealed a significant difference in the
heterophoria
measured through ACT when compared with PBCT and MTT. These
alterations state that the accommodation and associated vergence
for a stimulus at a particular distance is asymmetrical between the
eyes. Further, on proximal movement of the target, it gets
displaced off the midline, and the resultant adduction will be
asymmetrical with dynamic properties of slow vergence. It was
reported in spite of both eyes sharing common substratum in a
natural viewing environment, it is necessary to test each eye
separately to identify specific defects for precise diagnosis
[3].
A study on the influence of eye position signals on perceived
visual direction [20], proposed that the egocentric visual
direction (EVD), is connecting the retinal image and signals from
eccentric points in regard to the position of the eye in the head.
The oculomotor commands are generated by the amalgamation of neural
signals from conjugate and convergent eye positions, which grant
the brain to restore separate eye position for each eye.
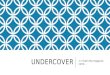
The movement of the eye and angular shift for distance and near
is mathematically represented in Figures 1 and 2
Table 3: Means of heterophoria for distance and near measured
through different methods.
Measurement MethodHeterophoria (PBCT) Heterophoria
(Alternatecover-uncover test) ∆OD ∆ OS ∆
Distance PBCT with Cover-Uncover test 0.56 (±4.1) ESO 0.87
(±3.89) ESO
1.60 (± 0.51) EXODistance MTT 0.20 (±3.73) ESO 0.47 (±3.73)
ESO
Near PBCT with Cover-Uncover test 1.13 (±3.53)EXO 1.05 (±3.76)
EXO
1.69 (± 0.51) EXONear MTT 0.99 (±3.41) EXO 0.99 (±3.70) EXO
PBCT: Prism bar cover test, MTT: Modified thorington test, ∆:
Prism Diopter, EXO: Exophoria, ESO: Esophoria
-
Central
Kalikivayi L, et al. (2020)
JSM Ophthalmol 7(1): 1072 (2020) 4/5
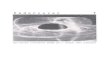
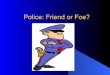
left eye when viewing a target exactly at a 40 cm distance in
the center is 85.755⁰ i.e., ∠PLM/PRM is 4.25⁰ inwards. The angular
shift ∠OLM and ∠ORM with a displacement of the object by 10 cm to
the right side is 13.79⁰ adducted and 14.11⁰ abducted for the left
and right eye respectively.
These calculations are helpful in understanding the asymmetry
presented by each eye with minimal displacement, which are common
during clinical examination settings. Generally, while performing a
PBCT, the target is given to the patient to be held at 40cm, as the
examiner holds both the occluder and the prism bar. A right or left
side shift of the target is observed if the patient is right or
left handed. Similarly, for distance, the target is not exactly
placed at the midline of the patient. Further facial asymmetry and
unequal distribution of inter pupillary distance (IPD), can
contribute to varied heterophoria between ACT and cover/uncover
measurements.
An earlier study reported that on quantitative analyses of the
eye movements during cover/uncover test, the mean phoria after
occlusion was 0.1⁰ ± 1.4 esophoria for 3m distance and 1.6⁰ ± 2
exophoria for near at 40 cm distance [21]. Whereas this study
revealed a mean phoria of 0.71⁰ ± 1.99 esophoria for 3 m distance
and 1.09⁰ ± 1.82 exophoria for near.
It was observed that 1.6∆ exophoria for distance with ACT
altered to 1.43∆ esophoria with cover/uncover test. This drift can
be attributed to the higher dissociation effect with ACT than
cover/uncover test, while the tonic vergence of the fixating eye
impacts the phoria of the other eye with cover/uncover test as
opposed to ACT.
Conversely, for near, the 1.69∆ exophoria exhibited with ACT
increases to 2.18∆ exophoria with cover/uncover test, which could
be due to the equal disruption of accommodative convergence during
ACT, whereas with cover/uncover test, the fixating eye exhibits
more accommodation compared to the covered eye as observed with
diagnostic occlusion.
From earlier studies, the prevalence of non-strabismic binocular
vision anomalies among school children was 29.6% in rural India
[8], hence it is appropriate to measure heterophoria through
cover/uncover test which is more pertinent with the dynamic spatial
environment than ACT during school screening programs. A study on
the relationship between posture and myopia had stated that poor
posture [22], principally neck angle had a significant relation to
the degradation of unaided vision. Another study revealed that
prolonged near reading of an hour or more, metamorphoses the
resting postures of both accommodation and vergence [23]. The same
study also alleged that changes in tonus accommodation are
responsible for blurred distance vision after an hour of near
reading and tonus vergence is responsible for visual fatigue.
Besides the above rationale, the head tilts present when children
are writing influence the increase in myopia as the asymmetrical
viewing angle between the eyes impact the asymmetrical vergence and
induced hyperopic defocus amidst the eyes [10]. Hence the
importance of measuring phoria separately for each eye is befitting
than measuring through ACT, as these motor mechanisms have an
implication on the sensory mechanism in presenting heterophoria,
thereby enhancing the cognition in children.
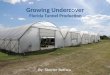
Figure 1 Mathematical representation of the eye movement
associated angular shift for a target viewed at 3 meters
distance.
Figure 2 Mathematical representation of the eye movement
associated angular shift for a target viewed at 40 meters
distance.
respectively. The letters M, R, L in the figure are Midline for
the right and left eye, P is the target placed exactly at midline
and O is the target displaced by 10cm to the right side.
In a hypothecated example, the distance viewed by the right and
left eye increase by 1mm and 3mm respectively if an object at 3 m
is shifted to the right side by 10cm and vice versa if the shift is
to the left side. The angle subtended by the right and left eye
when viewing a target exactly at the 3m distance in the center is
85.89⁰ i.e., ∠PLM/PRM is 4.11⁰ inwards. The angular shift ∠OLM and
∠ORM with the displacement of the object by 10cm to the right side
is 1.91⁰ adducted and 5.73⁰ abducted for the left and right eye
respectively.
Similarly, when considered for an object placed at 40 cm for
near, with a displacement by 10cm to the right side, the associated
shift in the distance by the right and left eye is 6.1 mm and 20.6
mm respectively and vice versa if shifted to the left side. Similar
to distance target, the angle subtended by the right and
-
Central
Kalikivayi L, et al. (2020)
JSM Ophthalmol 7(1): 1072 (2020) 5/5
CONCLUSIONThere is a significant difference in the measurement
of
heterophoria between cover/uncover test and ACT. Hence the
importance of measuring heterophoria unilaterally for each eye
through cover/uncover test cannot be more emphasized than
measurements through ACT. These are beneficial in diagnosing
non-strabismic binocular anomalies conclusively during school
screening programs and routine clinical evaluations. These findings
will be of value in children with myopia, to alter their reading
and viewing posture appropriately for near in controlling the
myopic progression. Unilateral measurements taken for each eye will
be pragmatic for correction required when strabismic surgeries are
performed monocularly. Further studies correlating these findings
with the effect of AC/A ratio is recommended.
REFERENCES1. Bharadwaj SR, Candy TR. Cues for the control of
ocular accommodation
and vergence during postnatal human development. J Vis. 2008; 8:
14.
2. Currie DC, MANNY RE. The development of accommodation. Vision
Res. 1997; 37: 1525-1533.
3. Leigh RJ, Zee DS. The neurology of eye movements. Oxford
University Press, USA; 2015.
4. Hong SW, Park SC. Development of distant stereoacuity in
visually normal children as measured by the Frisby–Davis distance
stereotest. Br J Ophthalmol. 2008; 92: 1186-1189.
5. Saladin JJ. Stereopsis from a performance perspective. Optom.
Vis. Sci. 2005; 82: 186-205.
6. Shim HS, Kim SH, Kim YC. Correlation of near stereoacuity and
phoria, and refractive error. J Korean Ophthalmic Opt Soc. 2015;
20: 67-73.
7. Goldstand S, Koslowe KC, Parush S. Vision, visual-information
processing, and academic performance among seventh-grade
schoolchildren: A more significant relationship than we thought? Am
J Occup Ther. 2005; 59: 377-389.
8. Hussaindeen JR, Rakshit A, Singh NK. Prevalence of
non-strabismic anomalies of binocular vision in Tamil Nadu: report
2 of BAND study. Clin Exp Optom. 2017; 100: 642-648.
9. Dusek W, Pierscionek BK, McClelland JF. A survey of visual
function in an Austrian population of school-age children with
reading and writing difficulties. BMC Ophthalmol. 2010; 10: 16.
10. Li SM, Li SY, Kang MT, Zhou Y, Liu LR, Li H, et al. Near
work related parameters and myopia in Chinese children: the Anyang
Childhood Eye Study. PLoS One. 2015; 10: e0134514.
11. Sheedy JE, Bailey IL, Raasch TW. Visual acuity and chart
luminance. Am J Optom Physiol Opt. 1984; 61: 595-600.
12. Sharma IP. RAF near point rule for near point of
convergence-a short review. Ann Eye Sci. 2017; 2.
13. Neely JC. The RAF near-point rule. Br J Ophthalmol. 1956;
40: 636.
14. Scheiman M, Gallaway M, Frantz KA, Peters RJ, Hatch S, Cuff
M, et al. Nearpoint of convergence: test procedure, target
selection, and normative data. Optom. Vis. Sci. 2003; 80:
214-225.
15. Eye world: Diseases of the eye and treatment. Evaluation of
a case of concomitant strabismus. December 30, 2010.
16. Nema HV, Nema N. Diagnostic procedures in ophthalmology. JP
Medical Ltd. 2014 May 30.
17. American academy of ophthalmology: Clinical Education.
Dissimilar image tests. 2019.
18. Goss DA, Reynolds JL, Todd RE. Comparison of four
dissociated phoria tests: reliability & correlation with
symptom survey scores. J Behav Optom. 2010; 21: 99-104.
19. Okuda FC, Apt L, Wanter BS. Evaluation of the TNO random-dot
stereogram test. Am Orthopt J. 1977; 27: 124-130.
20. Sridhar D, Bedell HE. Binocular retinal image differences
influence eye-position signals for perceived visual direction.
Vision Res. 2012; 62: 220-227.
21. Barnard NS, Thomson WD. A quantitative analysis of eye
movements during the cover test–a preliminary report. Ophthalmic
Physiol Opt. 1995; 15: 413-419.
22. Marumoto T, Sotoyama M, Villanueva MB, et al. Relationship
between posture and myopia among students. In: Myopia Updates,
Springer; 1998: 63-66.
23. Owens DA, Wolf-Kelly K. Near work, visual fatigue, and
variations of oculomotor tonus. Invest Ophthalmol Vis Sci. 1987;
28: 743-749.
Kalikivayi L, Salim R, Jacob SC, Kalikivayi V (2020)
Effectiveness of Unilateral or Alternating Methods Employed to
Measure Phoria When Targets Get Deviated From Midline among School
Children. JSM Ophthalmol 7(1): 1072.
Cite this article
https://pubmed.ncbi.nlm.nih.gov/19146280/https://pubmed.ncbi.nlm.nih.gov/19146280/https://core.ac.uk/download/pdf/81926503.pdfhttps://core.ac.uk/download/pdf/81926503.pdfhttps://oxfordmedicine.com/view/10.1093/med/9780199969289.001.0001/med-9780199969289https://oxfordmedicine.com/view/10.1093/med/9780199969289.001.0001/med-9780199969289http://europepmc.org/article/MED/18614571http://europepmc.org/article/MED/18614571http://europepmc.org/article/MED/18614571https://pubmed.ncbi.nlm.nih.gov/15767874/https://pubmed.ncbi.nlm.nih.gov/15767874/http://koreascience.or.kr/article/JAKO201510665813355.pagehttp://koreascience.or.kr/article/JAKO201510665813355.pagehttps://pubmed.ncbi.nlm.nih.gov/16124204/https://pubmed.ncbi.nlm.nih.gov/16124204/https://pubmed.ncbi.nlm.nih.gov/16124204/https://pubmed.ncbi.nlm.nih.gov/16124204/https://onlinelibrary.wiley.com/doi/full/10.1111/cxo.12496https://onlinelibrary.wiley.com/doi/full/10.1111/cxo.12496https://onlinelibrary.wiley.com/doi/full/10.1111/cxo.12496https://pubmed.ncbi.nlm.nih.gov/20500851/https://pubmed.ncbi.nlm.nih.gov/20500851/https://pubmed.ncbi.nlm.nih.gov/20500851/https://pubmed.ncbi.nlm.nih.gov/26244865/https://pubmed.ncbi.nlm.nih.gov/26244865/https://pubmed.ncbi.nlm.nih.gov/26244865/https://pubmed.ncbi.nlm.nih.gov/6507580/https://pubmed.ncbi.nlm.nih.gov/6507580/http://aes.amegroups.com/article/view/3639/htmlhttp://aes.amegroups.com/article/view/3639/htmlhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC1324705/https://pubmed.ncbi.nlm.nih.gov/12637833/https://pubmed.ncbi.nlm.nih.gov/12637833/https://pubmed.ncbi.nlm.nih.gov/12637833/http://ikeyes.blogspot.com/2010/12/evaluation-of-case-of-concomitant.html.http://ikeyes.blogspot.com/2010/12/evaluation-of-case-of-concomitant.html.https://books.google.co.in/books/about/Diagnostic_Procedures_in_Ophthalmology.html?id=ksIDBAAAQBAJ&redir_esc=yhttps://books.google.co.in/books/about/Diagnostic_Procedures_in_Ophthalmology.html?id=ksIDBAAAQBAJ&redir_esc=yhttps://www.aao.org/bcscsnippetdetail.aspx?id=c964238e-4121-4346-90e2-043186bb1869.https://www.aao.org/bcscsnippetdetail.aspx?id=c964238e-4121-4346-90e2-043186bb1869.https://www.semanticscholar.org/paper/COMPARISON-OF-FOUR-DISSOCIATED-PHORIA-TESTS-%3A-%26-Goss-Ph./9e3b1b580460a9ee9333750def08cc9348bbeaa5https://www.semanticscholar.org/paper/COMPARISON-OF-FOUR-DISSOCIATED-PHORIA-TESTS-%3A-%26-Goss-Ph./9e3b1b580460a9ee9333750def08cc9348bbeaa5https://www.semanticscholar.org/paper/COMPARISON-OF-FOUR-DISSOCIATED-PHORIA-TESTS-%3A-%26-Goss-Ph./9e3b1b580460a9ee9333750def08cc9348bbeaa5https://europepmc.org/article/med/900610https://europepmc.org/article/med/900610https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374399/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374399/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374399/https://pubmed.ncbi.nlm.nih.gov/8524567/https://pubmed.ncbi.nlm.nih.gov/8524567/https://pubmed.ncbi.nlm.nih.gov/8524567/https://link.springer.com/chapter/10.1007/978-4-431-66959-3_11https://link.springer.com/chapter/10.1007/978-4-431-66959-3_11https://link.springer.com/chapter/10.1007/978-4-431-66959-3_11https://pubmed.ncbi.nlm.nih.gov/3557879/https://pubmed.ncbi.nlm.nih.gov/3557879/
Effectiveness of Unilateral or Alternating Methods Employed to
Measure Phoria When Targets Get DeviaAbstractIntroductionMaterials
& Methods ResultsTable 1Table 2Table 3DiscussionFigure 1Figure
2ConclusionReferences