Embed Size (px)
DESCRIPTION
Preserving Pulp Vitality
Citation preview
DENTAL HEALTH26 27Volume 52 No 2 of 6 March 2013
CLINICAL
Preserving pulp vitalityUdita Patel and Jennifer Hughes
KEY WORDS: Dentine-pulp complex • Vital pulp therapy • Pulpotomy • Biocompatibility
Pulp exposure from caries, trauma or tooth cavity preparation can be severe and lead to pain and/or infection, resulting in either root canal treatment or an extraction: both conditions are unfavourable, for various reasons. An alternative treatment could be a vital pulp capping procedure.
Restorative therapy The goals of restorative therapy are to restore the tooth to proper form and function, minimise post operative sensitivity and preserve pulp vitality. However, cavity preparation and restoration variables have an uncertain relationship to pulp injury and repair responses, thereby threatening tooth vitality.
Clinicians are keen to preserve the pulpally involved tooth: pulp tissue has an innate capacity for repair in the absence of microbial contamination. Vital pulp therapy is broadly defined as treatment to preserve and maintain pulp tissue in a tooth that has been compromised by caries, trauma, or restorative procedure. The objective is to stimulate the formation of reparative dentine to retain the tooth as a functional unit. This involves placing a medicament directly over exposed pulp or a cavity liner/sealant over residual caries in an attempt to give the pulp some time to ‘heal’, thereby maintaining vitality of that tooth. Immediate and long-term success of root canal treatment is widely accepted by clinicians but vital pulp capping is perhaps a less widely used procedure due to its controversial success rates 1.
There are many arguments about the best medicaments suitable for this role and their long term advantages and disadvantages. Pulp capping is a conservative dental treatment due to the regenerative nature of the dentine-pulp complex and its ability to secrete tertiary dentine. Research shows a higher failure rate for endodontically treated teeth. One of the reasons for this could be that a non-vital tooth requires 2.5 times more force than a vital tooth to register response2. The natural tooth tissues have an inherent capacity to withstand this load and hence the chances of
fracture in a root filled tooth are higher. Pulp vitality is imperative for the tooth viability, since it provides nutrition and detects pathogenic stimuli. Common clinical protocol is either a root canal treatment or extraction. Over time, the pulpless tooth, lacking proper blood supply and nervous system, becomes vulnerable to injury, increasing the interest in preserving pulp vitality.
Challenges Preservation of pulp vitality is a major challenge in restorative dentistry. The dentine pulp complex is uniquely capable of reparative responses to various environmental stimuli which determine much of the success of restorative work. The nature of protective response is determined by the type of cells involved. Injuries can range from tooth wear (including attrition, abrasion and erosion) which invokes a mild response, to extensive wear and dental caries which initiates a more substantial response. The odontoblasts which are responsible for dentinogenesis can either die due to the injurious stimuli or survive to initiate reparative tissue response3.
Particular growth factors from the TGF-ß (transforming growth factor- beta) family have the ability to initiate odontoblast differentiation and hence produce tertiary dentine by cell signalling. Odontoblast cells also line the pulp chamber and have long processes with the dentinal tubules around them, which are filled with tissue fluid containing plasma proteins. On exposure of the distal ends of these tubules, there is outward movement of tissue fluid which could result in pulpal inflammation, but its main aim is to prevent inward movement of toxins. Generally the greater the area of exposed dentine, the greater the effect on the pulp4.
The main aim of managing caries or any other damage to teeth should be to preserve pulp vitality. The best root canal ‘filling’ is healthy pulp tissue and it cannot be assumed that all damaged pulp must be extirpated or that all pulp conservation procedures are unsatisfactory. Cavity preparation is a minor procedure to clinicians, but it is a crisis to the dental pulp. For example, use of sharp, cutting burs can produce disturbances like vibrations and fluid shifts. Further outward fluid shifts are caused by application of bond, primer, varnishes, etc. which can cause pain to an un-anaesthetised patient and also inflame the pulp. On administration of local analgesia, fluid shifts still occur, but fewer nerves are affected which results in less inflammation of the pulp 5.
Dentine is the most effective protection for pulp due to its excellent insulation and capacity to reduce diffusion of chemicals from cavity floor to the pulp. However, it is possible to prepare cavities without pulpal inflammation or tertiary dentine production by using a combination of air-water spray, good lighting, intermittent cutting
forces and use of sufficiently sharp burs. In a prepared cavity, remaining dentine thickness of more than 0.5 mm is ideal for avoiding pulpal inflammation6. Reactionary dentine forms when remaining dentine thickness is 2.5- 0.01 mm due to presence of a layer of surviving odontoblasts in the area, whereas reparative dentine is formed following pulp exposure. Very deep cavities greatly reduce the number of surviving odontoblasts and hence none remain to secrete tertiary dentine. Remaining dentine thickness not only influences vitality of the underlying pulp tissue but also determines the repair response.
The distance of diffusion as determined by cavity preparation influences the signalling process of TGF-ß to lay down tertiary dentine. Unfortunately, too much tertiary dentine, reparative or reactionary, can very well cause ‘pulpal strangulations’, and in severe cases death. Yet another reason for practising minimally invasive dentistry in order to least traumatise the healthy tissues. Pulpal cell death can also be avoided by the use of a lining agent to reduce secretion of reactionary dentine.
Healing of an exposed pulp depends on the success of vital pulp therapy. Failed pulp treatment can principally be attributed to factors like bacterial microleakage, biocompatibility of the material and moisture contamination. Extent of pulp injury, cavity preparation, formation of tertiary dentine, open tooth apex, lack of pre existing symptoms, patient’s age etc. are the other aspects which can cumulatively contribute to the success or failure of the procedure. Very few dental materials are truly inert and tend to bring about a variety of physiochemical and biological changes in the dental tissues, healthy or otherwise. The interaction, effects of, and problems associated with these restorative materials
like bacterial microleakage, biocompatibility, etc. are important when considering saving pulp vitality.
Techniques Techniques to avoid extensive treatment such as extraction or endodontic therapy include direct pulp capping, indirect pulp capping and partial/full pulpotomy.
The main aim of lining and base materials used in pulp capping procedures
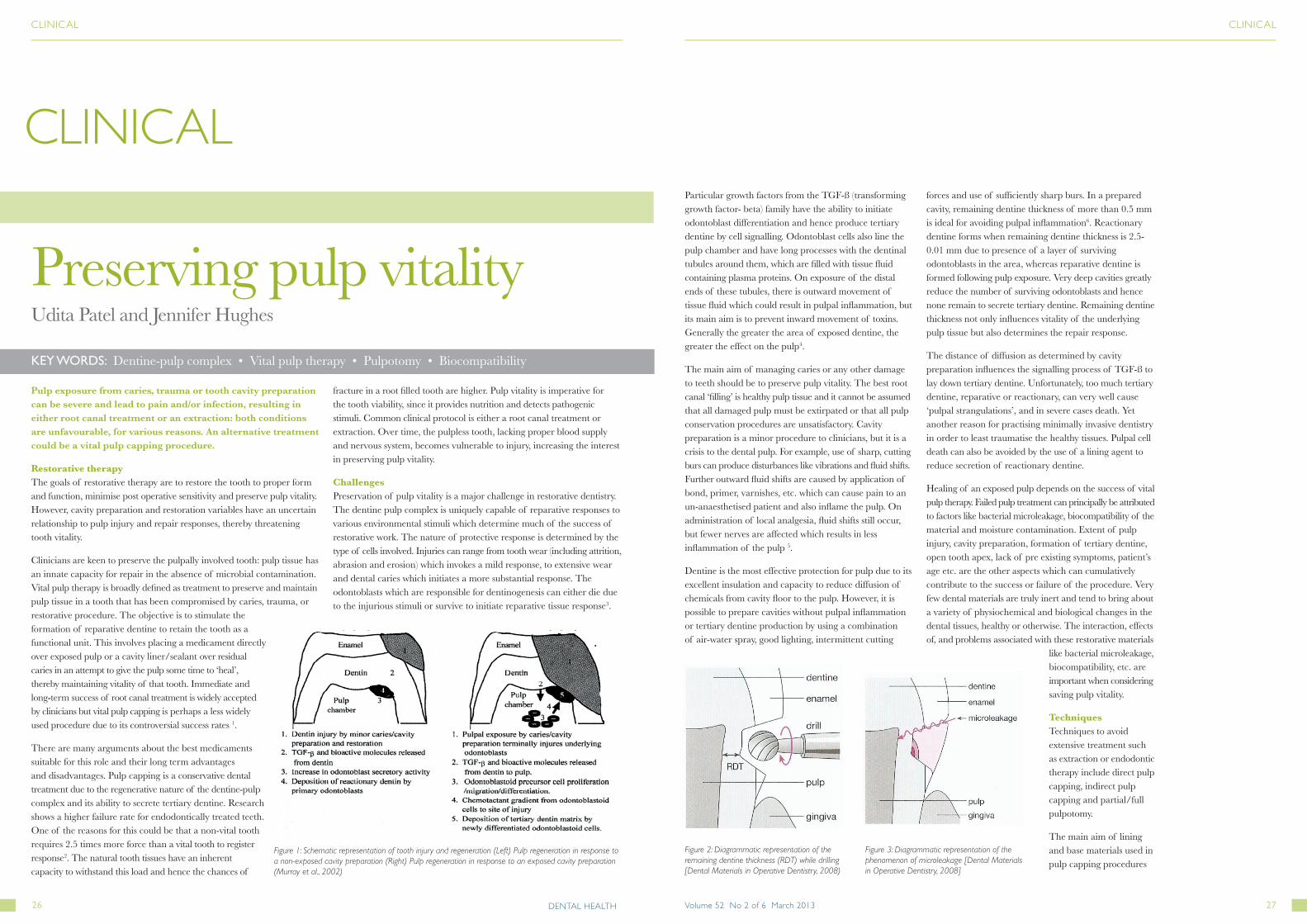
Figure 1: Schematic representation of tooth injury and regeneration (Left) Pulp regeneration in response to a non-exposed cavity preparation (Right) Pulp regeneration in response to an exposed cavity preparation (Murray et al., 2002)
Figure 2: Diagrammatic representation of the remaining dentine thickness (RDT) while drilling [Dental Materials in Operative Dentistry, 2008)
Figure 3: Diagrammatic representation of the phenomenon of microleakage [Dental Materials in Operative Dentistry, 2008]
CLINICALCLINICAL

DENTAL HEALTH28 29Volume 52 No 2 of 6 March 2013
is to prevent or retard pulpal inflammation. The other purposes depend on the material used. Dentine is probably the best lining material for pulp protection and maintenance of vitality as it is capable of preventing toxic substances from infiltrating the pulp. The thicker the remaining dentine, the better its protection ability will be. Historically, it was believed that restorative materials themselves were harmful to pulp and for this reason, use of bases or liners was considered imperative to protect pulp vitality and ensure successful restorations. In light of the knowledge of the importance of remaining dentine thickness, it is essential that sound dentine is never removed in order to accommodate for a lining, base or sealer material.
New materials Some common materials currently used in clinical practice are calcium hydroxide, mineral trioxide aggregate (MTA), zinc-oxide eugenol (ZOE), adhesive cements, glass ionomer and resin modified glass ionomer cements.
All current materials used for vital pulp therapies have at least one or more disadvantages. The field of dentistry is constantly evolving and scientists are always trying to find a better alternative to the current materials on the market. Two of the most promising materials include Biodentine™ and propolis.
Calling it ‘the next big thing in dentistry’, Septodont launched Biodentine™ in September 2010. This new experimental material is a Ca3SiO5 (calcium silicate) based Portland cement. Being a Portland cement (similar to MTA) it is biocompatible and bioactive in nature; and
has the ability to initiate the formation of dentine bridges (probably due to the presence of calcium hydroxide in its formulation). An experiment of damaged pulp fibroblasts was conducted to test for bioactivity. Of all the materials tested, only ProRoot® MTA and Biodentine™ were able to stimulate the formation of tertiary dentine. Both displayed presence of enhanced levels of TGF-ß. Biodentine™ also showed presence of other growth hormones (in addition to TGF-ß) which contribute to the formation of dentine bridges7.
Another study of indirect pulp capping on rat molars concluded that Biodentine™ was able to stimulate (thick and dense) reactionary dentine formation, which stopped after about three months when a sufficient dentine barrier was formed. Studies conducted to test Biodentine™ for application as a direct pulp capping agent and for pulpotomy showed that it was well tolerated even when in direct contact with the pulp. It was even suggested that the quality of dentine bridges formed were better than those formed by calcium hydroxide alone8, 9.
A three year study concluded that it is suitable as a dentine substitute, a pulp capping material and a bulk restorative material at the same time. They confirmed that it has the two main important qualities for a dentine substitute; biocompatibility and longevity. If a later re-intervention is required (due to marginal leakage or secondary caries), Biodentine™ is safe to retain as a lining and does not interfere with other adhesive fillings. Additionally, it does not
require any preliminary conditioning treatment of the cavity, greatly simplifying the pulp capping techniques 10.
Biodentine™ adheres to tooth surface by micromechanical adhesion. Its crystals succeed in growing within the dentine tubules leading to a micromechanical anchor, without the application of a conditioning treatment or bonding material. It is also suggested that there might be a possible ion exchange contributing to further adhesion of the cement giving it outstanding resistance to microleakage and bacterial infiltration11. Drawbacks of Biodentine™ include mixing two separate components which can prove to be a hassle, its high cost and the fact that the patient needs to be called back for another appointment. Its use is still not indicated for use in root caries and still requires more research in the area.
Propolis is a non-toxic resinous glue collected by Apis Mellifera honey bees from various plant juices. Propolis was historically used in folk medicine especially to treat battle wounds. Hippocrates, the founder of modern medicine, used it for healing sores and ulcers.
A review article suggested various applications of Propolis in dentistry, such as in wound healing, as a cariostatic agent and as alternative treatments for dentine hypersensitivity, among others 12. As a pulp capping agent, flavonoids and caffeic acid found in Propolis reduce the inflammatory response and aid the immune system by promoting phagocytic activities and stimulating cellular immunity. It also successfully aids dentine bridge formation as a result of the presence of arginine, vitamin C, provitamin A and B complex, factors which also contribute to wound healing. A study concluded that Propolis was an effective alternative measure to prevent dental caries since its antimicrobial activity is effective against Steptococcus mutans, commonly associated with dental caries. Enterococcus faecalis a gram positive, facultative anaerobic has the ability to invade dentinal tubules and it was found that the antimicrobial activity of Propolis against E. faecalis, was just as effective as Chlorhexidine. 10% Propolis gel (as opposed to 30%) was suggested to be as effective as fluoride gel in reducing dentine permeability (and hence hypersensitivity) by partial obliteration and sealing of dentinal tubules13, 14, 15.
Conclusion It would appear that there are now alternative materials, for maintaining pulp vitality during restorative procedures, to the tried and tested ‘gold standard’ calcium hydroxide. Some of these, such as Biodentine™ or Propolis would seem to present clinicians with an advantage during pulp capping procedures. Clinical Implementation of Biodentine as suggested in the brochure by Septodont UK in 2011
BiodentineTM labelled with fluorescein dye which has moved from the cement into the dentine tubules. Notice the plugs of material in the tubule openings (Picture taken from the Biodentine™ brochure UK 2011- original courtesy Dr Amre Atmeh, King’s College London)
Raw, dried Propolis (www.healthywealthyyou.org, accessed in October 2011)
Acknowledgements With thanks to my supervisor and co-author Dr. Jennifer Hughes BDS, FDS RCS (Eng) Director of Hygiene & Therapy School of Dental Hygiene & Therapy Dental Institute, 3rd Floor Dental Extension, Caldecot Road, London.
References 1. Swift JR., Edward J., Trope M, Ritter A.. Vital pulp therapy for the mature tooth- can it work? Endodontic Topics. 2003; 5(1): 49-56.
2. Dunitz M (2000). Tooth Wear and Sensitivity: Clinical advances in Restorative Dentistry. London: Blackwell Science Inc.
3. Chong, B.S. (ed.). (2010). Maintaining dental pulp vitality. In: Harty’s Endodontics in Clinical Practice, Churchill Livingstone Elsevier Ltd.
4. Pashley, DH. Dynamics of the Pulpo-Dentin Complex. Crit Rev Oral Biol Med 1996;. 7(2): 104-33.
5. Murray PE., Smith AJ, Windsor LJ Mjor IA. Remaining dentine thickness and human pulp responses. Int Endodon J.2003; 36(1): 33-43.
6. Stanley HR. Pulp capping: Conserving the dental pulp - Can it be done? Is it worth it?. Oral Surg Oral Med Oral Pathol. 1989; 68(5): 628-39.
7. About, I. (2011). Effets des matériaux bioactifs Biodentine TM et Calcipulpe® sur les étapes. London, UK: Septodent UK- R&D Department.
8. Goldberg, M. (2009). Etude PC08-002. RD 94 après implantation à 3 mois dans la première. Report RD EN RA EXT-RD 94 106. London, UK: Septodent R&DDepartment.
9. Shayegan A. (2009). RD 94. Etude n PC08-001. Etude de RD 94 comme agent pulpaire dans le cadre de pulpotomie et coiffage direct sur les dents lactéales de cochon. Septodent R&D Department.
10. Koubi, G.F., Franquin, JC, Colon P (2009). A Clinical Study of a New CA3Si5-based Material Indicated as a Dentine Substitute. In: Conseuro. Seville, Spain: Septodent, UK.
11. Septodont. 2011. Biodentine™- Active Biosilicate Technology™. London, United Kingdom.
12. Parolia, AM. Kudabala, N. Rao N et al. A comparative histological analysis of human pulp following direct pulp capping with Propolis, Mineral Trioxide Aggregate and Dycal. Austra Dent J .2010; 55(1): 59-64.
13. Duailibe, SA, Goncalves AG, Mendes FJ.. Effect of Propolis extract on Streptococcus Mutans counts in vivo. J Applied Oral Science 2007. 15(5): 420-430.
14. Kayaoglu G, Omurlu H, Akca G et al. Antibacterial Activity of Propolis versus Conventional Endodontic Disinfectants against Enterococcus faecalis in Infected Dentinal Tubules. J Endodont. 2011; 37(3): 376-81.
15. De Carvalho Sales-Peres, SH, De Carvalho FN, Marsicano JA et al. 2011. Effect of propolis gel on the in vitro reduction of dentin permeability. J Applied Oral Scien. 2011; 19(4): .318-23.
About the author: Udita qualified as a dental hygienist and therapist from King’s College Hospital. She also has an engineering degree in Dental Materials from Queen Mary- University of London. This project combined knowledge from both disciplines and hence inspired her to research the subject further. Udita currently works as a dental therapist in Smileright™ at Boots stores.
Address for correspondence: [email protected]
CLINICALCLINICAL
Preserving pulp vitality





























