Embed Size (px)
Citation preview

Number: Dent 44 Date: October 3, 2011 Page: 1 of 1
Subject: Cleft Palate Dental Indemnity Program – fee increase retroactive to April 1, 2010
Reference: Schedule of Cleft Palate Dental Indemnity Program Benefits
To: all dentists and billing staff A three-year funding increase of 5.5% per year has been applied to benefits payable under the Cleft Palate Dental Indemnity Program, retroactive to April 1, 2010. This Program provides funding for Albertans under the age of 25 years, who are born with a congenital cleft palate and who, as a result, require uninsured dental services. Under this Program, benefits are payable for dental services such as radiographs, restorations, extractions, orthodontics, crowns, bridges and dental implants. Eligible services are paid on a fee-for-service basis up to a maximum amount as listed in the Program’s benefits schedule. The following documents are enclosed for your reference:
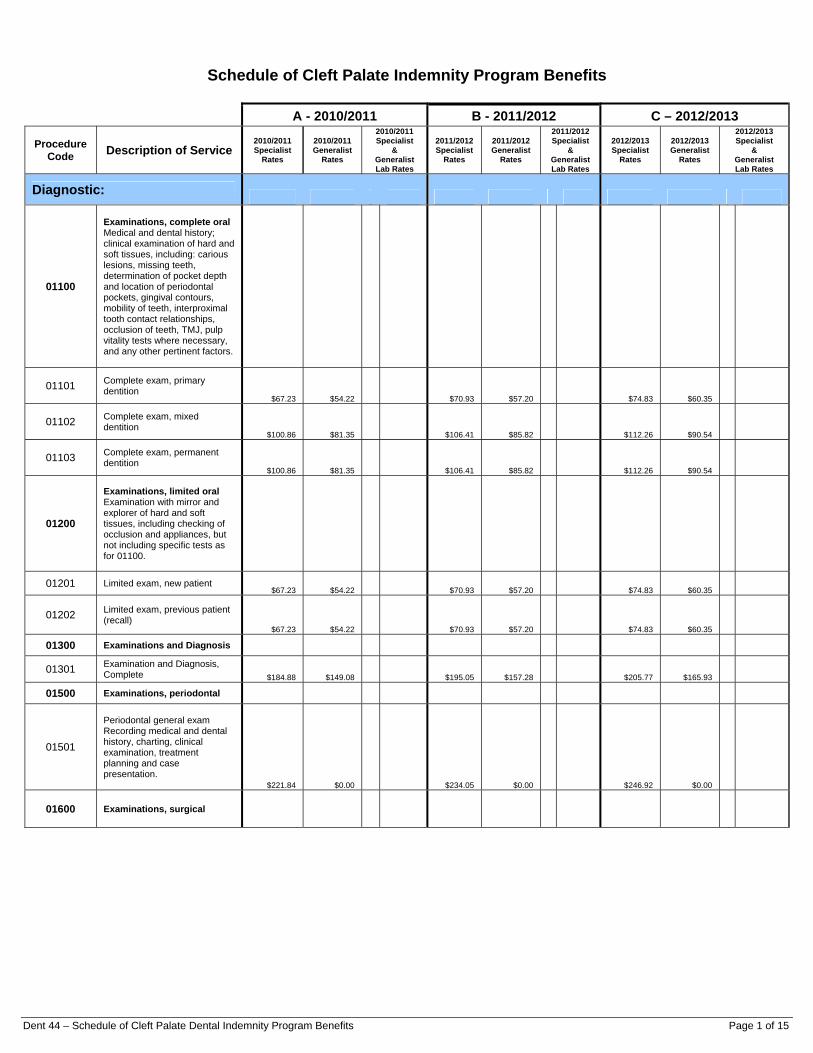
The Schedule of Cleft Palate Dental Indemnity Program Benefits, which includes the rates effective April 1, 2010 to March 31, 2011 (column A), April 1, 2011 to March 31, 2012 (column B), and April 1, 2012 to March 31, 2013 (column C).
The Cleft Palate Dental Indemnity Program Fee Guidelines which apply to services provided on or after April 1, 2010.
Alberta Health Services is responsible for managing and administering the Program for eligible patients who are registered with the Cleft Palate Clinic at the Stollery Children’s Hospital in Edmonton, or the Alberta Children’s Hospital in Calgary. Any inquiries about the Program, including claim processing and payments, should be directed to Alberta Health Services at:
Analyst/Program Coordinator Cleft Palate Dental Indemnity Program Alberta Children’s Hospital 2888 Shaganappi Trail NW Calgary AB T3B 6A8 Telephone: 403-955-2528 Toll-free: 1-866-218-7811 Fax: 403-955-7799
Contact: Innovative Compensation Branch
Telephone: Edmonton 780-415-1475 Toll free 310-0000
Fax: 780-422-5208
Approval: original signed by Yolanda Lackie
Position: Executive Director Innovative Compensation Branch
Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 1 of 15
Schedule of Cleft Palate Indemnity Program Benefits
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
Diagnostic:
01100
Examinations, complete oral Medical and dental history; clinical examination of hard and soft tissues, including: carious lesions, missing teeth, determination of pocket depth and location of periodontal pockets, gingival contours, mobility of teeth, interproximal tooth contact relationships, occlusion of teeth, TMJ, pulp vitality tests where necessary, and any other pertinent factors.
01101 Complete exam, primary dentition
$67.23 $54.22 $70.93 $57.20 $74.83 $60.35
01102 Complete exam, mixed dentition
$100.86 $81.35 $106.41 $85.82 $112.26 $90.54
01103 Complete exam, permanent dentition
$100.86 $81.35 $106.41 $85.82 $112.26 $90.54
01200
Examinations, limited oral Examination with mirror and explorer of hard and soft tissues, including checking of occlusion and appliances, but not including specific tests as for 01100.
01201 Limited exam, new patient $67.23 $54.22 $70.93 $57.20 $74.83 $60.35
01202 Limited exam, previous patient (recall)
$67.23 $54.22 $70.93 $57.20 $74.83 $60.35
01300 Examinations and Diagnosis
01301 Examination and Diagnosis, Complete $184.88 $149.08 $195.05 $157.28 $205.77 $165.93
01500 Examinations, periodontal
01501
Periodontal general exam Recording medical and dental history, charting, clinical examination, treatment planning and case presentation.
$221.84 $0.00 $234.05 $0.00 $246.92 $0.00
01600 Examinations, surgical

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 2 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
01601
Surgical general exam Recording medical and dental history, may include in-depth analysis of medical status, medication, anaesthetic and surgical risk, initial consultation with referring dentist or physician, parent or guardian, evaluation of source of chief complaint, evaluation of pulp vitality, mobility of teeth, occlusal factors, TMJ, or where the patient is to be admitted to hospital for dental procedures.
$147.90 $0.00 $156.03 $0.00 $164.61 $0.00
01602 Surgical specific exam
$73.95 $0.00 $78.02 $0.00 $82.31 $0.00
01700 Examinations, prosthodontic
01701 Prosthodontic general exam $100.86 $0.00 $106.41 $0.00 $112.26 $0.00
01702 Prosthodontic specific exam $67.23 $0.00 $70.93 $0.00 $74.83 $0.00
01703
Examination and Diagnosis, Prosthodontic, Fixed Oral Rehabilitation, to include: (a) History, Medical and Dental (b) Clinical Examination of Hard and Soft Tissues, including carious lesions, missing teeth, determination of sulcular depth, gingival contours, mobility of teeth, interproximal tooth contact relationships, occlusion of teeth, TMJ, pulp vitality test/analysis, where necessary and any other pertinent factors. (c) Evaluation of specific sites for implant supported or retained prosthesis; (d) Radiographs extra, as required. $124.81 $0.00 $131.67 $0.00 $138.92 $0.00
01800 Examinations, endodontic
01801
Endodontic general exam Examination and/or complicated diagnosis. May include vitality tests, thermal test, cracked tooth tests, occlusal exams, percussion, palpation, transillumination, anaesthetic tests and mobility tests. $147.90 $0.00 $156.03 $0.00 $164.61 $0.00
01802 Endodontic specific exam $73.95 $0.00 $78.02 $0.00 $82.31 $0.00
01900 Examinations, orthodontic
01901
Orthodontic general exam To include the following: diagnostic models, complete intraoral radiograph series or panoramic film, cephalograms, facial and intraoral photographs, consultations and case presentation. $369.75 $0.00 L $178.91 $390.09 $0.00 L $188.75 $411.55 $0.00 L $199.13
01902 Orthodontic specific exam $73.95 $0.00 $78.02 $0.00 $82.31 $0.00
02000
Radiographs (including radiographic examination and interpretation)
02111 Periapical radiograph - One film $26.85 $21.65 $28.33 $22.85 $29.89 $24.10
02112 Periapical radiograph - Two films $44.72 $36.07 $47.18 $38.05 $49.78 $40.14

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 3 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
02113 Periapical radiograph - Three films $62.65 $50.52 $66.10 $53.30 $69.73 $56.23
02131 Occlusal radiograph - One film $44.72 $36.07 $47.18 $38.05 $49.78 $40.14
02601 Panoramic radiograph - One film $89.50 $72.19 $94.43 $76.16 $99.62 $80.35
02701 Cephalometric radiograph - One film $107.09 $86.36 $112.98 $91.11 $119.19 $96.12
02702 Cephalometric radiograph - Two films $167.92 $135.43 $177.16 $142.87 $186.90 $150.73
02751 Cephalometric tracing and interpretation - One unit of time
$73.95 $59.64 $78.02 $62.92 $82.31 $66.38
02752 Cephalometric tracing and interpretation - Two units of time
$147.90 $119.27 $156.03 $125.83 $164.61 $132.75
02801 Interpretation of radiographs from another source - One unit of time
$70.59 $56.94 $74.47 $60.07 $78.57 $63.37
02921 Radiograph - hand and wrist - per case $107.09 $86.36 $112.98 $91.11 $119.19 $96.12
02931 Single view $90.37 $72.88 $95.34 $76.89 $100.58 $81.12
02932 Radiographs, two views $167.97 $135.45 $177.21 $142.90 $186.96 $150.76
04700 Interpretation of models from another source
04722 Wax-up, Diagnostic, two units $134.48 $108.45 L $65.07 $141.88 $114.41 L $68.65 $149.68 $120.70 L $72.42
04741 First unit of time $63.89 $51.52
$67.41 $54.36
$71.11 $57.35
04800 Photographs, diagnostic
04801 Single photo $15.97 $12.88 $16.85 $13.59 $17.77 $14.34
04802 Two photos $31.94 $25.75 $33.70 $27.17 $35.55 $28.66
04803 Three photos $47.91 $38.64 $50.54 $40.76 $53.32 $43.01
04809 Each additional photo over three $15.97 $12.88 $16.85 $13.59 $17.77 $14.34
04900 Casts, diagnostic
04911 Un-mounted $63.89 $51.52 L $30.91 $67.41 $54.36 L $32.61 $71.11 $57.35 L $34.41
04921 Mounted $95.83 $77.28 L $46.37 $101.10 $81.53 L $48.92 $106.66 $86.01 L $51.61
04922 Mounted using face bow transfer $127.77 $103.04 L $61.83 $134.80 $108.71 L $65.23 $142.21 $114.69 L $68.81
04931 Orthodontic casts $127.77 $103.04 L $61.83 $134.80 $108.71 L $65.23 $142.21 $114.69 L $68.81
05100
Treatment planning This service is only for extra time spent on unusually complicated cases.
05101 One unit of time $67.23 $54.22 $70.93 $57.20 $74.83 $60.35
05102 Two units of time $134.48 $108.46 $141.88 $114.42 $149.68 $120.72
05103 Three units of time $201.72 $162.68 $212.81 $171.63 $224.52 $181.07
05109 Treatment planning-each additional unit over four $67.23 $54.22
$70.93 $57.20 $74.83 $60.35
05200 Consultation, with patient
05201 One unit of time $67.23 $54.22 $70.93 $57.20 $74.83 $60.35
05202 Two units of time $134.48 $108.46 $141.88 $114.42 $149.68 $120.72
Preventive:
11100 Polishing
11101 One unit of time $63.67 $51.34 $67.17 $54.17 $70.87 $57.15

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 4 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
11110 Scaling
11111 One unit of time $67.00 $54.03 $70.69 $57.01 $74.58 $60.14
11112 Two units of time $134.00 $108.08 $141.38 $114.03 $149.15 $120.30
11117 1/2 unit of time $28.37 $22.88 $29.93 $24.14 $31.58 $25.47
12100 Fluoride treatments
12101 Fluoride treatment - topical application $31.83 $25.67 $33.58 $27.08 $35.43 $28.57
13100 Nutritional counselling
13101 One unit of time $63.67 $51.34 $67.17 $54.17 $70.87 $57.15
13200 Oral hygiene instruction/plaque control
13211 One unit of time $63.67 $51.34
$67.17 $54.17 $70.87 $57.15
13400 Sealants, pit and fissure (acid etch preparation included)
13401 First tooth in quadrant $31.83 $25.67 $33.58 $27.08 $35.43 $28.57
13409 Each additional tooth in same quadrant $15.91 $12.84 $16.79 $13.55 $17.71 $14.29
13700 Disking of teeth, interproximal
13701 Disking of teeth - One unit of time $63.67 $51.34 $67.17 $54.17 $70.87 $57.15
14000 Control of oral habits
14101 Appliances, removable - maxillary $442.17 $356.58 L $213.95 $466.49 $376.19 L $225.71 $492.15 $396.88 L $238.13
14201 Appliances, fixed/cemented - maxillary $442.17 $356.58 L $213.95 $466.49 $376.19 L $225.71 $492.15 $396.88 L $238.13
15000
Space maintainers (including the design, separation, fabrication, insertion, and where applicable initial cementation and removal)
15101 Space maintainers - fixed unilateral $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15102 Space maintainers - fixed unilateral w/ intra alveolar attachments $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15103 Space maintainers - fixed bilateral $294.77 $237.72 L $142.63 $310.98 $250.79 L $150.48 $328.09 $264.59 L $158.75
15104 Space maintainers - fixed bilateral with teeth attached
$294.77 $237.72 L $142.63 $310.98 $250.79 L $150.48 $328.09 $264.59 L $158.75
15105 Space maintainers - fixed bilateral tubes and locking wire
$294.77 $237.72 L $142.63 $310.98 $250.79 L $150.48 $328.09 $264.59 L $158.75
15200 Space maintainers, stainless steel crown type
15201 Space maintainers, stainless steel crown type, fixed $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15202 Space maintainers, stainless steel crown type, fixed with intra alveolar attachments
$221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15400 Space maintainers, acrylic, removable
15401 Space maintainers - removable, bilateral clasps, retaining wires $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15402 Space maintainers - removable, bilateral clasps, retaining wires with teeth $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
15403 Space maintainers - removable, no clasps $221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 5 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
15500 Space maintainers, acid etched, pontic type
15501 Space maintainers - acid etched, pontic type
$221.08 $178.29 L $106.97 $233.24 $188.09 L $112.86 $246.07 $198.44 L $119.06
Restorative:
20100 Caries, trauma and pain control
20110
Caries, trauma and pain control - removal of carious lesions or existing restorations and placement of a sedative/protective dressing, includes pulp caps when necessary, as a separate procedure
20111 First tooth $152.60 $123.07 $161.00 $129.84 $169.85 $136.98
20119 Each additional tooth in same quadrant $152.60 $123.07 $161.00 $129.84 $169.85 $136.98
20120
Caries/trauma and pain control - same as 20110 with use of a band for retention and support, as a separate procedure
20121 First tooth $190.76 $153.84 $201.25 $162.31 $212.32 $171.23
20129 Each additional tooth in same quadrant $190.76 $153.84 $201.25 $162.31 $212.32 $171.23
20130 Trauma control, smoothing of fractured surfaces per tooth
20131 First tooth $36.34 $29.30 $38.34 $30.92 $40.45 $32.62
20139 Each additional tooth in same quadrant $36.34 $29.30 $38.34 $30.92 $40.45 $32.62
21100 Restoration, amalgam, primary teeth, non-bonded
21111 One surface $89.06 $71.82 $93.96 $75.77 $99.13 $79.94
21112 Two surfaces $130.91 $105.57 $138.11 $111.38 $145.71 $117.51
21113 Three surfaces $168.31 $135.74 $177.57 $143.21 $187.34 $151.08
21114 Four surfaces $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
21115 Five/max. surfaces $224.42 $180.98 $236.77 $190.94 $249.79 $201.44
21120 Restorations, amalgam, primary teeth, bonded
21121 One surface $106.88 $86.20 $112.75 $90.94 $118.96 $95.94
21122 Two surfaces $149.62 $120.65 $157.85 $127.29 $166.53 $134.29
21123 Three surfaces $187.02 $150.82 $197.31 $159.11 $208.16 $167.86
21124 Four surfaces $224.42 $180.98 $236.77 $190.94 $249.79 $201.44
21125 Five/max. surfaces $243.12 $196.07 $256.49 $206.86 $270.60 $218.24
21210 Restorations, amalgam, permanent bicuspids and anteriors, non bonded
21211 One surface $89.06 $71.82 $93.96 $75.77 $99.13 $79.94
21212 Two surfaces $130.91 $105.57 $138.11 $111.38 $145.71 $117.51
21213 Three surfaces $168.31 $135.74 $177.57 $143.21 $187.34 $151.08
21214 Four surfaces $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
21215 Five/max. surfaces $224.42 $180.98 $236.77 $190.94 $249.79 $201.44

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 6 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
21230 Restorations, amalgam, bonded, permanent bicuspids and anteriors
21231 One surface $106.88 $86.20 $112.75 $90.94 $118.96 $95.94
21232 Two surfaces $149.62 $120.65 $157.85 $127.29 $166.53 $134.29
21233 Three surfaces $187.02 $150.82 $197.31 $159.11 $208.16 $167.86
21234 Four surfaces $224.42 $180.98 $236.77 $190.94 $249.79 $201.44
21235 Five/max. surfaces $243.12 $196.07 $256.49 $206.86 $270.60 $218.24
21300 Restorations, amalgam cores
21301 Non-bonded, in conjunction with crown $187.02 $150.82 $197.31 $159.11 $208.16 $167.86
21302 Bonded, in conjunction with crown $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
21400
Pins, retentive, per restoration (for amalgams and tooth coloured restorations)
21401 One pin $27.62 $22.28 $29.14 $23.51 $30.75 $24.80
21402 Two pins $41.43 $33.41 $43.71 $35.24 $46.11 $37.18
21403 Three pins $55.25 $44.55 $58.29 $47.00 $61.49 $49.58
21404 Four pins $69.05 $55.69 $72.85 $58.75 $76.86 $61.98
21405 Five pins or more $82.87 $66.83 $87.43 $70.50 $92.24 $74.38
21500
Restorations made to a tooth supporting an existing partial denture clasp (additional to restoration)
21501 Per restoration $69.05 $55.69 $72.85 $58.75 $76.86 $61.98
22200 Restorations, prefabricated, full coverage
22201 Primary anterior $168.31 $135.74 $177.57 $143.21 $187.34 $151.08
22202 Primary anterior - open face $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
22300 Restorations, prefabricated, metal, permanent teeth
22301 Permanent anterior $224.42 $180.98 $236.77 $190.94 $249.79 $201.44
22302 Permanent anterior - open face $261.83 $211.15 $276.23 $222.76 $291.42 $235.02
22400 Restorations, prefabricated, plastic, primary teeth
22401 Restorations, prefabricated, plastic, primary anterior tooth
$152.60 $123.07 $161.00 $129.84 $169.85 $136.98
22500 Restorations, prefabricated, plastic, permanent teeth
22501 Permanent anterior $209.83 $169.22 $221.37 $178.53 $233.55 $188.35
23110 Restorations, tooth coloured, permanent anteriors, acid etch/bond technique
23111 One surface $130.91 $105.57 $138.11 $111.38 $145.71 $117.51
23112 Two surfaces $149.62 $120.65 $157.85 $127.29 $166.53 $134.29
23113 Three surfaces $168.31 $135.74 $177.57 $143.21 $187.34 $151.08
23114 Four surfaces $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
23115 Five/max. surfaces $243.12 $196.07 $256.49 $206.86 $270.60 $218.24
23120 Restorations, tooth coloured, veneer applications
23122 Non prefabricated direct build-up - acid etch/bond $317.94 $256.39 $335.42 $270.49 $353.87 $285.37

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 7 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
23123 Diastema closure, interproximal only, acid etch/bond
$243.12 $196.07 $256.49 $206.86 $270.60 $218.24
23410 Restorations, tooth coloured, primary, anterior, acid etch/bond technique
23411 One surface $130.91 $105.57 $138.11 $111.38 $145.71 $117.51
23412 Two surfaces $149.62 $120.65 $157.85 $127.29 $166.53 $134.29
23413 Three surfaces $168.31 $135.74 $177.57 $143.21 $187.34 $151.08
23414 Four surfaces $205.72 $165.91 $217.03 $175.03 $228.97 $184.66
23415 Five/max. surfaces $243.12 $196.07 $256.49 $206.86 $270.60 $218.24
25700 Posts
25711 Single section $304.30 $245.41 L $147.24 $321.04 $258.90 L $155.34 $338.70 $273.14 L $163.89
25712 Two sections $380.38 $306.75 L $184.05 $401.30 $323.62 L $194.17 $423.37 $341.42 L $204.85
25713 Three sections $456.45 $368.11 L $220.86 $481.55 $388.35 L $233.01 $508.04 $409.71 L $245.83
25720 Posts, cast metal (including core) concurrent with impression for crown
25721 Single section $152.14 $122.70 L $73.62 $160.51 $129.45 L $77.67 $169.34 $136.57 L $81.94
25722 Two sections $228.22 $199.14 L $119.48 $240.77 $210.09 L $126.05 $254.01 $221.64 L $132.99
25723 Three sections $304.30 $245.41 L $147.24 $321.04 $258.90 L $155.34 $338.70 $273.14 L $163.89
25724 Post, cast as part of a crown $152.14 $122.70 L $73.62 $160.51 $129.45 L $77.67 $169.34 $136.57 L $81.94
25730 Post, prefabricated retentive
25731 One post $114.12 $92.02 $120.39 $97.08 $127.01 $102.42
25732 Two posts $228.22 $184.05 $240.77 $194.17 $254.01 $204.85
25733 Three posts $342.33 $276.07 $361.16 $291.25 $381.03 $307.27
27110 Crowns, plastic, processed
27111 Crown, plastic - processed $608.59 $490.80 L $294.48 $642.07 $517.79 L $310.67 $677.38 $546.27 L $327.76
27120 Crowns, plastic, direct
27121 Crown, plastic - direct/transitional (chair-side)
$114.12 $92.02 $120.39 $97.08 $127.01 $102.42
27200 Crowns, porcelain/ceramic
27201 Crown, porcelain/ceramic jacket $820.33 $661.55 L $396.93 $865.45 $697.93 L $418.76 $913.05 $736.32 L $441.79
27211 Crown, porcelain fused to metal base $820.33 $661.55 L $396.93 $865.45 $697.93 L $418.76 $913.05 $736.32 L $441.79
27212 Crown, porcelain/ceramic $1,418.94 $1,064.21 L $638.52 $1,496.98 $1,122.74 L $673.64 $1,579.32 $1,184.49 L $710.69
27213 Crown, porcelain fused to metal base, screwed directly to implant
$1,647.56 $1,328.68 L $797.21 $1,738.18 $1,401.75 L $841.05 $1,833.77 $1,478.85 L $887.31
27215 Crown, porcelain/ceramic fused to metal base $1,472.51 $1,104.38
L
$662.63 $1,553.50 $1,165.12 L $699.07 $1,638.94 $1,229.20 L $737.52
27300 Crowns, metal cast
27301 Crown, metal, full cast $820.33 $661.55 L $396.93 $865.45 $697.93 L $418.76 $913.05 $736.32 L $441.79
27311 Crown, metal, 3/4 partial veneer $820.33 $661.55 L $396.93 $865.45 $697.93 L $418.76 $913.05 $736.32 L $441.79
27600 Veneers, laboratory processed
27601 Veneers, plastic, acid etch/bonded $608.59 $490.80 L $294.48 $642.07 $517.79 L $310.67 $677.38 $546.27 L $327.76

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 8 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
27602 Veneers, porcelain/ceramic, acid etch/bonded $608.59 $490.80 L $294.48 $642.07 $517.79 L $310.67 $677.38 $546.27 L $327.76
29300 Removal of inlay/on-lay/crown/veneer (single units only)
29301 One unit of time $76.07 $61.34 $80.26 $64.72 $84.67 $68.28
29302 Two units of time $152.14 $122.70 $160.51 $129.45 $169.34 $136.57
29303 Three units of time $228.22 $184.05 $240.77 $194.17 $254.01 $204.85
29304 Each additional unit over three $76.07 $61.34 $80.26 $64.72 $84.67 $68.28
Endodontic:
32230 Pulpotomy, primary teeth
32231 Primary tooth, as a separate procedure $115.77 $98.01 $122.14 $103.40 $128.85 $109.09
32310 Pulpectomy, permanent teeth/retained primary teeth
32311 One canal $91.15 $73.51 $96.16 $77.55 $101.45 $81.82
32320 Pulpectomy, primary teeth
32321 Anterior tooth $91.15 $73.51 $96.16 $77.55 $101.45 $81.82
33110
Root canals, permanent teeth/retained primary teeth - includes clinical procedures with appropriate radiographs, excluding final restoration
33111 One canal $626.93 $505.58 $661.41 $533.39 $697.79 $562.72
33121 Two canals $946.43 $763.26 $998.49 $805.24 $1,053.40 $849.52
Periodontics:
42200 Periodontal surgery, gingivoplasty
42201 Per sextant $227.57 $183.53 $240.09 $193.62 $253.29 $204.27
42500 Periodontal surgery, Grafts, Soft Tissue
42561 Grafts, Free Connective per site $764.50 $573.37
$806.54 $604.91 $850.90 $638.18
42581 Grafts, Gingival Onlay per site $764.50 $573.37
$806.54 $604.91 $850.90 $638.18
43400 Root planing, periodontal
43421 One unit of time $72.41 $58.39 $76.40 $61.61 $80.60 $64.99
43422 Two units of time $144.83 $116.79 $152.79 $123.21 $161.20 $129.99
Prosthodontics (removable):
51000
Denture, Complete (includes: impressions, initial & final jaw relation records, try-in evaluation & check records, insertion & adjustments, including three month post insertion care)
51101 Complete, standard denture, maxillary $700.39 $564.83 L $338.90 $738.92 $595.90 L $357.54 $779.56 $628.67 L $377.20
51102 Complete, standard denture, mandibular $700.39 $564.83 L $338.90 $738.92 $595.90 L $357.54 $779.56 $628.67 L $377.20
51701 Complete over-dentures - maxillary $700.39 $564.83 L $338.90 $738.92 $595.90 L $357.54 $779.56 $628.67 L $377.20
52100 Dentures, partial, acrylic base, without clasps (transitional)
52101 Maxillary $200.14 $161.40 L $96.84 $211.15 $170.28 L $102.17 $222.76 $179.65 L $107.79

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 9 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
52300 Dentures, partial, acrylic, with metal wrought/cast clasps and/or rests
52301 Maxillary $667.12 $538.00 L $322.80 $703.81 $567.60 L $340.56 $742.52 $598.81 L $359.29
53100 Dentures, partial, free end, cast frame/connector, clasps and rests
53101 Maxillary $700.39 $564.83 L $338.90 $738.92 $595.90 L $357.54 $779.56 $628.67 L $377.20
53200 Dentures, partial, tooth-borne, cast frame/connector, clasps and rests
53201 Partial dentures, tooth-borne, cast frame $700.39 $564.83 L $338.90 $738.92 $595.90 L $357.54 $779.56 $628.67 L $377.20
55400 Denture, repairs/additions, partial denture, impression required
55401 Maxillary $133.42 $107.61 L $64.56 $140.76 $113.52 L $68.11 $148.50 $119.77 L $71.86
56210 Dentures, reline, direct complete denture
56211 Maxillary $200.14 $161.40 L $96.84 $211.15 $170.28 L $102.17 $222.76 $179.65 L $107.79
56220 Denture, reline, direct, partial denture
56221 Maxillary $200.14 $161.40 L $96.84 $211.15 $170.28 L $102.17 $222.76 $179.65 L $107.79
56230 Denture, reline, processed, complete denture
56231 Maxillary $200.14 $161.40 L $96.84 $211.15 $170.28 L $102.17 $222.76 $179.65 L $107.79
56240 Denture, reline, processed, partial denture
56241 Maxillary $200.14 $161.40 L $96.84 $211.15 $170.28 L $102.17 $222.76 $179.65 L $107.79
56410 Denture, remake, using existing framework, partial denture
56411 Maxillary $400.28 $322.81 L $193.68 $422.29 $340.56 L $204.34 $445.52 $359.29 L $215.57
57200 Prosthesis, maxillofacial, obturators
57204 Obturator, Temporary palatal (prosthesis extra) $900.06 $0.00 L $540.10 $949.57 $0.00 L $569.81 $1,001.79 $0.00 L $601.15
57300 Prosthesis, maxillofacial, other
57301 Velar bulb (prosthesis and obturator extra) $900.06 $725.86 L $435.52 $949.56 $765.78 L $459.47 $1,001.79 $807.90 L $484.74
57311 Feeding appliance (for infants with cleft palate)
$900.06 $725.86 L $435.52 $949.56 $765.78 L $459.47 $1,001.79 $807.90 L $484.74
57371 Palatal life prosthesis, modification (relines or repairs)
$630.04 $508.11 L $304.86 $664.69 $536.05 L $321.63 $701.25 $565.53 L $339.32
Prosthodontics (fixed):
62500 Pontics, porcelain
62501 Pontics, porcelain fused to metal $408.13 $329.13 L $197.48 $430.57 $347.23 L $208.34 $454.25 $366.33 L $219.80
62502 Pontics, porcelain, aluminous $408.13 $329.13 L $197.48 $430.57 $347.23 L $208.34 $454.25 $366.33 L $219.80
67140 Retainers, plastic/acrylic, indirect, processed to metal, attached to implants
67141 First implant $1,088.31 $877.68 L $526.61 $1,148.17 $925.95 L $555.57 $1,211.32 $976.88 L $586.13
67149 Each additional implant $1,088.31 $877.68 L $526.61 $1,148.17 $925.95 L $555.57 $1,211.32 $976.88 L $586.13

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 10 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
67200 Retainers, porcelain/ceramic/polymer glass
67201 Retainers, porcelain/ceramic $889.14 $717.05 L $430.23 $938.04 $756.49 L $453.89 $989.64 $798.09 L $478.86
67202 Retainers, porcelain/ceramic veneer $711.32 $573.65 L $344.19 $750.44 $605.20 L $363.12 $791.72 $638.49 L $383.09
67210 Retainers, porcelain fused to metal
67211 Retainers, porcelain/ceramic fused to metal
$889.14 $717.05 L $430.23 $938.04 $756.49 L $453.89 $989.64 $798.09 L $478.86
67220 Retainers, porcelain fused to metal, attached to implant
67221 First implant $1,088.31 $877.68 L $526.61 $1,148.17 $925.95 L $555.57 $1,211.32 $976.88 L $586.13
67229 Each additional implant $1,088.31 $877.68 L $526.61 $1,148.17 $925.95 L $555.57 $1,211.32 $976.88 L $586.13
67300 Retainers, metal, cast
67301 Retainers, metal, full cast $889.14 $717.05 L $430.23 $938.04 $756.49 L $453.89 $989.64 $798.09 L $478.86
Oral and Maxillofacial Surgery
71100 Removals (extractions), erupted teeth
71101 Single tooth, uncomplicated $95.58 $77.07 $100.83 $81.31 $106.38 $85.79
71109 Each additional tooth, same quadrant, same appointment
$95.58 $77.07 $100.83 $81.31 $106.38 $85.79
71200 Removals, erupted teeth, complicated
71201
Odontectomy, extraction, erupted tooth, surgical approach, surgical flap and/or sectioning of tooth
$189.20 $152.59 $199.61 $160.98 $210.59 $169.84
71209 Each additional tooth, same quadrant, same appointment
$189.20 $152.59 $199.61 $160.98 $210.59 $169.84
72110
Removals, impaction, requiring incision of overlying soft tissue and removal of the tooth
72111 Single tooth $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
72119 Each additional tooth, same quadrant, same appointment
$171.55 $138.35 $180.98 $145.95 $190.94 $153.98
72210
Removals, impaction, requiring incision of overlying soft tissue, elevation of a flap and either removal of bone and tooth or sectioning and removal of tooth (partial bone impaction)
72211 Single tooth $257.33 $207.53 $271.48 $218.94 $286.41 $230.98
72219 Each additional tooth, same quadrant, same appointment $257.33 $207.53 $271.48 $218.94 $286.41 $230.98
72220
Removals, impaction, requiring incision of overlying soft tissue, elevation of a flap, removal of a bone and/or sectioning of tooth for removal (complete bone impaction)
72221 Single tooth $343.11 $276.69 $361.98 $291.91 $381.89 $307.96

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 11 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
72229 Each additional tooth, same quadrant, same appointment $343.11 $276.69 $361.98 $291.91 $381.89 $307.96
72230
Removals, impaction, requiring incision of overlying soft tissue, elevation of a flap, removal of bone and/or sectioning of tooth for removal and/or presents unusual difficulties and circumstances
72231 Single tooth $467.78 $377.24 $493.51 $397.98 $520.65 $419.87
72239 Each additional tooth, same quadrant, same appointment $467.78 $377.24 $493.51 $397.98 $520.65 $419.87
72310 Removals, residual roots, erupted
72311 First tooth $78.00 $62.89 $82.29 $66.35 $86.82 $70.00
72319 Each additional tooth, same quadrant, same appointment $78.00 $62.89 $82.29 $66.35 $86.82 $70.00
72320 Removals, residual roots, soft tissue coverage
72321 First tooth $116.99 $94.34 $123.42 $99.53 $130.21 $105.00
72329 Each additional tooth, same quadrant, same appointment $116.99 $94.34 $123.42 $99.53 $130.21 $105.00
72330 Removals, residual roots, bone tissue coverage
72331 First tooth $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
72339 Each additional tooth, same quadrant, same appointment $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
72510
Surgical exposure, un-erupted, uncomplicated, soft tissue coverage (includes operculectomy)
72511 Single tooth $155.99 $125.81 $164.56 $132.72 $173.62 $140.02
72519 Each additional tooth, same quadrant, same appointment $155.99 $125.81 $164.56 $132.72 $173.62 $140.02
72520 Surgical exposure, complex, hard tissue coverage
72521 Single tooth $280.67 $226.35 $296.11 $238.80 $312.39 $251.94
72530 Surgical exposure, un-erupted tooth, with orthodontic attachment
72531 Surgical exposure of teeth, un-erupted tooth, with orthodontic attachment $374.23 $301.80 $394.81 $318.40 $416.53 $335.91
72539 Each additional tooth, same quadrant, same appointment $374.23 $301.80 $394.81 $318.40 $416.53 $335.91
72540
Surgical exposure, un-erupted tooth, soft tissue coverage with positioning of attached gingivae
72541 Single tooth $233.99 $188.70 $246.86 $199.08 $260.43 $210.03
72549 Each additional tooth, same quadrant, same appointment $233.99 $188.70 $246.86 $199.08 $260.43 $210.03
72550
Surgical exposure, un-erupted tooth, hard tissue coverage with positioning of attached gingivae
72551 Single tooth $311.97 $251.59 $329.13 $265.43 $347.23 $280.03
72710 Enucleation, surgical, un-erupted tooth follicle
72711 Enucleation of un-erupted tooth follicle $343.11 $276.69 $361.98 $291.91 $381.89 $307.96

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 12 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
72719 Each additional tooth, same quadrant, same appointment $343.11 $276.69 $361.98 $291.91 $381.89 $307.96
73150 Excision of bone
73152 Excision of Torus Palatinus $343.11 $276.69 $361.98 $291.91 $381.89 $307.96
73160 Removal of bone, exostosis, multiple
73161 Per quadrant $514.66 $415.04 $542.96 $437.86 $572.83 $461.94
73210 Independent procedure
73211 Per sextant $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
73220 Miscellaneous procedures
73224 Excision of pericoronal gingiva (for retained tooth/implant) per tooth/implant $85.78 $69.18 $90.50 $72.99 $95.48 $77.00
73230
Removals, tissue, hyperplastic (includes the incision of the mucous membrane, the dissection and removal of hyperplastic tissue, the replacing and adapting of the mucous membrane)
73231 Per sextant $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
73240 Removal, mucosa, excess (complete removal without dissection)
73241 Per sextant $171.55 $138.35 $180.98 $145.95 $190.94 $153.98
73400 Vestibuloplasty
73461 Vestibuloplasty per sextant $406.17 $304.64 $428.51 $321.39 $452.08 $339.07
77500 Genioplasty
77501 Genioplasty, sliding, reduction or augmentation $1,624.74 Not Eligible $1,714.11 Not Eligible $1,808.38 Not Eligible
77600 Miscellaneous treatment of maxillofacial deformities
77603 Surgical expansion of the palate $748.09 Not Eligible $789.23 Not Eligible $832.64 Not Eligible
79900 Implantology
79931 Implant with cover screw $2,208.75 Not Eligible $2,330.23 Not Eligible $2,458.40 Not Eligible
79933 Implant with healing element $2,208.66 Not Eligible $2,330.14 Not Eligible $2,458.30 Not Eligible
79951 First stage surgical placement, maxilla per implant $1,227.09 Not Eligible $1,294.58 Not Eligible $1,365.78 Not Eligible
79953 Second stage exposure and temporization, maxilla per implant $981.67 Not Eligible $1,035.66 Not Eligible $1,092.62 Not Eligible
Orthodontics:
80600 Orthodontic, observations and adjustments
80601 Orthodontic observation for tooth guidance - per appointment $72.64 $58.58 $76.63 $61.80 $80.85 $65.20
80602 Orthodontic observation and adjustment to orthodontic appliance - per appointment $72.64 $58.58 $76.63 $61.80 $80.85 $65.20
80640 Alterations to removable or fixed appliances
80641 One unit of time $72.64 $58.58 L $35.15 $76.63 $61.80 L $37.08 $80.85 $65.20 L $39.12
80642 Two units of time $145.26 $117.14 L $70.29 $153.25 $123.59 L $74.15 $161.67 $130.38 L $78.23

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 13 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
80650 Re-cementation of fixed appliances
80651 One unit of time $72.64 $58.58 $76.63 $61.80 $80.85 $65.20
80660 Separation (except where included in the fabrication of an appliance)
80661 One unit of time $72.64 $58.58 $76.63 $61.80 $80.85 $65.20
80670
Removal of fixed orthodontic appliances (by a practitioner other than the original treatment practice or practitioner)
80671 One unit of time $72.64 $58.58 $76.63 $61.80 $80.85 $65.20
81110 Appliances, removable, space regaining
81111 Maxillary, unilateral $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81113 Maxillary, bilateral $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81120 Appliances, removable, cross-bite correction
81121 Maxillary, simple $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81130 Appliances, removable, dental arch expansion
81131 Maxillary, simple $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81140 Appliances, removable, closure of diastemas
81141 Maxillary, simple $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81150 Appliances, removable, alignment of anterior teeth
81151 Maxillary, simple $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81210
Appliance, fixed, space regaining (e.g., lingual or labial arch with molar bands, tubes, locks)
81211 Maxillary $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81220 Appliance, fixed, space regaining, unilateral
81221 Maxillary $217.89 $175.72 L $105.43 $229.88 $185.39 L $111.23 $242.52 $195.58 L $117.35
81230 Appliance, fixed, cross-bite correction - anterior
81231 Maxillary $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81240 Appliance, fixed, cross-bite correction - posterior
81241 Maxillary $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81243 Two-molar band, hooked and elastics $217.89 $175.72 L $105.43 $229.88 $185.39 L $111.23 $242.52 $195.58 L $117.35
81250 Appliance, fixed, dental arch expansion
81251 Maxillary $363.15 $292.87 L $175.72 $383.12 $308.97 L $185.38 $404.19 $325.97 L $195.58
81253 Maxillary, rapid expansion $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 14 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
81260 Appliance, fixed, closure of diastemas
81261 Maxillary, simple $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81270 Appliance, fixed, alignment of incisor teeth
81271 Maxillary, simple $363.15 $292.87 L $175.72 $383.12 $308.97 L $185.38 $404.19 $325.97 L $195.58
81290 Appliance, fixed, mechanical eruption of tooth/teeth
81291 Maxillary, impaction $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
81293 Maxillary, erupted $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
83100 Appliances, removable, retention
83101 Maxillary $217.89 $175.72 L $105.43 $229.88 $185.39 L $111.23 $242.52 $195.58 L $117.35
83103 Tooth positioner $217.89 $175.72 L $105.43 $229.88 $185.39 L $111.23 $242.52 $195.58 L $117.35
83200 Appliances, fixed/cemented, retention
83201 Maxillary $290.53 $234.29 L $140.57 $306.51 $247.17 L $148.30 $323.36 $260.77 L $156.46
89500
Neonatal dento-facial orthopaedics (comprehensive treatment for first 6 months of life)
Nasoalveolar Molding Appliance: fees include initial exam, insertion/fitting, lab component, continuing care and post procedural visits.
89501 Unilateral cleft $3,067.72 Not Eligible L $190.00 $3,236.44 Not Eligible L $200.45 $3,414.44 Not Eligible L $211.47
89502 Bilateral cleft $3,681.26 Not Eligible L $190.00 $3,883.73 Not Eligible L $200.45 $4,097.33 Not Eligible L $211.47
89503 Stage I - Initial expansion $1,472.50 Not Eligible $1,553.49 Not Eligible $1,638.93 Not Eligible
89504 Stage II - Anterior alignment $1,840.63 Not Eligible $1,941.86 Not Eligible $2,048.67 Not Eligible
89505 Stage III - Final alignment (complete banding)
$6,135.43 Not Eligible $6,472.88 Not Eligible $6,828.89 Not Eligible
89506 Stage III - Where Stage I and II were not provided for
$7,976.06 Not Eligible $8,414.74 Not Eligible $8,877.55 Not Eligible
Adjunctive General Services:
92210 General anaesthesia
92212 Two units of time $166.39 $134.19 $175.54 $141.57 $185.20 $149.36
92213 Three units of time $249.59 $201.28 $263.31 $212.35 $277.79 $224.03
92214 Four units of time $332.80 $268.38 $351.10 $283.14 $370.41 $298.72
92216 Six units of time $498.98 $402.57 $526.43 $424.72 $555.38 $448.07
92220 Provision of dental and anaesthetic facilities, equipment and supplies
92222 Two units of time $166.39 $134.19 $175.54 $141.57 $185.20 $149.36
92223 Three units of time $249.59 $201.28 $263.31 $212.35 $277.79 $224.03
92224 Four units of time $332.80 $268.38 $351.10 $283.14 $370.41 $298.72
92226 Six units of time $498.98 $402.57 $526.43 $424.72 $555.38 $448.07

Dent 44 – Schedule of Cleft Palate Dental Indemnity Program Benefits Page 15 of 15
A - 2010/2011 B - 2011/2012 C – 2012/2013
Procedure Code Description of Service
2010/2011 Specialist
Rates
2010/2011 Generalist
Rates
2010/2011 Specialist
& Generalist Lab Rates
2011/2012Specialist
Rates
2011/2012 Generalist
Rates
2011/2012 Specialist
& Generalist Lab Rates
2012/2013 Specialist
Rates
2012/2013 Generalist
Rates
2012/2013 Specialist
& Generalist Lab Rates
92300
Anaesthesia, deep sedation (includes neurolept analgesia/anaesthesia or dissociative anaesthesia, regardless of route of administration)
92302 Two units of time $150.58 $121.43 $158.86 $128.11 $167.60 $135.16
92303 Three units of time $225.87 $182.15 $238.29 $192.17 $251.40 $202.74
92304 Four units of time $301.16 $242.87 $317.72 $256.23 $335.20 $270.32
92410
Nitrous Oxide Time is measured from the placement of the inhalation device and terminates with the removal of the inhalation device
92411 One unit of time $26.28 $19.45 $27.73 $20.52 $29.25 $21.65
92412 Two units of time $39.42 $29.18 $41.59 $30.78 $43.88 $32.48
92413 Three units of time $52.57 $38.91 $55.46 $41.05 $58.51 $43.31
92414 Four units of time $65.71 $46.64 $69.32 $49.21 $73.14 $51.91
99999 Unlisted Procedures
Pre-surgical work-up:
Includes diagnostic records, radiographs, models, model surgery, treatment planning, lab charges etc. Maximum amount payable: $3,681.15 Not eligible $3,883.61 Not eligible $4,097.21 Not eligible
B.R.
By Report: the fee will be determined by Alberta Health Services' delegate in consultation with the program dental consultant and the treating practitioner on a "by report" basis.
Cleft Palate Dental Indemnity Program Dental Fee Guidelines
Effective for services provided on or after April 1, 2010 Program eligibility criteria:
In accordance with the eligibility criteria established in section 2 of the Treatment Services Regulation, and as further provided herein, to be eligible to receive coverage under the Cleft Palate Dental Indemnity Program (Program), a patient must:
Have a complete or incomplete congenital cleft affecting the alveolus (when there is a bony defect detected by radiographic imaging or when there is a congenitally missing lateral incisor) or of the hard palate if the hard palate has orthodontic implications as determined by a Program dental consultant.
Be 24 years of age or younger unless Alberta Health Services (the “Minister’s delegate”), determines that major surgical treatment to repair a congenital cleft of the alveolus or hard palate is required and that the dental treatment is required to restore adequate oral functioning in conjunction with the surgery.
Have the dental services performed in Alberta (unless the service is not available in Alberta).
Have no, or have exhausted, third party coverage and all other provincial or federal government benefit programs.
General program information:
Service provider fees will be as established by the Minister in a schedule of procedures and prices.
A Cleft Palate Dental Indemnity Program dental consultant (“Program dental consultant”) will assess all requests for payment in accordance with these guidelines and the schedule of procedures and prices. Final funding approval will be made by the Minister’s delegate.
If a dental service is deemed required by the treating dentist and is recommended for funding approval by a Program dental consultant and is not listed in the schedule of procedures and prices, the service may be claimed as an unlisted procedure using code 99999. Benefits for unlisted procedures will be assessed by comparing the benefit claimed to the benefits listed for similar procedures requiring similar responsibility and skill. Documentation to support the claim must be submitted by the treating dentist.
Where a price is determined “By Report”, that price will be determined by the Minister’s delegate in consultation with the Program dental consultant and the treating dentist.
Where a dental implant, prosthesis, appliance or dental device is required, the Program covers only the initial cost of the service. Except as otherwise provided herein, maintenance, replacements and repairs required for any reason, are the financial responsibility of the patient/parent/guardian.
Coverage under the Program is restricted to treatment on the two teeth on either side of the cleft unless otherwise stated in these guidelines.
Dent 44 – Cleft Palate Dental Indemnity Program Fee Guidelines Page 1 of 5
Pre-authorization from the Minister’s delegate is required for all general anaesthetic services and all treatment that exceeds $400. Diagnostic records and treatment plans must accompany a request for pre-authorization unless the Minister’s delegate determines otherwise. To qualify for payment of benefits, pre-authorized treatment by the treating dentist must commence within six months of the date of the approval.
In cases where pre-authorization has been granted and there is a subsequent change in the treatment plan requiring additional funding, the new treatment plan must be submitted to the Minister’s delegate for pre-authorization.
Coverage may be discontinued due to the patient's non-compliance with treatment plans. The Program will not provide coverage for dental conditions that were treated under the Program but have subsequently deteriorated due to non-compliance with treatment plans. Patients seeking reinstatement must provide evidence of compliance with prescribed plans before any coverage will be considered.
Claims must be submitted within 12 months from the date of service.
Funding approved for a specific dental service cannot be applied towards another dental service. Included benefits:
Services eligible for coverage under the Program include the following: Diagnostic Services: One initial complete examination, per specialty, for services directly related to the treatment of
the cleft area. (Please note: oral and maxillofacial surgeons may claim this exam if the required procedure is not insured under the Alberta Health Care Insurance Plan (AHCIP); neonatal consultations and treatment plans must be provided by a practitioner registered by the Alberta Dental Association and College in the area of pedodontics, orthodontics or oral and maxillofacial surgery).
One recall examination per patient, per 12 month period, when the service is provided by a general practitioner or pedodontist.
A maximum of two recall examinations performed by an oral and maxillofacial surgeon relating to an oral and maxillofacial surgical procedure not insured under the AHCIP.
Cleft site related periapical radiographs and maxillary occlusal radiographs as required.
One panoramic radiograph per patient, per five-year period. In addition, a panoramic radiograph if required for pre-surgical work-up (see the Oral and Maxillofacial Services section for information regarding pre-surgical work-up coverage).
Cephalometric radiograph as needed only when required in conjunction with oral maxillofacial surgery, comprehensive orthodontic treatment or insertion of a speech appliance.
Dent 44 – Cleft Palate Dental Indemnity Program Fee Guidelines Page 2 of 5

Preventive Services: One unit of scaling, one unit of polishing and one fluoride treatment, per 12 month period,
when the services are provided by a general practitioner or pedodontist.
One unit of dental related nutritional counselling and/or oral hygiene instruction per 12 month period for paediatric patients exhibiting a high caries index.
Pit and fissure sealants once per tooth for the first permanent molars and the two teeth on either side of the cleft.
Restorative Services: Basic restorative services, where applicable, for the two teeth on either side of the cleft. Endodontic Services: Endodontic services (including root canal therapy), where applicable, for the maintenance of
permanent dentition on the two teeth on either side of the cleft. Periodontic Services: Periodontal services (including periodontal surgery not covered under the AHCIP) for the
maintenance and stability of teeth and soft tissues directly associated with the cleft site, or for the abutment teeth involved in the prosthetic restoration of missing teeth associated with the cleft. In addition to one unit of scaling provided by a general practitioner or pedodontist, two additional units of scaling within the cleft site are payable if performed by a periodontist.
Prosthodontic Services: Removable and fixed prostheses to replace missing teeth in the cleft area may include a standard
partial/complete denture, bridgework and, on a one-time basis only, dental implants (Note: Fixed bridgework up to two teeth on either side of the cleft. A complete upper denture is payable at 100%. A complete lower denture is payable at 50% when there is a complete upper denture.)
Replacement of a removable or fixed prosthesis (excluding dental implants) after 5 years from the initial placement if deemed necessary by the Minister’s delegate or modification of removable or fixes prosthesis (excluding dental implants) within 5 years of the initial placement will only be considered for patients where replacement/modification is due to changes in the arch form or due to surgical procedures. Each request for funding will be considered on a case by case basis after an assessment at one of the two clinics.
Dental implants are eligible for coverage on a one-time basis only.
A maximum of one denture reline per 3 year period.
Neonatal appliances fabricated by a dentist when the appliance was prescribed by the treating specialist physician or oral and maxillofacial surgeon.
Prosthodontic laboratory fees associated with a procedure. The invoice must be included with a claim for the procedure.
Dent 44 – Cleft Palate Dental Indemnity Program Fee Guidelines Page 3 of 5

Oral and Maxillofacial Surgery Services: Dental extraction coverage may include those teeth associated with the cleft that are
supernumerary, malformed or non-functional and/or extractions of premolars where extraction is required for the provision of orthodontic/maxillofacial surgical services and/or eruption guidance.
A pre-surgical work-up (e.g. diagnostic records, radiographs, models, model surgery, development of a treatment plan and related lab charges) when required for an insured oral surgical procedure listed in the Schedule of Oral Maxillofacial Surgery Benefits or a procedure eligible for coverage under the Cleft Palate Dental Indemnity Program. Pre-surgical work-up fees, whether billed as one fee for all included services or billed as separate items, are claimable under the program one time only in the amount set out in the Schedule of Cleft Palate Dental Indemnity Program Dental Fee Payment Benefits.
General Anaesthesia: Pre-authorized general anaesthesia and neurolept anaesthesia when administered by a physician
in a hospital or in an accredited non-hospital surgical facility (plus non-hospital facility fees), provided that neither the anaesthesia nor the oral surgical procedure is an insured benefit under the AHCIP. The anaesthesia must be required for the provision of one of the services that are eligible for coverage under the Cleft Palate Dental Indemnity Program.
Orthodontic Services: Fees for the services in this section include all active treatment, insertion of retainers,
orthodontic records, observation appointments, radiographs and retention observation appointments. Multistage or extended orthodontic treatment must be identified by the orthodontist at the time of application. Treatment plan updates may be required periodically to assess the patient’s need for services.
Speech appliances: Speech appliances if prescribed by the Speech, Language and Pathology member of one of the
Cleft Palate Clinic specialist teams.
Replacement or modification of a removable speech appliance only in the instance of eruption of additional permanent teeth rendering changes necessary. (An initial cephalogram is eligible for coverage only when a velar bulb is needed as part of the speech appliance design).
Emergency services: Emergency services may be covered if the service relates to the dentition or soft tissues in direct
association with the cleft site and are a result of injury or development anomaly.
Dent 44 – Cleft Palate Dental Indemnity Program Fee Guidelines Page 4 of 5

Dent 44 – Cleft Palate Dental Indemnity Program Fee Guidelines Page 5 of 5
Excluded Services
The following services are excluded from coverage under the Program:
Services to patients over 24 years of age unless the Minister’s delegate determines that major surgical treatment to repair a congenital cleft of the alveolus or hard palate is required and that the dental treatment is required to restore adequate oral functioning in conjunction with the surgery.
Services provided outside of Alberta unless the service is not available in Alberta;
Services received before the patient meets Program eligibility criteria or before being pre-authorized where required;
Dental services which are not directly related or required solely due to a cleft of an alveolar ridge or hard palate or are cosmetic;
Except where provided in these guidelines, replacement, repairs, maintenance costs, of Program funded dental implants, prosthetic treatments, prosthetic devices, or dental appliances for any reason including treatment failures.
Local anaesthesia;
General anaesthesia and neurolept anaesthesia (and related facility fee) if provided by a dentist;
Any health care goods and services - including general anaesthesia - which are eligible for coverage under the AHCIP, or are part of an insured service provided in a hospital or in a private facility under contract with the regional health authority;
Pre-surgical work-up for procedures that are not insured under the Alberta Health Care Insurance Plan (Schedule of Oral Maxillofacial Surgery Benefits) and are not eligible for funding under this program;
Laboratory, diagnostic, therapeutics and other services provided under contract with the regional health authority;
Services and/or devices which are experimental, are the subject of clinical trials, are considered alternative dental therapy, or are no longer endorsed by the Alberta Dental Association and College;
Subsistence, travel/mileage and accommodation costs for the person receiving eligible goods under the program or anyone who accompanies that person;
Services provided to patients who are not entitled to coverage with the Alberta Health Care Insurance Plan.