Embed Size (px)
Citation preview

1
Presented by: Scott Truong & Phil Chrapka

2
Method of using low electrical currents to restore body functions by stimulating nerves
Can be used to help patients with many conditions especially Spinal Cord Injury (SCI)

3

4
Overview
Nervous & Muscular systemComplicationsHistoryFES PrinciplesFES System ComponentsApplicationsFuture Directions

5
The NerveThe foundation of FES relies on stimulating motor nerves

6
100’s to 10,000’s of neurons, along with connective tissue and blood vessels compose nerves
Nerves run throughout body to muscles
Traveling electric gradient

7
Motor Nerve

8
Motor NerveNeurotransmission at the end of action potential to muscle

9
CNS: consists of thebrain and spinal cordSpinal cord sendssignals to motorsnerves of the PNSPNS runs throughoutbodyCNS and PNS arecontinuous

10
Spinal Cord Injury (SCI)◦
Complete paraplegia
T-1 to T-12◦
Complete tetraplegia
C-1 to C-8

11
CNS damage = spinal cord damagePNS damage = nerve damageCNS damage vs PNS damageFES functions on the basis of CNS damage not PNS damageA break in neurotransmissionCommon results of damages: paraplegics, foot drop, paralysis, etc.

12
First developed in 1961 by Libersonand colleaguesCoined term “functional electrotherapyCorrected drop foot in hemiplegicpatients using electrical stimulation

13
FES: a technique that uses short electrical pulses to activate nerves affected in paralysisRestores function to people with disabilitiesBasic components:◦
Electrodes ◦
stimulator◦
controller

14
There are 2 types of Electrodes:◦
Surface (transcutaneous) electrodes
◦
Implanted (percutaneous) electrodes

15
Placed on patient’s skin over target nervesAdhesive or non-adhesiveElectric signals passed through skin to stimulate nerves

16
Advantages Disadvantages
Not permanentGood for short-term useReuseableGood for nerves that aren’t deepNon-invasive
Hard to place exactly over correct areaA hassle to put on all the timeDifficult to stimulate deep nervesCan stimulate pain feedback nervesPrecision is lowCan cause skin burns

17
Electrode attached to nerves or to muscles close to nervesInvasiveLeads exiting skin for external controller or none for remote controller

18
Advantages Disadvantages
Does not require reapplicationVery precise muscle stimulationGood for long-term use
InvasiveDifficult to replace if requiredPermanent

19
Pulses create an electric field near the target nerve and depolarize it -> action potentialAction potentials spread down axon and stimulate target muscleTetanization (muscle contraction) requires at least 20 pulses per second

20

21
Typical pulse parameters:◦
Biphasic (monophasic
causes burns)
◦
20-30 pulses/sec◦
Duration of primary signal: 100-200 μsec◦
Current: 25 –
35 mA
◦
Amplitudes: 25 –
35V
Pulse determines strength of contractionMain condition – motor nerves need to be intact (not “denervated”)

22
StimulatorImplanted stimulator receives signals from controller via radio wavesExternal stimulator can receive radio waves or be directly connected to the controller via wiresConnected to electrodes via leads wrapped in an “insulated conducting”material

23
ControllerStationary version◦
Usually large and bulky◦
A computer◦
Controlled by another person or automated◦
Often used for short term rehabilitationPortable version◦
Often worn on hip◦
Convenient for long term use◦
Manual and automated versions available

24
Spinal Cord Injury (SCI)Foot dropWalkingCardiac pacemakersBladder voidingPain suppression
25
Hand Grasp◦
Surface electrode versions
Bionic GloveHandmaster
◦
Implanted electrode versions
Freehand SystemNEC-FES System

26
2-way depolarization
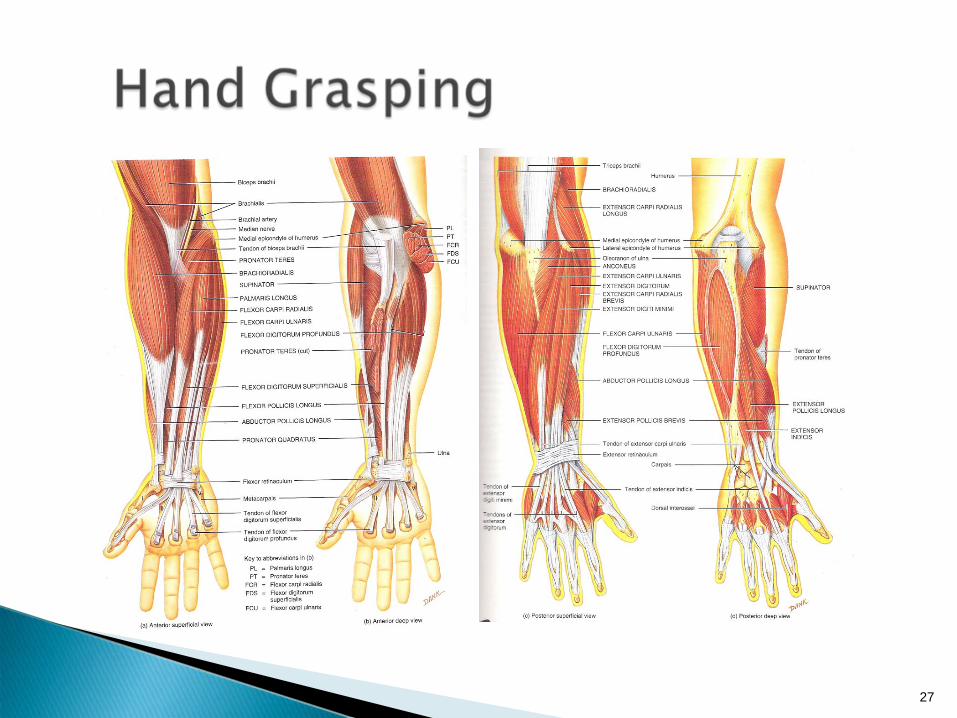
Ulnar and Median nervecontrol fingers
Electrodes should be implanted or cuffed in/on the forearm
27

28
Flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor pollicis longus = median nerveFlexor carpi ulnaris = ulnar nerveFlexor digitorum profundus = median and ulnar nervesExtensor carpi radialis longus, extensor carpi radialis brevis, and extensor digitorum = radial nerveExtensor digiti minimi, extensor carpi ulnaris, and deep posterior muscles = deep radial nerve

29
Holding and manipulationTwo main objectives:◦
Reliable and long lasting power grasp
Adjustable◦
Smooth pinch grasp to manipulate small objects
Easily controllable Should not interfere with existing functionShould be normal physiological movementUsually C-5 to C-7 tetraplegia

30

31
Opening and closing of hand controlled by position sensor on shoulder of patient’s opposite armFront (protraction), back (retraction) – for opening and closingUp (elevation), down (depression) –
for
logic commands and freezing the grasp
32
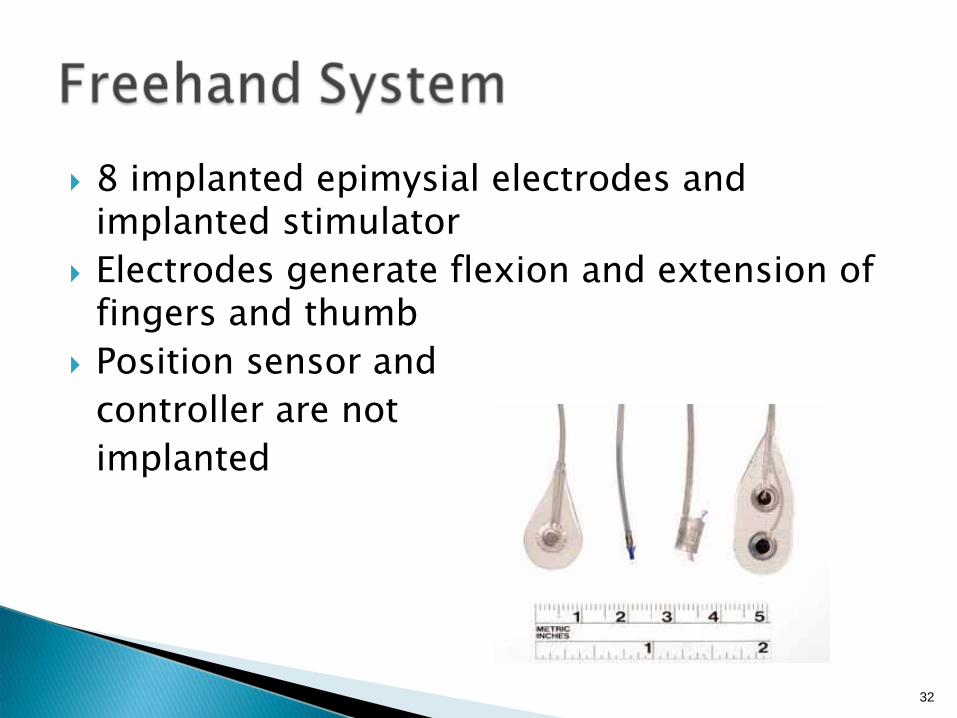
8 implanted epimysial electrodes and implanted stimulatorElectrodes generate flexion and extension of fingers and thumbPosition sensor and controller are not implanted

33
First neuroprostheses approved by the USA FDA130 patients currently using this systemCommercially availableTime required to take on or off is quick18-24 month wait after injury is needed

34

35
Designed to enhance tenodesis grasp in patients that have control of wrist flexion and extensionUses position transducer on wrist to detect wrist flexion and extension3 adhesive surface electrodes,placed over motor points of target muscles1 anodic electrode placed proximal to the wrist crease

36

37
38
OFF

39
ON

40
Can be used early in rehabilitationShortcomings:◦
Stimulator on forearm is subjected to abuse
◦
Position transducer is delicate
◦
Contacts between electrodes and mesh are disrupted due to arm movements
◦
Electrode on thumb slips off with use

41
FES has had promising progressLimited use◦
Highly technical◦
High expectations from family
After FES treatment, some patients recovered grasping functions

42
BIONs (Biological Neurons)
“Thought” – control FES
43
Any Questions?

44
Gerard J. Tortora, Sandra Reynolds Grabowski, “Principles of Anatomy & Physiology”, John Wiley & Sons, Inc. 2003Sir Ludwig Guttmann, “Functional Electrical Stimulation after spinal cord injury: current use, therapeutic effects and future directions”, International Spinal cord society, 2007.P. Hunter Peckham, Peter H. Gorman, “Functional Electrical Stimulation in the 21st century”, Thomas Land Publishers, Inc. 2004Xu Qi, He Jiping, Wang Yongji, Xu Tao, Huang Jan, “A review of fundamental mechanisms and techniques in functional electrical stimulation”, Huahzong University of Science and Technology, 26 May, 2005Hambrecht, FT, “FES: How and when it started?”, IFESS organization, volume 1 number 2, Last updated: Jan 19, 2007http://www.ifess.org/Services/News%20and%20Views/Volume_1/Number_2/number_2.htmCleveland FES Center, “FES Resource Guide”, Last accessed: Oct 2, 2007http://fescenter.case.edu/site2/GRFX/FESRG.pdfPopovic et al. “Functional electrical stimulation for grasping and walking: indications and limitations.”Spinal Cord (2001) 39:403-412.Popovic et al. “Modular transcutaneous functional electrical stimulation system.” Medical Engineering & Physics 27 (2005) 27:81-92.Prochazka, Arthur. “The Bionic Glove: An Electrical Stimlator Garment That Provides Controlled Grasp and Hand Opening in Quadriplegia.” Arch Phys Med Rehabil Vol 78, June 1997.Pfurtscheller et al. “Thought – control of functional electrical stimulation to restore hand grasp in a patient with tetraplegia.” Neuroscience Letters (2003) 251:33-36





























