Upload
kasrasr
View
79
Download
1
Embed Size (px)
DESCRIPTION
Physiological and biochemical concepts in biotechnology.Introductory biotechnology principles.
Citation preview
PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
aTypewritten Text"This page is Intentionally Left Blank"
aTypewritten Text
Physiology, Biochemistry
and Biotechnology
Dr. Madan Lal Bagdi
MANGLAM PUBLISHERS & DISTRIBUTORS DELHI - 110 053 (INDIA)
Published by MANGLAM PUBLISHERS & DISTRIBUTORS L-2111, Street No. 5, Shivaji Marg, Near Kali Mandir, l.P. Nagar, Kartar Nagar, West Ghonda, Delhi -53 Phone: 22945678, Cell.: 9868572512
Physiology, Biochemistry and Biotechnology
Reserved
First Published 2007
ISBN
Preface
The text book entitle, Physiology, Biochemistry and l!iotechnology as a distinct subject developed in the middle ofthe 20th century as researchers started to understand the molecular approach of the various systems of the body. It is designed to introduce the principles of physiology and biochemistry and their application to the students aiming for a career as a nurse, medical assistant, physician's assistance, medical laboratory technologists, radiologists, pharmaceutical and molecular biologist. It encompasses all the chemical reactions carried out by the cells, organ and systems. In clear and compelJing language this text book describes the ideas and techniques that are creating a new domain of science and technology. It also provides a real service to the layman interested in this exploding technology.
aTypewritten Text"This page is Intentionally Left Blank"
aTypewritten Text
Contents
1. Alimentary System and Nutrition ............................ 1-32 1. 1 Gastrointestinal System ....................................... 1
1. 1. 1 Gastric Activity ..................................... 8 1.1.2 Gastric secretions .................................. 9 1. 1. 3 Protein Digestion. . . . . . . . . . . . . . . . . .. .. . . . . .. .. .... 11 1.1.4 Control of Gastric Secretion.................... 11 1.1.5 1.1.6 1.1.7 1.1.8 1.1.9 1.1.10 1.1.11
1.1.12 1.1.13 1.l.l4 1.1.15 1.l.l6 1.1.17 1.l.l8
Histamine Receptors ............................. 14 Gastric Emptying. .............. .. . .... .. . . . . . . . .. 14 tntestinal Absorption ............................. 15 oarbohydrates .................................... 15 Proteins... ... ...... . .... ... . ....... .... ... . . .... ... 17 Fats ................................................. 18 The Structure and Catalytic Mechanisms of Pancreatic Enzymes .......................... 19 Control of Pancreatic Secretion ................ 21 Control of Bile Secretion ........................ 22 Motility of Small Intestine ., .................. " 24 Absorption of Water and Electrolytes ......... 24 Vitamins ........................................... 25 The Large Intestine .............................. 25 Defaecation ....................................... 26
1.2 Metabolic Rate ............................................... 27
2. Respiratory System ............................................. 33-63 2.1 Respiration .................................................... 33
2.1.1 Diffusion of Gases in Respiration .............. 33
(ii) 2.1.2 2.1.3 2.1.3 2.1.4 2.15 2.1.6
2.1.7
CONTENTS
Ventilation of the Lungs ..... ., ................. 34 Pulmonary Circulation .......................... 36 Mechanics of Respiration ....................... 38 Lung Volumes .................................... 45 Gas Mixtures and Pressures .................... 46 Respiratory Dead Space and Alveolar Ventilation ............................. 48 The Transfer of Gases Between Alveoli and Blood ................................ 50
2.1.8 Gravity Effects on Blood and Gas Flow to the Lungs ..................... 51
2.1.9 Carriage of 02 and CO2 by the Blood ......... 52 2.1.10 Oxygen Dissociation Curves ................... 53 2.1.11 The Carriage of CO2 and
the CO2 Dissociation Curve .................... 54 2.2 Regulation of Respiration ................................... 57
2.2.1 Control System ................................... 57 2.2.2 Non-chemical Influences on Respiration ...... 58 2.2.3 Chemical Control of Respiration .............. 59 2.2.4 Ventilatory Response to Pure
Changes in CO2, 02 or [H+] .................... 61 2.2.5 Ventilatory Response to Combined
2, CO] and [H+] Changes ..................... 62 2.2.6 Non-respiratory Features of
Pulmonary Circulation .......................... 62 2.2.7 Nutritional Blood Supply to the Lungs ........ 63
3. Blood and Body Fluids ......................................... 64-88 3.1 Cells of the Blood ............................................ 64
3.1 . I Erythrocytes ...................................... 65 3.1 .2 Erythrocyte Production and Destruction ...... 65 3.1.3 Haemolysis of Erythrocytes .................... 66 3.1.4 The blood pigments .............................. 66 3.1.5 Abnormal Haemoglobins ........................ 67 3.1.6 Synthesis and Destruction of
Haemoglobin .......... " ............... " ....... " 69 3.1 .7 Substances Essential to Erythropoieses ....... 69 3. 1. 8 Vitamin B72 and Folic Acid .................... 70
CONTENTS (iii) 3. 1.9 Death of erythrocytes, degradation of
haemoglobin and metabolism of bile pigments ...................................... 72
3. 1.10 Blood Groups ............... ,..................... 72 3. 1.11 The Leucocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 75
3.2 The Lymphoreticular Organs ..... " ........................ 77 3.2.1 Lymphocytes and Immunity .................... 78 3.2.2 Two Populations of Lymphocytes:
T - and B-cells ..................................... 79 3.2.3 The Platelets ...................................... 81
3.3 Plasma ......................................................... 81 3.3.1 Salts ................................................ 82 3.3.2 Plasma Proteins .................................. 82 3.3.3 Haemostasis ....................................... 83 3.3.4 Anti-clotting Mechanisms ....................... 85 3.3.5 Lymph ............................................. 87
4. The Cardiovascular System ................................. 89-140 4.1 Circulation of the Blood ..................................... 89 4.2 The Heart ..................................................... 89
4.2.1 Outline of Function .............................. 89 4.2.2 Physiological Properties of the Heart ......... 90 4.2.3 The Cardiac Action Potential.. ................. 92 4.2.4 Conduction of the Action
Potential Over The Heart ....................... 96 4.2.5 Contraction of Heart Muscle Cells ............ 97 4.2.6 Events of the Cardiac Cycle .................... 98
4.3 The Vascular System ....................................... 103 4.3.1 Arteries ........................................... 103 4.3.2 Veins .............................................. 110 4.3.3 Arterioles and Capillaries ...................... 113 4.3.4 Peripheral Circulation as a Whole ............ 118 4.3.5 Methods of Measuring Blood Flow ........... 120
4.4 The Overall Control of the Circulation .................. 122 4.4.1 Control of Blood Pressure ..................... 123 4.4.2 Sensory Receptors in the Heart and Aorta .. 125 4.4.3 Regulation of Cardiac Output ................. 126
(iv)
4.4.4 4.4.5 4.4.6 4.4.7 4.4.8
CONTENTS
Control of Heart Rate ........... :: ............. 127 Control of Stroke Volume ..................... 127 Regulation of the Peripheral Resistance ..... 129 Coronary Circulation ......... , ................. 133 Cerebral Circulation ............................ 133
4.4.9 Effects of Posture on the Circulation ......... 135 4.5 Placental and Foetal Circulation .......................... 137
4.5.1 Uterine Circulation ............................. 137 4.5.2 Placenta ........................................... 137. 4.5.3 Foetal Circulation ............................... 137 4.5.4 Changes at Birth ................................. 139
5 The Kidney and Micturition .............. 141-161 5. 1 Gross Structure of the Kidney ............... " ............ 141
5.1.1 The Structure of the Nephron ................. 142 5.2 The Control of Urine Formation .......................... 144
5.2.1 Glomerular Filtration ........................... 144 5.2.2 5.2.3 5.2.4 5.2.5
5.2.6 5.2.7
5.2.8
5.2.9 5.2.10
5.2.11 5.2.12 5.2.13
5.2.14
The Concept of Clearance ..................... 146 The Urea Clearance ............................ 148 Control of Blood Osmolality .................. 149 Iso-osmotic Reabsorption in the Proximal Tubule ............................................ 149 Trans-tubular Potentials ........................ 150 Reabsorption in the Distal Parts of the Nephron .................................. 151 Hormonal Control of Sodium Reabsorption ..................................... 154 Urea Excretion .................................. 154 Reabsorption of Sugars and Amino Acids ..................................... 155 Tubular Secretion ............................... 157 Potassium Regulation ........................... 157 Renal Regulation of Hydrogen Ion Concentration ............................... 158 Mechanism of Micturition ..................... 160
6 Reproductive Physiology .................................... 162-189 6.1 Sex Differentiation. . . . . .. . .. .. . .. .. . .. . .. .. .. .. .. .. .. .. .. ... 162
CONTENTS (v) 6.2 Female Reproductive System .............................. 164
6.2.1 Ovarian and Uterine Cycles ................... 166 6.2.2 Ovarian Cycle ................................... 166 6.2.3. Uterine Cycle .................................... 169 6.).4 Ovarian Hormones .............................. 169 6.2.5. Anterior Pituitary and Hypothalamus ........ 171 6.2.6 Control of the Ovarian Cycle .................. 171 6.2.7. Oral Contraceptives ............................. 174 6.2.8 Pregnancy ........................................ 174 6.2.9 Hormones in Pregnancy ........................ 175 6.2.10 Pregnancy Diagnosis ............................ 177 6.2.11. Parturition ........................................ 179 6.2.12 Lactation .......................................... 180
6.3 Male Reproductive System ................................ 183 6.3.1 Spermatogenesis ................................. 183 6.3.2 Control of Testicular Function ................ 184 6.3.3 Fertilisation ...................................... 187
6.4 Puberty ....................................................... 188 190
7. Endocrinology and Metabolism ....... .................... 190-246 7.1 Hormones in General ....................................... 190
7.1.1 Factors which Determine the Blood, Concentration of Hormones ................... 191
7.1.2 Blood Transport ................................. 192 7.1.3 Hormone Action on Target Cells ............. 193 7.1.4 The Way in which the Primary
Event Alters Cellular Functions ............... 195 7.1.5 Levels of Complexity of
. " Hormone As;tlon ................................. 197 7.1. 6 Endocrine Investigations ....................... 198
7.2 The Hypothalamus and Pituitary .......................... 199 7.3 Growth Hormone ........................................... 202 7.4 Prolactin and the
Pituitary Gonadotrophins ................................... 206 7.5 Hormones of the Posterior
Pituitary Gland .............................................. 206
\
(vi) CONTENTS 7.6 The Thyroid Gland ......................................... 209 7.7 The Control of Growth ..................................... 213 7.8 Adrenal Gland ............................................... 2 I 6 7.9 Adrenal Cortex .............................................. 217
7.9. 1 Glucocorticoids .................................. 219 7.9.2 Mineralocorticoids .............................. 223
7.10 Organic Metabolism and the Glucose Regulating Hormones ........................ 227 7.10.1 Outline of Absorptive and
Post -absorptive Events ......................... 229 7.10.2 The Absorptive State ........................... 230 7.10.3 Post-absorptive or Fasting State .............. 231 7.10.4 Insulin ............................................. 234
7.11 Bone and the Calcium Regulating Hormones ....................................... 239 7.11.1 Calcium ........................................... 239 7.11.2 Calcium Regulation ............................. 242 7.11.3 Other Modulators of Ca ........................ 246
8. Introduction to Metabolism and Energy Metabolism ............................. 247-257 8.1 Characterization of Metabolism ........................... 247 8.2 Energy Cycles in Animate Nature ........................ 249 8.3 Energetics of Biochemical Reactions ..................... 252 8.4 Hight-Enegry and Low-Energy Phosphates: General
Considerations ............................................... 254 8.5 Energy Transfer in
Biochemical Processes ..................................... 256
9. Carbohydrate Metabolism .............................. 258-272 9.1 Carbohydrage Catabolism in Tissues ..................... 258
9.1. 1 Pentose Phosphate Cycle ....................... 259 9. 1.2 Interrelation of the Pentose
Phosphate Cycle and Glycolysis .............. 262 9.1.3 The Biological Function of
the Pentose Phosphate Cycle .................. 263 9.2 Biosynthesis of Carbohydrates in Tissues ............... 265
9.2.1 Gluconeogenesis ................................. 265
CONTENTS (vii) 9.2.2 Biosynthesis of Glycogen
(Glycogenogenesis) ............................. 268 9.2.3 Biosynthesis of Other
Oligosaccharides and Polysaccharides ....... 269 9.3 Carbohydrate Metabolism
Control in the Organism ................................... 270
10. Lipid Metabolism ............................................ 273-293 10. I Degradation of Lipids in Tissues ............. " ........... 273
10.1.1 Intracellular Hydrolysis of Lipids ............. 273 10.1.2 Oxidation of Glycerol .......................... 274 10.1.3 Oxidation of Fatty Acids ....................... 274
10.2 Biosynthesis of Lipids in Tissues .......... '" ............ 279 10.2.1 Biosynthesis of Fatty Acids .................... 279 10.2.2 Biosynthesis of Triglycerides .................. 282 10.2.3 Phospholipid Biosynthesis ...................... 283 10.2.4 Biosynthesis of Ketone Bodies ................ 285 10.2.5 Biosynthesis of Cholesterol .................... 287
10.3 Regulation of Lipid Metabolism in the Organism .............................. 288
10.4 Pathology of Lipid Metabolism ........................... 290 10.5 Applications of Lipids and Their
Components in Pharmacotherapy .... '" .................. 292
,
f
aTypewritten Text"This page is Intentionally Left Blank"
aTypewritten Text
1
Alimentary System and Nutrition
1.1 GASTROINTESTINAL SYSTEM The tract is, in effect, a long muscular tube of variable diameter
lined with mucous membrane, running from the mouth to the anus. Into ~he lumen of this tube various organs and glands add their secretions and these, together with those of the mucous membrane itself, are responsible for the digestive process whereby the complex foodstuffs we ingest are broken down into much simpler molecules. This is necessary as only simple molecules can be absorbed from the intestinal lumen and carried in the blood to supply the nutritional needs of cells.
Structure. Although the structure of the alimentary canal varies somewhat along its It!ngth, it does have a basic form which can be recognised in most parts. From within outwards, the gut wall consists of four layers:
1. Mucosa. 2. Submuoosa. 3. Muscular layer. 4. Serosal or adventitous coat. The mucosal lining has an epithelial layer with supporting
connective tissue beneath it in which the blood capillaries run, and this in turn is in contact with a thin layer of smooth muscle called the muscularis mucosae. This muscle is innervated by sympathetic nerve fibres and contraction of the muscle results in folding of the mucosa.
The submucosal layer is composed of more dense connective tissue in which run larger blood vessels and a plexus of nerves (Meissner's
2 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
plexus) to supply the mucosal glands. The main muscle layer consists of an outer longitudinal layer and an inner circular one of smooth muscle with a nerve network between them (Auerbach's plexus) .
Ducts~::---"""r7"--.t"I .. __ . ____ Parotid gland ___ Pharynx
1+-_______ Oesophagus
Gall bladder
Liver
Stomach
~pancreas __ Splenic
flexure Duodenum --t----:;>..co
ALIMENTARY SYSTEM AND NUTRITION 3
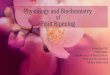
glands of the mouth, in gastric juice, bile from the liver, in pancreatic juice and in secretions from the mucous membrane of the small intestine. Layers
Mucosal_
Longitudinal muscle
Circular muscle
Muscularis mucosae
H'-+'""7""'"'+t,t;~II:+:i~Epithelial layer
Muscosal blood vessels
Submucosal nerve plexus
Myenteric nerve plexus
Figure 1.2 Cross-sectton showing basic layers of the gastrointestinal tract. The start of carbohydrate digestion occurs in the mouth because
of the presence of salivary gland secretion of the enzyme ptyalin. The main carbohydrate in our diet is starch, a polymer of glucose. either in the unbranched chains of amylose or in the branched form, amylopectin. We also ingest the disaccharides sucrose and lactose. Only very small amounts of monosaccharides are normally ingested.
The digestive enzymes found in the human intestinal tract can break the 1,4-a type of linkage found in the straight chains and also the 1,6-a linkage found at the branches of amylopectin. We do not, however, secrete enzymes capable of breaking the linkages between the glucose subunits of cellulose (1, 4-f3 linkage) and so we are unable to digest this and it passes through the gut adding bulk to the faeces.
Saliva. The active enzyme in saliva is ptyalin, an amylase, which hydrolyses l,4-a linkages. The optimal pH for amylase activity is 6-7 and so its action is to some extent limited because food does not stay long in the mouth and, once it has passed into the stomach, the food bolus is subjected to a high acidity which inhibits amylase activity.
4 PHYSIOLOGY. BIOCHEMISTRY AND BIOTECHNOLOGY
The enzyme activity will of course continue in the middle of a bolus until penetration by the gastric acid.
H OH lal
(bl
Figure 1.3. (a) Maltose .. u 1.4 linkage of glucose subumts. (b) Celiobiose-j3 J.4 linkage o. glucose subunits. .
Saliva is also important in that it moistens the food, enhancing the p .,..:ess of chewing and making food more easily swallowed; in addition it has a bacteriostatic action. Saliva comes partly from the many mucous glands in the mucosa of the mouth but mainly from discrete glands which lie outside the mouth and pass their secretions into the mouth by ducts. These acinar glands are the parotids. the sub-mandibular and sub-lingual glands and they secrete both mucous and serous fluid. The secretion is continuously fonned at a slow rate. even when the mouth is empty, at an average of 0 2 ml/minute in man; this may increase 20 times when eating. As with gastric secretion, the increase in flow of saliva is partly caused by a conditioned reflex. The thought of food acts as a stimulus to secretion. but the presence of food in the mouth also acts as a stimulus. Impulses from receptors in the oral mucosa pass in the lingual and glos~opharyngeal nerves to the medulla from whence efferent impulses pass to the salivary glands. The presence of anything in the mouth. for example a piece of gnt, acts as a stimulus in this unconditioned reflex.
ALIMENTARY SYSTEM AND NUTRrnON 5
The salivary glands receive both sympathetic and parasympathetic nerve supplies. Stimulation of the latter causes an increased blood flow through the glands and a copious watery secretion is formed. This does not mean that the secretion from the gland is merely a filtrate of blood. The increased oxygen consumption of the gland which accompanies this increased activity shows that saliva is being formed by a metabolically active process in the gland. When the sympathetic supply is stimulated these glands produ.ce a viscid saliva with a high concentration of mucus.
Chewing. When food is taken into the mouth it is broken into smaller particles which can be more easily swallowed by chewing. This is obviously a voluntary process but also occurs as an involuntary reflex. The contact of food on the palate and tongue causing a reflex opening of the mouth, but this results in an anti-gravity reflex closing it, thus setting up a rhythmic movement. Chewing continues until ingested food is soft, small enough and sufficiently well mixed with saliva to be swallowed; but this is greatly influenced by habit and external forces such as conversation. The amount of chewing probably does not influence the digestion of food very much.
Swallowing. Once food has been chewed and mixed thoroughly with saliva, it is formed into a small ball or bolus which can be swallowed. Swallowing is a complex series of contraction and inhibition of many voluntary and involuntary muscles. The tongue initiates the process by pushing the bolus into the back of tbe mouth, resulting in the stimulation of receptors there. You can convince yourself that swallowing is not a purely voluntary process but requires stimulation of receptors by trying to swallow your saliva three times in succession; after swallowing twice, no saliva remains in the mouth and you cannot initiate a third swallowing movement. Impulses from these swallowing receptors in the mouth pass to a 'swallowing centre' in the medulla which coordinates the train of events. Once swallowing has been initiated it cannot be voluntarily stopped.
As the tongue pushes the bolus backwards in the midline the soft palate is raised to shut off the naso-pharynx, respiration is inhibited, the larynx raised and the glottis closed to prevent food entering the trachea.
This movement of the bolus backwards and downwards folds the epiglottis back over the glottis although this is not sufficient by itself to protect the trachea from food; closure of the glottis is essential. Occasionally a small particle of food or fluid may reach the respiratory
6 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
tract before closure of the glottis and cause coughing by stimulation of respiratory tract receptors.
Oesophagus. The oesophagus is the tube which carries food from the pharynx to the stomach. It has skeletal muscle around its upper third and smooth muscle in its lower two-thirds. Before and after , swallowing both the upper and lower ends of the oesophagus are closed, but swallowing results in relaxation of both sphincters. Once food has passed through the upper sphincter it closes, the glottis opens and respiration starts again.
Perisfollic wove
Figure 1.4. Peristalsis in oesophagus. Muscle fibres below food bolus relax, those behind contract.
Once a bolus has entered the oesophagus a wave of contraction passes along the smooth muscle of the wall from the oral to the stomach end. This wave of contraction is immediately preceded by a wave of relaxation and results in the food bolus being pushed onward through the relaxed gastro-oesophageal or cardiac sphincter into the stomach. This process is called peristalsis.
Peristalsis is a feature of many different parts of the gastrointestinal tract and its coordination is the result of local nerve-plexus activity in the gut wall. In the oesophagus, however, the nerve network in the
ALIMENTARY SYSTEM AND NUTRITION 7
wall is coordinated by the swallowing centre and occurs only if the vagal efferent nerves from the centre to the oesophagus are intact. Normally a peristaltic wave passes along the oesophagus in about 10 seconds. (You can time this for yourself by listening for liquid reaching your empty stomach.) The passage of a bolus is normally assisted by gravity, but it is possible to swallow while standing on one's head when movement of food along the oesophagus depends entirely on peristalsis. If a bolus sticks in the oesophagus this distending stimulus results in a secondary wave of peristalsis, and this again requires an intact extrinsic nerve supply.
High - pressure zone~jiiiiiiiiiiiiiiiiiiiiii-'
+ ve pressure
+ ve pressure
Figure 1.5. Part of the oesophagus lies below the diaphragm am so is exposed to the positive intra-abdominal pressure which helps to squeeze it am prevent reflux.
The lower end of the oesophagus normally remains closed and so prevents reflux of gastric contents. Although the muscle fibres of the lower end of the oesophagus do not form an anatomical sphincter, the lowest 4 cm is normally in a state of contraction and acts as a physiological sphincter. This region has been called the high-pressure zone (HPZ). Intra-abdominal pressure is always higher than the normally negative intrathoracic pressure, and at times becomes very much higher, so it is surprising that stomach contents do not get pushed back into the oesophagus. This is prevented not only by this high-pressure-zone sphincter but also by the fact that part of the oesophagus lies below the diaphragm and any increase in intra-abdominal pressure which would squeeze the stomach also 'squeezes this part of the oesophagus and keeps it closed. The oesophagus runs diagonally through the diaphraj!m to enter the abdomen; it has been suggested that a part of
8 PHYSlOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
the muscle of the diaphragm may pinch the oesophagus shut, particularly during a deep inspiration. The oesophagus enters the stomach at an acute angle; perhaps a fold of mucosa acts as a flap-valve to prevent ret1ux of contents into the oesophagus. 1.1.1 Gastric Activity
One function of the stomach is to act as a hopper, collecting swallowed food so that it can be held there until it is passed on to the duodenum at a controlled rate for digestion and absorption. Gastric muscle shows 'receptive relaxation'; this means that as the quantity of food in its lumen increases during a meal the muscle in the wall relaxes to enlarge the cavity, so preventing an increase in intraluminal pressure.
Figure 1.6. Gastric peristalSIS. As the move of contraction doe~ not close the lumen of stomach completely, some contents escape back into the fundus and cause mixing.
ALIMENTARY SYSTEM AND NUTRITION 9
Another function of the stomach is to help mix the swallowed food with gastric secretions forming a semi-liquid substance called chyme. This mixing process is accomplished by rhythmic contractions of the gastric smooth muscle. The longitudinal layer of smooth muscle has a basic electrical rhythm of 3 beats/minute; the propagation of this electrical activity produces a wave of contraction spreading across the stomach to the pyloric area. This peristaltic wave pushes the more liquid contents through the pylorus into the duodenum, but as the pyloric muscle contracts its lumen closes and this forces the antral contents back into the body of the stomach resulting in further mixing of food and gastric juices. 1.1.2 Gastric secretions
Gastric secretions consist of mucus, pepsinogens, hydrochloric acid and intrinsic factor, all of which arise from cells in the gastric mucosa. Their total volume is about 3 litres/day. The mucous membrane is
Surface
Neck mucous
cell
Parietal cell
Lumen __
Chief cell " ___ -...
epithelial cell
Figure 1.7 Diagram of cells to be found in the body of the stomach.
10 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
not the same throughout the stomach, the epithelium of the body of the stomach being arranged in gastric pits and glands. The different components of gastric secretion arise from different types of cells in these pits and glands. Seventy-five per cent of the gastric mucosa is of this type. The antral area has larger pits and branching coiled glands with no parietal or chief cells but instead rounded cells lying between the mucus- secreting cells. These rounded cells secrete gastrin.
The main enzyme in gastric juice is secreted as inactive pepsinogen from serous or chief cells and in the presence of acid or pepsin the inactive pepsinogen becomes active pepsin. Hydrochloric acid is secreted by the parietal or oxyntic cells which have small channels or canaliculi in them into which Hel is secreted, carried to the lumen of the gastric glands and so to the stomach. The process of acid production by these cells is not fully understood but as the hydrogen ion concentration in gastric juice can be as high as 150 mmol compared with 000004 mmol in blood, hydrogen ions have to be secreted by the parietal cells against a very large gradient. Separate pumps are thought to deal with the hydrogen and chloride ions.
Blood Parietal Lumen vessel cell of Cl- Cl- stomach
Cl-
COz CO2 + HzO 1 eo. boo;<
anhydrase
~C03 !
HCOi+ H+ H+
Figure 1.8 Secretion of He) by parietal cell. The mucous neck cells of the gastric glands secrete both mucus
and intrinsic facto. Mucus, by adhering to the surface of the mucosa, plays a role in the protection. of gastric mucosa from digestion by gastric juice. It has lubricating properties which allow the chyme to move over the mucosal surface and the proteins and bicarbonate in it act as local buffers protecting the mucosa from the hydrochloric acid without altering the pH of the bulk of the contents.
ALIMENTARY SYSTEM AND NUTRITION 11
1.1.3 Protein Digestion The pepsins secreted by the chief cells of the stomach start the
digestion of protein. Enzymes break down proteins by attacking the bonds between the amino-acid units of the molecule with certain enzymes attacking specific bonds. There are several different active pepsins-pepsins I, II and III-derived frum the inactive pepsinogens secreted by the gastric cells. These hydrolyse proteins into polypeptides of various sizes by attacking the bonds within the protein molecule between aromatic and other amino acids. The optimal pH for this reaction is between I and 3, so their activity is stopped on entry of stomach contents into the alkaline milieu of the duodenum. Further digestion of the polypeptides depends on enzymes in the small intestine w h i c h are active in an alkaline environment. 1.1.4 Control of Gastric Secretion
The experimental techniques of 'sham feeding' and 'gastric pouches' have proved very useful in the investigation of the control of gastric secretion. If the eosophagus of an animal is divided and brought to the body surface, then that animal may chew and swallow food but it comes out from the exteriorised oesophagus and does not reach the sto . Gastric pouches are basically of two types: the
Figure 1.9 Oesophagus is exteriorised to allow 'sham' feeding. When food is chewed and swallowed it does nOI reach the stomach. Gastric juice can be collected easily and is uncontaminated by food. This preparation also allows food to be placed directly in the stomach without chewing having taken place. Pavlov pouch and the Heidenhain one. In the Pavlov pouch part of the stomach is made into a pouch so that its lumen is not in continuity
12 PHYSIOLOGY. BIOCHEMISTRY AND BIOTECHNOLOGY
with the main lumen but the blood and nerve supply to both is the same. In the Heidenhain one the nerve supply to the pouch has been cut but it still has an intact blood supply. Pouch secretions can thus be collected easily, uncontaminated by food and the factors controlling these secretions can be studied.
, .
~. '. CNS
Bostrin _+ .......... l~~H~C:l~-J~!M-t1 Secretion '. +
Distension
~4~-'--+------~~ Polypeptides SecretoCJQQues
VOQus
Figure 1.16 Interrelationship of factors causing gastric secretion. Increased vagal activity causes'release not only of Hel but also of gastrin which in turn stimulates He!. Distension stimulates HeI secretion directly and through gastrin released from G cells. Gastrin is also released by polypeptides and secretogogues in the gastric lumen.
There is a small, continuous gastric secretion, which increases markedly during a meal; in adult man this amounts to 2-3 litres/day. The first phase of increased secretion has been called the cephalic phase because it is mediated from the brain via the vagus nerve. This can be shown by sham' feeding when secretions appear in the innervated Pavlov pouch but not in the denervated Heidenhain one. This reflex is partly a conditioned one as the thought of food is sufficient stimulus to produce an increase in gastric secretion, but the smell and taste of food also act as stimuli.
The presence of food in the stomach also causes an increase in
ALIMENTARY SYSTEM AND NUTRITION 13
secretion, the gastric phase; this secretion occurs in both tbe Pavlov and Heidenhain pouches. Since an increased secretion is found in the denervated pouch, the stimulus to secretion must be blood borne. The presence of food in the stomach causes the release of a local hormone, gastrin, from the antral mucosa into the blood by which it is carried to the fundal mucosa to stimulate acid secretion. The main stimulus for gastrin release is the presence of polypeptides in contact with antral mucosa, but distension of the stomach and the presence of substances like alcohol and other secretogogues also act as stimuli. These two controlling mechanisms for gastric secretion are interrelated and indeed synergistic. Vagus
Acid Hormonal inhibition
Acid Gastrin
Duodenum Inhibition of vagal activlty
Figure 1.11 Inhibition of gastric secretion. Acid inhibits gastrin release; its presence in the duodenum causes the reflex inhibition ~f He! release from the parietal cells.
There is evidence that the presence of food in the duodenum may also cause an increase in gastric secretion; gastrin has been isolated from the proximal duodenal mucosa but there is no agreement on the importance of this intestinal phase of gastric secretion.
We have seen how gastric secretion is stimulated, but is there any mechanism for turning it off? It has been observed that when the pH in the antrum falls below 3 inhibition of acid secretion occurs. This results from the inhibition of gastrin release which in turn leads
14 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
to less stimulation of the parietal cells. An additional factor, however, is that the passage of acid, fat and to a lesser extent hyperosmolal solutions into the duodenum also inhibit gastric secretion, and although the vagal nerve plays a role in this mechanism the evidence points to the main inhibition being due to the release of an inhibitory hormone. The hormone responsible is not known and although secretin and cholecystokinin-pancreozymin, hormones involved in the control of pancreatic and bile secretion, have inhibitory effects on gastric secretion there is additional evidence that a separate inhibitory hormone may exist. 1.1.5 Histamine Receptors
We have seen that both acetylcholine, released by vagal nerves, and gastrin cause an increase in gastric acid secretion. For many years it has also been known that histamine will cause an increase in acid secretion by the stomach; the current view is that it has this action by virtue of histamine receptors on the parietal cells of the stomach. Experiments with drugs which block the action of histamine suggest that there are two classes of these receptors: H2 in most areas of the body and ~ on the parietal cells. Drugs are currently available which block these ~ receptors-and thereby heal peptic ulcers-but the physiological role for histamine in normal gastric secretion is not yet clear. 1.1.6 Gastric Emptying
The rate at which the stomach empties depends, to some extent, on the volume of its contents, which suggests that stretching of the gastric wall stimulates stretch receptors which then increase motility. The main control over gastric emptying, however, is exerted by the duodenum. The presence of acid, fat or hyperosmolal solutions in contact with duodenal mucosa results in decreased activity of gastric muscle and, in consequence, a decrease in theamount of gastric contents entering the duodenum. Passage of water into the lumen of the duodenum through the intestinal wall soon renders the contents iso-osmolal, bicarbonate in the pancreatic juice neutralises the acid and the inflow of bile and lipase results in the digestion and absorption of the fat. This mechanism has the logical effect of controlling the rate of gastric emptying so that the duodenum is not at any time overloaded with chyme.
How is this inhibitory int1uence of the duodenum on gastric muscle activity mediated? It seems to be due to both nervous and humoral mechanisms. Vagal denervation of the stomach markedly reduces the
ALIMENTARY SYSTEM AND NUTRITION 15
inhibitory effect of acid or fat in the duodenum on gastric motility; this has been called the enterogastric reflex. The fact that the inhibitory effect, although reduced, is still seen after denervation indicates that the effect must also be produced by humoral means; the name enterogastrone has been suggested for this agent. There is still doubt about the n~ture of this hormone: both secretin and cholecystokinin-pancreozymin have been shown to decrease gastric motility as well as decreasing secretion; polypeptides such as motilin and gastro-inhibitory peptide (GIP) , released from the mucosa of the small intestine, also alter gastric emptying rates, so at present it is probably best to use the term enterogastrone to describe the active agents in this humoral feedback mechanism. 1.1. 7 Intestinal Absorption
The main site of digestion and absorption is in the small intestine. This part of the alimentary tract consists of about 30 cm of duodenum and 240 cm of jejunum and ileum. The small intestine is adapted for absorption in that the surface area of its mucous membrane is increased by infolding and by a large number of finger-like projections, the villi, which project into the lumen. These villi are up to 1 mm in length and covered with epithelium, with capillaries, lymph vessels and smooth muscle fibres in their core. The epithelial cells have a brush border of hundreds of microvilli which increase their surface area and absorptive surface even more. Hydrolytic enzymes are located in this brush border and it is here that the [mal stages of carbohydrate and protein digestion occur. All epithelial cells are formed in the depressions between villi, the crypts of Lieberkiihn, and migrate up the villus to be extruded from its tip over a period of 2 days. These extruded cells add to the enzymic content of the lumenal contents.
The transfer of substances across the intestinal epithelium from the lumen to blood and lymph occurs in different ways. Molecules can diffuse passively down concentration or electrochemical gradients but, for most, an active transport mechanism is required to move them against a gradient. This movement of substances also depends on their physical characteristics; lipid, soluble substances, for example ethanol, move readily through the lining epithelium of all parts of the gut. Watersoluble molecules, unless they have a molecular weight less than 100, do not pass through readily and require carrier mechanisms. 1.1.8 Carbohydrates
The second stage of carbohydrate digestion occurs in the duodenum.
16 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
Smooth muscle __
Micra-vi \Ii --I--"'I!1'111.
Ly:nphotic vessel
(locteall-:ilj~~'- .'IDIt=-1l>
Crypt of lieberkUhn
Artery
Terminal web
To Iymphatlcs
~~==:::~;;;~_Ti9ht ~ junction ~ __ .. _t-Na+ -ti~~~-_...J transport
Microvillus
Figure 1.12 Intestinal villus supplied with a large lymph vessel in addition to a capillary network. Note the smooth muscle fibres from the muscularis mucosa layer which cause shortening vf villi and so aid movement within the lacteals. Inserts show details of cells and a single microvillus; each microvillus has a central cone of microfilarnents which intermingle with the mesh work of microtubuies and ftIaments called the 'terminal wel>'. In some species actm has been idenllfied in the microfilaments and the addition of ATP causes them to contract. Here the bicarbonate in the pancreatic secretion ensures an optimal pH for amylase activity in the subsequent breakc'own of carbohydrate to dextrins and maltose. The maltose is hydrolysed to monosaccharides by maltase and the 1-6 linkages are hydrolys':d by oligo 1-6 glucosidase. The final breakdown occurs mainly in thf. microvilli of the epithelial cells-which contain the enzymes concemed, i.e. maltase, sucrase, lactase, etc. -and not to any great extent within the lumen of the duodenum.
AUMENTARY SYSTEM AND NUTRITION 17
Carbohydrates ingested
__________ I ~ Lactase Starch Glucose Sucrose
Maltolriose Maltose
I Maltase I
Galactose Glucose Glucose Glucose Glucose Glucose Fructose
[ ENZYMES Figure 1.13 Digestion of carbohydrates by various enzymes. The amylase activity takes place in the lumen of the gut: that of the uther enzymes in the brush border.
Absorption. An active carrier mechanism is responsible for the absorption of the monosaccharide end-products of carbohydrate absorption. There is competition between different sugars and they show different absorp tion rates, glucose and galactose having the highest rate. A fll.:tor which affects the rate of absorption is the concentrati0n of sodium ions in the lumen; the fact that ollabain inhibits absorption of S\l2,:!I's points to the probable importance of sodium pumps in the ab~orp\ion process. 1.1.9 irotebns
Secretions from the pancreas entering the duodenum contain trypsin and chymotrypsin, enzymes which break down protein into dipeptides and amino acids; these enzymes, unlike gastric pepsin, are active in alkaline conditions. AllY remaining polypeptides are broken down to their final amino acids by carboxy peptidase and amino peptidase from the intestinal mucosa. Some of this final digestion occurs within the lumen of the gut but much of it is carried out in the brush border of the mucous membrane epithelial cells.
18 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
Absorption. Only amino acids are absorbed into the bloodstream from the lumen of the gut; once again this is by an active process. There appears to be three- carrier mechanisms involved in carrying the amino a,cids according to whether their side chains are neutral, basic or acidic. These carriers also show a preference for laevo amino acids. As with the carriage of sugars, the carriage of amino acids is . linked with the active transport of sodium. 1.1.10 Fats
The main fat in our diet is the ester of long-chain fatty acids and glycerol; this is digested and absorbed in the small intestine. Under normal conditions almost all the fat we ingest is absorbed and only in abnormal conditions do we find fat in the faeces .
. Fat leaves the stomach in large droplets within the aqueous solution of chyme. If it remained in this form the water-soluble lipase, which digests it, would have great difficulty in getting into contact with most of it; however, bile salts emulsify these large droplets, breaking them down into much smaller ones, so enabling lipase to come into contact over a much larger area. Agitation within the duodenum helps break up the large droplets, the lipid part of the bile salt molecule dissolves in the fat and the electric charge on the polar part of its molecule faces outward towards the aqueous phase of the mixture, preventing these droplets from coalescing. The action of pancreatic lipase on the triglycerides in these small droplets results in the formation of di- and monoglycerides, free fatty acids and a little glycerol. Free fatty acids and glycerol help the bile salts in the formation of even smaller droplets called micelles. These are small water-soluble droplets of up to 10 nm diameter. These micelles come into contact with the intestinal mucosa enabling the lipid-soluble free fatty acids and mono glycerides to pass through the epithelial membranes into the interior of the epithelial cells. Within these cells triglycerides are synthesised again from fatty acids and glycerol by the activity of the endoplasmic reticulum. These triglycerides form chylomicrons which are small droplets with over 90% triglycerides with a surface film of lecithin, cholesterol and protein. They are released by the epithelial cells into the interstitial spaces and from there they pass not into the blood capillaries but into the lymphatic channels called lacteals.
Short-chain fatty acids are directly absorbed into blood capillaries; the bile salts which have been left in the lumen of the intestine during this process pass to the terminal ileum where they are actively absorbed and returned to the liver in the blood.
ALIMENTARY SYSTEM AND NUTRITION
la)
Ester linkage
"Fatty+ acid
Bile (b) salts
Lipase
Glycende
Monoglycerides Free fatty acid
~
Fatty acid
Free
fatty acid
Monoglycendes
19
Figure 1.14 (a) Pancreatic lipases show specificity for the I-ester linkages on the rriglycerides. The end products are: (i) free fatty acids; (ii) 2-monoglvcerides; and (iii) a small amount of glycerol. (b) Formation of a micelle. The water-insoluble fatty acids and mllnoglyceTldes are solubilised in the hydrophobic centre of the micelle.
1.1.11 The Structure and Catalytic Mechanisms of Pancreatic Enzymes
The enzymes secreted by the pancreas need (a) to be activated from precursors, (b) to recognise the peptide bond which is to be
20 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
attacked, (c) attack this bond and (d) be inactivated when the process is over. Recent evidence using the techniques of molecular biology has given much new information on this process; this will now be outlined.
+ Bile salts o Free folly acids Glycerides
Ta ileum ++
Micelles
Protein
@) @ +- Chylomicron'3
Lymphatic f
ALIMENTARY SYSTEM AND NUfRITION 21
This mt:chanism of activation, recognition, catalysis and inhibition has been described in some detail because it appears to be exploitt:d over and over again for different functions; examples are: the c1ottinr, of blood; the dissolution of blood clots; the disposal of complexes of antigen and antibody by complement; and in some functions of kinins. 1.1.12 Control of Pancreatic Secretion
The exocrine secretions of the pancreas are of two types: a watery solution with a high bicarbonate content which is secreted by the cells lining the ducts of the glands; and a secretion rich in enzymes which comes from the acinar cells at the base of the glands.
Recognition pocket closed
RecOgnition
! Trypsin pocket open -I(fo;~~
Recognition pocket occupied
by side chain of protein
~ + protein
Protected bond
Inactive enzyme
I Active enzyme
1 Enzyme blocked by molecule
Figure 1.16 Diagram showing activation. n:cognition. catalysis and inhlbll'
22 PHYSIOLOGY. BfOCHEMISTRY AND BIOTECHNOLOGY
As with most glands the pancreas has a resting secretion level which increases when food is eaten. The initial increase is due to increased vagal activity as in the cephalic phase of gastric secretion; the presence of food in the stomach causes a further increase in secretion due to the release of gastrin which stimulates the release of a bicarbonate-rich secretion. The main secretion from the gland occurs, however. when gastric contents enter the duodenum. TIle characteristics of the secretion depends on the type of chyme entering the duodenum; if the chyme is acid then the pancreatic secretion is rich in bicarbonate which neutralises the acid; this response is mediated by the release of the hormone secretin from the duodenal mucosa. (Incidentally secretin was the first gastro-intestinal hormone to be discovered.) The presence of amino acids and fatty acids in the duodenal contents results in a pancreatic juice rich in enzymes being released, the mediator in this case is another duodenal hormone cholecystokinin-pancreozymin (CCK-PZ), which as its name implies was described originally as two separate hormones. 1.1.13 Control of Bile Secretion
Bile, which is required for the digestion and the absorption of fat, is secreted by liver cells into small ducts which eventually converge into the common bile duct by which bile is conveyed to the duodenum. As the bile duct leaves the liver it is joined by another duct coming from the gall-bladder, a small sac lying under cover of th: liver. Just before it enters the duodenum the bile duct is usually joined by another duct coming from the pancreas, and the resultant ('1let carries both bile and pancreatic secretion into the gut. At a point of entry the duct is surrounded by smooth muscle, the sphincter of Oddi.
Bile is secreted continuously by liver cells but does not enter the duodenum because the sphincter of Oddi is normally closed. This results in bile being diverted into the gall-bladder where sodium is actively absorbed from bile into blood, with water following by osmosis. The bile is therefore concentrated in the gall bladder. Bile ~ consists of (a) bile salts, (b) cholesterol, (c) lecithin-a phospholipid-
and (d) bile pigment. The bile pigment, which gives bile its yellow colour, is bilirubin, a breakdown product of haemoglobin. This is changed in the intestine to a brown pigment which gives faeces their normal colour. If bile pigment is prevented from reaching the intestine faeces become greyish-white.
The secretion of bile by the liver is a continuous process; up to
ALIMENTARY SYSTEM AND NUTRITION 23
1000 mllday being formed. This rate of secretion is increased by substances called cholertics, one such substance being the bile salts themselves. After bile salts have assisted in the absorption of fat they are absorbed in the ternlinal ileum and carried in the venous blood from the intestine which ends in the portal vein. This vein enters the
Gall bladder
Na+ and H20 to bloodstream
Sphincter ofOddi __ ./
__ ~ ___ Duodenum
Figure 1.17 Storage and concentration of bile in the gall bladder and the route to the duodenum. liver and breaks up into a second type of capillary bed in the liver before returning from the liver to the right atrium in the hepatic vein. This portal circulation ensures that substances absorbed from the intestine are carried first to the liver. The bile salts are thus returned to the liver where they act as cholertics and are released again into the intestine in bile. This has been called the entero-hepatic circulation. As the total amount of bile salts in the body is about 3 g, and up to 8 g may be required for the digestion and absorption of a fatty meal, it is very necessary that this recirculation exists.
Although bile is secreted continuously, in man it is stored in the gall-bladder until required for the digestion of a meal. Contraction of a gall-bladder and relaxation of the sphincter of Oddi results in bile gaining entry to the duodenum. The mechanism controlling this discharge of bile is twofold, first the increased activity of the vagus which accompanies eating causes contraction of the gall-bladder and later the cholecystokinin-pancreozymin released from the duodenum also has this effect.
24 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
1.1.14 Motility of Small Intestine Various types of movement of the small intestine have been
described; their purpose is to mix the contents with digestive secretions, allowing the digestive end-products to come into contact with the mucosa so they may be absorbed, and to move the residue onwards into the large intestine. The main mixing movement is segmentation in which rings of intestinal wall contract, dividing the contents into segments. These rings of wall then relax and adjacent rings contract, breaking up the first segments. One of the reasons for chyme moving along the intestine is that the frequency of segmentation
Figure 1.18. Segmentation; as the rings of contraction occur at different points in the intestine the contents are moved in opposite directions and mixed. is greater at the duodenal end than the ileal end of the intestine. In addition, there is peristaltic activity in the small intestine which always proceeds towards the large intestine, although these waves of contraction only travel a few centimetres and then cease. Peristaltic waves do not normally travel along the whole length of the intestine as in the oesophagus. Distension by the intestinal contents causes an increase in muscle activity. The motility is coordinated by the internal nerve network; parasympathetic nerve activity increases and sympathetic activity decreases the general level of activity. 1.1.15 Absorption of Water and Electrolytes
Water moves freely in either direction through the intestinal wall, depending on the osmotic gradient. Although the average intake of water only amounts to about 1200 mI/day, a large amount of water is found in the secretions poured into the intestine each day, and as the average water content of faeces is only about 100 mI/day a large quantity must oe absorbed. This takes place mainly in the small intestine. In most parts of the gut the contents are nearly isotonic as water quickly follows the osmotic gradient (mainly due to sodium); as in other areas of the body where sodium ions are absorbed, this process
ALIMENTARY SYSTEM AND NUTRITION 25
is affected by blood aldosterone levels. Chloride and bicarbonate ions may be actively absorbed or may follow passively. Sulphate and magnesium ions are not well absorbed and their presence in lumenal fluid will tend to hold water there, so producing a large volume of intestinal contents and thus acting as a purgative.
Water reabsarbed =::::::;E:---into blood
Mouth
Food (8009) +
Fluid (1300 mll
~
__ Saliva (1200ml)
Gastric juice (3000ml)
Bile (500mll - Pancreatic juice 11000 mll
Intestinal secretions (2000 ml)
Faeces [Water (lOOml) + Solids (60 91] Figure 6.19 Although large volumes of water are secreted into the gastrointestinal tract only 100 rnl remain in faeces.
1.1.16 Vitamins Water-soluble vitamins are freely diffusable and so rapidly
absorbed in the small intestine. One of them does depend for absorption on the presence of a mucopolysaccharide from the stomach, the intrinsic factor. This absorption takes place in the terminal ileum.
Fat-soluble vitamins are absorbed along with fats in the jejunum. 1.1.17 The Large Intestine
The colon or large intestine forms the final part of the gastroint-estinal tract and, as its name implies, it is wider than the small intestine and not so coiled. Its function is to absorb water and electrolytes from chyme, and to store the resultant faeces until the time is convenient for their excretion. About 500 ml of chyme enters through the ileocaecal valve daily and normally 400 ml of water would be absorbed, although
26 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
this does depend on the length of time the contents stay in the large intestine. Active absorption of sodium is again the _ mechanism responsible for the removal of water. The potassium content of the intestinal contents is greater than the plasma level, potassium being exchanged for the sodium absorbed.
Hepatic flexure_
Ascending colon __
Taenia -~i-+'
Ileo-caecal valve
Caecum
Transverse colon
Figure 1.20 The large intestine.
Splenic flexure
Descending colon
Sigmoid colon
t--_______ Rectum
Peristaltic movements travel for greater distances in the large intestine than in the small intestine, propelling the contents into the sigmoid colon. A non-propulsive movement like segmentation also occurs and is responsible for mixing. 1.1.18 Defaecation
When the contents of the sigmoid colon are carried by peristalsis into the rectum, the distension of the rectal ~alls acts as a stimulus for defaecation. If conditions are appropriate, further peristalsis occurs in the sigmoid colon, the rectal walls contract and both the internal and external anal sphincters relax resulting in the elimination of faeces through the anus. This is usually assisted by inhalation of a deep breath, closure of the glottis and an increase in intra-abdominal pressure due to the forced contraction of abdominal muscles. If circumstances are not suitable for defaecation, the external anal sphincter-which is under voluntary control-remains closed, the intestinal muscle activity
ALIMENTARY SYSTEM AND NUTRITION 27
is depressed, the rectal wall relaxes and so the urge to defaecate disappears.
1.2 METABOLIC RATE Catabolism, or the slow controlled combustion of molecules of
carbohydrates, fat and protein which occurs in the body, results in the release of energy from the breaking of carbon and hydrogen linkages. The energy thus liberated is either given off immediately as heat or stored as energy in the form of A TP. This energy store is used to perform both external work (movements through the contraction of skeletal muscle), or internal work (functional activities of cells). The units used for the measurement of energy are kilocalories (240 kcal=l06 J=lMJ).
Total energy = energy stored + energy used + heat When foodstuffs are burned outside the body the heat produced,
and so its potential energy, can be measured. The amounts of energy produced in the body in the catabolism of food is not exactly the same but are approximately equal to 4 kcal/g for carbohydrates and protein, and 9 kcal for fat. The amount of energy liberated by the body in unit time is called the metabolic rate.
The heat output from man can be measured directly in a human calorinleter, but is more often done by indirect calorimetry. This depends on the fact that the amount of heat produced when 1 mole of oxygen is consumed in the oxidation of different foodstuffs is known. To do this calculation the relative amount of fat, carbohydrate and protein needs to to be known. This additional information can be obtained from the respiratory quotient (RQ). This is the ratio of the volume of CO2 produced to the volume of 02 consumed when a substance is oxidised,
e.g. C6H1P6 + 602 = 6C02 + 6Hp so the RQ for carbohydrate is 1. The RQ for fat is about 0-7 and for protein approximately 0 82.
The RQ of the whole body can be calculated from analysis of expired air, but factors other than metabolism, for example an increase in ventilation, will vary the ratio of CO2 exhaled to 02 inhaled. Measurement of the CO2 exhaled to 02 inhaled ratio is now usually referred to as the respiratory exchange ratio (R).
As the body consumes a mixture of carbohydrate, fat and protein, the energy liberated when I litre of oxygen is consumed is approximately 482 kcal. If we therefore measure the oxygen consumed by a subject
- 28 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
we can calculate the energy production or metabolic rate by multiplying the 02 consumed per minute (STPD) by 482.
The metabolic activity of an individual will vary with activity, so that in order to make comparisons of the metabolic rates it must be determined under standardised resting conditions. It is then known as the basal or resting metabolic rate; in an average adult male this amounts to 2000 kcal (84 MJ) per day.
There must be a balance between the energy output of a person and the potential energy or calorific value of food ingested. If the calorific value of ingested food is greater than his energy output, the energy is stored and a person gains weight. Food intake and energy expenditure vary widely from day to day and, although body weight varies over time, it is constant enough to suggest there must be a mechanism which regulates it.
Many mechanisms are advanced to account for the close matching of caloric intake to energy expenditure in normal animals; it has, however, proved difficult to decide which are the most important. From a consideration of other control systems it is thought that there must be sensing devices which monitor food intake and the current amount of foodstuffs in the body; also neural mechanisms in the hypothalamus to integrate these signals, and effector mechanisms which cause the animal to hunt and eat food.
Possible sensory inputs involved in these mechanisms are: I. A system in the mouth or eosophagus which monitors the
food intake; for 'sham feeding' leads to cessation of feeding even though the food is not absorbed into the body.
2. A system which responds to distension or partial filling of the stomach; for distension of the stomach leads to cessation of feeding, and if the stomach is partly filled (through a stomach tube) the animal, or man, only eats enough to make up its normal intake. 3 A system of receptors (perhaps in the hypothalamus) which respond to the circulating levels of glucose and fatty acids in the blood.
The hypothalamus is thought to contain a 'feeding' or 'hunger' area and a separate 'satiation' area; destruction of the former produces animals which will not eat, destruction of the latter produces animals which overeat and become obese.
The control of food intake is not always successful in keeping the body weight constant; when errors occur they are in the direction of too much weight gain rather than too little. Perhaps, as with the
ALIMENTARY SYSTEM AND NUTRITION 29
control of fluid intake, our mechanisms are more successful in guarding against deficits rather than excesses. Some animals (rat and possibly man) gain much more weight if fed a constant amount of food in a few big meals than in many small ones, but there is no resulting alteration in food intake-a puzzling finding. It has been suggested that appetite control is more successful at high rather than low exercise levels; this may explain Western man's difficulty in controlling his weight. In man it has been suggested that eating habits together with some voluntary control (clothes getting tighter, etc.) is enough to regulate body weight.
Our diet is composed of carbohydrate, protein, fat, vitamins, minerals and water. In the diet of most people carbohydrate forms the biggest portion; the poorer the individual or community the greater the percentage of carbohydrates. Most of it is eaten in the form of starch in grain or root vegetables, although an increasing amount in the diet of the more 'advanced' societies is in the form of sugars. Most of the sugars are the disaccharides, sucrose, lactose and maltose with ~ little as the monosaccharides, glucose and fructose.
Proteins not only act as a source of energy, like carbohydrates and fat. but supply the nitrogen and sulphur required for the synthesis of proteins to replace the body proteins which are continuously being broken down. This is a constant need for normal maintenance, but the body's protein requirement is obviously increased in children for growth and in mothers during pregnancy and lactation. A simple guide to our protein requirements is that for each kg of body weight we require I g in our diet. This is a generous allowance and, as protein is expensive and its supply is inadequate in many areas of the world, many people exist on much less, but it is a good level to aim for in order to provide a safety margin. Some amino acids are not synthesised in the body and so must be present in our diet; these are called essential amino acids. Because all proteins do not contain all possible amino acids, we find that some are more suitable as a human dietary protein than others and for this reason it is wise to provide a mixture of proteins in our intake.
Fats, because of their high calorific value, make up a large proportion of the energy we derive from our diet. This is not necessarily taken as obvious fa( but forms part of much of the food we eat; indeed it is necessary to improve the palatability of our food, as can be vouched for by anyone who has had to take a low-fat diet for any length of time.
30 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
Oesophageal monitoring
of food intoke
F"""'''ol ~ th."~'h / Receptors for measuring the
blood concentration
of glucose and fatty
acids
? Voluntary control (man)
1
Figure 1.21 Suggested mechanisms for appetite control.
_____ Appetite
'& Behavioural challQes
Our daily calorific requirement obviously varies with our age, size and activity but for an adult male of sedentary disposition 2800 kcal (11 7 MJ) would suffice. Remembering that the calorific value of carbohydrate and protein is 4 calories and of fat 9 callg, a reasonable diet might be as follows:
cal MJ 375 g of carbohydrate 1500 6-27 100 g of protein 400 1-67 100 g of fat 900 376
2800 11-70 Vitamins. These are organic substances in our diet which are
essential, as the body cannot usually synthesise them. They are required in many enzymatic processes and their absence leads to deficiency diseases. Since they have been isolated and synthesised they have been given their correct chemical names but are still often referred to by letters. They can be classified into two groups, the fat-soluble Vitamins A, D, E and K, and the water-soluble Vitamins Band C.
Mineral and water. The normal minerals in our diet, sodium, potassium, calcium, phosphorus and iron, are dealt with in other sections of the book.
ALIMENTARY SYSTEM AND NUTRITION 31
Table 1.1 Fat-soluble vitamins. Vitamin Chemical Source Deficiency disease
name
A Retinol Dairy products Night blindness Liver Some can be formed Keratinisation of in gut from carotene epithelium
D Cholecalciferol Dairy products Rickets in Eggs children Liver oil Some can be formed Osteomalacia in in skin from action adults of UV light on 7-dehydrocholesterol
E Tocopherol Wheatgerm Unknown F Naphthoquinone Green vegetables Not primary
derivatives Synthesised by gut failure to absorb bacteria it in disease of G-I
tract or sterilisation of gut with antibiotics leads to failure of prothrombin
Table 1.2 Water-soluble vitamins. Vitamins Chemical Source Deficiency disease
name
C Ascorbic acid Citrus fruit Scurvy Blackcurrants Fragility of blood Vegetables vessels
B complex B, thiamine Wheatgerm, pulses, Beriberi, polyneuritis, yeast heart failure
B2 riboflavin Meat, milk, Degeneration of wholemeal flour, skin-mucous
membrane beer junctions
Nicotinic acid Milk, liver, yeast Pellagra, dermatitis, dementia, diarrhoea
Pantothenic acid Widely distributed None known Pyridoxine Widely distributed None known B,z cyano- Foods of animal Pernicious anaemia, cohalamin origin lack of intrinsil:
factor, thus failure of absorption
32 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
Trace elements. Certain elements are needed in our diet in very small amounts and are present in tissues in as small a concentration as 1 part in 20,000. These are called trace elements; the most important are iodine, copper, cobalt, manganese and zinc.
2
Respiratory System
2.1 RESPIRATION Respiration is the transfer of gases between body cells and the
environment. It goes hand in hand with metabolism, the process by which food produces energy for the needs of the body. In metabolism oxygen is taken from the environment and carbon dioxide added to it; in our bodies these processes proceed at 37'C due to the presence of catalysts-the enzymes. Lavoisier thought that similar processes occurred in a flre and in animal metabolism as in both q is absorbed, CO2 given off and energy produced. We now know that, though the end results of these processes are similar, the detailed reactions are very different; in metabolism hydrogen is removed from substrates whereas in a flre oxygen is added to them. The reason for these differences is probably that animal metabolism evolved before the atmosphere contained oxygen to act as an electron acceptor; so metabolism predates combustion. 2.1.1 Diffusion of Gases in Respiration
Most living animals ultimately gain their 02 and lose their CO2 by diffusion. '1 hIS IS the process whereby a net movement of molecules occurs from an area of higher concentration to one of lower concentration. The rate at which substances diffuse increases with the driving force and the area available for diffusion and decreases with the distance. Diffusion in gases is much faster than in liquids because the molecules in a gas are less tightly packed. Such a transfer of substances is fast over short distances but very slow over large distances. As animals increase in size there are two reasons why the
33
34 PHYSIOLOGY. BIOCHEMISTRY AND BIOTECHNOLOGY
supply of gases by diffusion becomes inadequate. The first is that the distance for diffusion becomes too great and the second IS that the surface area of the animals becomes relatively smaller than the mass of the metabolising tissue. With spherical animals this point is reached at sizes of about 1 mm. All animals with sizes greater than this require a specialised respiratory system together with an associated circulatory system. In man this respiratory system consists of lungs in which gas movement occurs by a bellows action of the chest wall. which creates a negative pressure in the chest and so draws air in. As we require a large gaseous exchange with the environment the surface area of our lungs is very large due to their division into hundreds of millions of small air spaces, the alveoli. 2.1.2 Ventilation of the Lungs
Distribution of gas and blood to the lungs. Air is filtered by hairs in [he nose-which remove the larger dust particles-moistened and warmed by the mucosa of the nose and pharynx so that by the time
F'1gure 2.1. Schematic dlagrdm of lung function.
Bulk flow (external "breathing") respiration Diffusion
Bulk flow (transport in blood) Diffusion
Internal respirotion
it reaches the trachea it is saturated with water vapour and is at body temperature. The hairs in the nose only tilter out gross particles from the inspired air, and particles smaller than I pm stay in suspension and are breathed out again. Dust of interIP~diate size, that is from 10 down to 1 pm, is removed from the ai during its passage along the respiratory tract, the larger particles in the nasopharynx and upper respiratory tract and the smaller in tP..! bronchial tree itself. An important factor in this filtration is thl' presence of mucous on the surface of the respiratory tract epithelium. Turbulence occurs in the air flow as it changes direction, particles impinge on the walls and
RESPIRATORY SYSTEM
Table 7.1 Symbols used in respiratory physiology. Primary symbols P pressure or partial pressure V volume of gas V volume of gas per unit time F fractional concentration in dry gas Q volume of blood Q volume of blood per unit time C concentration of gas in blood S percentage saturation of haemoglobin with 02 Secondary symbols 1 Gas phase
I inspired air E expired air A alveolar air T tidal air D dead space air B barometric
2 Blood phase a arterial blood v venous blood c capillary blood v mixed venous blood c' end capillary blood
Examples Partial pressure of CO2 in mixed venous blood Pv, co2 Fractional concentration of N2 in inspired gas PI' N2 02 concentration in arterial blood Ca, 02
35
are trapped in the mucous. This particle-laden mucous must then be disposed of and this is the task of the ciliated epithelium. The epithelium of the respiratory tract is ciliated. that is it has minute hair-like projections from its surface on which the sheet of mucous is carried, These cilia move in a coordinated fashion with a fast stroke in one direction and a slow one in the other. This has the eHect of carrying the sheet of mucous, with its entrapped particles, ill onc dire('tioll, downwards in the nasal mucosa towards thl' pharynx and
36 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
upwards in the bronchial tree to the pharynx. Once in the pharynx the mucous is unconsciously swallowed.
The ciliated epithelium ends at the terminal bronchioles, so what happens to particles which are deposited in the respiratory bronchioles and the alveoli? In the main they are mopped up by wandering alveolar macrophages which get to the mucociliary 'escalator' and so to the pharynx, or are carried away in lymph vessels or are sequestered in lung tissue by a tissue reaction.
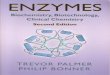
The trachea divides into right and left branches and then continues dividing into smaller and smaller bronchi, fmally reaching the terminal bronchioles which lead to the alveoli. The incoming air thus eventually reaches the alveoli where the main exchange of CO2 and 02 occurs. These alveoli are some 100-300 pm in diameter and consist essentially of a bundle of capillary vessels suspended in air. Most of the alveolar surface is covered by these blood vessels, which are some 1500 miles in length spread out over the 40-60 m2 of diffusing surface. At rest the capillary blood is renewed every second and during exercise every third of a second or less. To do so the total blood flow is about 5 titres/minute at rest and during exercise about 20-30 litres/minute. The air flow to the alveoli is about 4 litres/minute at rest and up to 100 litres/minute during exercise.
The details of the blood and air flow to the lungs will be considered in more detail, separately. 2.1.3 PuImonary Circulation
The pulmonary circulation, being in series with the systemic one, receives the total cardiac output. The right ventricle pumps this blood-mixed venous blood-through the pulmonary artery to the lungs, and its branches accompany the bronchioles to the terminal bronchioles where they break up into the capillary bed.
02 removal from lungs = arterial-venous oxygen concentration x blood flow or
blood flow = 02 uptake arterial - venous oxygen cOllcentratio
all per unit of time. If 02 usage is 250 mllminute and arterial and venous contents are
200 and 150 mlllitre the cardiac output = 5 litres/minute. This neglects the nutritional blood flow.
The main difference hetween the pulmonary circulation and the
RESPIRATORY SYSTEM 37
systemic one is that it is a low-pressure system with a systolic/diastolic pressure of 25110 mmHg (33/13 kPa) and a mean pressure of IS mmHg (2 kPa). The left atrialpressure is about 6 mmHg (08 kPa), so the driving force for blood flow through the pulmonary circulation is only some 10 mmHg (13 kPa) compared to about 80 mmHg (106 kPa) for the systemic one. As the same volume of blood flows through both circulations this means that the resistance to flow in the pulmonary circulation is much less than iri the systemic one; this is because the walls of the pulmonary arterioles are much thinner and contain less smooth muscle than those elsewhere.
__ Oxygen consumption V02
Blood flow 0
Figure 2.2 Measuring cardiac output by the Fick prinCIple. Blood leaving th. lung~ contains more oxygen than blood entering the lungs. This difference in amount IS equal to the oxygen added by the lungs. So
When cardiac output rises, as in exercise, the pulmonary arten pressure does not rise and this must mean that resistance to blood 0(1\\ through the lungs decreases. There is both an increase in the diamelel of pulmonary vessels and an opening up of some which have heen closed under resting conditions; this results in a decreased resistance to flow, so enabling the pressure to remain low.
The pulmonary circulation is also different from the systemic onc in other respects:
1. The capillary network is more dense in lung than elsewhere in order to give a large interface for gas exchange.
2. Because the hydrostatic pressure in lung capillaries is always much lower than the oncotic pressure of the plasma protein there is less tiltration of fluid out of the capillaries into the lung interstitial space.
3. The pulmonary arterioles constrict to a fall in P02 or a rise in Pco~, the opposite of what happens in the systemic
38 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
circulation. This has the 'useful' effect of diverting blood away from poorly ventilated segments where less exchange of gases could occur.
Pulmonary vein ___
\
Lymphatics
Vasomotor nerves
Pulmonary
(artery
;
_ Vasometer I nerves
/ Lymphatics
Figure 2.3 Composite diagram (Jf thf lung s!ructul'el>. The diagT"dm on the left is taken from a ca,t of the airw'IY~ of a human lung. showing airways from rhe trachea to the nght terminal bronchioles (the alveoli are removed). The diagram on the right continues the airways down to the alveoli. Note the difference in scales.
4. Because mean pressure is so low the difference due to gravity above and below heart level is significant, particularly in the upright posture. Blood is therefore normally distributed preferentially to dt:pendem parts.
2.1.3 Me(:hanic~ of Respiration Air moves into and (Jut of the lungs as a result of changes in
... res
RESPIRATORY SYSTEM 39
shrinking passively. The energy for these changes comes from contraction of the diaphragm at the bottom of the chest cavity and the muscles of the chest wall. The lungs do, however, contribute an elasticity to the system by virtue of their tendency to collapse. Nonnally they are prevented from doing so by adhering to the inside surface of the barrel-like thoracic cage.
Blood flow
~?~mlL,--- Interstitial space
Figure 2.4 Forces and fluid movement in lung capillaries. Bulk flow of plasma filtrate occurs into the interstitial space, as elsewhere; it is then either reabsorbed or forms lymph. Little fluid passes into the alveoli mainly because of the presence of tight junctions between the alveolar epithelial cells. Gas exchange occurs at the 'thin regions' shown.
About 500 rn1 of air are taken into the chest during each breath as a result of descent of the diaphragm and the elevation of the rib cage. The descent of the diaphragm occurs because of nerve impulses in the phrenic nerve supplying it; the rib cage is altered mainly by the contraction of external intercostal muscles. During quiet respiration movements of the diaphragm account for 75% of the air movement. Because of the way the ribs are articulated, the breadth as well as the depth of the chest is increased during a breath.
At the end of a normal quiet inspiration the nervous activity
40 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
driving the muscles of the diaphragm and chest wall falls off, and the chest size decreases due to the elastic recoil of the lungs. So at the end of a normal expiration the elasticity of the lungs tending to cause them to collapse is exactly balanced by the elastic tendency of the chest wall to expand. During vigorous respiration this passive collapse of the chest and diaphragm is too slow, and active expiration occurs. This involves various thoracic and abdominal muscles which pull the chest wall-down and push the diaphragm up, thus increasing the rate of expiration.
Figure 2.5 Diagram showing the tendency of the lungs to collapse and the tendency of the chest wall to expand. At the end of a normal expiration these forces are balanced.
Quantitative information on the mechanical factors modifying breathing has been obtained by measuring pressures in various parts of the system, together with the volume of gas breathed into and out of the chest and the rate of gas flow. The important pressures are:
1. The intrapleural or intrathoracic pressure, which is measured in the 'space' between the pleural membrane lining the inside of the chest wall and that lining the outside of the lung. (These layers are normally only separated by a thin film of pleural fluid.)
2. The intrapulmonary pressure, which is the pressure inside an airway. The place where it is measured must be specified as there is a pressure gradient between the mouth and the alveoli, with the alveolar pressure most negative during inspiration. It is this pressure gradient which 'pulls' the gas along the airway.
3. Atmospheric pressure is the reference level to which the others are compared.
RESPIRATORY SYSTEM
Inspiration: Expiration o I
-6 ~---..
-7
- 8 1--'---"'''1''''''-------4 +0.5
'-----+0
-0.5
+1 '------.0
-I
41
Figure 2.6. Alveolar pressure, intrapleural pressure and volume of air breathed. plotted during one respiratory cycle.
The effect of the inspiratory effort is to reduce the intrathoracic pressure, which causes a reduction in the alveolar pressure and thus causes a gas flow to occur.
The intrapleural pressure may be measured by inserting a hollow needle, connected to a manometer, through the chest wall so that the needle tip lies between the two pleural layers. Normally it is negative (or subatmospheric) throughout the cycle, with a value of about -5 cmH20 (-05 kPa) at the end of a quiet expiration. At the end of a deep inspiration it may become -20 cmH20 (-20 kPa), and during forced expiration against a resistance, for example, blowing bagpipes, it may reach + 70 cmH20 (+ 69 kPa) or so. The relation of the change in intrapleural pressure to the volume of air inhaled is about 02 litres/cmH20 (i.e. if the pressure drops by I cmHp, 02 litres of air are inhaled).
Air flows through the airways because there is a pressure difference between the alveoli and the atmosphere. This circumstance may be used to calculate a resistance to flow, using Ohm's law. In a normal subject this is about 2 cm/litre/second, i.e. if air is breathed
42 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
in at a rate of I litre/second, there is a 2 cm Hp drop of pressure between the alveoli and the atmosphere.
During one respiratory cycle the events are quite complex. Figure 7.6 shows these various pressures, volume changes and rate of gas flow during one breath. Air flow into and out of the lungs depends on the pressure difference between atmospheric air and that in the alveoli. The alveolar pressure depends on the algebraic sum of the pressure created by the lung elasticity, and the superimposed pressure due to respiratory muscles. Pressure swings are much greater during heavy breathing leading to more rapid flows of air. To create a pressure difference requires work and larger pressure differences require more work than small ones. During vigorous breathing the work of breathing is therefore greater than at rest.
Lung elasticity + sur face tension of alveolar fluid
o~ __________________________ ~
+ Pressure
Figure 2.7 The behaviour of isolated lungs to changes in pressure. The lung elasticity was obtained by inflation with saline whereas the lung+ surface tension was obtained by air inflation.
The elastic behaviour of lung is made up of two different components; that due to the elasticity of the lung tissue and that due to the surface tension of the thin layer of fluid lining the alveoli. These may be shown by inflating an isolated lung with air-which measures both componentsand then with saline, which removes the surface tension effect and so measures that due to the tissue elasticity. The elastic property of lung tissue is fairly constant with distension, whereas that due to lung and surface tension is complex and differs depending on whether the lung is being inflated or deflated, i.e. shows hysteresis. This complexity is due to the effects of the surface tension of the fluid lining the alveoli and small bronchioles.
RESPIRATORY SYSTEM 43
We all know that it is more difficult to start inflating a balloon than to continue inflating it once it is big. This is partly because the wall becomes thinner as the size increases, but largely because of the physical properties of spheres. This can be studied most easily in gas bubbles which have a constant wall thickness; small bubbles require a greater force to stop them collapsing than larger bubbles. 'Fhis can be shown by connecting a large and small bubble together, the small one collapses and empties into the larger one. It would clearly be inconvenient if small alveoli in the lungs collapsed and emptied into larger ones. This effect is counteracted in normal lungs by the presence of surfactant, which not only diminishes the surface tension but also diminishes it more in the smaller alveoli than in the larger ones. Surfactant therefore adjusts the surface tension of the wall of an alveolus to correspond with its size. Reducing surface tension also decreases the force causing the exudation of fluid from the capillaries.
The alveoli can be considered as spheres of various sizes. The relationship between the internal pressure (P) applied to them, the wall tension (T) and radius (rJ is described by Laplace's law:
P=~ The work of breathing is of two kinds: non-elastic required to
move air through the airways; and elastic required to overcome the elasticity of the lungs and chest wall. The non-elastic work depends on the rate of breathing, for as the rate increases the velocity of air flow in the airways increases and so there is an increase in frictional work; whereas the elastic work depends 011 the depth of breathing for as the depth increases the lungs need to be stretched more. The amount of air breathed depends both on the rate and depth, so that any particular ventilation can be obtained by various combinations of these. If the total work of breathing is measured over a range of different combinations of rate and depth at constant ventilation then a minimum value is found. In natural breathing rate and depth are set to this minimum value. It is an interesting but so far unresolved question as to how the body works this out; perhaps it is related to volume information via the vagus and length-tension infomIation from respiratory muscles. It is likely that the total work of breathing rarely exceeds 3 % of the total energy expenditure of the body.
The non-elastic frictional work is small during quiet respiration, for the frictional resistance to air moving through the airways is then not very great. The friction is enough, however, to mean that the air
44 PHYSIOLOGY, BIOCHEMISTRY AND BIOTECHNOLOGY
p:~ ,
A
! Air-fluid~ interface ~
Some surfactant
B present
0---0---0
c
! 0-------0
Figure 2.8 Surface tension is due to intermolecular attraction forces (A). Surfactant (the black circles) reduces this attractive force between molecules (B); the smaller the surface area, the less is surface tension (C). The higher pressure in the alveolus (A) would cause air to pass into the other two, with collapse of A.
\
III
, ,
\ \
'-
'-,
Elastic~""
Increasing volume decreasing rate [slow deep breaths]
.....
/ ./
,./ ,/ Non-elastic
or frictional
Decreasing volume increasing rate [fast shallow breath~
FIgUre 2.9 The work of breathing at constant total ventilation but differing combinations of rate and volume.
RESPIRATORY SYSTEM 45
flow, and so the change in volume, lags slightly ,pn the pressure so th