Embed Size (px)
Citation preview

PANCREATIC AND HEPATOBILIARY DISORDERS IN INFLAMMATORY BOWEL DISEASE
BENGTHEIKIUS
Department of internal Medicine,Vaasa Central Hospital
Department of Internal Medicine,University of Oulu
OULU 2000

BENGT HEIKIUS
PANCREATIC AND HEPATOBILIARY DISORDERS IN INFLAMMATORY BOWEL DISEASE
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in Auditorium 10 of the University Hospital ofOulu, on October 6th, 2000, at 12 noon.
OULUN YLIOPISTO, OULU 2000

Copyright © 2000University of Oulu, 2000
Manuscript received: 23 August 2000Manuscript accepted: 28 August 2000
Communicated byDocent Risto JulkunenDocent Isto Nordback
ISBN 951-42-5756-1 (URL: http://herkules.oulu.fi/isbn9514257561/)
ALSO AVAILABLE IN PRINTED FORMATISBN 951-42-5755-3ISSN 0355-3221 (URL: http://herkules.oulu.fi/issn03553221/)
OULU UNIVERSITY PRESSOULU 2000

Heikius, Bengt, Pancreatic and hepatobiliary disorders in inflammatory boweldiseaseDepartment of internal Medicine, Vaasa Central Hospital, , FIN 65130 Vaasa, Finland, Departmentof Internal Medicine, University of Oulu, P.O.Box 5000, FIN-90014 University of Oulu, Finland2000Oulu, Finland(Manuscript received: 23 August 2000)
Abstract
Extraintestinal manifestations in inflammatory bowel disease (IBD) have been described with vary-ing frequencies. The aim of this study was to estimate the prevalence of pancreatic duct abnormalities,exocrine and endocrine dysfunction, elevated pancreatic enzymes, hepato-biliary disease, coexistingcholangiographic and pancreatographic duct changes, and elevated serum levels of fibrosis markersin IBD, and to correlate the findings with clinical, endoscopic and histologic variables.
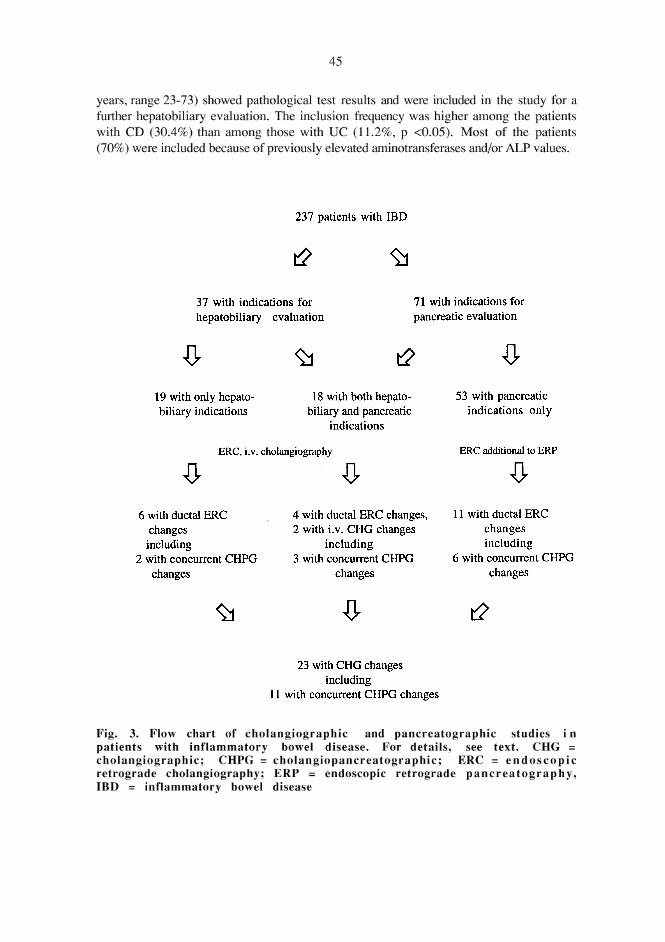
From a local patient register, 237 patients were randomly selected and studied. Of these, 170 hadulcerative colitis (UC), 46 had Crohn’s disease (CD), and 21 had indeterminate colitis (IC). A detailedhistory was obtained from medical records and in a face-to-face interview. The patients were screenedwith a para-aminobenzoic acid (PABA) test and, for pancreatic enzymes, liver function tests, serumaminoterminal propeptide of type III procollagen (PIIINP), and laminin. Further pancreatic evalua-tion included endoscopic retrograde cholangiopancreato-graphy (ERCP), ultrasound (US), secretintest, and glucagon C-peptide test. Further hepatobiliary evaluation consisted of ERCP, US, and liverbiopsy.
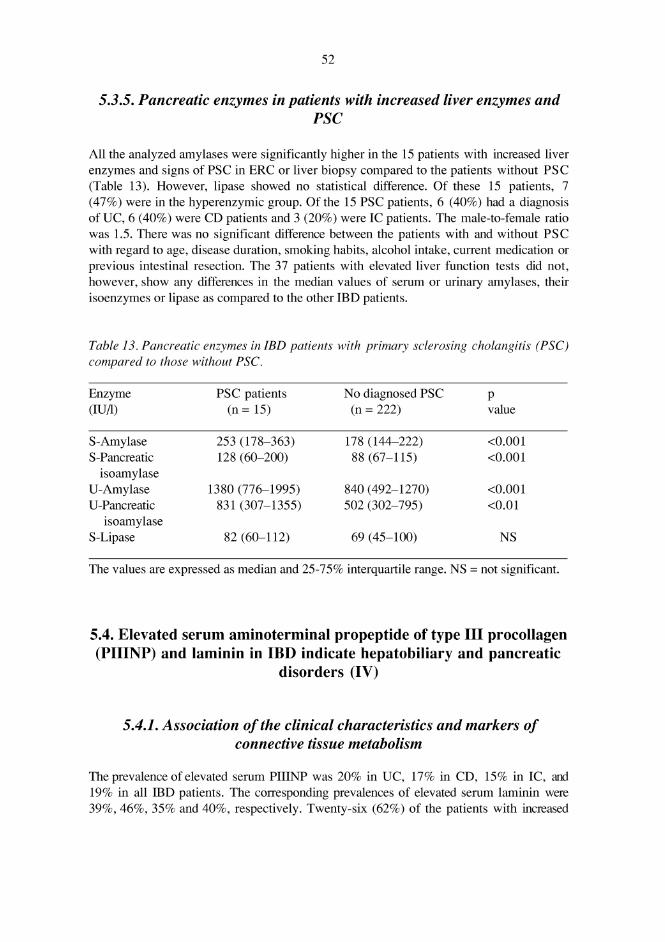
In IBD, the prevalence rates of pancreatic duct abnormalities and exocrine dysfunction were 8%and 4%, respectively. Parallel impairment of exocrine and endocrine functions was shown. Acute id-iopathic pancreatitis may complicate IBD. About 7-17% presented with elevated pancreatic enzymes.Enzyme elevation was associated with extensive and histologically active disease and, in some cases,with primary sclerosing cholangitis (PSC). Abnormal liver test results were commoner in patientswith CD than in patients with UC (30% versus 11%). The prevalence of PSC in IBD was 11%, whichis higher than previously reported (3.7-7.5%). PSC was commoner in patients with CD than in pa-tients with UC (17.4% versus 7.6%). About half of the PSC patients had concomitant pancreatic ductchanges, and the prevalence of concurrent cholangiographic and pancreatographic duct changes inIBD was 4.6%. Both serum PIIINP and laminin were increased in IBD patients. This was not onlyseen in patients with hepatobiliary disease and PSC, but also in patients with pancreatic disease.
In conclusion, pancreatic and hepatobiliary complications in IBD occur with high and similar fre-quencies in all IBD categories and are associated with each other. They are not clearly associated withthe clinical course of IBD.
Keywords: collagen markers, pancreatic enzymes, primary sclerosing cholangitis.