Embed Size (px)
Citation preview
Acute Abdomen and Appendix
Xu Xiao
M.D. Ph.D.
Department of Hepatobiliary and Pancreatic Surgery
The First Affiliated Hospital, College of Medicine, Zhejiang University
1
Part Acute AbdomenⅠ
2

Definition of acute abdomen
Acute abdominal pain
the patient feel pain anywhere between chest and groin. This is often referred to the stomach region or belly
sudden, severe abdominal pain that is less than 24 hours in duration
medical emergency in many cases, requiring urgent and specific diagnosis. Several causes need surgical treatment
3
Classification
Physiology of abdominal pain
Diagnosis
Differential diagnosis
Treatment
4

Classification
Internal acute abdomen Refers to the existing medical disease which can induce abdominal
pain with no surgical or gynecological indications, abdominal pain can be
alleviated after existing medical disease control with the comprehensive
examination and dynamic observation
Such as acute myocardial infarction, acute mesenteric lymphadenitis,
abdominal purpura, abdominal epilepsy, acute non-specific appendicitis
Surgical acute abdomen
Refers to the existing abdominal pain caused by some diseases which
need surgical treatment
5
Classification of surgical acute abdomen
Peritonitis is the most specific term
Five types
Perforation: perforated ulcer, intestinal perforation
Parenchymatous organic rupture:
hepatorrhexis, splenic rupture
Inflammatory: acute peritonitis, appendicitis
Obstruction: intestinal obstruction
Strangulation: mesenteric thrombosis
6
The Physiology of Abdominal Pain
Visceral PainThe most common form of pain
Manifestation of damaged or injured internal organs
Many forms of visceral pain are particularly prevalent in women and are associated with their reproductive life
period pains, labour pain or postmenopausal pelvic pain
For both men and women, pain of internal origin is the number one reason to consult a doctor
pain
7

Parietal Pain
Corresponds to the segmental nerve roots innervating the peritoneum
Tends to be sharper and better localized
Caused by pneumonia; empyema; pneumothorax; tuberculosis; neoplasm; or the accumulation of fluid resulting from heart, liver, or kidney disease
Aggravated by respiration and thoracic movements
The Physiology of Abdominal Pain
8
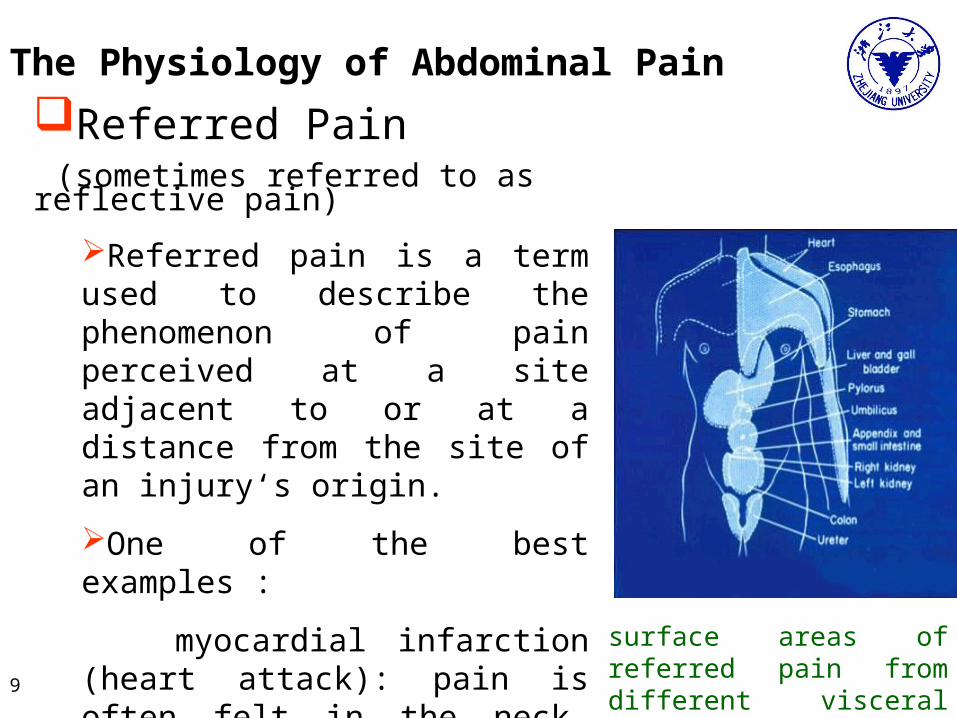
Referred Pain (sometimes referred to as reflective pain)
Referred pain is a term used to describe the phenomenon of pain perceived at a site adjacent to or at a distance from the site of an injury‘s origin.
One of the best examples :
myocardial infarction (heart attack): pain is often felt in the neck, shoulders, and back rather than in the chest, the site of the injury
surface areas of referred pain from different visceral organs
The Physiology of Abdominal Pain
9

Common Causes of Acute Abdomen
Appendicitis
Peritonitis
Bowel Perforation
Pancreatitis
Diverticular disease
Cholecystitis
Perforating gastric/duodenal ulcer
Ruptured ectopic pregnancy
Ruptured or hemorrhagic ovarian cyst
Pelvic inflammatory disease
Abdominal aortic aneurysm
Tubo-ovarian abscess
10

Diagnosis
History
Physical examination
Laboratory Findings
Imaging studies
Diagnostic laparoscopy
Atypical patients11

History
Type of onset
Sudden - rupture of viscus, mesenteric thrombosis
Gradual - cholecystitis, appendicitis
Quality
Dull - initial epigastric pain of appendicitis
Sharp - renal or biliary colic or obstruction of gut
Aching - pelvic inflammatory disease
Pleuritic - intensified by breathing
Lancinating - acute pancreatitis
Tearing - dissecting aneurysm
12

Frequency & duration
History
Intensity
Severe - rupture of viscus or blood in the peritoneal cavity
Moderate - RLQ appendiceal mild peptic ulcer, without perforation
Features
Pulsatile - abdominal aneurysm
Continuous - acute pancreatitis
Transient pain of short duration which does not recur is usually insignificant. The longer the duration the more likely a surgical condition13

History
Factors which intensify or relieve pain
Relation to meals - peptic ulcer pain relieved by food,
cholecystitis pain aggravated by fatty meal
Posture jack-knifing - leg drawn up to decrease peritoneal
irritation in suppurative appendicitis
Motion - any movement causes intense pain in generalized
peritonitis and the patient lies motionless
14

History
Associated nausea and vomiting
Nausea & vomiting - reflex, or irritative non-specific
vomiting occurs in many conditions
Such as acute appendicitis, anorexia always occurs
and vomiting, if it occurs, usually follows abdominal pain
rather than preceding it, as in gastroenteritis
Repeated vomiting of large amounts occurs in gut
obstruction, is often bile stained and may become fecal
15
History
Diarrhea
Most occur with acute gastroenteritis or food poisoning
May also occur with appendicitis or other focal inflammatory lesions of the gut
Constipation or obstipation
With complete small bowel obstruction - unrelenting constipation (obstipation)
Progressive constipation with carcinoma of the large bowel
Gas stoppage with decreased or absent bowel sounds - paralytic ileus
16

Physical Examination
Overall appearance ( Facial expression, diaphoresis, pallor,
and degree of agitation)
Inspection: scars, hernias, masses
Palpation : The most critical step
Tenderness
Rigidity and guarding
Board-like abdomen
Rebounding pain
17
Physical Examination
Auscultation
Hyperactive BS(bowel sound) , hypoactive BS or silent BS
Percussion
Digital examination of rectum A routine part of the physical examination
Check for problems with organs or other structures in the pelvis and lower belly
18

Laboratory Findings
WBC-DC (differential counting )
The total leukocyte count and percentage of polymorph nuclear cells are usually elevated in acute inflammatory conditions
Whereas early in the course of intestinal obstruction there may be no significant alterations
Urinalysis
Blood in the urine suggest disease of the urinary tract and can also result from an inflamed appendix lying in proximity to the ureter or bladder
In dehydration the specific gravity of the urine may be increased, and the red cell and hemoglobin values
19
Amylase, lipase
Serum amylase values in excess of 500 units are significant and levels
of 1500-2000 units or more are not unusual in the early stages of severe
acute pancreatitis.
β-HCG (human chorionic gonadotrophin)
– woman of childbearing age
Bilirubin, ALT, AST, Alkaline phosphatase
Laboratory Findings
20

Imaging Studies
Standing CXR and KUB
Ultrasound for solid organs
CT of abdomen for abscess, free air, vessel, tumor and
ischemia bowel
Angiography: Especially in non-diagnostic ischemia bowel
21

Imaging Studies
Gastric ulcer
22
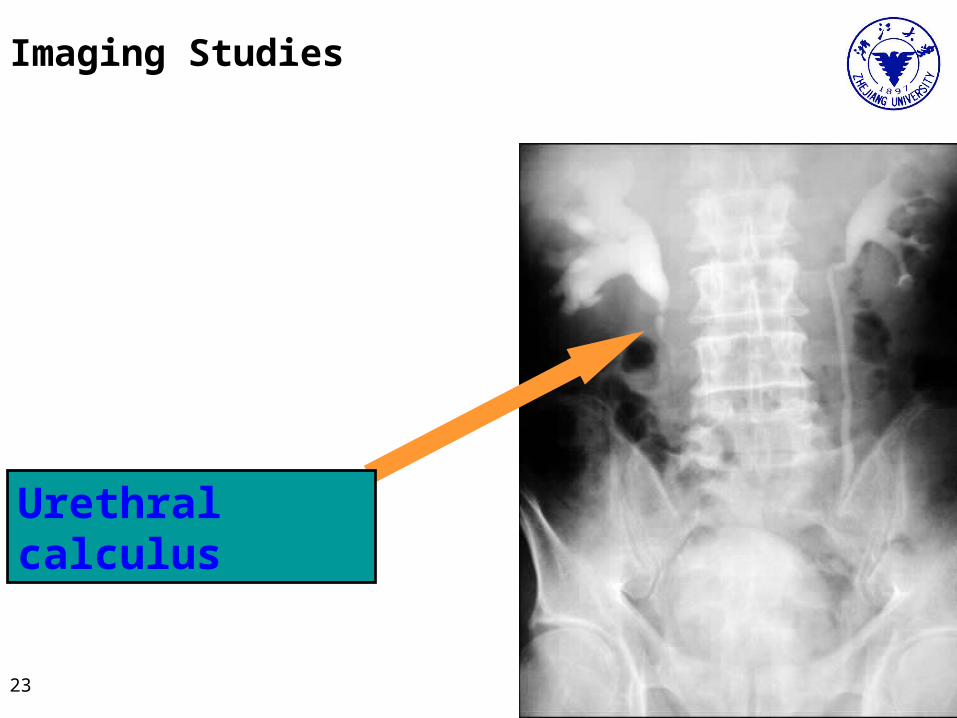
Imaging Studies
Urethral calculus
23
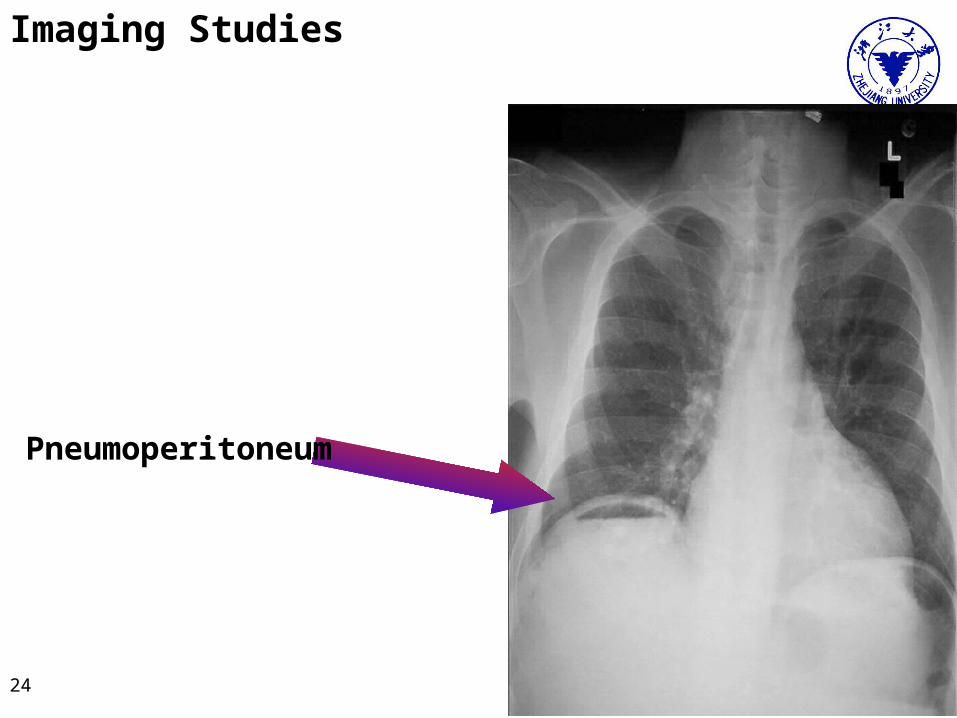
Imaging Studies
Pneumoperitoneum
24
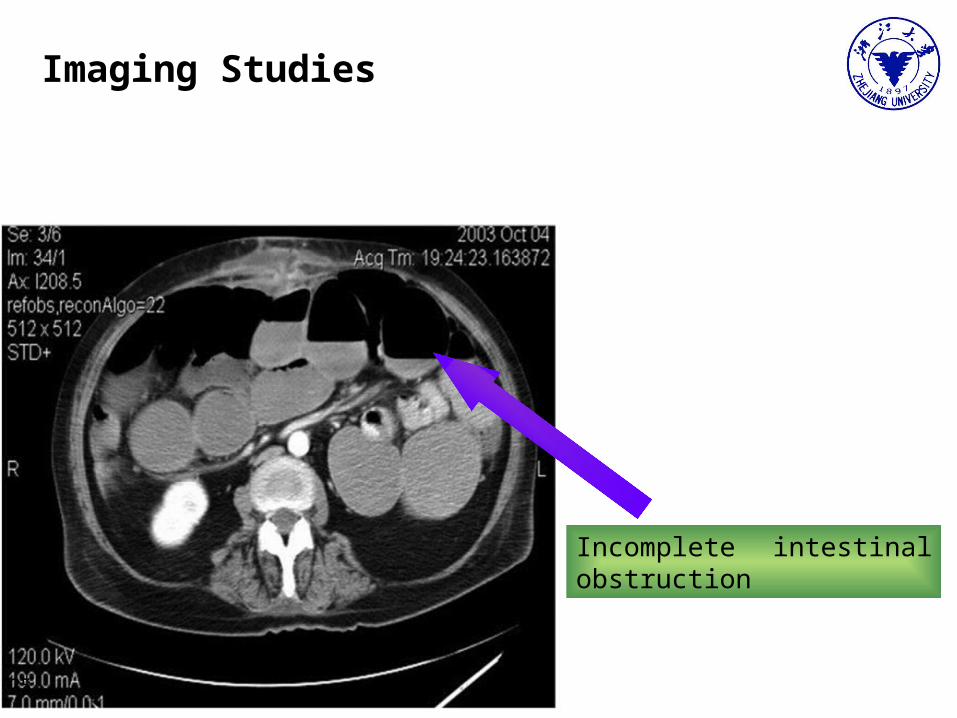
Imaging Studies
Incomplete intestinal obstruction
25
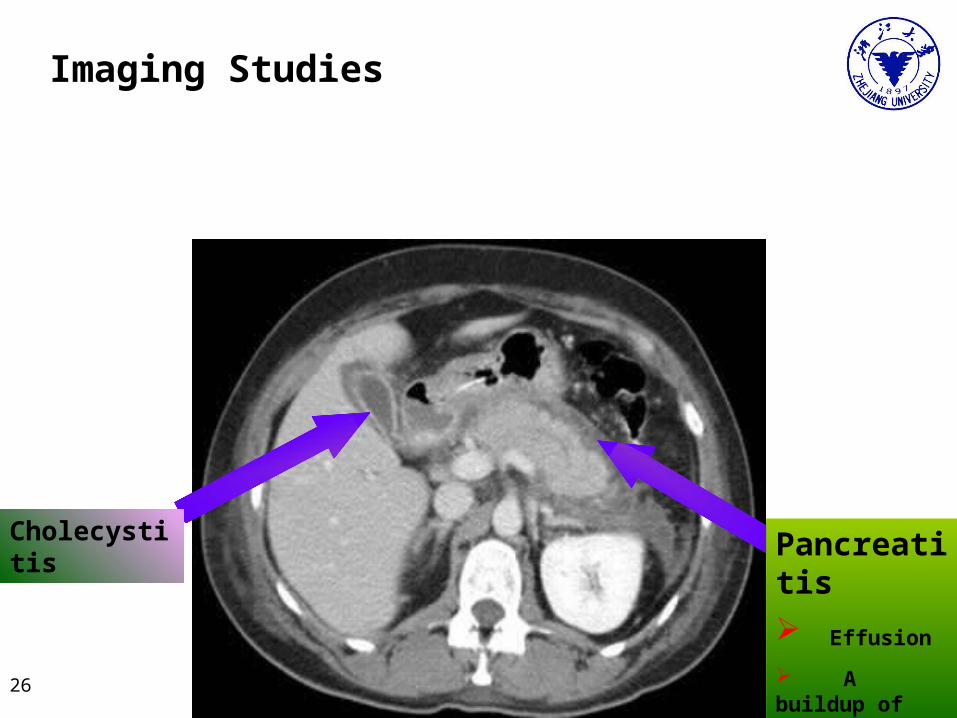
Imaging Studies
Cholecystitis Pancreatitis
Effusion
A buildup of fluid
26

Imaging Studies
Gall stone
27

Imaging Studies
Hemorrhage of large hepatocellular carcinoma
TACE (Transcatheter Arterial Chemoembolization )
28
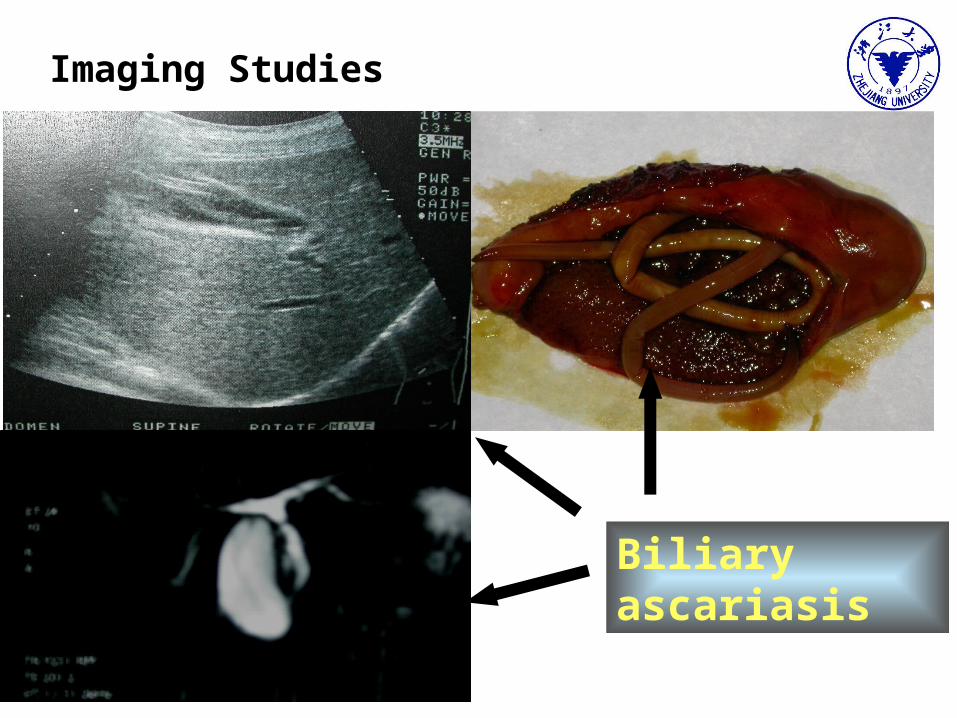
Imaging Studies
Biliary ascariasis
29

Diagnostic Laparoscopy
A high sensitivity and specificity
Decreased morbidity and mortality
Decreased length of stay
Decreased overall hospital costs
30
Atypical Patients
Pregnancy
Acute Abdomen in the Critically Ill
Immunocompromised Patients With Acute Abdomen
Acute Abdomen in the Morbidly Obese
31
(1) Pregnancy
The underlying pregnancy has symptoms similar with acute abdomen, including abdominal pains, nausea, vomiting, and anorexia
Pregnancy can alter the presentation of some disease processes and make the physical examination more challenging because of the enlarged uterus in the pelvis
Pregnancy can alter the laboratory findings, such as white blood cell counts
Pregnancy can influence the doctor’s decision to perform typical imaging studies because of concern about radiation exposure to the developing fetus
The reasons for delayed diagnosis
32
(1) Pregnancy
Most common surgical diseases seen in pregnancy
Appendicitis
Appendicitis is the most common nonobstetric disease requiring surgery, occurring in 1 of 1500 pregnancies
Biliary tract disorders
Surgery for biliary disease occurs in 1 to 6 per 10,000 pregnancies. Symptoms of pain, nausea, and anorexia are the same as in nonpregnant patients
Bowel obstructions
Bowel obstructions are much less common, occurring in about 1 or 2 per 4000 deliveries
33

(2)Acute Abdomen in the Critically Ill
The reasons for delayed diagnosis
Many of the underlying diseases and treatments
encountered in the intensive care unit can predispose to
acute abdominal disease
Critically ill patients are often unable to appreciate
symptoms to the same degree as healthy peers because
of nutritional or immune compromise, narcotic
analgesia, or antibiotic use
34
(3) Immunocompromised Patients With Acute Abdomen
The reasons for delayed diagnosis
Most common Immunocompromised Patients
Immunocompromised patients have variable presentations with acute abdominal diseases. The variability is highly correlated to the degree of immunosuppression
Elderly, malnourished, and diabetic patients
Transplant recipients on routine maintenance therapy
Cancer patients; renal failure patients
HIV patients
35
(4) Acute Abdomen in the Morbidly Obese
The reasons for delayed diagnosis
Alterations in the signs and symptoms of
peritonitis in the morbidly obese
Exam findings can also be difficult to confirm
distention or intra-abdominal mass because of
the size and thickness of the abdominal wall.
Abdominal imaging is also adversely affected
by obesity
36
Effective management of acute abdominal pain involves a careful history taking, ultrasound, electrocardiography and blood tests. Computed tomography of abdominal organs and visceral vessels is probably important already at the beginning of the diagnostic work up
Treatment for Acute Abdomen
37

Treatment Algorithms (1)
CT, computed tomography; NG, nasogastric tube; NL, normal study; OR, operation
Algorithm for the treatment of acute-onset severe, generalized abdominal pain
38

Treatment of gradual-onset severe, generalized abdominal pain.
Treatment Algorithms (2)
CT, computed tomography;
ERCP, endoscopic retrograde cholangiopancreatography; LFTs, liver function tests
39
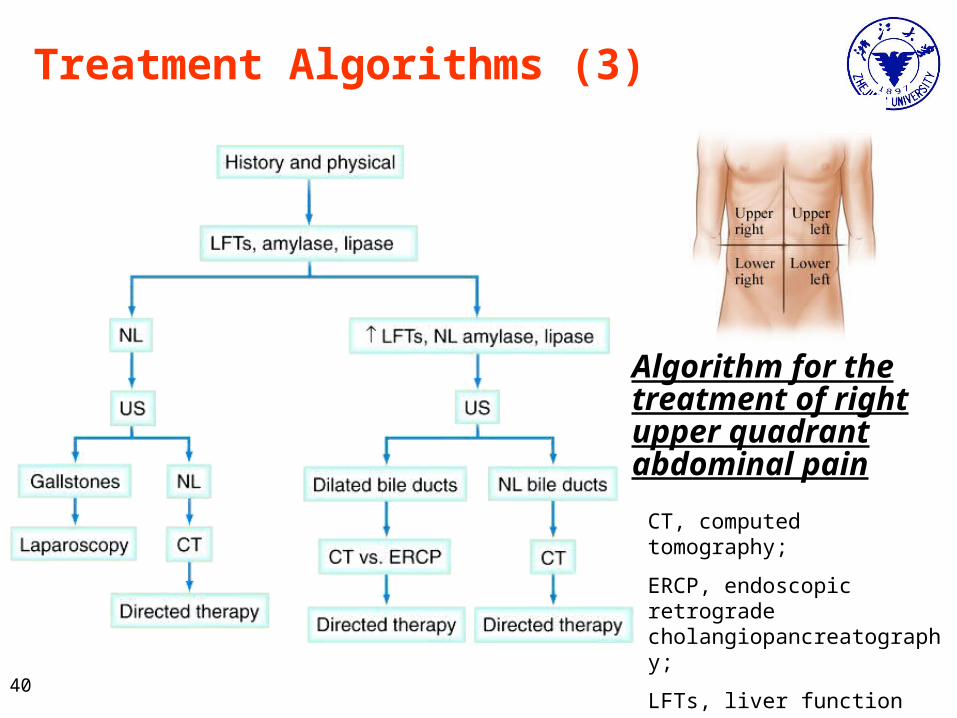
Algorithm for the treatment of right upper quadrant abdominal pain
Treatment Algorithms (3)
CT, computed tomography;
ERCP, endoscopic retrograde cholangiopancreatography;
LFTs, liver function tests;
NL, normal study;
US, ultrasound. 40
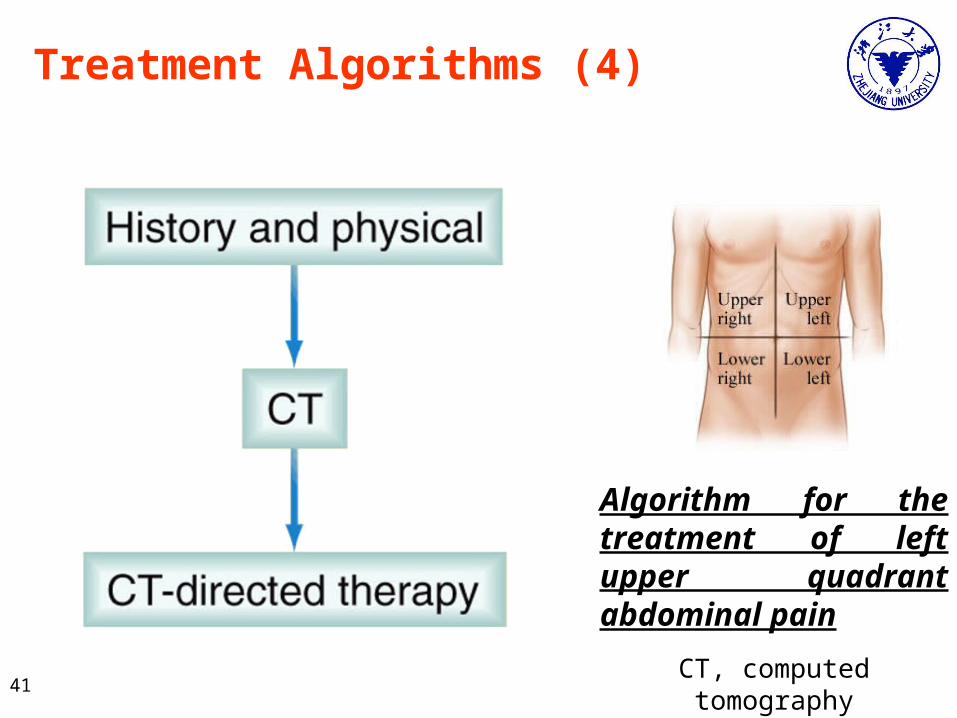
Algorithm for the treatment of left upper quadrant abdominal pain
Treatment Algorithms (4)
CT, computed tomography41
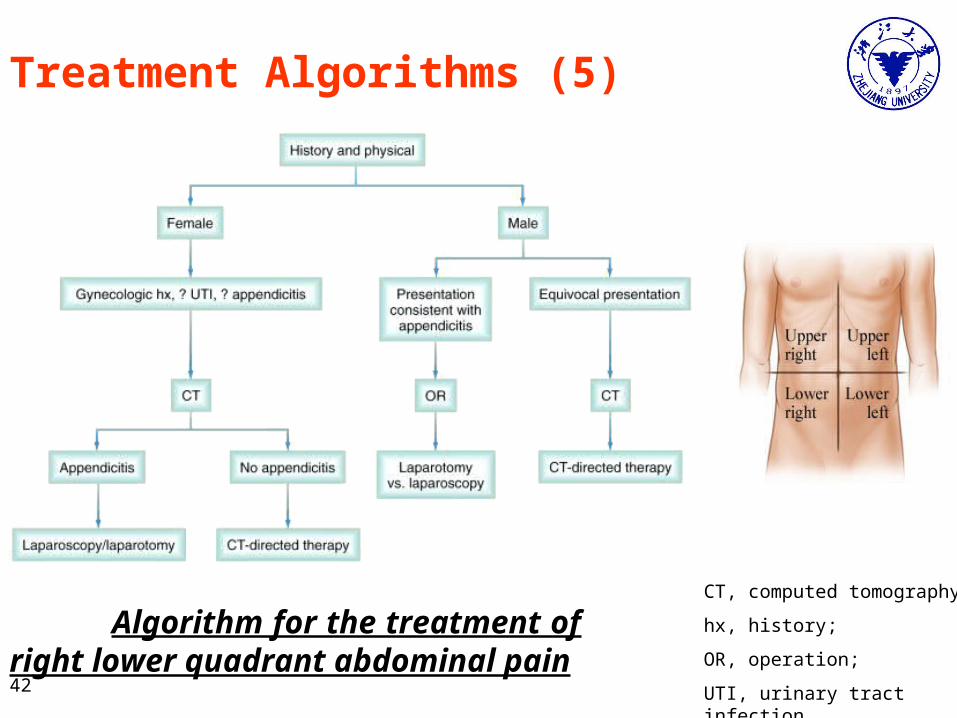
Algorithm for the treatment of right lower quadrant abdominal pain
Treatment Algorithms (5)
CT, computed tomography;
hx, history;
OR, operation;
UTI, urinary tract infection42
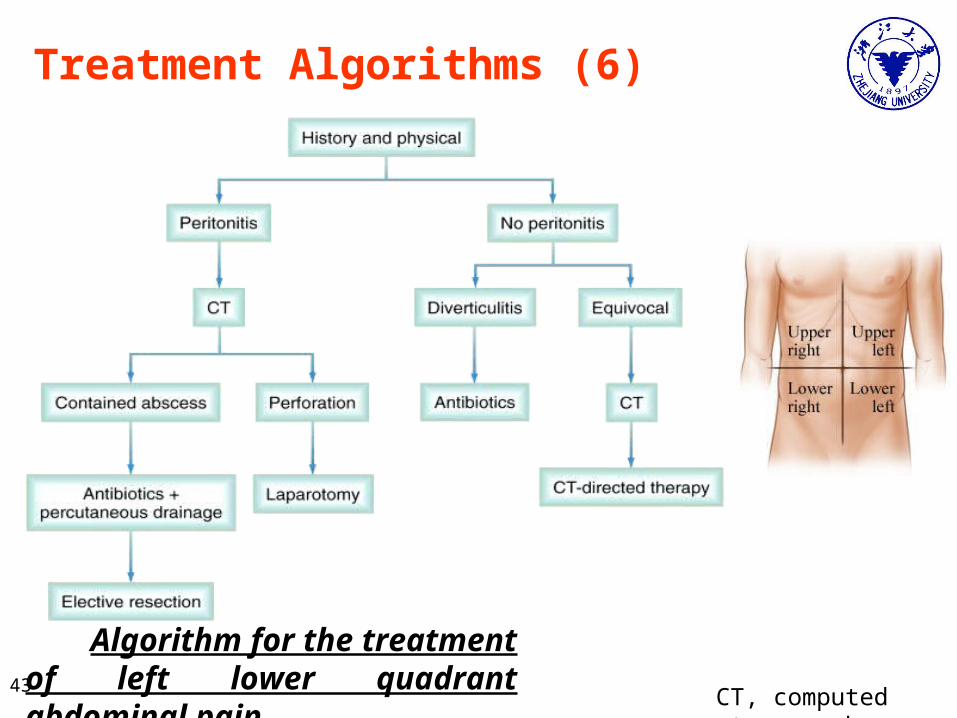
Algorithm for the treatment of left lower quadrant abdominal pain
Treatment Algorithms (6)
CT, computed tomography43

Preparation for emergency operation
IV access
Antibiotic infusions
Nasogastric tube
Foley catheter bladder drainage
Hydroelectrolytic equilibration
Crossmatched blood available
44
Summary
Acute abdomen remains a challenging part of a surgeon's practice
KEY: A patient with an acute abdomen is an EMERGENCY, and it is IMPERATIVE to get a correct diagnosis
Although advances in imaging techniques, a careful history and physical examination remain the most important part of the evaluation
Perform a laparoscopy or laparotomy for diagnosis with a good deal of uncertainty as to the expected findings
45

Case Study
20-Year-Old Male with Abdominal Pain for 18 Hours
Pain started in the Mid-Abdomen
Constant
Anorexia, Nausea, and Vomiting
First Episode
No Diarrhea, Dysuria
Pain Now Seems Worse in the Right Lower Abdomen
History
46

Case Study
Lying flat, avoids moving
Afebrile
Abdomen tender mostly in the RLQ
Significant guarding
Positive Roving's Sign
Physical Exam
47

Case Study
WBC 14*109/L
AST,ALT Normal
Amylase, Lipase Normal
Urine Culture Negative
CT scan
Lab Data
Further Testing
•Diagnosis?
48

49

Part Ⅱ Appendix
•Appendicitis
•Appendiceal Abscess
50

Appendicitis
Reginald Fitz first described acute and chronic appendicitis in 1886
It has been recognized as one of the most common causes of severe acute abdominal pain worldwide
Appendicitis is a condition characterized by inflammation of the appendix Vermiform appendix
All cases require removal of the inflamed appendix, either by Laparotomy or laparoscopy.
Untreated, mortality is high, mainly because of peritonitis and shock
51
Appendicitis
Anatomy and position
Pathophysiology
Diagnosis
Differential Diagnoses
Treatment
Outcome52

Anatomy and position
Anatomy A closed-ended, narrow tube up to several inches in length that attaches to the cecum like a worm
The inner lining of the appendix produces a small amount of mucus that flows through the open center of the appendix and into the cecum
The wall of the appendix contains lymphatic tissue that is part of the immune system for making antibodies
Position The vermiform appendix has no constant position
The appendix is more often found in the pelvic rather than the retrocaecal position
pelvic
Pre-ileal
post-ileal
retrocaecal
Para-caecal
53

Pathophysiology
Acute appendicitis is thought to begin with
obstruction of the lumen
Obstruction can result from food matter, adhesions,
or lymphoid hyperplasia
Mucosal secretions continue to increase
intraluminal pressure
54
Pathophysiology
Acute simple appendicitis
Acute purulent appendicitis
Acute gangrenous appendicitis
55
Diagnosis
History
Physical Examination
Laboratory Studies
Radiography
Diagnostic Laparoscopy
56

History
Primary symptom: abdominal pain
Pain beginning in epigastrium or periumbilical area that is vague and hard to localize
Associated symptoms: indigestion, discomfort, flatus, need to defecate, anorexia, nausea, vomiting
Migration of pain from initial periumbilical to RLQ was 64% sensitive and 82% specific
Anorexia is the most common of associated symptoms
Vomiting is more variable, occuring in about ½ of patients
57

Physical Examination
Findings depend on duration of illness prior to exam
Early on patients may not have localized tenderness
With progression there is tenderness to deep palpation over McBurney’s point
McBurney’s Point: just below the middle of a line connecting the umbilicus and the ASIS ( anterior superior iliac spine)
Rectal exam: pain can be most
pronounced if the patient has
pelvic appendix
58
Physical Examination
Roving's sign
Pain in RLQ with palpation to LLQ
A sign of appendicitis. If palpation of the lower left
quadrant of a person's abdomen results in more pain in
the right lower quadrant, the patient is said to have a
positive Rovsing's sign and may have appendicitis
59

Physical Examination
Psoas sign
Place patient in L lateral decubitus and extend R leg at
the hip. If there is pain with this movement, then the sign
is positive.
Occasionally, an inflamed appendix lies on the
Psoas muscle and the patient will lie with the right hip
flexed for pain relief.
60

Physical Examination
Obturator sign
Passively flex the R hip and knee and internally rotate the
hip. If there is increased pain then the sign is positive
If an inflamed appendix is in contact with the obturator
internus, spasm of the muscle can be
demonstrated by flexing and internally
rotating the hip. This maneuver
will cause pain in the hypogastrium
61

Laboratory Studies
WBC
The white blood cell count is elevated with more than 75% neutrophils in most patients
A completely normal leukocyte count and differential is found in about 10% of patients with acute appendicitis
A high white blood cell count (>20,000/mL) suggests complicated appendicitis with either gangrene or perforation
Urinalysis
Be helpful in excluding pyelonephritis or nephrolithiasis
Microscopic hematuria is common in appendicitis
Gross hematuria is uncommon and may indicate the presence of a kidney stone
62

Radiography
Plain abdominal radiographs
Ultrasonography
Computed tomography (CT)
CT : best choice based on availability and alternative
diagnoses
CT : greater sensitivity, accuracy, predictive value
63
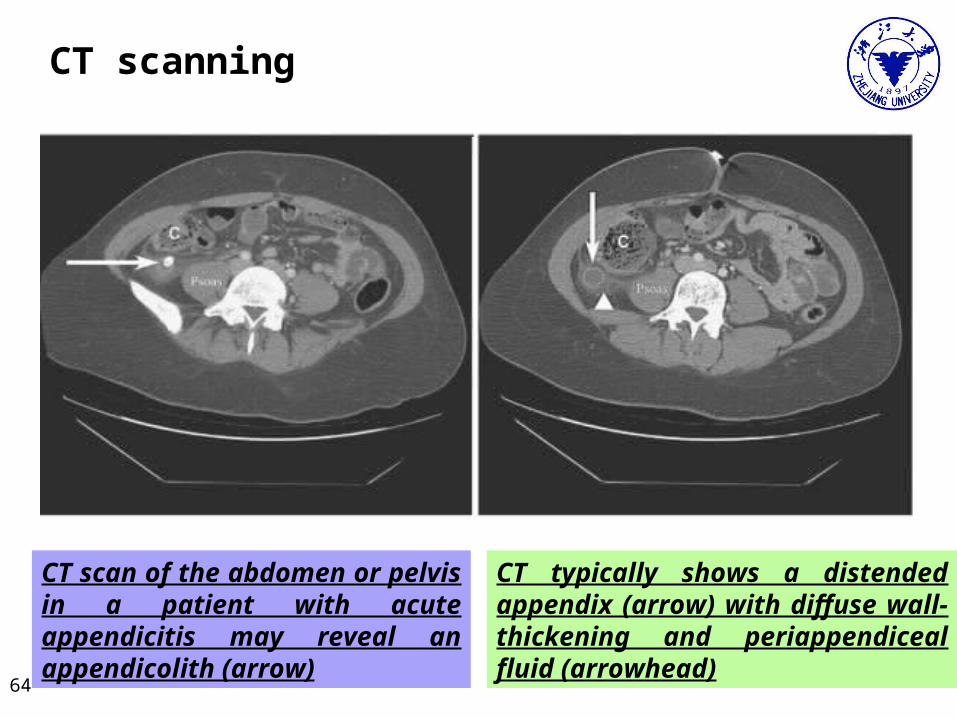
CT scan of the abdomen or pelvis in a patient with acute appendicitis may reveal an appendicolith (arrow)
CT typically shows a distended appendix (arrow) with diffuse wall-thickening and periappendiceal fluid (arrowhead)
CT scanning
64
Diagnostic Laparoscopy
A direct examination of the appendix
A survey of the abdominal cavity for other possible causes of pain.
Primarily for women of childbearing age in whom preoperative pelvic ultrasound or CT scan
65

Diagnostic Algorithm
Algorithm for the evaluation and management of patients with possible acute appendicitis based on surgical assessment of clinical probability of the diagnosis66

Diagnostic Algorithm
Algorithm summarizing the treatment of acute appendicitis 67

Differential Diagnoses
Two type : A: required surgery B: not required surgery
Required surgery
Perforation of gastrointestinal tract ulcer, tumor, diverticulitis
Obstetrics and gynecologic disease: ectopic pregnancy, ovarian torsion
Meckel’s diverticulitis
Tumor
Not required surgery
Pelvic inflammation
Mesenteric adenitis: at exploration a normal appendix and enlarged lymph nodes in the mesentery
Viral &bacterial gastroenteritis
Pneumonia, pleurisy68

Treatment
Surgical removal of appendix is definitive treatment
Incision Incision over the point of maximal tenderness,generally at McBurny point McBurney’s incision, tansvers skin incision , 3—6cm long
Process The taenia of the colon are followed to the base of the appendix
Mesoappendix is divided between clamps and ligated
The base of appendix is divided and ligated 0.5cm from caceum and inverted using a purse-string
Suspected case
Admit the patient to hospital for further observation 12-24hrs
69

Open Appendectomy (OA)
Location of possible incisions for an open appendectomy
Division of the mesoappendix
cecum
Anterior cecal artery
70

B. Ligation of the base and division of the appendix
C. Placement of purse-string suture or Z stitch
D. Inversion of the appendiceal stump
Open Appendectomy (OA)
71
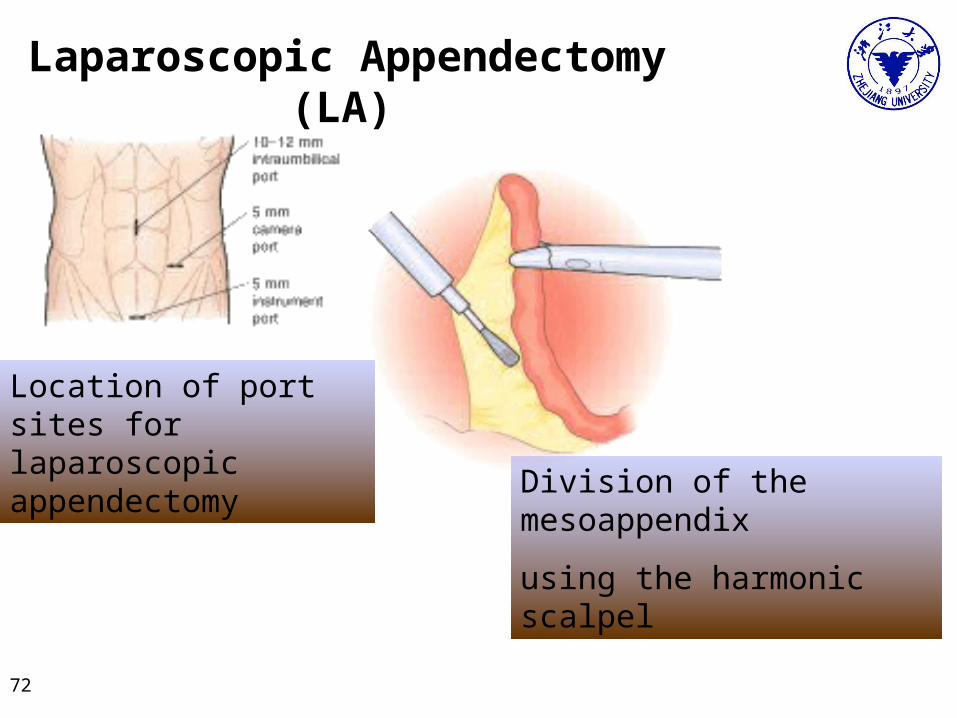
Location of port sites for laparoscopic appendectomy
Division of the mesoappendix
using the harmonic scalpel
Laparoscopic Appendectomy (LA)
72
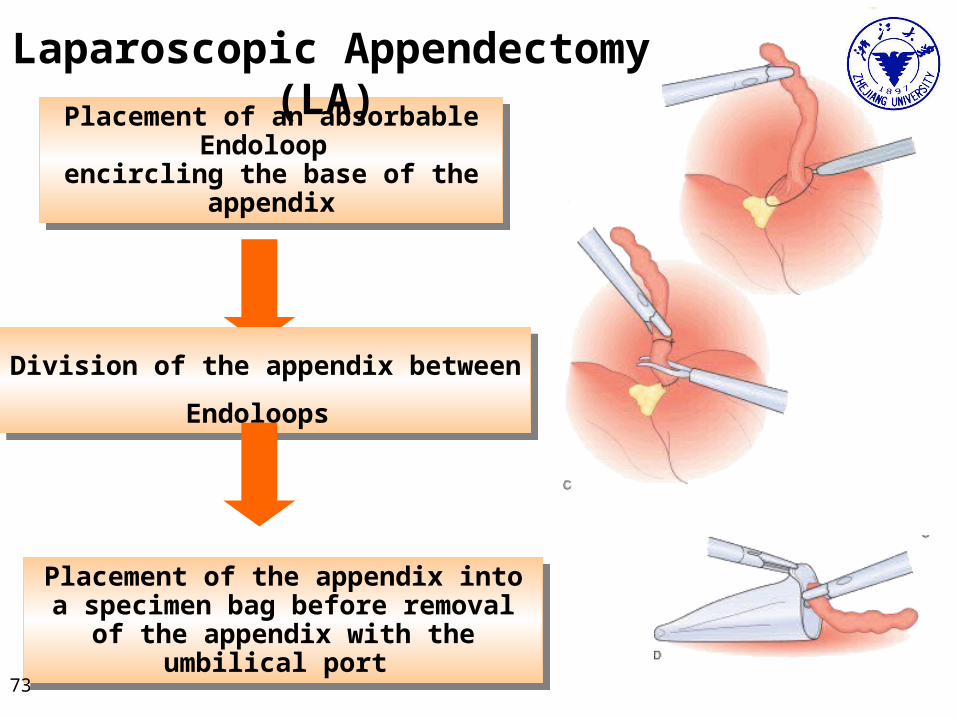
Placement of an absorbable Endoloop encircling the base of the appendix
Placement of an absorbable Endoloop encircling the base of the appendix
Division of the appendix between Endoloops Division of the appendix between Endoloops
Placement of the appendix into a specimen bag before removal of the appendix with
the umbilical port
Placement of the appendix into a specimen bag before removal of the appendix with
the umbilical port
Laparoscopic Appendectomy (LA)
73
Antibiotic thearpy
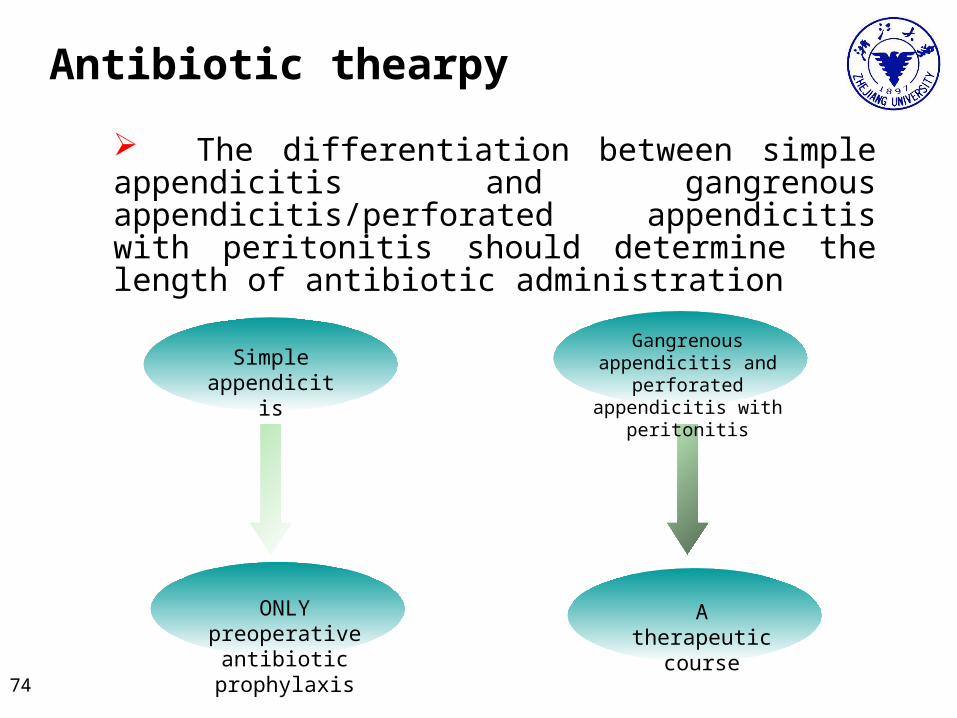
The differentiation between simple appendicitis and gangrenous appendicitis/perforated appendicitis with peritonitis should determine the length of antibiotic administration
Simple appendicitis
ONLY preoperative antibiotic prophylaxis
Gangrenous appendicitis and perforated appendicitis
with peritonitis
A therapeutic course
74
Appendiceal Abscess An abscess in the peritoneal cavity resulting from the spread of
infection in acute appendicitis, especially with perforation of the appendix.
Also called periappendiceal abscess.
Imaging studies are useful both in confirming the diagnosis and in
evaluating the size of any abscess present
Those patients with smaller abscesses or phlegmon and who are not
sick may be successfully managed initially with antibiotics alone.
Patients who continue to have fever and leukocytosis after several days
of nonoperative treatment are likely to require appendectomy during the
same hospitalization, whereas those who improve promptly may be
considered for interval appendectomy
75
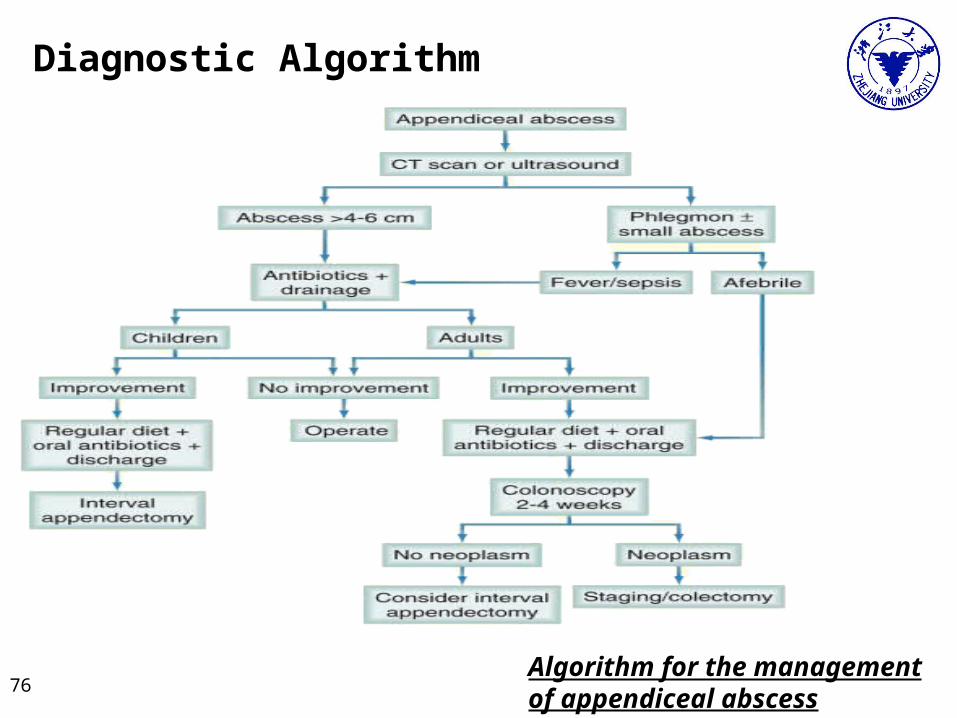
Diagnostic Algorithm
Algorithm for the management of appendiceal abscess
76
Outcomes
The mortality rate after appendectomy is less than 1%.
Surgical site infections are the most common complications seen after appendectomy.
Small bowel obstruction occurs in less than 1% of patients after appendectomy for uncomplicated appendicitis and in 3% of patients with perforated appendicitis who are followed for 30 years.
The risk for infertility following appendectomy in childhood appears to be small.
There are rare reports of appendicocutaneous or appendicovesical fistulas after appendectomy, typically for perforated appendicitis.
77

Thanks !Thanks !78