Embed Size (px)
Citation preview

AIDS RESEARCH AND HUMAN RETROVIRUSESVolume 20, Number 10, 2004, pp. 1037–1045© Mary Ann Liebert, Inc.
Once-Weekly Epoetin Alfa Improves Quality of Life andIncreases Hemoglobin in Anemic HIV� Patients
MICHAEL S. SAAG,1 PETER BOWERS,2 GERHARD J. LEITZ,3 and ALEXANDRA M. LEVINE,4 FORTHE COMMUNITY HIV ANEMIA MANAGEMENT PROTOCOL SITES (CHAMPS) STUDY GROUP
ABSTRACT
This prospective, open-label, multicenter trial evaluated the effects of once-weekly (qw) epoetin alfa on qual-ity of life (QOL) and hemoglobin (Hb) levels in anemic human immunodeficiency virus (HIV)-infected adultsreceiving antiretroviral therapy. A total of 650 patients with Hb � 11 g/dl received epoetin alfa 40,000 U qwsubcutaneously, with dose escalation to 60,000 qw if Hb increases was �1 g/dl after 4 weeks. The Linear Ana-log Scale Assessment (LASA) overall QOL score, LASA energy score, and LASA activity score each signifi-cantly improved from baseline to final measurement (p � 0.0001 for each parameter). Improvements in theMedical Outcomes Study (MOS)-HIV physical and mental health summary scores were also significant (p �0.0001), and coincided with Hb increases. Mean Hb increased from baseline to final measurement by 2.5 g/dl(95% CI: 2.3, 2.6 g/dl; p � 0.0001). Objective hematological response rate, defined as a �1 g/dl Hb increasefrom baseline to week 8, was 86%. Hemoglobin increased significantly in all subgroups of race, zidovudineuse, CD4� cell count, and viral load. Once-weekly epoetin alfa was well tolerated. Once-weekly epoetin alfais effective in improving QOL and Hb measures.
1037
INTRODUCTION
ANEMIA IS THE MOST FREQUENT HEMATOLOGICAL ABNORMAL-ITY affecting human immunodeficiency virus (HIV)-in-
fected patients, even in the era of highly active antiretroviraltherapy (HAART),1–6 and represents an important contributorto symptoms that can compromise daily activity and adverselyaffect quality of life (QOL). Given the impact of anemia in theHIV-infected population, maintaining a more normal hemo-globin (Hb) level has clinical value. The common symptoms ofanemia take on greater importance as HIV-infected patients arenow living longer.7
The rate of Hb decline, presence of underlying disease, andspecific symptoms and signs of the patient should all be con-sidered in the decision to treat mild-to-moderate anemia. Oncespecific correctable causes of anemia have been identified andtreated, recombinant human erythropoietin (epoetin alfa) can be
used and has been shown to be efficacious in correcting HIV-related anemia.8,9 Correction of HIV-related anemia has beenassociated with significant improvements in energy, health per-ception, home management (e.g., shopping, housework, yardmaintenance), and role function (e.g., how health interferes withdaily activities).9–11 The use of epoetin alfa for the treatmentof anemia in HIV-infected patients has also been associatedwith an improvement in overall patient survival in one study.12
An earlier study in HIV-infected patients that evaluated epo-etin alfa administered three times weekly (tiw) versus onceweekly (qw) demonstrated that both regimens had similar effi-cacy in increasing Hb levels, decreasing transfusion require-ments, and improving QOL, with similar safety profiles.8 Thepresent study evaluated the efficacy of qw administration ofepoetin alfa in improving QOL, alleviating anemia, and reduc-ing transfusion requirements in anemic HIV-infected patientsreceiving antiretroviral therapy.
1AIDS Outpatient Clinic, University of Alabama at Birmingham, Birmingham, Alabama 35294.2Johnson & Johnson Pharmaceutical Services, Raritan, New Jersey 08869.3Ortho Biotech Clinical Affairs, LLC, Bridgewater, New Jersey 08807.4Division of Hematology, Keck School of Medicine, University of Southern California, and USC/Norris Cancer Center, Los Angeles, Cali-
fornia 90033.
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1037

MATERIALS AND METHODS
Inclusion criteria
HIV-infected men and women were included in the study ifthey satisfied the following criteria: (1) 18–75 years of age; (2)Hb � 11 g/dl, currently maintained on stable antiretroviral ther-apy at least 4 weeks prior to enrollment; (3) baseline endoge-nous serum erythropoietin level �500 mU/ml; (4) provision ofwritten informed consent; and (5) willing and able to completethe QOL assessment tools.
Exclusion criteria
Patients were excluded for the following reasons: (1) if theypresented with acute, symptomatic opportunistic infection orother acute AIDS-defining illness; (2) history of any primaryhematological disease; (3) presence or history of uncontrolledhypertension (diastolic blood pressure � 100 mm Hg); (4) ane-mia attributable to factors other than HIV infection, such as ironor folate deficiency, hemolysis, or acute or chronic blood loss;(5) therapy with ganciclovir, cidofovir, ribavirin, and/or inter-feron; (6) ferritin �40 ng/ml; (7) current, active substanceabuse; (8) previous exposure to epoetin alfa within 6 monthsprior to study enrollment; and (9) pregnant or breast-feedingwomen, or women of childbearing potential not using adequatebirth control methods.
Study design and assessments
This 16-week, open-label trial was conducted in 209 centersthroughout the United States. Study protocol and informed con-sent forms were approved by local Institutional Review Boards.Epoetin alfa (PROCRIT®; Ortho Biotech Products, L.P.,Bridgewater, NJ) was initiated at 40,000 U qw as a subcuta-neous injection. Following 4 weeks of therapy, if the Hb risewas �1.0 g/dl from the baseline Hb level, the epoetin alfa dosewas increased to 60,000 U qw. If Hb did not increase by �1.0g/dl over baseline after 4 more weeks of therapy at the 60,000U qw dose, treatment with epoetin alfa was discontinued. If theHb level exceeded 13 g/dl, epoetin alfa was discontinued untilthe Hb level decreased to 12 g/dl. When treatment was resumed,the epoetin alfa dose was reduced by 25% and titrated to main-tain desired Hb. Hematological response was defined as a �1g/dl increase in Hb by week 4 at 40,000 U qw or by week 8 at60,000 U qw. Dosing continued for a total of 16 weeks. Pa-tients were offered oral iron supplements per investigator dis-cretion to prevent iron deficiency and support erythropoiesis.
Complete blood counts were obtained and blood pressureswere measured at baseline, at weeks 2, 4, 8, 12, and 16, andweekly for the 4 weeks following any dose adjustment. Trans-fusion utilization was documented prior to and throughout thestudy. HIV-RNA level and CD4� cell count and percentagewere recorded at baseline and week 16 or upon early with-drawal. All adverse events were recorded and classified as mild,moderate, or severe as well as by whether they were study drugrelated.
QOL was assessed at baseline, week 8, week 16, or uponearly withdrawal. Two separate QOL self-reporting instrumentswere used: (1) the 100-mm Linear Analog Scale Assessment(LASA) and (2) the Medical Outcomes Study HIV (MOS-HIV)
Health Survey. LASA is a validated measure of QOL that hasbeen used extensively to evaluate self-perceived improvementsin overall QOL, energy level, and ability to perform daily ac-tivities in HIV-infected subjects.13–16 Higher scores indicatebetter health, with 100 mm being the best.15 The MOS-HIVHealth Survey contains 35 questions measuring 10 dimensionsof health in addition to an item evaluating health transition inHIV-infected subjects. The 10 dimensions are scored as sum-mated rating scales ranging from 0 to 100, with higher scoresindicating better health, and can be grouped into one of twosubscales—physical health summary and mental health sum-mary. For patients with physical or mental health summaryscores above or below 50, it can be inferred that they have bet-ter or worse QOL, respectively, than the HIV-infected patientpopulation used to develop these scales.17 The MOS-HIV hasbeen shown to be reliable, valid, and sensitive to the symptomfrequency and body system affected.18–20
Outcome variables and statistical analyses
The primary end point was patient self-reported QOL usingLASA and MOS-HIV. Secondary end points included changesin Hb as well as number of transfusion and number of unitstransfused. The study was powered to detect statistically sig-nificant changes in QOL, Hb, and transfusions from baselineto final assessment. Descriptive statistics were used to summa-rize baseline characteristics of the study population. One-wayrepeated measure analysis of variance (ANOVA) with Bonfer-roni adjustment for multiple comparisons was used to comparemean change in Hb over time. The following characteristicswere compared using a two-sided, paired t test: CD4� cellcount, viral load, zidovudine treatment, race, and gender, aswell as the mean changes in Hb from baseline to final mea-surement. One-way ANOVA was used to compare mean changein Hb among the subgroups of CD4� cell count, viral load, gen-der, and race. QOL improvements were compared using two-sided, paired t tests. Changes in the frequencies of patients re-quiring transfusion were evaluated using the McNemar’s test.Regression analyses were used to evaluate the relationships be-tween final Hb levels and both overall MOS-HIV and LASAscores. Three study populations were analyzed. The safety pop-ulation (Group 1) included any subject who received at leastone dose of epoetin alfa. The efficacy population (Group 2) in-cluded any patient who received epoetin alfa, had one post-treatment measurement, and satisfied the inclusion/exclusioncriteria (the last value carried forward was used to impute anymissing values). Group 3 was a subgroup of Group 2 that in-cluded patients who received epoetin alfa and had multiple mea-surements taken precisely according to protocol.
RESULTS
Accrual, eligibility, baseline characteristics
A total of 789 anemic, HIV-infected patients were enrolledby 209 community centers between August 20, 1998 and Oc-tober 9, 2000. Four enrolled patients never received epoetin alfaand therefore were excluded from all analyses. There were 785patients evaluable for safety (i.e., patients who received at leastone dose of epoetin alfa), and 650 patients evaluable for effi-
SAAG ET AL.1038
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1038

cacy (i.e., patients who met all inclusion/exclusion criteria andhad at least one posttreatment measurement). The 135 patientswho were not evaluable for efficacy were unevaluable for thefollowing reasons: baseline Hb � 11.0 g/dl (n � 57); baselineserum ferritin �40 ng/ml or missing (n � 41); no postbaselineassessments (i.e., Hb, QOL, epoetin alfa dose) (n � 17); fail-ing more than one criteria previously listed (e.g., baseline Hb �11.0 g/dl, serum ferritin �40 ng/ml or missing, or no post-baseline assessments) (n � 19); and prior exposure to epoetinalfa (n � 1). As shown in Table 1, of the 650 patients evalu-able for efficacy, 66% were men and nearly half (49%) wereAfrican-American. Mean baseline measurements were as fol-lows: Hb of 9.7 � 1.1 g/dl, CD4� cell count of 188 cells/�l(range, 0 to 1505 cells/�l), and HIV viral load of 83,290copies/ml (range, 0–750,000 copies/ml). Patients were receiv-ing FDA-approved and investigational antiretroviral agents, aswell as other medications (Table 2). Sixty-eight percent of pa-tients were receiving HAART. Two hundred and twenty pa-tients (all included in Group 2) withdrew before week 16 forthe following reasons: patient noncompliance (n � 101), other(n � 24), death (n � 17), intercurrent illness (n � 17, adverseevents (n � 12), patient decision (n � 11), physician decision(n � 11), lost to follow-up (n � 11), disease progression (n �9), and inadequate Hb response (n � 7).
QOL assessments
Results for the LASA and MOS-HIV at baseline, week 8,week 16, and final measurement are shown by point changesin Table 3. The improvements in QOL were also analyzed us-ing effect size.
LASA QOL assessment. For all three LASA parameters (en-ergy level, daily activity, and overall QOL), patients had meanbaseline scores of less than 50 mm (range, 38.0–46.4 mm), con-sistent with functional impairment.15,21 As early as week 8, sig-nificant increases were seen and these increases were main-tained for the study duration (Table 3). At week 16, energylevel, daily activity, and overall QOL showed significant meanimprovements from baseline with effect sizes of 1.14, 0.85, and0.78, respectively (p � 0.0001). In the Group 2 analysis, meanincreases in LASA scores from baseline to last value measured
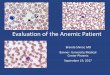
were 23.2 mm for energy (95% CI: 20.8, 25.6), 20.4 mm foractivity (95% CI: 18.0, 22.8), and 19.3 mm for overall QOL(95% CI: 16.8, 21.7) (p � 0.0001 for each parameter), with ef-fect sizes similar to those observed in the on-treatment analy-sis at week 16. Improvements in overall QOL were directly as-sociated with increases in Hb. Using regression analysis, themaximum incremental increase in LASA overall QOL occurredwhen Hb increased from 11 to 12 g/dL (range, 10–13 g/dL),with the maximum incremental effect at 11.64 d/dL (Fig. 1).
MOS QOL assessment. All 10 dimensions of the MOS-HIVplus the health transition item improved significantly from base-line to week 8 (p � 0.002), week 16 (p � 0.0001), and to lastvalue measured (p � 0.0001) for all components measured(Table 3). As seen with LASA, improvements in all dimensionsof the MOS-HIV were seen at week 8 and continued to slightlyincrease until the end of study. The MOS-HIV dimensions withthe greatest mean improvements from baseline to last valuemeasured were energy/fatigue (16.8-point increase), physicalfunctioning (13.6-point increase), and social functioning (12.7-point increase) (Table 3). Improvements in the MOS-HIV phys-ical and mental summary scores from baseline to last value mea-sured were 5.7 points (95% CI: 4.8, 6.6) and 6.0 points (95%CI: 5.1, 6.9), respectively (p � 0.0001 for each item).
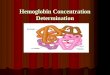
Improvements in MOS-HIV scores were also associated withincreases in Hb. For patients whose Hb increased 0–2 g/dl, 2–4g/dl, or �4 g/dl from baseline to final measurement, the great-est improvements on the MOS-HIV were seen in energy/fa-tigue, physical functioning, and social function dimensions(Fig. 2). For each 2 g/dl increase in Hb, there were significantimprovements in these MOS-HIV dimensions (p � 0.0001).
Hematological assessments
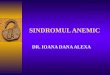
Mean Hb increased from 9.7 g/dl at baseline to 12.2 g/dl atfinal measurement, a significant increase of 2.5 g/dl (p �0.0001) for Group 2 (n � 650) (Table 3). Hemoglobin increasedrapidly. In the analysis of Group 3 (n � 430, with all follow-up data collected), Hb increased as early as week 2 by 1.3 g/dl,and by week 4, a 2.1 g/dl increase was observed (Fig. 3). He-moglobin continued to increase through week 8 (2.7 g/dl in-crease) and week 16 (2.8 g/dl increase) (p � 0.0001 for all time
QW EPOETIN ALFA IN ANEMIC HIV� PATIENTS 1039
TABLE 1. DEMOGRAPHIC AND BASELINE CHARACTERISTICS (n � 650)
Gender, nMen 431 (66%)Women 219 (34%)
Age (years)a 43.4 � 9.0 (20.9–71.3)00.Race/ethnicity, n
African-American 319 (49%)White 213 (33%)Hispanic 95 (15%)Asian 17 (2%)Other 6 (1%)
Hemoglobin (g/dl)a 9.7 � 1.1 (3.4–11.0)00.CD4� cell count (cells/�l) (n � 646)a 187.6 � 213.4 (0–1505)000.Viral load (copies/ml) (n � 616)a 83,290 � 157,419 (0–750,000)
aMean � standard deviation (range).
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1039

points versus baseline). When results were compared betweenGroup 2 and 3 for these time points, they were similar. Basedon the Group 2 efficacy analysis, the hematological responserate (defined as a �1 g/dl increase in Hb from baseline to week8) was 86%. Of this 86%, 8.3% (n � 46) of responders weredose escalated to epoetin alfa 60,000 U qw.
In the Group 2 analysis, 7.2% of patients had no increase inHb from baseline to final measurement (week 16 or early with-drawal); 14.2% had a 0 to �1 g/dl Hb increase; 18.8% had a �1to �2 g/dl Hb increase; 23.9% had a �2 to �3 g/dl Hb increase;16.2% had a �3 to �4 g/dl Hb increase; and 17.1% had a �4g/dl Hb increase. A significant Hb response to epoetin alfa wasshown for all subgroups of race, gender, zidovudine use, CD4�
cell count, and viral load; therefore, Hb increase was indepen-dent of these factors (Tables 4 and 5). Mean change in Hb wasnot significantly different between patients receiving HAARTversus those receiving a non-HAART regimen at any time point.
Transfusion requirements
There was a significant decrease in transfusion requirementsfrom baseline to week 16. Compared with the transfusion rateduring weeks 1–4 (5.7% of patients), significantly fewer pa-tients required transfusions during weeks 5–8 (1.7%), 9–12(1.2%), or 13–16 (1.4%) (p � 0.0001 for each time point ver-sus weeks 1–4). Transfusion requirements were inversely re-lated to increases in HB. Mean increase in Hb from baseline tolast value measured did not differ significantly between patientsreceiving transfusions plus epoetin alfa (mean increase, 2.9 g/dl)and patients who received epoetin alfa only (mean increase, 2.5g/dl; p � 0.321).
Safety and tolerability
There were 785 patients evaluable for safety. A total of 840adverse events were reported. Adverse events reported in �2%of patients were diarrhea (3.9%), fever (3.8%), nausea (3.7%),abdominal pain (3.1%), fatigue and vomiting (2.9%), pneumonia(2.5%), and dehydration, dyspnea, or monoliasis (2.2% each).
Serious adverse events were reported in 132 patients; the vastmajority of these adverse events were unrelated to epoetin alfaand were attributed to HIV treatment or underlying HIV dis-ease. Four patients experienced serious adverse events deemedrelated to study drug by the investigators. One of these patientsdied due to severe asthenia, anemia, thrombocytopenia, and de-hydration. The remaining three patients discontinued studydrug: the second due to the development of Kaposi sarcomaand cellulitis, and the third due to moderate asthma. The fourthpatient was hospitalized due to severe hemolytic anemia. Thepatient was treated with packed red blood cells and cortico-steroids, and the anemia resolved completely with sequelae afew weeks later.
A total of nine patients reported mild-to-moderate hyperten-sion. Two reports of mild hypertension and two reports of mod-erate hypertension were deemed related to study drug. Of therelated events, one of the patients with moderate hypertensioninterrupted treatment and the remaining three patients contin-ued with no treatment interruption.
These adverse events are similar to those reported in previ-ous studies evaluating qw and tiw dosing of epoetin alfa in theHIV-positive population.8–10 Epoetin alfa was well tolerated.
DISCUSSION
The results of this study demonstrate that qw subcutaneousdosing of epoetin alfa results in significant improvements inQOL. Improvements in QOL were measured using two scales:LASA and the MOS-HIV. At baseline, mean LASA scores foreach parameter (energy level, daily activity, and overall QOL)were less than 50 mm, consistent with the significant functionalimpairment observed in previous studies of anemic cancer pa-tients receiving chemotherapy.15,21 Significant improvements inLASA were seen at week 8 and were associated with increasesin Hb levels. The changes in LASA scores were associated withlarge effect size, which indicates that real clinical benefit is as-sociated with improved QOL scores. Wu et al. have shown that
SAAG ET AL.1040
TABLE 2. ANTIVIRAL MEDICATIONSa (n � 650)
Medication n Medication n
HAART 445 (69%) NNRTIsART (not HAART) 205 (32%) Efavirenz 173 (27%)NRTIs Nevirapine 114 (18%)
Stavudine 291 (45%) Delavirdine 9 (1%)Lamivudine 253 (39%) Protease inhibitorsZidovudine and lamivudine 244 (38%) Nelfinavir 164 (25%)Abacavir 160 (25%) Indinavir 127 (20%)Didanosine 120 (19%) Ritonavir 118 (18%)Zidovudine 66 (10%) Saquinavir 96 (15%)Adefovir 10 (2%) Amprenavir 53 (8%)
Other drugsAnabolic steroids 85 (13)Hydroxyurea 74 (11)
aHAART, highly active antiretroviral therapy; NRTI, nucleoside reverse transcriptase inhibitors; ART, antiretroviral therapy;NNRTI, nonnucleoside reverse transcriptase inhibitors.
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1040

an effect size (as expressed in terms of standard deviation units)of 0.2 indicates a small clinical effect, 0.5 a moderate effect, and0.8 a large effect; a change of 1.0 is likely to be highly mean-ingful in a clinical sense.20 In our study, we demonstrated effectsizes of 1.14, 0.85, and 0.78 for baseline to week 16 changes inenergy level, daily activity, and overall QOL, respectively, withsimilar results observed in both the Group 2 and 3 analyses. Thisdegree of improvement in LASA scores was larger than that ob-served in previous studies of epoetin alfa in anemic HIV-infectedpatients10 and in studies of anemic cancer patients undergoingchemotherapy.22 These differences may be related to the fact thatmany of the current patients were on stable HAART therapy, thatHb levels were higher at study entry, and/or because use of ef-fective antiretroviral therapy also contributed to lower baselinelevels of functional impairment and QOL.
QOL was also evaluated using the MOS-HIV in order to con-firm the findings from the LASA analysis and because theMOS-HIV was designed specifically for use in the HIV-infectedpopulation. The physical and mental health summary scoresshowed a statistically significant increase from baseline (p �0.0001). All 10 dimensions plus the health transition item ofthe MOS-HIV improved significantly from baseline. Energy/fa-tigue, physical functioning, and social functioning demon-strated the largest mean improvements. Based on two earlierstudies of HIV-infected patients receiving zidovudine, Wu etal. presented an approach for assessing the clinical implicationsof MOS-HIV scores.20,23,24 In their analysis, improvement of
�7 points on the energy/fatigue dimension score was consis-tent with a clinical change from a symptomatic to an asympto-matic HIV-infected patient in terms of energy and fatigue. Adifference of 5.5 points on the physical functioning dimension
QW EPOETIN ALFA IN ANEMIC HIV� PATIENTS 1041
TABLE 3. MEAN BASELINE AND INCREASE IN QUALITY-OF-LIFE PARAMETERSa
Baseline 8-week change 16-week change Final change (LVCF)b,c
Measure n mean � SD n mean � SD (ES) n mean � SD (ES) n mean � SD (ES)
Hemoglobin (g/dl) 650 9.7 � 1.1 522 2.7 � 1.9 (2.48) 384 2.8 � 1.9 (2.51) 632 2.5 � 2.0 (2.27)LASA (mm)
Energy 637 38.0 � 22.3 503 20.7 � 26.1 (0.93) 455 25.3 � 28.4 (1.14) 550 23.2 � 28.6 (1.04)Activity 637 42.4 � 25.7 501 17.3 � 27.2 (0.67) 454 21.9 � 28.1 (0.85) 548 20.4 � 28.8 (0.79)Oveall QOL 638 46.4 � 26.1 502 16.6 � 27.7 (0.63) 456 20.4 � 29.3 (0.78) 549 19.3 � 29.4 (0.74)
MOS-HIVOverall health 636 28.7 � 22.1 497 9.1 � 19.1 (0.41) 457 12.0 � 21.6 (0.54) 545 10.8 � 21.2 (0.49)Physical function 642 48.4 � 28.0 508 11.5 � 27.0 (0.41) 464 15.0 � 26.8 (0.54) 550` 13.6 � 27.1 (0.49)Role function 642 33.9 � 42.8 507 5.3 � 38.4 (0.12) 459 11.5 � 41.0 (0.27) 550 9.9 � 41.7 (0.23)Social function 640 55.0 � 31.4 505 11.0 � 30.4 (0.35) 460 13.7 � 33.2 (0.43) 550 12.7 � 33.1 (0.40)Cognitive function 640 66.2 � 27.3 504 5.4 � 22.7 (0.20) 463 7.7 � 25.5 (0.28) 548 7.0 � 24.6 (0.26)Pain 638 57.8 � 27.3 503 6.6 � 25.1 (0.24) 462 8.5 � 26.9 (0.31) 546 8.0 � 27.0 (0.29)Mental health 642 58.7 � 22.4 509 6.5 � 19.1 (0.29) 465 8.2 � 20.3 (0.37) 551 7.8 � 20.3 (0.35)Energy/fatigue 643 37.7 � 23.2 508 14.5 � 21.9 (0.63) 465 18.2 � 24.2 (0.78) 552 16.8 � 23.8 (0.72)Health distress 642 53.7 � 29.4 507 10.7 � 26.3 (0.36) 465 13.0 � 28.1 (0.44) 551 11.9 � 27.7 (0.41)Quality of life 637 52.4 � 23.9 503 9.1 � 24.4 (0.38) 457 11.7 � 26.3 (0.49) 546 10.7 � 26.2 (0.45)Health transition 636 58.3 � 26.2 501 12.6 � 31.5 (0.48) 455 12.7 � 32.6 (0.49) 544 12.2 � 32.2 (0.47)Mental summaryd 619 40.0 � 12.0 473 5.1 � 9.9 (0.43) 433 6.4 � 11.1 (0.54) 526 6.0 � 10.9 (0.50)Physical summaryd 619 36.5 � 11.5 473 4.7 � 8.9 (0.41) 433 6.3 � 10.2 (0.54) 526 5.7 � 10.1 (0.49)
aLVCF, last value carried forward; SD, standard deviation; ES, effect size; LASA, Linear Analog Scale Assessment; QOL,quality of life; MOS-HIV, Medical Outcomes Study-Human Immunodeficiency Virus.
bFinal value (LVCF) is the last observed value following the baseline value.cp � 0.0001 for all final values (LVCF) versus baseline.dSummary scores constructed using the factor score coefficients taken from the following article: Revicki DA, Sorensen S, and
Wu AW: Reliability and validity of physical and mental health summary scores from the Medical Outcomes Study-HIV HealthSurvey. Med Care 1998;36:126–137. The means and standard errors from clinical trial 1 were used to rescale the data.
FIG. 1. Linear Analog Scale Assessment (LASA) overallquality-of-life score by final hemoglobin (Hb).
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1041

represents the difference between being limited and not beinglimited in vigorous activity. In our study, mean changes frombaseline to final measurement for energy/fatigue and physicalfunctioning were 16.8 points and 13.6 points, respectively.These robust improvements in QOL scores very likely translateinto dramatic improvements in the functional capacity of pa-tients in our study.
Epoetin alfa qw also produced a rapid and sustained im-provement in Hb levels in anemic HIV-infected patients whoare receiving antiretroviral therapy. Transfusion requirementsalso decreased significantly from baseline (p � 0.0001) andwere inversely related to increases in Hb. Once-weekly epoetinalfa was effective in improving Hb levels regardless of race,antiretroviral therapy with or without zidovudine, CD4� cellcount, and/or viral load, suggesting that the improvements inHb were not likely to be elated to improvements in HIV dis-ease status. For the Group 2 analysis, the hematological re-sponse rate was 86%; 8.3% (n � 46) of these patients requireddose escalation of epoetin alfa to 60,000 U qw.
An incremental analysis technique was used to determine theoptimal Hb levels at which patients have the largest improve-
SAAG ET AL.1042
FIG. 2. Mean change in Human Immunodeficiency Virus-Medical Outcomes Study (MOS-HIV) dimensions from base-line to final measurement by hemoglobin increase (n � 650).*p � 0.0001 for difference from baseline to final measurement(last value carried forward).
FIG. 3. Increase in hemoglobin by week (n � 650). *p �0.0001 for difference from baseline; †p � 0.0001 for the dif-ference from the previous time period. Note: The last value car-ried forward method was used to impute missing hemoglobinvalues.
TABLE 4. MEAN BASELINE AND CHANGE IN HEMOGLOBIN FROM BASELINE TO
FINAL VALUE BY ZIDOVUDINE USE, RACE, AND GENDERa (n � 650)
Mean � SDb hemoglobin (g/dl)
Baseline (n) Change (n) pc
Zidovudine useZidovudine 9.7 � 1.2 (304) 2.6 � 2.0 (298) �0.0001No zidovudine 9.7 � 1.0 (346) 2.4 � 1.9 (334)) �0.0001
Race/ethnicityAfrican/American 9.6 � 1.2 (319) 2.4 � 1.9 (311) �0.0001White 9.7 � 1.1 (213) 2.6 � 2.2 (207) �0.0001Hispanic 9.9 � 0.8 (95) 2.4 � 1.6 (91) �0.0001Asian 10.1 � 0.8 (17) 2.2 � 2.5 (17) 0.0020
GenderMen 9.7 � 1.1 (431) 2.7 � 2.1 (418) �0.0001Women 9.7 � 1.1 (219) 2.2 � 1.5 (214) �0.0001
aNote: For zidovudine use and race, mean change in hemoglobin from baseline to final value was not significantly differentbetween subgroups.
bSD, standard deviation.cp value for hemoglobin change from baseline to final value.
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1042

ment in QOL. In our study, the greatest improvement in QOLscores for each 1 g/dl increase was found to occur when the Hblevel increased from 11 to 12 g/dl. Increases in Hb level cor-responded to improvement in MOS-HIV scores until an Hblevel of 13 g/dl was reached, at which time, by protocol design,epoetin alfa dosing was withheld. Based on the observed rela-tionship between increases in Hb and improvements in QOL,our data suggest that QOL may continue to improve as Hb in-creases beyond this point, as the slope of the line indicates acontinuing trend (Fig. 2).
The demonstration that functional improvements in QOL areassociated with Hb changes is important because anemia remainsa complication in up to 58% of patients with HIV infection dur-ing the HAART era.4,25–28 Although severe anemia is seen lessfrequently in patients receiving HAART, mild-to-moderate ane-mia remains a problem for many patients.27,28 For example,Semba et al. have shown that even after initiating HAART, ap-proximately 38% of patients were still anemic.1 In the presentstudy, the majority of patients were on stable HAART for at least4 weeks prior to baseline and presented with anemia that requiredintervention. Since most of these patients were receiving bothHAART and epoetin alfa, the study design did not allow us todiscern whether the Hb increases were due specifically toHAART or to epoetin alfa. However, a 1.3 g/dl increase in Hbwas seen as early as week 2 with qw dosing of epoetin alfa, andresolution of anemia by HAART would be expected to take sig-nificantly longer. Previous studies have demonstrated that pa-tients receiving HAART experience Hb increases ranging from1.1 to 2.7 g/dl after 12 months of treatment with HAART.29–31
Correction of anemia is important, as prior studies haveshown that anemia is associated with more rapid disease pro-gression and increased risk of mortality in HIV-infected pa-tients.25,32 The benefits of qw administration of epoetin alfa onhematopoietic response in the present study parallel those as-sociated with tiw therapy in HIV-infected patients. Both regi-mens demonstrate a positive relationship between increased Hbor hematocrit levels and QOL, independent of CD4� cellcount.8–10 As reported by Henry et al.,10 patients treated withepoetin alfa tiw showed significant increases in mean hemat-ocrit compared with placebo recipients, and QOL scores (asmeasured by LASA) improved most dramatically in hematocritresponders. In an additional open-label study of 221 anemic(Hb � 11 g/dl), HIV-infected patients, epoetin alfa 100–300U/kg administered subcutaneously tiw for 16 weeks resulted inmean Hb increases of 2.5 g/dl, which were independent ofCD4� count values.9 The level of increase in Hb and thechanges in QOL were similar to those measured in the presentstudy, while the qw dosing interval would be expected to beeasier in terms of patient compliance and drug costs.
In the present study, qw epoetin alfa was well tolerated. Ad-verse events reported in �2% of patients receiving epoetin alfatherapy included diarrhea, fever, nausea, abdominal pain, fa-tigue, vomiting, pneumonia, dehydration, dyspnea, and moni-liasis. The incidence and type of adverse events were similarto those reported in HIV-infected patients and in earlier stud-ies of tiw administration of epoetin alfa.9
The results of the present study confirm those found in pre-vious studies. However, as with many large, multicenter, com-
QW EPOETIN ALFA IN ANEMIC HIV� PATIENTS 1043
TABLE 5. MEAN BASELINE AND CHANGE IN HEMOGLOBIN FROM BASELINE TO
FINAL VALUE BY CD4� COUNT AND VIRAL LOAD RESPONSESa (n � 650)
Mean � SDb hemoglobin (g/dl)
Baseline (n) Changec (n) pc
CD4� cell count (cells/�l)��100 9.8 � 1.0 (44) 2.4 � 1.6 (44) �0.0001�100 to �50 9.9 � 1.2 (28) 2.6 � 1.6 (27) �0.0001�50 to 0 9.8 � 1.2 (125) 2.7 � 2.2 (124) �0.00010 to �50 9.7 � 1.1 (168) 2.7 � 1.9 (167) �0.0001�51 to �100 9.6 � 1.1 (63) 2.6 � 1.9 (63) �0.0001�100 9.7 � 1.0 (84) 2.9 � 1.8 (82) �0.0001
Log viral load (copies/�l)��2 9.6 � 0.9 (52) 2.6 � 1.9 (48) �0.0001�2.0 to �1.5 9.0 � 1.2 (14) 3.5 � 1.8 (14) �0.0001�1.5 to �1.0 9.4 � 1.3 (31) 3.9 � 2.3 (30) �0.0001�1.0 to �0.5 9.8 � 1.0 (71) 2.3 � 1.9 (71) �0.0001�0.5 to 0 9.7 � 1.1 (79) 2.2 � 2.0 (79) �0.00010 to �0.5 9.9 � 1.0 (169) 2.4 � 1.9 (169) �0.0001�0.5 to �1.0 9.6 � 1.0 (54) 2.4 � 1.8 (53) �0.0001�1.0 to �1.5 9.5 � 1.4 (27) 2.8 � 2.6 (27) �0.0001�1.5 to �2.0 9.9 � 0.7 (14) 2.9 � 1.0 (14) �0.0001��2.0 9.8 � 1.1 (22) 3.2 � 1.6 (22) �0.0001
aNote: For CD4� cell count change, mean change in hemoglobin from baseline to final value was not significantly differentbetween subgroups.
bSD, standard deviation.cp value for hemoglobin change from baseline to final value.
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1043

munity-based studies, a high dropout rate—due mainly to pa-tient noncompliance and infrequent monitoring—resulted inmany violations of inclusion/exclusion criteria. For example,46 patients were enrolled with baseline Hb between 11.0 and11.3 g/dl and were excluded from the current analysis; how-ever, we looked at this population and found no significant dif-ference in Hb or QOL outcomes.
This community-based study has demonstrated that adminis-tration of epoetin alfa therapy results in significant improvementsin QOL and functional capacity, significant increases in Hb levels(mean, 2.5 g/dl), and significant decreases in transfusion require-ments in patients living with HIV. A qw dosing schedule shouldalso offer added convenience for both patients and caregivers.
ACKNOWLEDGMENTS
The authors wish to acknowledge Kimberly Marino and K.Linda Tang from Ortho Biotech Clinical Affairs, LLC for theirtechnical and editorial assistance, and the following investiga-tors for their participation in the reported study: Lyssette Car-dona, M.D.; Christie Lamping, M.D.; Victoria L. Sharp, M.D.;Guillermo Santos, M.D.; Dennis Melton, M.D.; Joel Rosen-stock, M.D.; David Henry, M.D.; Michael G. Sension, M.D.;Allison J. Sigler, M.D.; Robert Sheneberger, M.D.; ChristopherMatthews, M.D.; Alexander McMeeking, M.D.; Bruce Olm-scheid, M.D.; Olivia Ortiz, M.D.; Daniel Pearce, D.O.; ScottUbillos, M.D.; Jack DeHovitz, M.D.; Robert C. Scott, M.D.;Daniel S. Berger, M.D.; Delia Bullock, M.D.; William Catena,M.D.; Paul Cimoch, M.D.; Timothy Cooley, M.D.; Peter En-gelhard, M.D.; Terrence Ibbs, M.D.; Mark Kaplan, M.D.;Miguel Mogyoros, M.D.; Patricia Salvato, M.D.; Malte Schultz,M.D.; Roberto Aymat, M.D.; Bonnie Bock, M.D.; Noe B. Ma-teo, M.D.; Kristin Razzeca, M.D.; Daliah K. Shamsuddin, M.D.;Theresa Soroko, M.D.; Mary Van den Berg-Wolf, M.D.; ManjuAgrawal, M.D.; Roger Anderson, M.D.; Leonard Bass, M.D.;Paul Benson, D.O.; Lawrence Brown, M.D.; Sibte Burney,M.D.; Alexis Corazon, M.D.; Joseph Exilhomme, M.D.; RonaldFlenner, M.D.; Michael Gottlieb, M.D.; Richard Hudson, M.D.;Nasir Husain, M.D.; Marah Lee, M.D.; Polly Lee, M.D.; An-thony J. Mangia, M.D.; Peter Marcus, M.D.; Craig E. Metroka,M.D., Ph.D.; Clark Mitchell, M.D.; Tim Poirier, M.D.; GaryRichmond, M.D.; Howard A. Stark, M.D.; Vilma Vega, M.D.;Daniel Warner, M.D.; Arthur Williams, M.D.; Barbara Akin-son, D.O.; Gary Block, M.D.; Patrick Dalton, M.D.; PatrickDaly, M.D.; Jerome DeVente, M.D.; Leslie Diaz, M.D.; CarolEncarnacion, M.D.; Jeff Enejosa, M.D.; Ronald J. Grossman,M.D.; Jose Hernandez, D.O.; Jason Leider, M.D., Ph.D.; BrianLipman, M.D.; Jesus Llanes, M.D.; Michael Pistole, M.D.;Karen Raben, M.D.; John Rawls, M.D.; Robert Roland, M.D.;Jihad Slim, M.D.; Steven Sotman, M.D.; Donna Sweet, M.D.;Anita Vaughn, M.D.; Jeffrey Vieira, M.D.; Daniel Barbaro,M.D.; Jim Braun, M.D.; Felix Carpio, M.D.; Phillipe Chiliade,M.D.; David Donnell, M.D.; Ricardo Dunner, M.D.; ThomasL. Horowitz, M.D.; Kenneth Horowitz, M.D.; Kimball John-son, M.D.; Allan Kelly, M.D.; Juan S. Latorre, M.D.; MichaelLevin, M.D.; David Lintz, M.D.; David McDonough, M.D.;Victor Mulanovich, M.D.; Carlos J. Page, M.D.; Jorge Rod-riguez, M.D.; Steven Santiago, M.D.; Robert Smith, M.D.;David Stein, M.D.; Gregory Strayer, M.D.; William Sutker,
M.D.; Mauro Torno, M.D.; Belinda Velazquez, M.D.; ElenaVillaviencio, M.D.; A.T.M. Yousuf, M.D.; Barbara Zeller,M.D.; Debra Adler-Klein, M.D.; Stephen Becker, M.D.; PhillipBonaparte, M.D.; Jeannine Bookhardt, M.D.; Philip Brachman,M.D.; Ron Cathcart, M.D.; Richard Cazen, M.D.; LawrenceCrane, M.D.; Dennis Deruelle, M.D.; Jordan Glaser, M.D.; Pe-ter Gomatos, M.D.; Stephen Green, M.D.; Kenneth Greenberg,D.O.; Kamal Hamed, M.D./MPH; Larry Hitzeman, M.D.; KarenHoover, M.D.; John Hostetler, M.D.; Steven Kooshian, M.D.;Jean Messihi, M.D.; Sajjad Mohammad, M.D.; Robert Mu-rayama-Greenbaum, M.D.; Mahmoud Mustafa, M.D.; SessineNajjar, M.D.; Steven Pounders, M.D.; Ronald A. Primas, M.D.;Bonnie Rabinowitch, M.D.; Uwe Schmidt, M.D.; Louis Sloan,M.D.; Harold Slotnik, M.D.; Eitan Sobel, M.D.; Alan Stein,M.D.; Lorraine Tosiello, M.D.; Thanes Vanig, M.D.; JaimeVasquez, D.O.; Keith D. Vrhel, M.D.; Terry Watson, D.O.; Tim-othy West, M.D.; David Wheeler, M.D.; Daniel A. Wolde-Ru-fael, M.D.; Shelly Wolland, M.D.; Bisher Akil, M.D.; SohanBassi, M.D.; Victor Beer, M.D.; Nicholas Bellos, M.D.; LeonardBerkowitz, M.D.; Kenneth Blair, M.D.; David Brand, M.D.;Mitchell V. Brodey, M.D.; Patrick H. Brown, M.D.; Larry M.Bush, M.D.; Patrick Cadigan, M.D.; Paul Cook, M.D.; Nila De-sai M.D.; John Doweiko, M.D.; Rinchen-Tzo Emgushov, M.D.;Marcia Epstein, M.D.; Victor Fainstein, M.D.; Alvan Fisher,M.D.; Joseph Gathe, M.D.; Adriana Grigroriu, M.D.; MargaretL. Hoffman-Terry, M.D.; Robert Holman, M.D.; William A.Johnson, M.D.; Pam Juba, M.D.; Jonathan Kaiser, M.D.; AllanA. Kaplan, M.D.; Peter Kraus, M.D.; Sharon Lee, M.D.; JeffreyR. Levenson, M.D.; Alvaro Lopez, M.D.; Rob MacGregor,M.D.; Christopher McNulty, D.O.; Chadia Morcos, M.D.;Steven Natterstad, M.D.; Joseph Nussbaum, M.D.; RomulaOrque, M.D.; Linsey Philip, M.D.; Karen Plunkett-Reid, M.D.;Richard Pokriefka, M.D.; Nina K. Regevik, M.D.; Judith A. Ri-ley, M.D.; David Rubin, M.D.; William Sanchez, M.D.; StefanSchwann, M.D.; Douglas Sepkowitz, M.D.; Peter Shalit, M.D.;Marina Sigidin, M.D.; Subasree Srinivasan, M.D.; KevinStephan, M.D.; Leoncio Tasca, M.D.; Camille Taylor-Mullings,M.D.; Derrick J. Tolbert-Walker, M.D.; Ramon (Gabe) Torres,M.D.; Anil Tulpule, M.D.; Chukwuemeka Ufomadu, M.D.; RajUttamchandani, M.D.; Olukemi Wallace, M.D.; Kenneth Wang,M.D.; Mark Watkins, M.D.; Susan Wehr, M.D.; Daniel C.William, M.D.; William Woodward, D.O.; Sam Yoon, M.D.;and Kevin S. Young, M.D.
Dr. Saag receives research support and honoraria from, andserves as a consultant for, Ortho Biotech Clinical Affairs, LLC,and Johnson & Johnson. Dr. Levine receives research supportand honoraria from, and serves as a consultant for, OrthoBiotech Clinical Affairs, LLC. Dr. Bowers and Dr. Leitz areemployed by Ortho Biotech Clinical Affairs, LLC. This studywas supported by Ortho Biotech Clinical Affairs, LLC.
Participating subjects provided written informed consent andwere willing and able to complete quality-of-life assessmenttools. Study protocol and informed consent forms were ap-proved by local Institutional Review Boards.
REFERENCES
1. Semba RD, Shah N, Strathdee SA, and Vlahov D: High prevalenceof iron deficiency and anemia among female injection drug users
SAAG ET AL.1044
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1044

with and without HIV infection. J Acquir Immune Defic Syndr2002;29:142–144.
2. Semba RD, Shah N, Klein RS, Mayer KH, Schuman P, and Vla-hov D: HER Human Immunodeficiency Virus Epidemiology Re-search Study Group. Prevalence and cumulative incidence of andrisk factors for anemia in a multicenter cohort study of human im-munodeficiency virus-infected and -uninfected women. Clin InfectDis 2002;34:260–266.
3. Lundgren JD, Mocroft A, Gatell JM, et al.: The change in risk ofclinical progression after initiation of HAART: The EuroSIDAstudy. 40th Interscience Conference on Antimicrobial Agents andChemotherapy, 340, 2000 (abstract).
4. Creagh T, Mildvan D, Bohn H, Moore R, and Ray L: A case-con-trol study to examine the association of anemia with HIV/AIDSprogression: Results from the 1996 enrollment cohort. The 1st IASConference on HIV Pathogenesis and Treatment, Buenos Aires,Argentina, July 9, 2001 (abstract ANO. 318).
5. Levine AM, Berhane K, Masri-Lavine L, et al.: Prevalence andcorrelates of anemia in a large cohort of HIV-infected women:Women’s Interagency HIV Study. J Acquir Immune Defic Syndr2001;26:28–35.
6. Servais J, Nkoghe D, Schmit J-C, et al.: HIV-associated hemato-logic disorders are correlated with plasma viral load and improveunder highly active antiretroviral therapy. J Acquir Immune DeficSyndr 2001;28:221–225.
7. Palella FJ Jr, Delaney KM, Moorman AC, et al.: Declining mor-bidity and mortality among patients with advanced human immu-nodeficiency virus infection. HIV Outpatient Study Investigators.N Engl J Med 1998;338:853–860.
8. Grossman HA, Goon B, Bowers P, Leitz G, and the 010 StudyGroup: Once-weekly epoetin alfa dosing is as effective as three-times-weekly dosing in increasing hemoglobin levels and is asso-ciated with improved quality of life in anemic, HIV-infected pa-tients. J Acquir Immune Defic Syndr 2003;34:368–378.
9. Abrams DI, Steinhart C, and Frascino R: Epoetin alfa therapy foranaemia in HIV-infected patients: Impact on quality of life. Int JSTD AIDS 2000;11:659–665.
10. Henry DH, Beall GN, Benson CA, et al.: Recombinant human erythropoietin in the treatment of anemia associated with humanimmunodeficiency virus (HIV) infection and zidovudine therapy.Ann Intern Med 1992;117:739–748.
11. Revicki DA, Brown RE, Henry DH, McNeill MV, Rios A, andWatson T: Recombinant human erythropoietin and health-relatedquality of life in AIDS patients with anemia. J Acquir ImmuneDefic Syndr 1994;7:474–484.
12. Moore RD Keruly JC, and Chaisson RE: Anemia and survival inHIV infection. J Acquir Immune Defic Syndr 1998;19:29–33.
13. Glaspy J, Bukowski R, Steinberg D, Taylor C, Tchekmedyian S,and Vadhan-Raj S: Impact of therapy with epoetin alfa on clinicaloutcomes in patients with nonmyeloid malignancies during cancerchemotherapy in community oncology practice. J Clin Oncol1997;15:1218–1234.
14. Demetri GD, Kris M, Wade J, Degas L, and Cella D: Quality-of-life benefit in chemotherapy patients treated with epoetin alfa isindependent of disease response or tumor type: Results from aprospective community oncology study. J Clin Oncol1998;16:3412–3425.
15. Gabrilove JL, Cleeland CS, Livingston RB, Sarokhan B, Winer E,and Einhorn LH: Clinical evaluation of once-weekly dosing of epo-etin alfa in chemotherapy patients: Improvements in hemoglobinand quality of life are similar to three-times-weekly dosing. J ClinOncol 2001;9:2875–2882.
16. McCormack HM, Horne DJ, and Sheather S: Clinical applicationsof visual analog scales: A critical review. Psychol Med 1988;18:1007–1009.
17. Revicki DA, Sorensen S, and Wu AW: Reliability and validity ofphysical and mental health summary scores from the Medical Out-comes Study HIV Health Survey. Med Care 1998;3:126–137.
18. Delate T and Coons SJ: The use of 2 health-related quality-of-lifemeasures in a sample of persons infected with human immunode-ficiency virus. Clin Infect Dis 2001;32:e47–e52.
19. Wachtel T, Piette J Mor V, Stein M, Fleishman J, and CarpenterC: Quality of life in persons with human immunodeficiency virusinfection: Measurement by the Medical Outcomes Study Instru-ment. Ann Intern Med 1992;116:129–137.
20. Wu AW, Revicki DA, Jacobson D, and Malitz FE: Evidence of re-liability, validity and usefulness of the Medical Outcomes StudyHIV Health Survey (MOS-HIV). Qual Life Res 1997;6:481–493.
21. Crawford J, Demetri GD, Gabrilove JL, Blasi MV, Sarokhan BJ,and Glaspy J: Clinical benefits of epoetin alfa therapy in patientswith lung cancer. Clin Lung Cancer 2002;3:180–190.
22. Littlewood TJ, Bajetta E, Nortier JWR, Vercammen E, RapoportB, and the Epoetin Alfa Study Group: Effects of epoetin alfa onhematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: Results of a randomized,double-blind placebo-controlled trial. J Clin Oncol 2001;19:2865–2874.
23. Volberding P, for the Anemia in HIV Working Group: Consensusstatement: Anemia in HIV infection—current trends, treatment op-tions, and practice strategies. Clin Ther 2000;22:1004–1020.
24. Fischl M, Galpin JE, Levine JD, et al.: Recombinant human eryth-ropoietin for patients with AIDS treated with zidovudine. N EnglJ Med 1990;322:1488–1493.
25. Moore RD: Improved survival with correction of anemia in HIVdisease. 6th Conference on Retroviruses and Opportunistic Infec-tions, Chicago, January 31, 1999 (abstract 706).
26. Sharp V, Paredes J, and Steinbock C: Anemia in HIV disease inthe HAART era: Is it common? Blood 1999;94(Suppl. 1):8b (ab-stract 3179).
27. Mildvan D and Creagh T, for the Anemia Prevalence Study Group:Anemia more prevalent in women and African Americans withHIV/AIDS. The 1st IAS Conference on HIV Pathogenesis and Treat-ment, Buenos Aires, Argentina, July 9, 2001 (abstract ANO. 319).
28. Mocroft A, Kirk O, Barton SE, et al.: Anaemia is an independentpredictive marker for clinical prognosis in HIV-infected patientsfrom across Europe. Acquir Immune Defic Syndr 1999;13:943–950.
29. Semba RD, Shah N, Klein RS, et al.: Highly active antiretroviraltherapy associated with improved anemia among HIV-infectedwomen. AIDS Patient Care STDs 2001;15:473–480.
30. Semba RD, Shah N, and Vlahov D: Improvement of anemia amongHIV-infected drug users receiving highly active antiretroviral ther-apy. J Acquir Immune Defic Syndr 2001;26:315–319.
31. Moore RD and Forney D: Anemia in HIV-infected patients re-ceiving highly active antiretroviral therapy. J Acquir Immune DeficSyndr 2002;29:54–57.
32. Sullivan PS, Hanson DL, Chu SY, Jones JL, and Ward JW: Epi-demiology of anemia in human immunodeficiency virus (HIV)-in-fected persons: Results from the Multistate Adult and AdolescentSpectrum of HIV Disease Surveillance Project. Blood 1998;91:301–308.
Address reprint requests to:Michael S. Saag
908 20th Street SouthCCB Room 142
Birmingham, Alabama 35294-2050
E-mail: [email protected]
QW EPOETIN ALFA IN ANEMIC HIV� PATIENTS 1045
5253_a01_p1037-1045 10/13/04 9:59 AM Page 1045