Embed Size (px)
Citation preview
NRP 2006:Assisted Ventilation
Khalid Aziz,
Canadian NRP Committee

Cape Spear from St. John’s, Newfoundland & Labrador
StitchesSeptember 2006
Philosophy
Establishing effective ventilation is the primary objective in the management of the apneic or bradycardic newborn infant in the delivery room. ILCOR 2005
Objectives
a) To present significant changes to the
practice of assisted ventilation
b) To explain the relevant ILCOR
consensus processes and summarize
some of the evidence
Areas of Focus
With respect to resuscitation of the newborn:
• Characteristics of initial assisted breaths
• Devices used for assisted ventilation
• Ventilatory needs of the preterm baby
NRP: Importance of Heart Rate
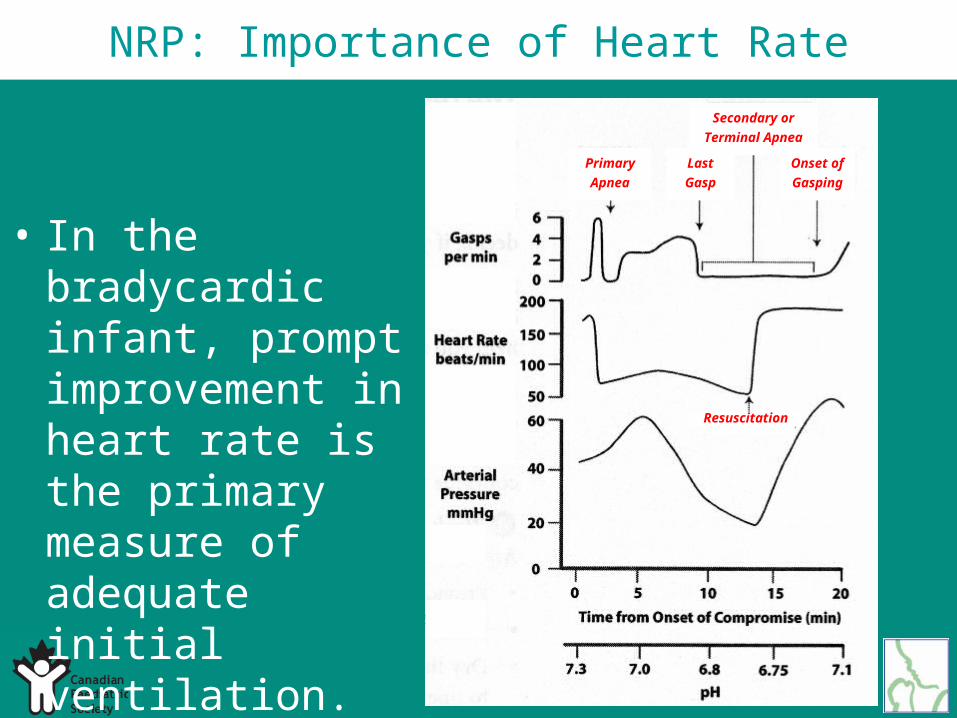
• In the bradycardic infant, prompt improvement in heart rate is the primary measure of adequate initial ventilation.
• Check signs of improvement after 30 seconds of PPV. This requires the assistance of another person.
NRP: Importance of Heart Rate
Primary
Apnea
Last
Gasp
Secondary or
Terminal Apnea
Onset of
Gasping
Resuscitation
• In the bradycardic infant, prompt improvement in heart rate is the primary measure of adequate initial ventilation.

NRP: Optimal Initial Ventilation
• An initial ventilation pressure of 20 cm H2O may be effective (ILCOR).
• >30-40 cm H2O may be necessary in some term babies (ILCOR).
NRP: Optimal Initial Ventilation
NRP: Positive End-Expiratory Pressure
• If ongoing positive pressure ventilation is required, PEEP of 3-6 cm of water should be used (Canadian NRP 2006).
• PEEP may be given with a flow-inflating bag or a T-piece resuscitator (Canadian NRP 2006).
• A self-inflating bag with a PEEP valve is also an acceptable alternative (Canadian NRP 2006).
NRP: Inflation Times
There is insufficient evidence to recommend optimal initial and subsequent inflation times (ILCOR 2005).
NRP: Assisted Ventilation Devices
• A self-inflating bag,
• a flow-inflating bag,
• or a T-piece mechanical device designed to regulate pressure as needed
can be used to provide bag-valve-mask ventilation to a newborn (ILCOR 2005)
NRP: Assisted Ventilation Devices
NRP: Self inflating bag and PEEP
• PEEP may be provided using an additional PEEP valve on a self-inflating bag
• Self-inflating bags cannot provide CPAP
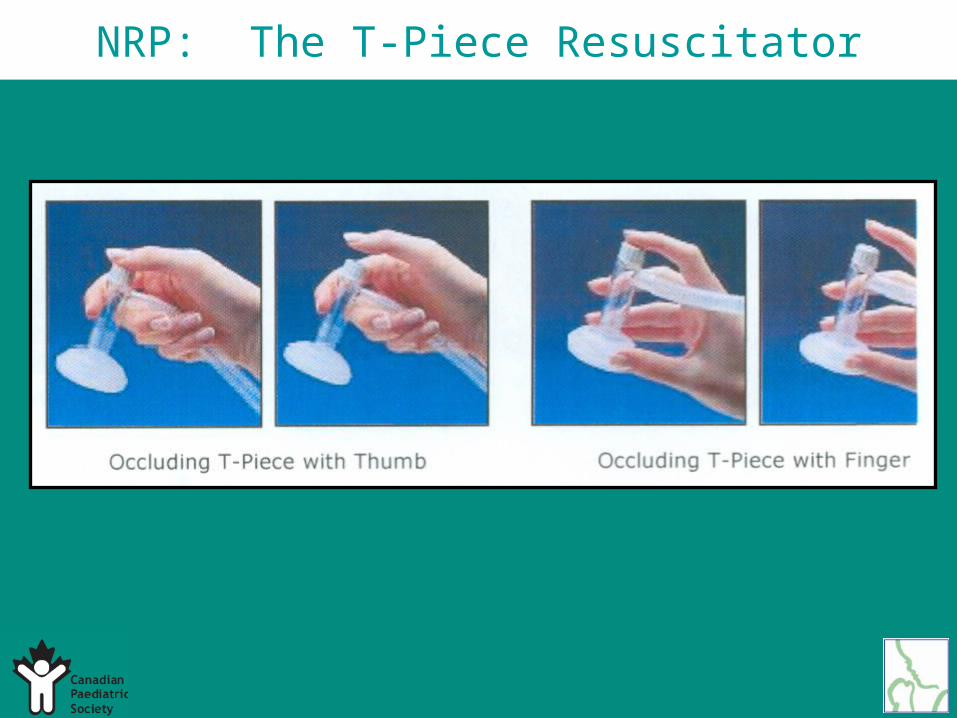
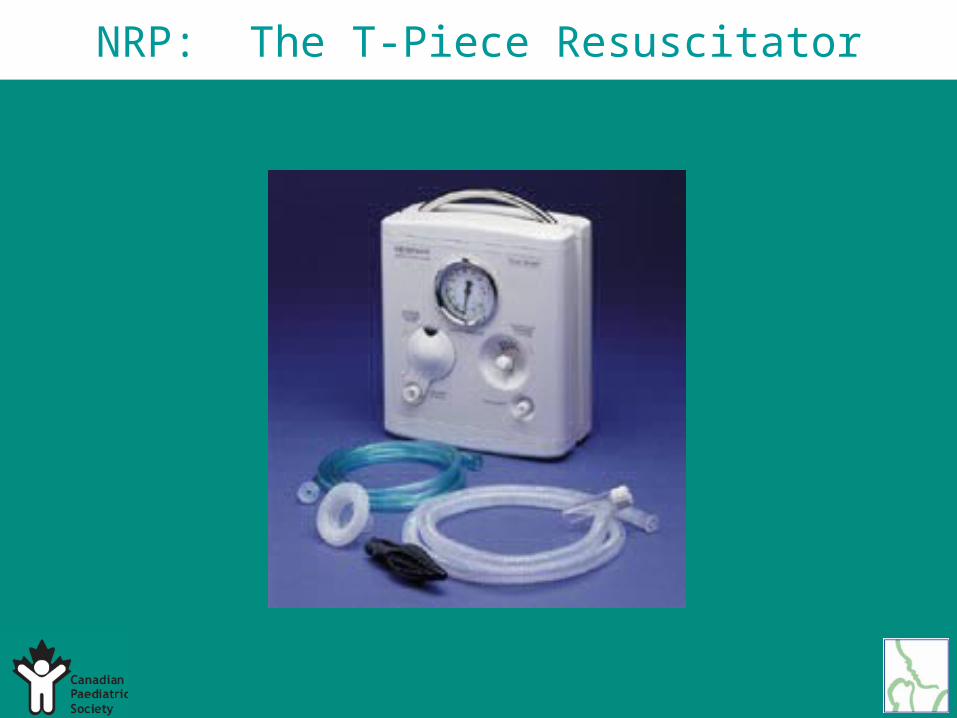
NRP: The T-Piece Resuscitator
NRP: The T-Piece Resuscitator
• The description
• Advantages and disadvantages
• Practical use
NRP: Confirming ETT Placement
• An increasing heart rate and exhaled CO2 detection are the primary methods for confirming endotracheal tube placement (NRP 2006).
• CO2 detector should be used as the primary method for confirming endotracheal tube placement (Canadian NRP 2006).
NRP: Confirming ETT Placement
NRP: Pressures in Preterm Infants
• Avoid creation of excessive chest wall movement (ILCOR 2005).
• An initial inflation pressure of 20-25 cm H2O is adequate for most preterm infants (ILCOR 2005).
NRP: Other Preterm Issues
• Use the lowest pressures necessary to achieve an adequate response
• Consider giving CPAP (not with a self-inflating bag)
• Consider giving surfactant if the baby is significantly preterm
The tip of the iceberg
Step 1A. Refine the research question(s)
Step 1B. Gather the evidence
The ILCOR Consensus ProcessThe ILCOR Consensus ProcessStep 1: State the Proposal
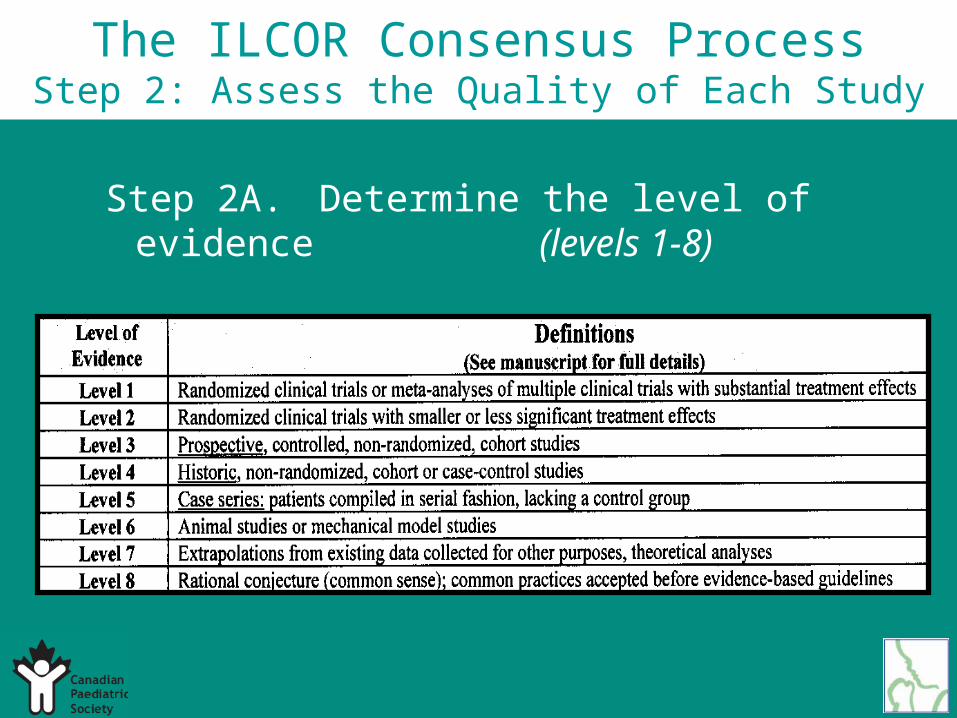
Step 2A. Determine the level of evidence (levels 1-8)
The ILCOR Consensus ProcessStep 2: Assess the Quality of Each Study
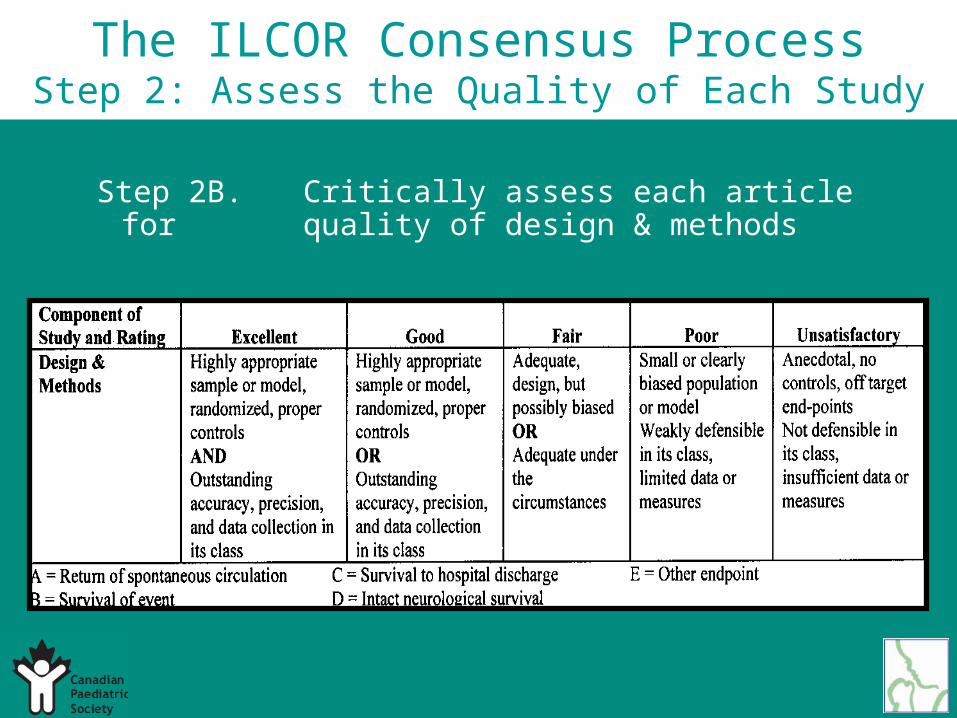
Step 2B. Critically assess each article for quality of design & methods
The ILCOR Consensus ProcessStep 2: Assess the Quality of Each Study
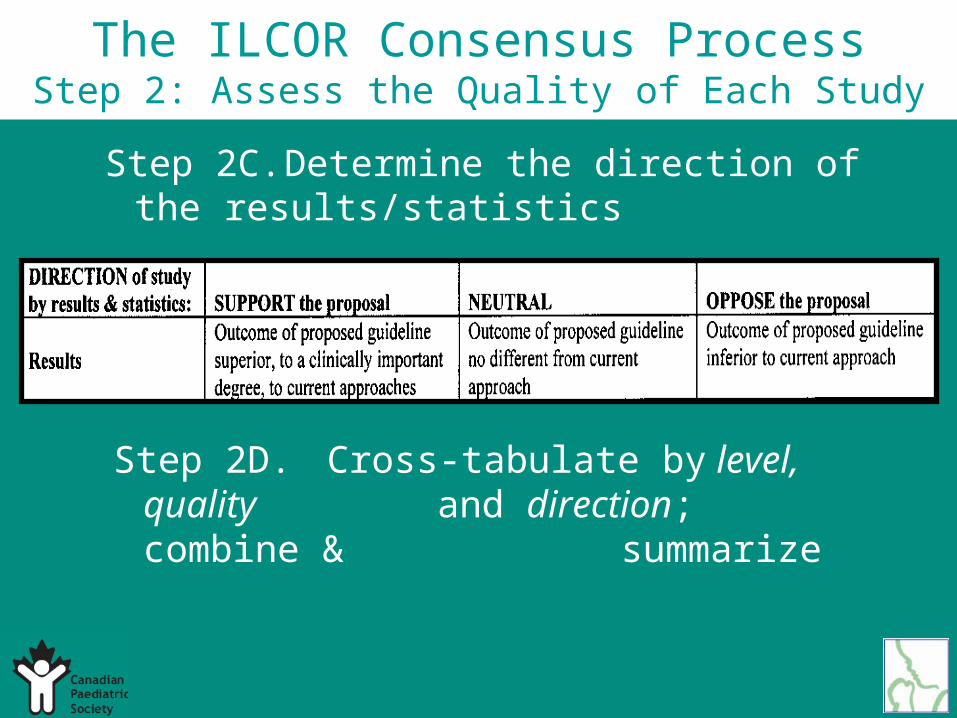
Step 2C. Determine the direction of the results/statistics
Step 2D. Cross-tabulate by level, quality and direction; combine &
summarize
The ILCOR Consensus ProcessStep 2: Assess the Quality of Each Study

The ILCOR Consensus Process Step 2: Example of result
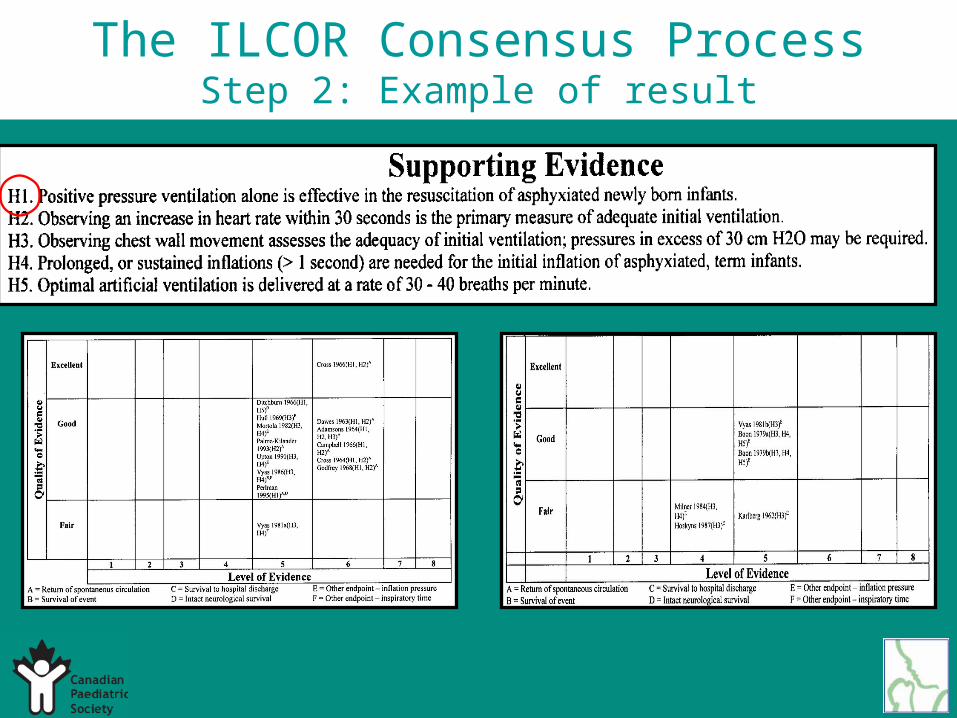
The ILCOR Consensus ProcessStep 2: Example of result
The ILCOR Consensus ProcessStep 2: Example of result
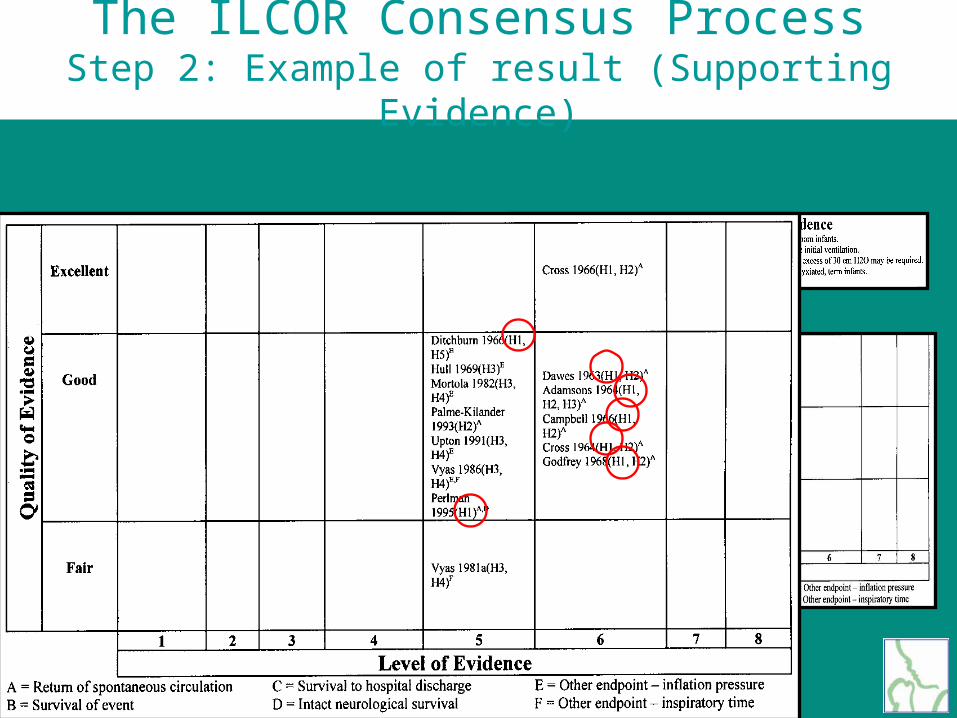
The ILCOR Consensus ProcessStep 2: Example of result (Supporting Evidence)
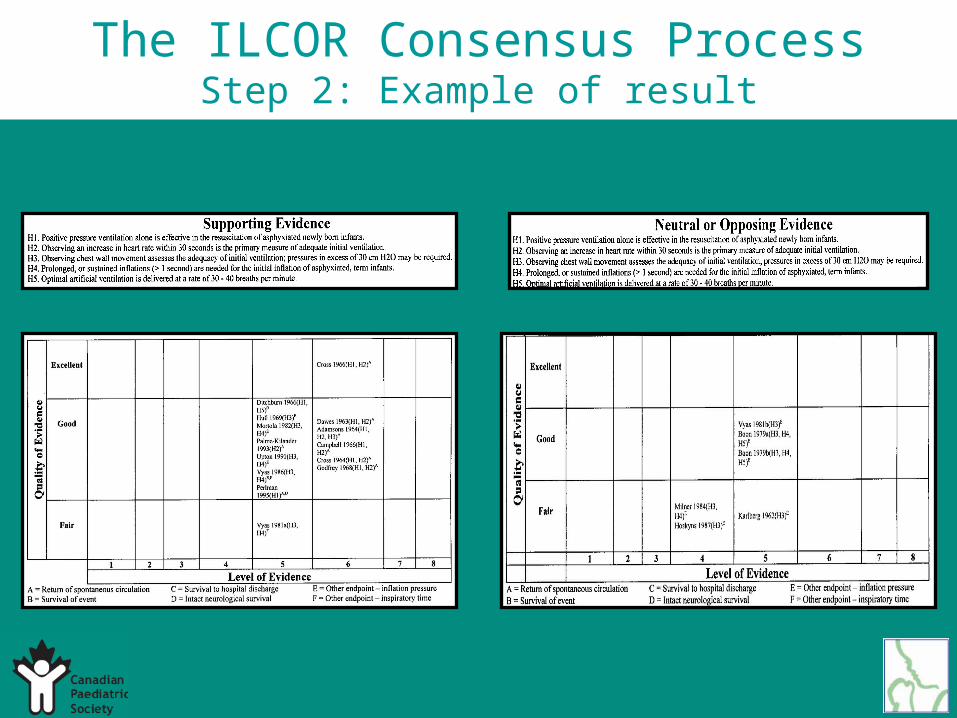
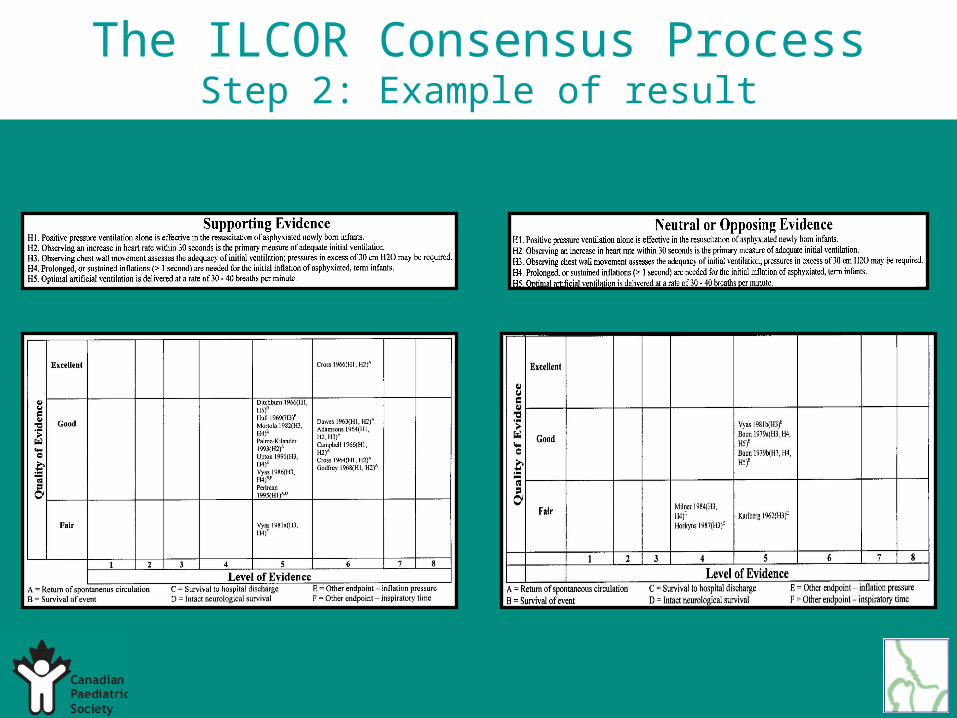
The ILCOR Consensus ProcessStep 2: Example of result
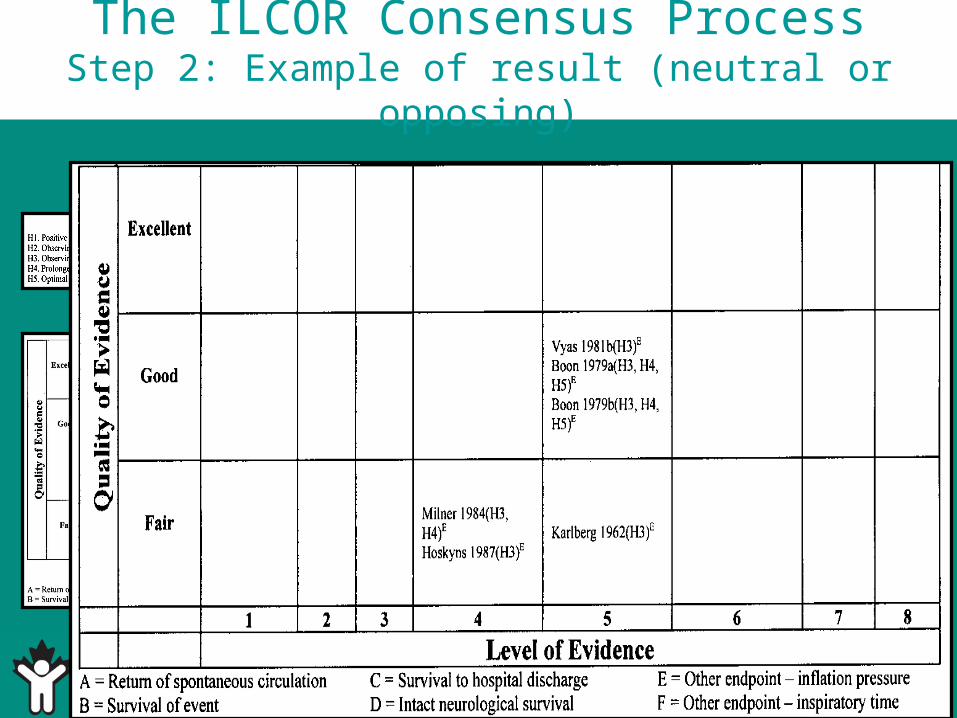
The ILCOR Consensus ProcessStep 2: Example of result (neutral or opposing)
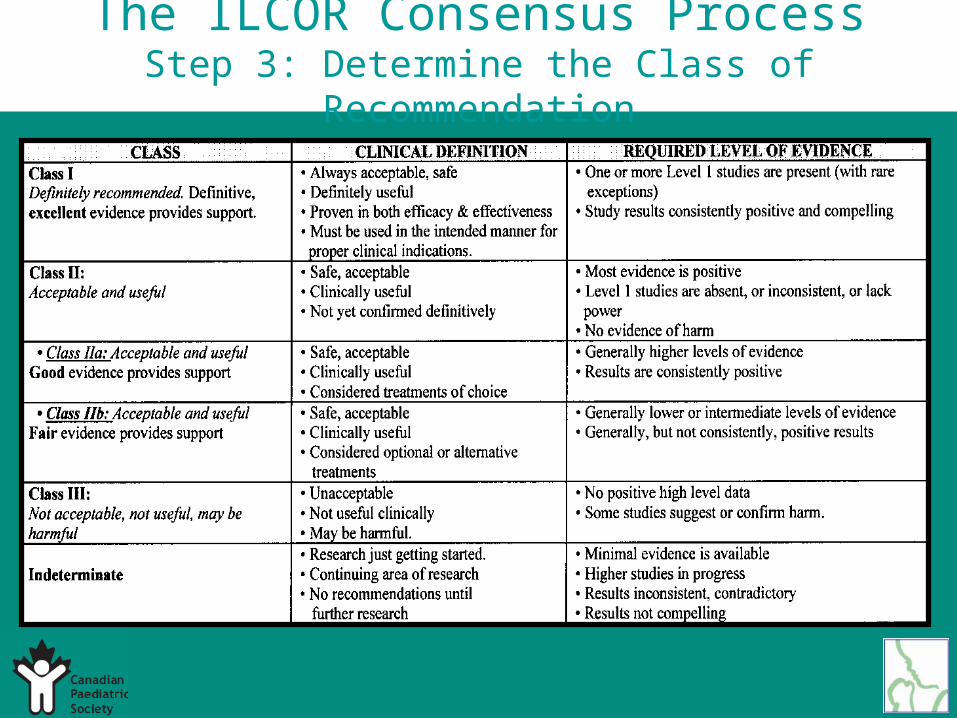
The ILCOR Consensus ProcessStep 3: Determine the Class of Recommendation
The ILCOR Consensus ProcessImportant Areas in Assisted Ventilation
• Initial Ventilation in Asphyxiated Term Newborns
• Initial Lung Inflation in Preterm Infants
• The use of CPAP during resuscitation of Very Premature Infants
Initial Ventilation in Asphyxiated Term Newborns
Step 1. State the Proposal5 Hypotheses:
• IPPV alone is effective• Best indicator of adequate initial ventilation is
heart rate• Chest movement assesses initial ventilation;
pressure >30cm H2O may be required• Prolonged/sustained inflations are needed
(>1sec) for initial inflation of asphyxiated term infant
• Optimal IPPV is 30-40 breaths per minute(728 articles reviewed / 20 included)
Initial Ventilation in Asphyxiated Term Newborns
Step 2. Assess the Quality of Each Study
2A. Determine the level of evidence
2B. Critically assess each article (researchdesign/methods)
2C. Determine direction of results statistics (+/- neutral)
2D. Cross-tabulate
Initial Ventilation in Asphyxiated Term Newborns
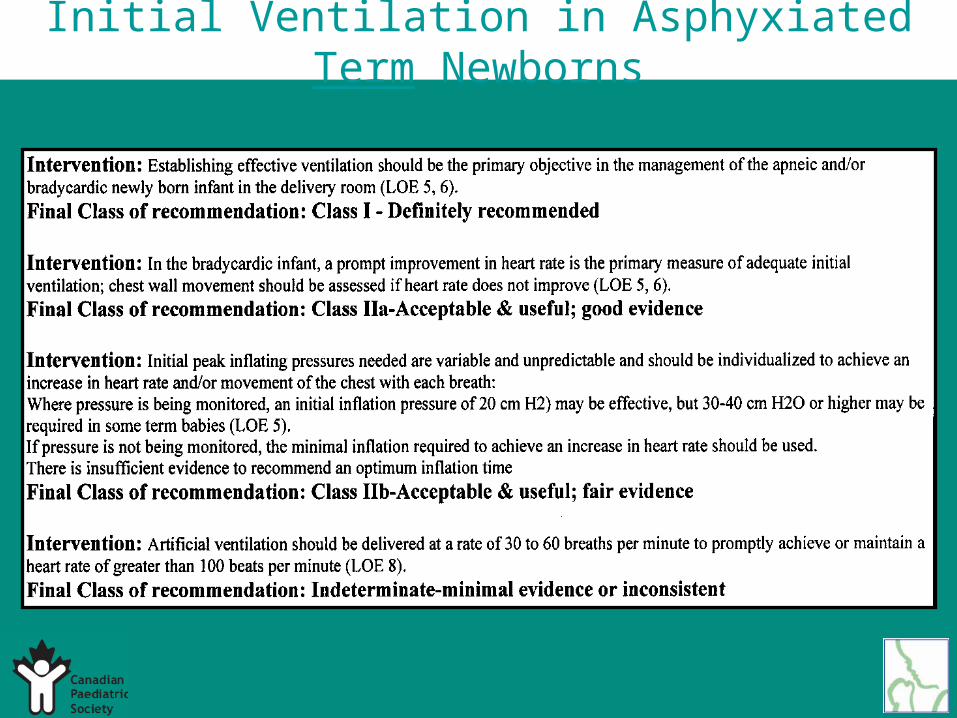
Step 3. Determine the Class of Recommendations
Class I
Class IIa
Class IIb
Class III
Indeterminate
Initial Ventilation in Asphyxiated Term Newborns
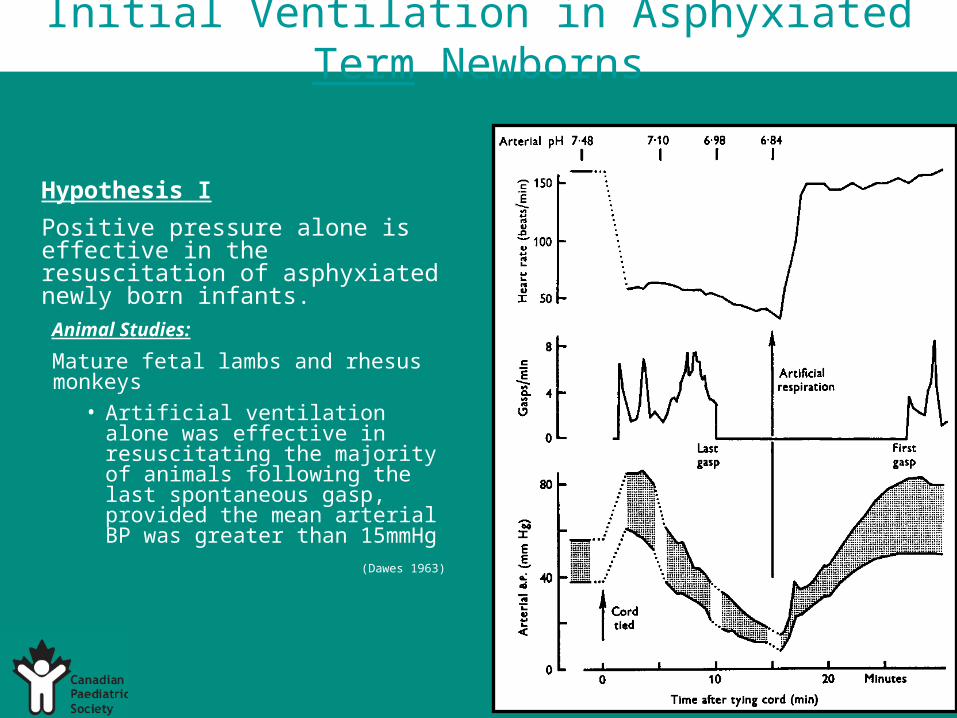
Hypothesis I
Positive pressure alone is effective in the resuscitation of asphyxiated newly born infants.
Animal Studies:
Mature fetal lambs and rhesus monkeys
• Artificial ventilation alone was effective in resuscitating the majority of animals following the last spontaneous gasp, provided the mean arterial BP was greater than 15mmHg
(Dawes 1963)
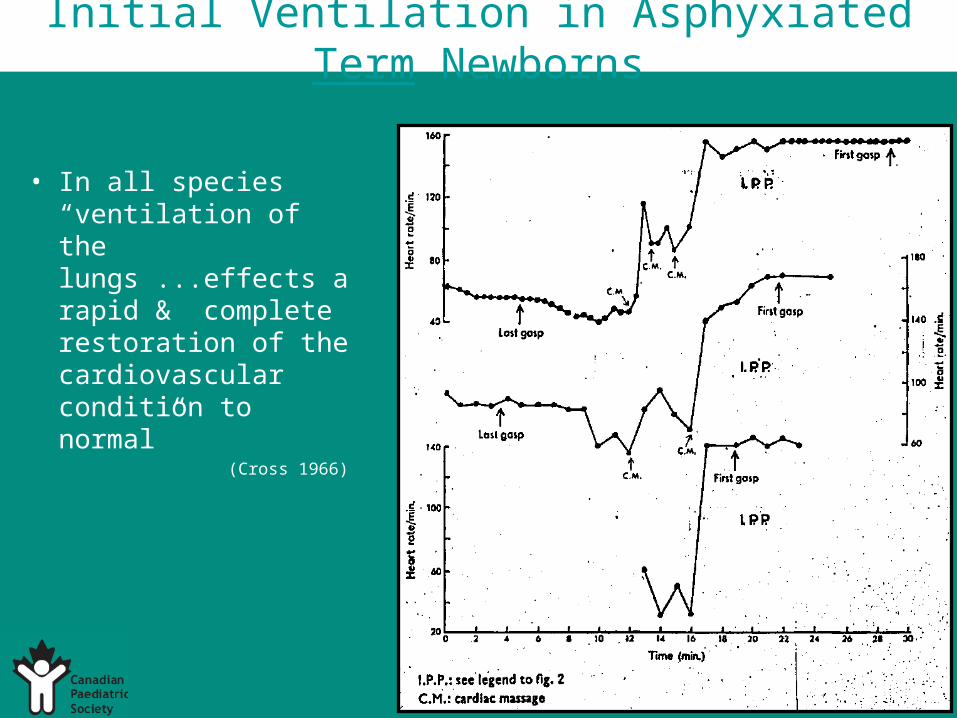
Initial Ventilation in Asphyxiated Term Newborns
• In all species “ventilation of the lungs ...effects a rapid & complete restoration of the cardiovascular condition to normal”
(Cross 1966)
Initial Ventilation in Asphyxiated Term Newborns
Criteria of Effective Treatment:
• Gasping returns only after recovery of the circulation
• The increase in heart rate (if maintained at a reasonable level) is a reliable guide to this recovery
(Cross 1966)
• IPPV is much more effective than hyperbaric O2 in newborn rabbits – 85% recovered with IPPV alone ~ 4mins. ...or IPPV and cardiac massage
(Campbell 1966)
Initial Ventilation in Asphyxiated Term Newborns
12 fetal rhesus monkeys asphyxiated under controlled conditions:
– 6/12 - rapid response to IPPV alone– remaining 6 – prompt response to chest compressions
and IPPV – mean arterial BP lower in those who required CPR
(Adamsons 1964)
Fetal and newborn rabbits under controlled asphyxia:“...surest sign that lung inflation was going to succeed was
an increase in heart rate and BP”(Godfrey 1968)
Initial Ventilation in Asphyxiated Term Newborns
Hypothesis II
Observing an increase in heart rate within 30 seconds is the primary measure of adequate initial ventilation.
Human Studies:
31 full term infants, delivered by c-section, required intubation and ventilation
– “IPPV through an endotracheal tube is at least as effective in producing lung expansion as is spontaneous respiration”
(Ditchburn 1966)
Demonstrated that prompt increase in heart rate ≥ 130/min. was proof of adequate ventilation
(Palme-Kilander 1993)
Initial Ventilation in Asphyxiated Term Newborns
Hypothesis III
Observing chest wall movement assesses the adequacy of initial ventilation – pressures in excess of 30cm H2O may be required
Hypothesis IV
Prolonged or sustained inflations (>1 second) are needed for the initial inflation of asphyxiated term infants
Initial Ventilation in Asphyxiated Term Newborns
Several studies looked at pressure and volume changes in healthy term newborns with the onset of spontaneous respirations:
• Babies produce large negative intrathoracic pressures of up to 50cm H2O before lung expansion occurs
• 7/11 babies had formed FRC at the end of the first breath(Karlberg 1960)
Initial Ventilation in Asphyxiated Term Newborns
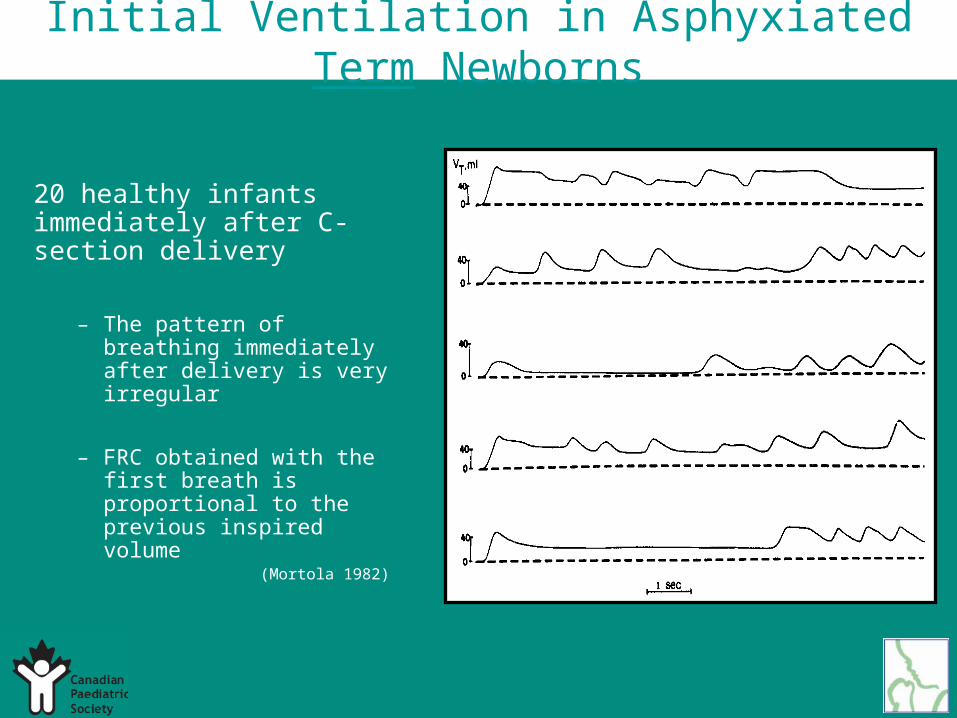
20 healthy infants immediately after C-section delivery
– The pattern of breathing immediately after delivery is very irregular
– FRC obtained with the first breath is proportional to the previous inspired volume
(Mortola 1982)
15 babies – elective c-section– 5/11 had formed FRC
35 babies – born vaginally– 20/21 had formed FRC
Initial Ventilation in Asphyxiated Term Newborns
Studied the first breath of 50 babies:
Possible explanations:
1) Vaginal birth canal squeeze2) Vaginal delivery – babies make a strong expiratory effort
(expiratory pressures in c/s group were 25% smaller)3) Balance of fluid dynamics within the lungs:
- no opening pressure- inspiratory pressure & volume same- expiratory pressure lower in c/s group
(Vyas 1981)
Initial Ventilation in Asphyxiated Term Newborns
Studied the establishment of FRC:
34 term babies vaginally delivered: recorded ~ the first 30 seconds (≥ 3 breaths)
Looked at:
– Magnitude of the birth canal squeeze– Interval between delivery of the chest and the onset of
the first breath– Inspiratory pressure changes– Expiratory pressure changes– Gaseous FRC at the end of the first breath
Initial Ventilation in Asphyxiated Term Newborns
Results:
– No evidence of opening pressure– All babies had a marked positive pressure during
expiration - in 13/16 this exceeded 50cm H2O
– All except 1 formed FRC following the first breath– * Significant correlation between inspiratory volume
and FRC
* emerged above all other factors in the formation of FRC(Vyas 1986)
Initial Ventilation in Asphyxiated Term Newborns
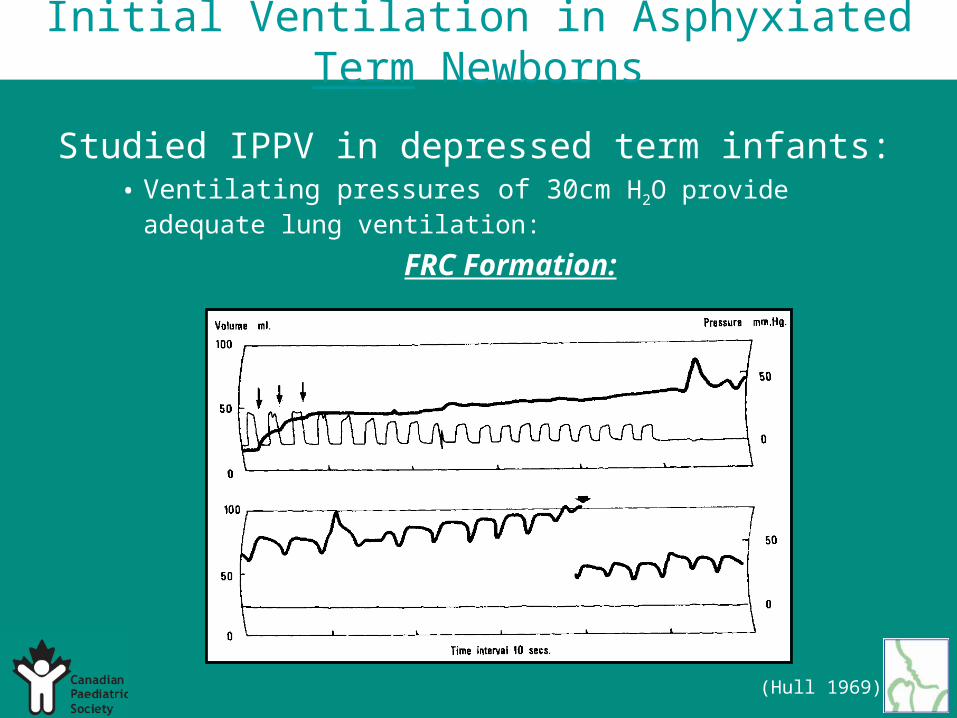
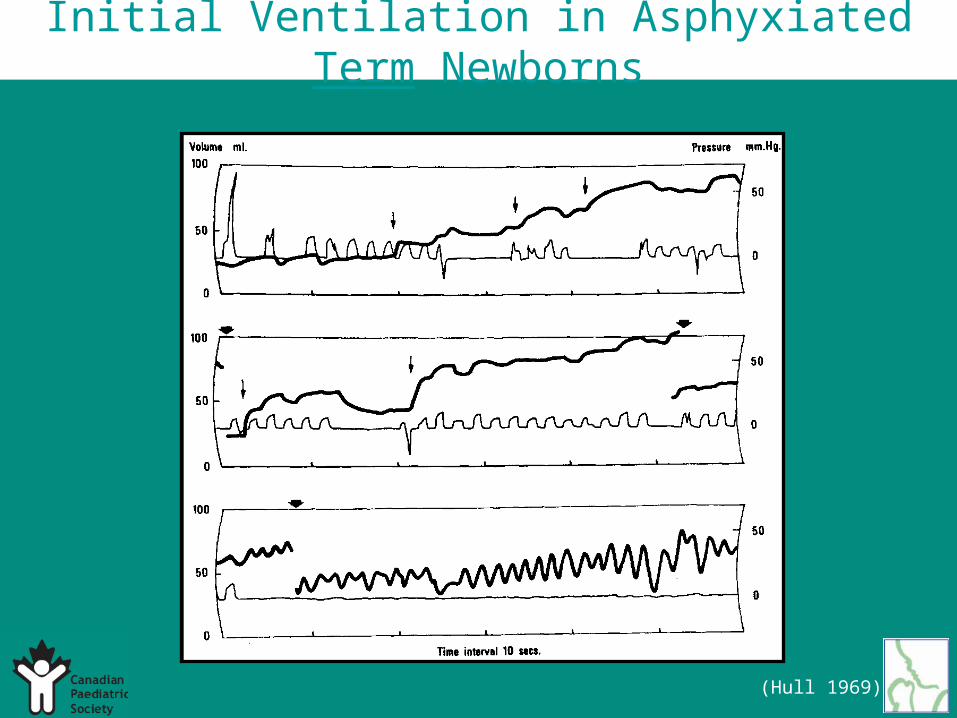
Studied IPPV in depressed term infants:• Ventilating pressures of 30cm H2O provide adequate lung
ventilation:
FRC Formation:
(Hull 1969)
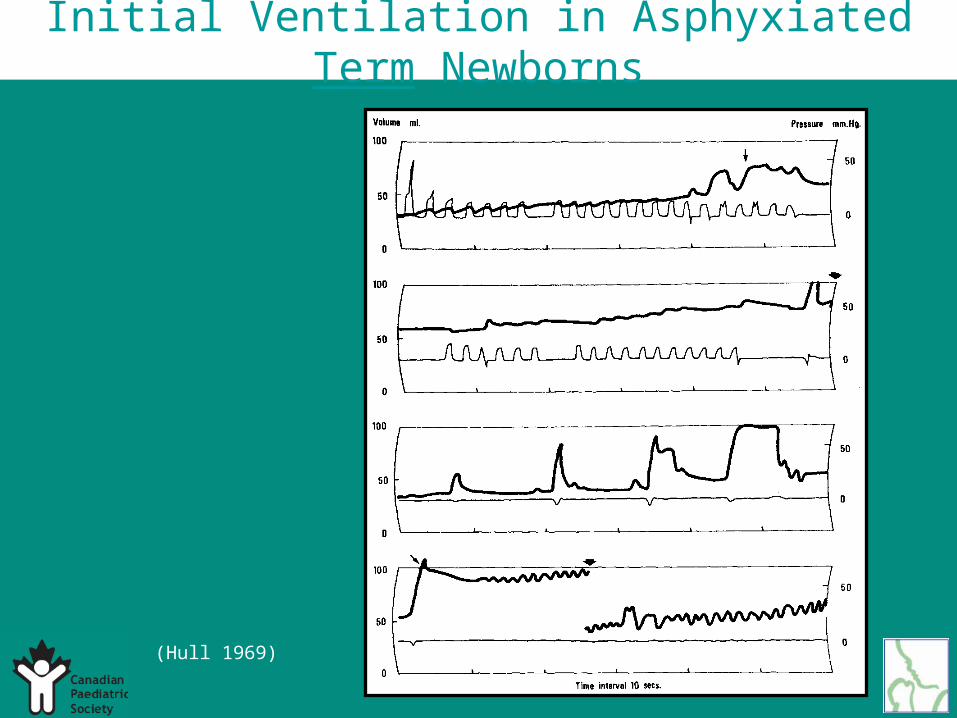
Initial Ventilation in Asphyxiated Term Newborns
(Hull 1969)
Initial Ventilation in Asphyxiated Term Newborns
(Hull 1969)

Initial Ventilation in Asphyxiated Term Newborns
(Hull 1969)
Initial Ventilation in Asphyxiated Term Newborns
Respiratory reflex responses:
– Strong expiratory effort (“rejection response”)
– Inspiratory efforts (paradoxical reflex of Head)
(Hull 1969)
Initial Ventilation in Asphyxiated Term Newborns
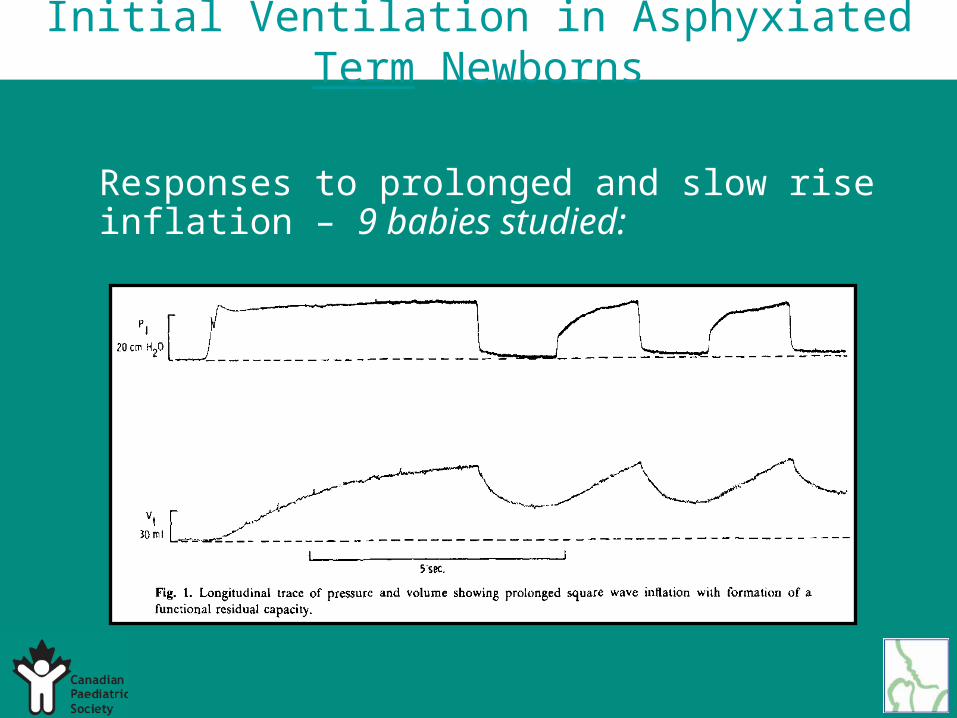
Responses to prolonged and slow rise inflation – 9 babies studied:
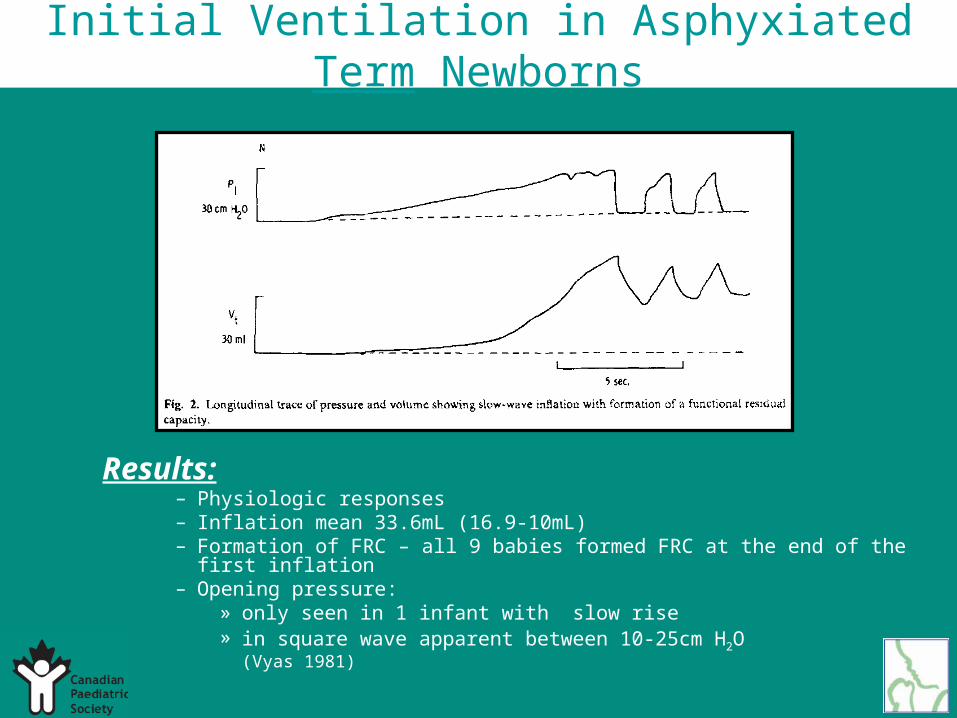
Initial Ventilation in Asphyxiated Term Newborns
Results:– Physiologic responses– Inflation mean 33.6mL (16.9-10mL)– Formation of FRC – all 9 babies formed FRC at the end of the first inflation– Opening pressure:
» only seen in 1 infant with slow rise» in square wave apparent between 10-25cm H2O
(Vyas 1981)
Initial Ventilation in Asphyxiated Term Newborns
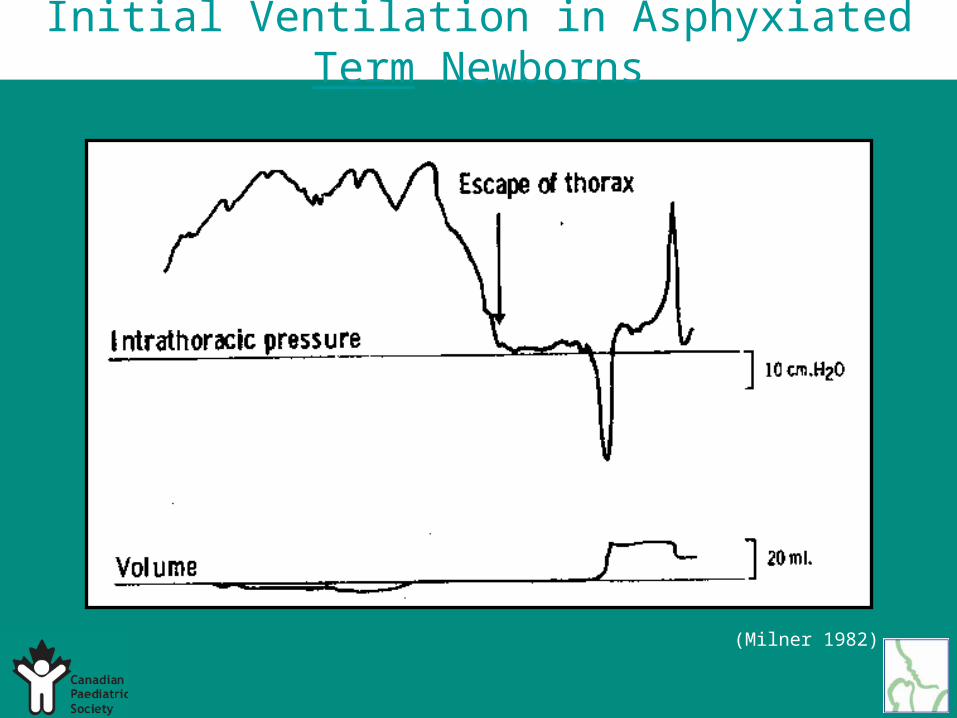
(Milner 1982)
Initial Ventilation in Asphyxiated Term Newborns
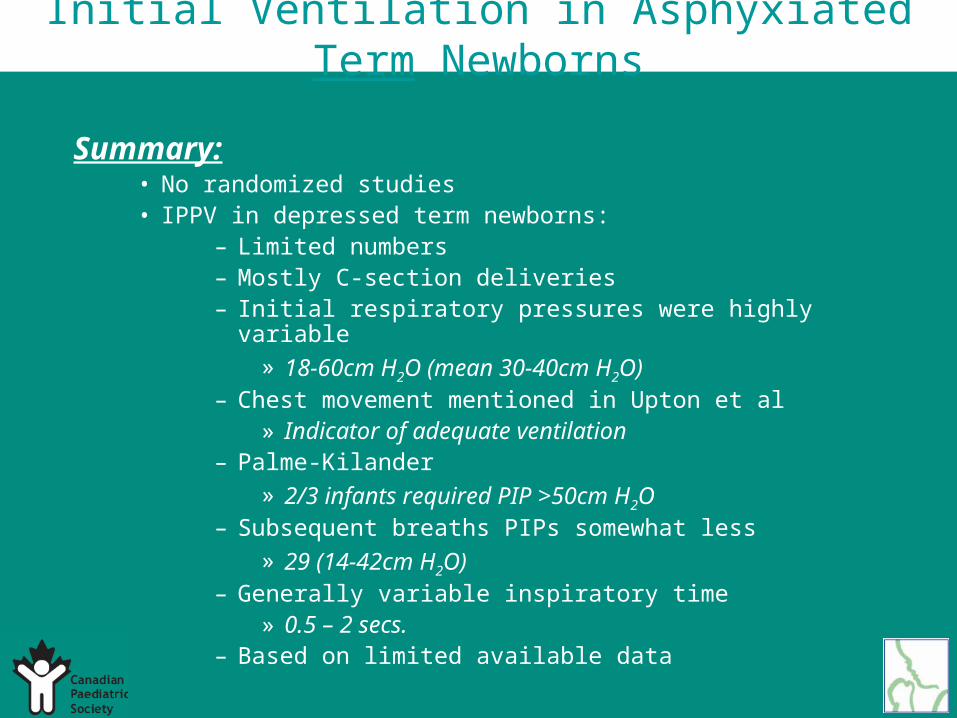
Summary:• No randomized studies• IPPV in depressed term newborns:
– Limited numbers– Mostly C-section deliveries– Initial respiratory pressures were highly variable
» 18-60cm H2O (mean 30-40cm H2O)– Chest movement mentioned in Upton et al
» Indicator of adequate ventilation– Palme-Kilander
» 2/3 infants required PIP >50cm H2O – Subsequent breaths PIPs somewhat less
» 29 (14-42cm H2O)– Generally variable inspiratory time
» 0.5 – 2 secs.– Based on limited available data
Initial Ventilation in Asphyxiated Term Newborns
Initial Lung Inflation in Preterm Newborns
Step 1. State the Proposal
Hypothesis:• Methods of achieving initial lung inflation during
resuscitation of term infants are inappropriate for use in preterm infants
Gather evidence:• 47 articles from human studies
• 13 articles from animal studies
Step 2. Assess the Quality of Each Study
2A Determine the level of evidence2B Critically assess each article
(research design/methods)2C Determine direction of results
statistics (+/- neutral)2D Cross-tabulate
* different endpoints
Initial Lung Inflation in Preterm Newborns
Step 3. Determine the class of Recommendations
Class IClass II
IIaIIb
Class IIIIndeterminate
Initial Lung Inflation in Preterm Newborns
Animal Studies:
44 premature rabbits:
- ventilated with standardized tidal volume of 10mL/kg of standardized insufflation
pressures of 35cm H2O from 10-30 minutes:
•Necrosis and degeneration of bronchiolar epithelium appeared in animals ventilated for 5 min. or more
(Nilsson 1980)
16 premature lambs, 8 received 4 sustained inflations for 5 seconds
•SI did not improve lung function(Klopping-Ketelaars 1994)
Initial Lung Inflation in Preterm Newborns

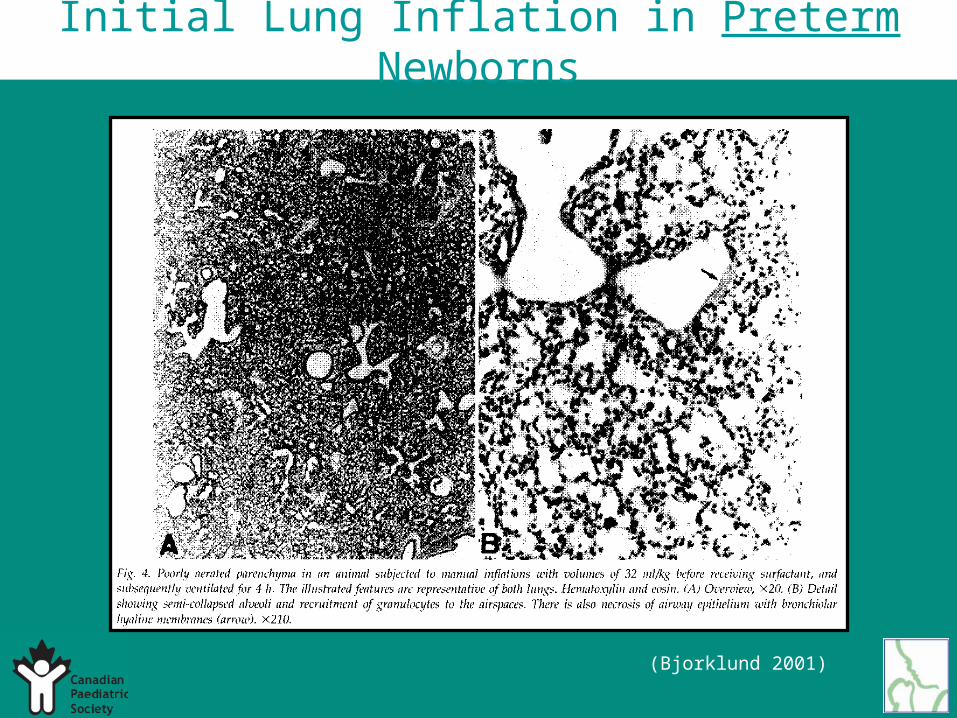
5 pairs of premature lamb siblings:- one of each pair given 6 manual inflations, 35-
40mL/kg (“bagging”)- all lambs given surfactant at 30 min. of age:
• Histological lung injury• Impairment of compliance• Inhibited the response to surfactant
Why did a few large breaths have such a deleterious effect on lung function?
– High airway pressure during bagging– The size of the breaths– The time at which they were given– The surfactant deficiency in the lungs
(Bjorklund 1997)
Initial Lung Inflation in Preterm Newborns
Initial Lung Inflation in Preterm Newborns
21 premature lambs:
- IPPV for 30 min. after birth (tidal volumes of 5mL/kg, 10mL/kg and 20mL/kg)
- then at 30 min. - given surfactant andventilatedx 6hrs:
The group with tidal volumes of 20mL/kg:
• Lower compliance• Difficult to ventilate• Depressed surfactant recovery• Increased protein recovery
(Wada 1997)
10 premature newborn lambs:
- 2 received surfactant before birth- 2 before the first breath- 2 recruitment maneuvers – 5 breaths, 8mL/kg *- 2 recruitment maneuvers – 5 breaths, 16mL/kg *- 2 recruitment maneuvers – 5 breaths, 32mL/kg *
* followed by surfactant
» Decreased inspiratory capacity» Decreased compliance» Decreased FRC» Decreased surfactant response» More lung injury
(Bjorklund 2001)
Initial Lung Inflation in Preterm Newborns
Initial Lung Inflation in Preterm Newborns
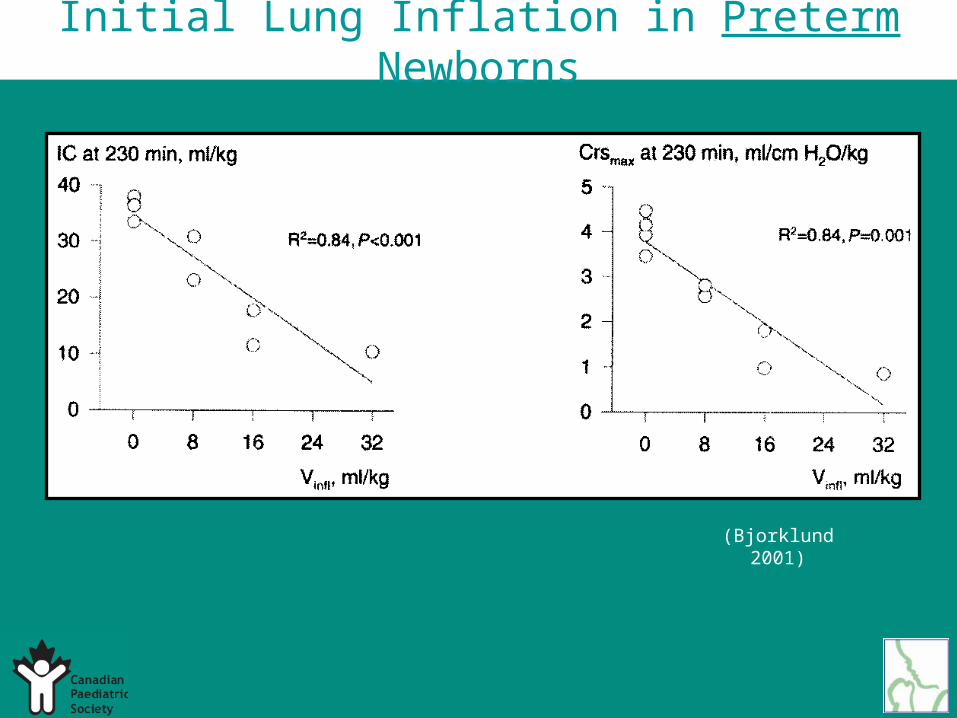
(Bjorklund 2001)
Initial Lung Inflation in Preterm Newborns
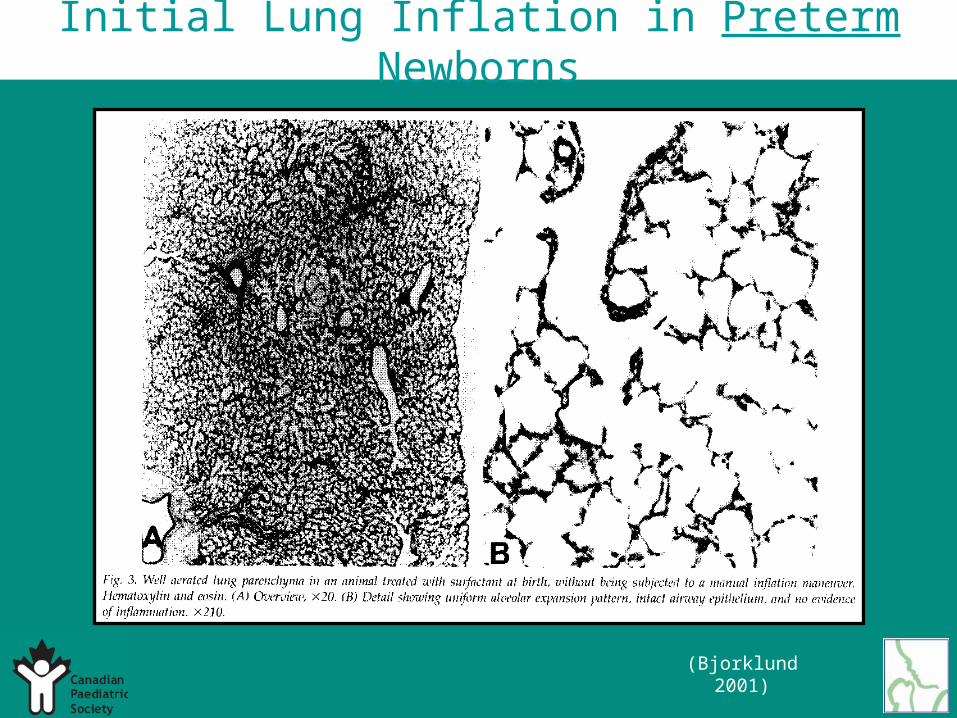
(Bjorklund 2001)
Initial Lung Inflation in Preterm Newborns
(Bjorklund 2001)
Study A. 12 preterm lambs:
Group 1 – 5 lung inflations at birth → surfactantGroup 2 – surfactant followed immediately by 5 inflationsGroup 3 – surfactant followed by inflations after 10min.Group 4 – surfactant followed by inflations after 60min.
* Inflations were 16mL/kg sustained x 5seconds
Study B. 10 pairs of twin preterm lambs:
- all received surfactant before the first breath- one of each pair got 5 inflations immediately after - the other got 5 inflations 10-15min. after
(Ingimarsson 2004)
Initial Lung Inflation in Preterm Newborns
Initial Lung Inflation in Preterm Newborns
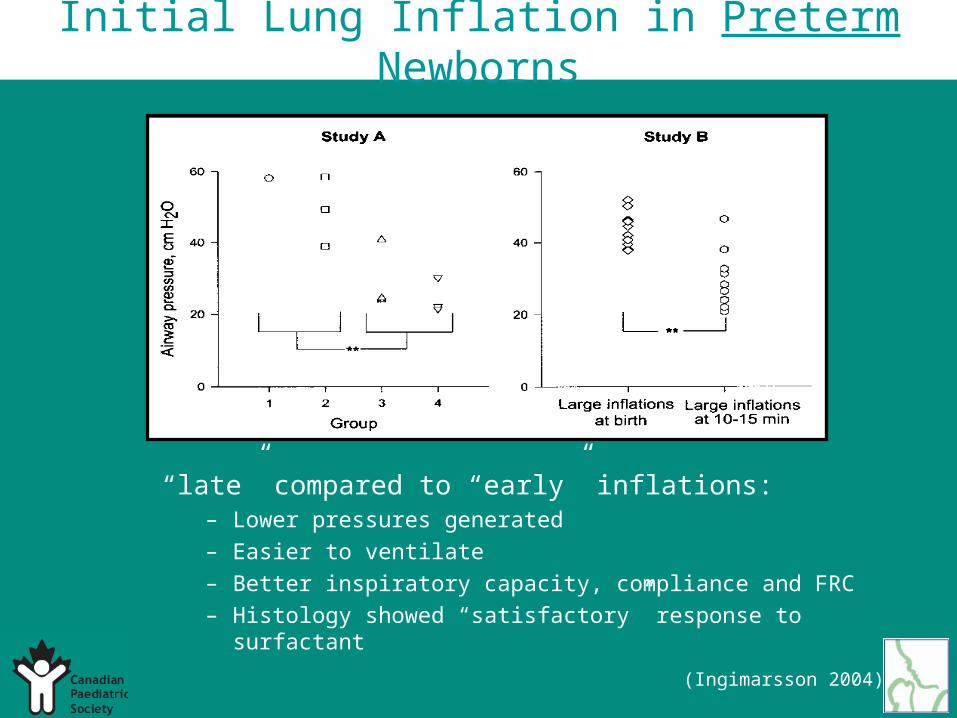
“late” compared to “early” inflations:– Lower pressures generated
– Easier to ventilate
– Better inspiratory capacity, compliance and FRC
– Histology showed “satisfactory” response to surfactant
(Ingimarsson 2004)
Initial Lung Inflation in Preterm Newborns
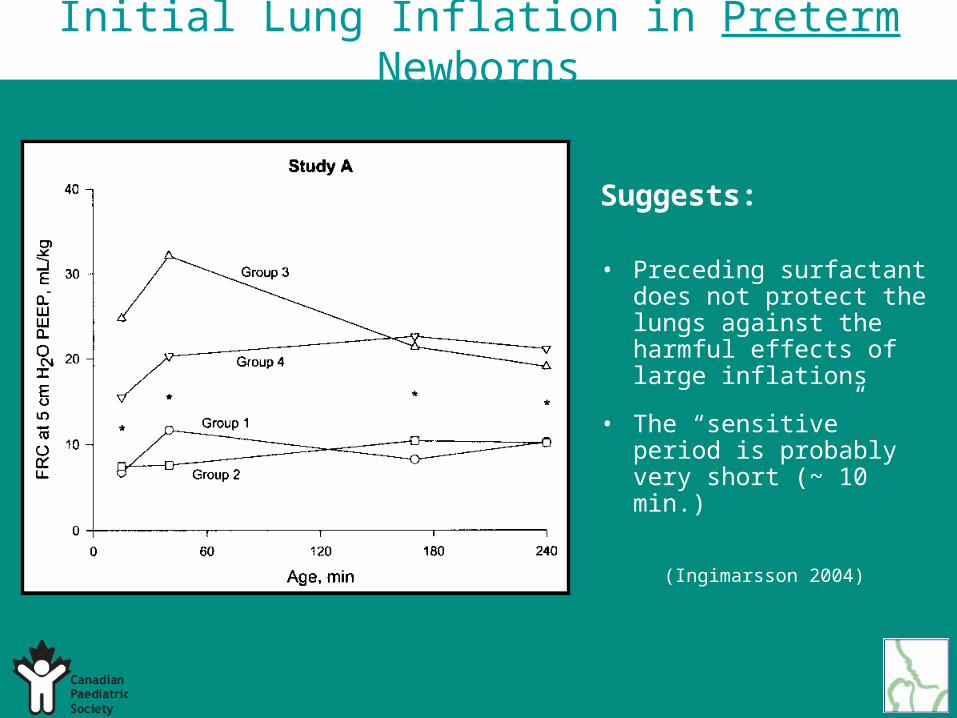
Suggests:
• Preceding surfactant does not protect the lungs against the harmful effects of large inflations
• The “sensitive” period is probably very short (~ 10 min.)
(Ingimarsson 2004)
Initial Lung Inflation in Preterm Newborns
Human Studies:
21 preterm infants, intubation and IPPV at birth (mean inflation pressure 27cm H2O)
(Hoskyns 1987)
70 preterm infants, (median pressure for adequate chest wall expansion = 22.8cm H2O):
- never required >30cm H2O(Hird 1991)
651 infants – multi-center randomized trial:
a)compared an immediate surfactant bolus
b) post-ventilatory aliqout strategy ~ 10min.
• No difference in survival
• Less chronic lung disease – O2 supplement at 36 weeks in (b)
Could be due to the vigorous bagging in the immediate group?(Kendig 1998)
Initial Lung Inflation in Preterm Newborns
123 preterm infants (retrospective cohort study):
2 different delivery room policies 1994 vs. 1996
1994 - ELBW infants intubated immediately for respiratory distress
1996 - NP tube inserted – continuous inflation 20-25cm H2O (15-20 sec.) → CPAP 4-6cm.
• Mean initial pressure requirement = 25cm H2O
• More infants in 1996 never intubated (25% vs. 7%)• Mortality & morbidity were the same
(Lindner 1999)
Initial Lung Inflation in Preterm Newborns
“Human” Element:
• Physicians unable to detect blocked ETT• Nurses with experience relied less on manometers but
were also less accurate in controlling PIP without the devices
• Junior doctors could not assess tidal volume visually in relation to inflation pressure
• NEOPUFF device – more consistent(Spears 1991)
(Howard-Glenn 1990) (Stenson 1995)
(Finer 2001)
Initial Lung Inflation in Preterm Newborns

Initial Lung Inflation in Preterm Newborns
Summary:
• Greater emphasis on improving heart rate
• Less emphasis on good chest wall movement– Encourages large, potentially damaging inflations to
preterm infants at a time when their lungs are most susceptable to injury
Initial Lung Inflation in Preterm Newborns
Use of CPAP in the Delivery Room
• Step 1. State the Proposal
Hypotheses:• CPAP is a safe and effective intervention in newborn
resuscitation compared to Endotracheal Intubation• CPAP during resuscitation of very preterm infants will
reduce oxygen requirements and the need for ventilation• The use of CPAP will decrease oxygen dependency at
36 wks. gestation
Gather evidence:• 27 articles from human studies • 3 articles from animal studies
Use of CPAP in the Delivery Room
• Step 2. Assess the Quality of EachStudy
– 2A Determine the level of evidence– 2B Critically assess each article
(research design/methods)– 2C Determine direction of results
statistics (+/- neutral)– 2D Cross-tabulate
* different endpoints
Use of CPAP in the Delivery Room
• Step 3. Determine the class of Recommendations
– Class I– Class II
• IIa• IIb
– Class III– Indeterminate
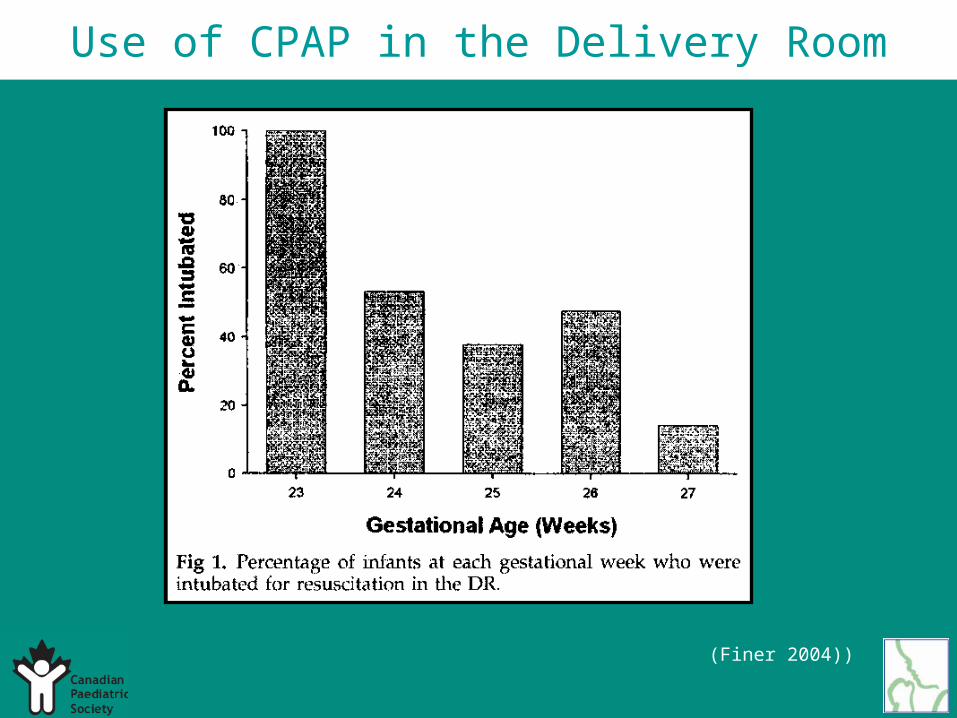
Use of CPAP in the Delivery Room
(Finer 2004))
Use of CPAP in the Delivery Room
Recommendation: Class B
• Acceptable & useful
• Fair evidence