Embed Size (px)
Citation preview

Nodal Status, Number of Lymph Nodes Examined, andLymph Node Ratio: What Defines Prognosis afterResection of Colon Adenocarcinoma?
Ana L Gleisner, MD, PhD, Harveshp Mogal, MD, Rebecca Dodson, MD, Jon Efron, MD, FACS,Susan Gearhart, MD, FACS, Elizabeth Wick, MD, Anne Lidor, MD, FACS, Joseph M Herman, MD, MSc,Timothy M Pawlik, MD, MPH, PhD, FACS
BACKGROUND: Lymph node ratio (LNR) has been proposed as an optimal staging variable for colorectalcancer. However, the interactive effect of total number of lymph nodes examined (TNLE)and the number of metastatic lymph nodes (NMLN) on survival has not been wellcharacterized.
STUDY DESIGN: Patients operated on for colon cancer between 1998 and 2007 were identified from theSurveillance, Epidemiology, and End Results database (n ¼ 154,208) and randomly dividedinto development (75%) and validation (25%) datasets. The association of the TNLE andNMLN on survival was assessed using the Cox proportional hazards model with terms forinteraction and nonlinearity with restricted cubic spline functions. Findings were confirmedin the validation dataset.
RESULTS: Both TNLE and NMLN were nonlinearly associated with survival. Patients with no lymphnode metastasis had a decrease in the risk of death for each lymph node examined up toapproximately 25 lymph nodes, while the effect of TNLE was negligible after approximately10 negative lymph nodes (NNLN) in those with lymph node metastasis. The hazard ratiovaried considerably according to the TNLE for a given LNR when LNR � 0.5, rangingfrom 2.88 to 7.16 in those with an LNR ¼ 1. The independent effects of NMLN andNNLN on survival were summarized in a model-based score, the N score. When patientsin the validation set were categorized according to the N stage, the LNR, and the N score,only the N score was unaffected by differences in the TNLE.
CONCLUSIONS: The effect of the TNLE on survival does not have a unique, strong threshold (ie, 12 lymphnodes). The combined effect of NMLN and TNLE is complex and is not appropriately rep-resented by the LNR. The N score may be an alternative to the N stage for prognostication ofpatients with colon cancer because it accounts for differences in nodal samples. (J Am CollSurg 2013;217:1090e1100. � 2013 by the American College of Surgeons)
Evaluation of an increasing number of lymph nodes (LN)has been shown to be associated with improved survivalafter resection of colon cancer.1-3 Currently, it is generally
accepted that at least 12 LN need to be evaluated in orderto accurately assign the “true” nodal status of patientswith colon cancer. This recommendation, initially madein 1991 by the working committee on staging for colo-rectal cancer of the World Congress of Gastroenterology,Digestive Endoscopy and Coloproctology,4 was based onthe recognition that a higher number of LNs examinedresulted in a higher proportion of patients with LNmetastasis.5-7 The 12 LN recommendation has sincebeen adopted by both the National Cancer Instituteand the National Quality Forum.8 Establishment of anLN “threshold” aims to prevent inadequate samplingand understaging, which are associated with worsesurvival due to stage migration and inappropriate omis-sion of adjuvant chemotherapy.9 Interestingly, more
CME questions for this article available athttp://jacscme.facs.org
Disclosure Information: Authors have nothing to disclose. Timothy J Eberlein,Editor-in-Chief, has nothing to disclose.
Received April 12, 2013; Revised July 16, 2013; Accepted July 29, 2013.From the Department of Surgery, St Louis University School of Medicine,St Louis, MO (Gleisner, Mogal) and The Johns Hopkins University Schoolof Medicine, Baltimore, MD (Dodson, Efron, Gearhart, Wick, Lidor,Herman, Pawlik).Correspondence address: Timothy M Pawlik, MD, MPH, PhD, FACS,Department of Surgery, Blalock 688, 600 N Wolfe St, Baltimore,MD 21287. email: [email protected]
1090ª 2013 by the American College of Surgeons ISSN 1072-7515/13/$36.00
Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jamcollsurg.2013.07.404

recently, several other studies have suggested that inde-pendent of LN metastatic status, a higher number ofLNs examined is associated with survivalda findingthat cannot be attributable to understaging.10,11 Othermechanisms, such as differences in quality of care, patientcharacteristics, and tumor biology, have been suggested toexplain these findings.12,13
Some investigators have questioned the use of 12 as anarbitrary cut-off value for the number of LNs examined.These authors have demonstrated an association betweensurvival and the number of nodes examined ranging from6 to 18.3 However, the actual shape of this associationand its interaction with the number of metastatic lymphnodes (NMLN), which could suggest a strong thresholdeffect and consequently the more appropriate cutoff, havenot been characterized. More recently, other groups haveproposed the use of lymph node ratio (LNR) as a betterindicator of prognosis rather than simply the number ofmetastatic LNs.14-18 Lymph node ratio is defined by theratio of metastatic LNs relative to number of nodes exam-ined. The assumption is that LNR accounts for both inad-equate nodal sampling (ie, the denominator), as well as thefact that prognosis worsens with more metastatic LNs (ie,the numerator). In turn, higher weight is given to an LNmetastasis in instances when fewer overall LNs are exam-ined. Lymph node ratio also assumes that the risk of deathis influenced the same waydalbeit inverselydby theNMLN as by the total number of lymph nodes examined(TNLE). Although such an assumptionmay be reasonable,to our knowledge, this assumption has not been formallytested. The lack of methodologic data regarding the under-pinnings of LNR and its true added prognostic valuecompared with LN status alone is important becauseLNRhas been increasingly proposed as the optimalmannerto stage patients with various malignancies.19-21
The purpose of this study was to define the associationof the TNLE and survival among patients undergoingsurgical resection of adenocarcinoma of the colon. Wecharacterized graphically the nature of the associationand, in turn, quantitatively delineated the relationship.In addition, we determined how the NMLN affects thisassociation. Finally, we identified how the relationship
between these variables affects the prognostic significanceof the N stage and the LNR and suggest a new prognostic“N score” based on this observed relationship.
METHODSUsing data from the 1998 to 2007 Surveillance, Epidemi-ology, and End Results (SEER) database, patients withadenocarcinoma of the colon who underwent resectionwere identified. The SEER database collects data from13 regional cancer registries covering 26% of the US pop-ulation. Follow-up information is updated annually byeach registry; data are de-identified before they becomeavailable for further analysis. Patients with a previousdiagnosis of cancer, no information regarding theTNLE or NMLN, and those patients with distant meta-static disease were excluded from the analysis.The patient data were randomly divided into a develop-
ment (75%) and a validation (25%) dataset. The develop-ment dataset was used initially to determine the bestmodel for the data and to define the shape of the associ-ation between NMLN and TNLE. Demographic andclinical variables for each sample were summarized andcompared. Proportions were used to describe categoricalvariables. Mean and standard deviation were used forcontinuous variables that were normally distributed;median and range were computed otherwise. Univariateanalysis of survival was performed using the Kaplan-Meier method.Demographic and clinical variables including age, race,
sex, tumor size, T category, site, and histologic differenti-ation were recorded. Differences in survival werecompared with the log-rank test; multivariable analysisused the Cox proportional hazards model. Proportionalityof hazards was verified for continuous variables dividedinto quartiles as well as for categorical variables. Restrictedcubic spline functions were used to characterize the associ-ation between continuous variables and the risk of death.Splines are used when modeling a relationship betweena continuous variable and an outcome that could benonlinear. In brief, a spline is a smoothed polynomialfunction that is piecewise defined and where these “pieces”blend smoothly at the “knots” where the polynomial piecesconnect. In order to determine the best model to describethe shape of the association between TNLE, NMLN, andsurvival, multiple models were compared. The first model(basic model) included clinic and demographic variables,as well as TNLE and NMLN as continuous (linear) vari-ables. The second model included restricted cubic splineswith 4 “knots” placed at 2, 10, 16, and 33 for TNLE,which corresponded to the 5th, 35th, 65th, and 95th percen-tiles, respectively; 3 “knots” were placed at 2, 8, and 12 for
Abbreviations and Acronyms
AIC ¼ Akaike’s information criteriaHR ¼ hazard ratioLN ¼ lymph nodeLNR ¼ lymph node ratioNMLN ¼ number of metastatic lymph nodesNNLN ¼ number of negative lymph nodesTNLE ¼ total number of lymph nodes examined
Vol. 217, No. 6, December 2013 Gleisner et al Lymph Node Ratio 1091

NMLN, corresponding to the 50th, 90th, and 95th percen-tiles to model for nonlinearity. Model 3 additionally eval-uated the presence of a multiplicative linear interactionbetween the 2 explanatory variables (ie, TNLE, NMLN);models 4 and 5 evaluated for a nonlinear interaction ofTNLE and NMLN, respectively. Finally, model 6 (fullmodel) included a product of each of the restricted cubicspline functions for TNLE and each of the restricted cubicsplines functions for NMLN in order to model fora nonlinear interaction between both variables. Themodels were compared using 3 criteria: the likelihood ratiotest, the c-statistic, and the Akaike’s information criteria(AIC). The likelihood ratio test was used to evaluate themodel fit, whereas the c-statistic was used to assess prog-nostic discrimination.22 The AIC measured fit andcomplexity, with low AIC values reflecting a model withboth a better fit and lower complexity.22 Using thesecriteria, the best adjusted model to describe the associationbetween TNLE and NMLN with the risk of death wasdetermined. Estimated hazard ratios (HR) based on the“best” model were compared using TNLE for fixed valuesof NMLN and for fixed values of LNR to compare graph-ically the variability of the estimated HR within levels ofeach of these 2 variables.After identification of the “best” model using the devel-
opment dataset, the validation cohort was used to confirmthe fit and accuracy of the proposed model. UnadjustedKaplan-Meier survival estimates were calculated andcompared with the predicted values.
RESULTS
Patient characteristics and impact on overallsurvival
A total of 154,208 patients were included in the analysis;115,656 (75%) patients were in the development subsetand 38,552 (25%) were in the validation sample. Mostpatients had T3 lesions (56.4%), and a right hemicolec-tomy was the operation performed most often (42.3%);roughly one-third of patients (33.8%) had at least 1lymph node metastasis. The mean TNLE and NMLNwere comparable in the development vs the validationsamples (TNLE: development, 14.5 SD � 10.1 vs valida-tion, 14.4 SD � 9.9; NLMN: development, 3.7 SD �3.9 vs validation, 3.7 SD � 3.8) (Table 1). The majorityof patients in both the development and validation data-sets had an LNR � 0.50 (development, 81.2% vs valida-tion, 81.1%).The median, 3-, and 5-year survivals were 108 months,
76.3%, and 65.7% respectively. Several factors were asso-ciated with survival (Table 2). Since 2000, there was a 1%yearly decline in the long-term risk of death after
operation for nonmetastatic colon cancer (HR 0.98,95% CI 0.98 to 0.99). Both female patients (HR 0.90,95% CI 0.87 to 0.93) and Asian patients (referent, whitepatients: HR 0.87, 95% CI 0.81 to 0.93) had animproved overall survival. Age was also associated withlong-term survival, with a 4% decrease in survival peryear �60 years (HR 1.04, 95% CI 1.04 to 1.04). Patientswith a T3 tumor had a 3-fold increase in the risk of death(HR 2.83; 95% CI 2.65 to 3.03); patients with T4tumors had a nearly 6-fold increased risk (referent, T1tumors: HR 5.69; 95% CI 5.30 to 6.10). Tumor sizewas associated with survival as well, even when correctedfor T stage (HR 1.05, 95% CI 1.03 to 1.06 for eachcentimeter up to 5 cm and HR 1.01, 95% CI 1.01 to1.02 for each centimeter above 5 cm). Similarly, histo-logic grade was associated with survival, with undifferen-tiated tumors having a worse prognosis (HR 1.46, 95%CI 1.30 to 1.64) compared with tumors that were welldifferentiated.
Impact of total number of lymph nodes examinedand number of metastatic lymph nodes on risk ofdeath: lymph node ratio as ideal prognosticstrategy?
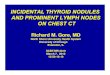
Both TNLE and NMLN were associated with long-termoutcomes. Specifically, TNLE was associated witha nonlinear decrease in the risk of death; NMLN wasassociated with a nonlinear increase risk of death(Fig. 1). Among patients with no lymph node metastasis,the risk of death decreased considerably for each negativenode up to 20 to 25 lymph nodes examined. The effect ofeach additional node examined on survival was negligibleafter 25 TNLE. Among patients with lymph node metas-tasis, the risk of death increased with the NLMN, inde-pendent of TNLE. When the TNLE was low (ie, lessthan 10 to 15), however, the risk of death was higherthan predicted by the independent effects of eitherTNLE or NLMN. As such, there appeared to bea more complex interaction between these variables, espe-cially at low TNLE counts (Fig. 1B).Various models were constructed to determine the
most parsimonious model that had the best fit to predictsurvival (Table 3). In comparing the various survivalmodels, model 4 was the most optimal based on theAIC. Model 4 accounted for both the nonlinearity ofthe effect between TNLE and NMLN, as well as theinteraction between these 2 predictive variables. Model4 also had the best fit, as well as better agreement betweenpredicted and observed values when compared witha simpler model 3 (likelihood-ratio test’s chi-square ¼24.24, p < 0.001). The complexity caused by inclusionof nonlinear parameters for interaction between TNLE
1092 Gleisner et al Lymph Node Ratio J Am Coll Surg

and NMLN was well compensated by the improvementin model adequacy (AIC 777661 vs AIC 777681, formodel 4 and model 3, respectively).The interaction between TNLE and NMLN was
further explored by defining the HR of death associated
with TNLE at 4 fixed NMLN “knots” placed at 2, 5,8, and 12, corresponding to the 50th, 75th, 90th, and95th percentiles (Fig. 2A). An increase in the HR forany NMLN “knot” was noted as the TNLE decreased,with the hazards overlapping between the different
Table 1. Patient and Tumor Characteristics for Populations in the Development and Validation Samples (n ¼ 154,208)
Characteristic Development sample Validation sample
n (%) 115,656 (75.0) 38,552 (25.0)
Age, y, mean (SD) 68.8 (13.3) 68.8 (13.2)
Sex, n (%)
Male 55,189 (47.7) 18,620 (48.3)
Female 60,467 (52.3) 19,932 (51.7)
Race, n (%)
White 94,285 (81.5) 31,492 (81.7)
Black 12,525 (10.8) 4,110 (10.7)
Asian 7,972 (6.9) 2,656 (6.9)
Other 874 (0.8) 294 (0.8)
Year of diagnosis, n (%)
1998 to 2003 52,230 (45.2) 17,684 (45.9)
2004 to 2009 63,426 (54.8) 20,868 (54.1)
Tumor site, n (%)
Cecum 27,756 (24.0) 9,114 (23.6)
Appendix 1,216 (1.1) 397 (1.0)
Ascending colon 22,890 (19.8) 7,687 (19.9)
Hepatic flexure 6,507 (5.6) 2,107 (5.5)
Transverse colon 10,513 (9.1) 3,580 (9.3)
Splenic flexure 4,319 (3.7) 1,438 (3.7)
Descending colon 6,861 (5.9) 2,268 (5.9)
Sigmoid colon 33,622 (29.1) 11,321 (29.4)
Not specified 1,972 (1.7) 640 (1.7)
Tumor size, cm, mean (SD) 4.8 (3.0) 4.8 (3.1)
T stage, n (%)
T1 18,670 (16.1) 6,214 (16.1)
T2 17,939 (15.5) 5,858 (15.2)
T3 65,183 (56.4) 21,828 (56.6)
T4 13,864 (12.0) 4,652 (12.1)
N stage, n (%)
N0 76,635 (66.3) 25,237 (65.5)
N1 25,527 (22.1) 8,785 (22.8)
N2 13,494 (11.7) 4,530 (11.8)
Nodes examined, n, mean (SD) 14.5 (10.1) 14.4 (9.9)
Positive nodes, n, mean (SD) 3.7 (3.9) 3.7 (3.8)
Lymph node ratio, median (IQR) 0.19 (0.09e0.39) 0.19 (0.09e0.38)
Histologic grade, n (%)
Well differentiated 11,350 (9.8) 3,755 (9.7)
Moderately differentiated 77,701 (67.2) 25,797 (66.9)
Poorly differentiated 19,917 (17.2) 6,667 (17.3)
Undifferentiated 1,165 (1.0) 380 (1.0)
Unknown 5,523 (4.8) 1,953 (5.1)
Vol. 217, No. 6, December 2013 Gleisner et al Lymph Node Ratio 1093

categories. For example, among patients with an NMLNof 5, the estimated HR of death was 2.29 (95% CI 1.90to 2.75) when TNLE was 20 nodes vs 3.25 (95% CI 2.73
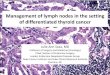
to 3.86) when TNLE was 10 vs 4.61 (95% CI 3.88 to5.51) when TNLE was 5. Similarly, heterogeneity wasnoted when analyzing different LNR groups. Althoughthe HR of death was relatively constant for patientswith an LNR ranging from 0.10 to 0.25, there wasconsiderable variation in the HR when the LNR was>0.50. Specifically, among patients with an LNR of0.5, the HR of death varied from 2.70 (95% CI 2.17to 3.38) when 1 of 2 nodes had metastatic disease vs anHR of 3.66 (95% CI 3.00 to 4.46) when 10 of 20 nodeshad metastases. Furthermore, among patients with anLNR of 1.0, there was even greater variation; the HRranged from 2.88 (95% CI 2.27 to 3.64) for those with1 of 1 node involved with metastatic disease to 7.16(95% CI 5.60 to 9.16) for patients with 20 of 20 nodesinvolved.For the TNLE, we couldn’t identify a specific cut-off
value after which there was minimal variation in theHR for a given NMLN. Instead, the TNLE cutoffincreased as the NMLN increased until plateauing.However, when the number of “negative” lymph nodeswas used as an alternative, the impact on survival wasfairly constant. After 10 to 12 “negative” lymph nodes(NNLN) were identified in the specimen, the effect ofany additional “negative” nodes (and therefore a higherTNLE) had no effect on the underlying hazard of death(Fig. 2B). In fact, when NNLN was included in a multi-variable model instead of TNLE, there was no significantinteraction with the NMLN. Still, in this simplifiedmodel (model 7), the estimates were similar to model4, which was the TNLE model with the best fit(Table 3). Based on model 7, an “N” score could bederived to account for both the contribution of theNMLN and the NNLN to the risk of death amongpatients with stage III colon cancer. This score used thecoefficients for the variables related to the NMLN andthe NNLN that were significantly associated withsurvival:
N score ¼ NMLN � 10�NNLN
� 10þ 0:05� ðNNLN � 10Þ2 þ 0:2
� ð10 < NMLN� 10 < NNLN � 25Þ
Performance of N score in validation subset
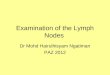
Survival of patients in the validation set was stratified bythe American Joint Committee on Cancer N categories,which are based on the presence or absence of metastaticlymph nodes (ie, N0 vs N1). There was heterogeneityamong patients within all N stage categories. Patientswho had NNLN � 3 had a worse prognosis comparedwith patients who had NNLN > 10, with differences
Table 2. Hazard Ratio for Long-Term Survival after Colec-tomy for Colon Cancer According to Multivariable ModelDerived from the Development Sample
VariableHazard ratio(95% CI)* p Value
Age, per year
Up to 60-y-old 1.00 (1.00e1.00) 0.479
Older than 60-y-old 1.04 (1.04e1.04) <0.001
Sex
Male Referent
Female 0.90 (0.87e0.93) <0.001
Race
White Referent
Black 1.34 (1.28e1.41) <0.001
Asian 0.87 (0.81e0.93) <0.001
Other 0.77 (0.63e0.95) 0.012
Year of diagnosis, per year
1998 Referent
1999 1.03 (0.99e1.07) 0.108
After 1999 0.98 (0.98e0.99) <0.001
Tumor site
Cecum Referent
Appendix 1.33 (1.19e1.50) <0.001
Ascending colon 0.98 (0.94e1.01) 0.238
Hepatic flexure 1.08 (1.02e1.14) 0.009
Transverse colon 0.99 (0.95e1.04) 0.697
Splenic flexure 1.07 (1.01e1.14) 0.030
Descending colon 1.00 (0.94e1.05) 0.863
Sigmoid colon 0.94 (0.91e0.98) 0.001
Not specified 1.15 (1.05e1.25) 0.002
Tumor size, per cm
� 5 cm 1.05 (1.03e1.06) <0.001
> 5 cm 1.01 (1.01e1.02) <0.001
Unknown 1.38 (1.29e1.47) <0.001
T stage
T1 Referent
T2 1.47 (1.36e1.59) <0.001
T3 2.83 (2.65e3.03) <0.001
T4 5.69 (5.30e6.10) <0.001
Histologic grade
Well differentiated Referent
Moderately differentiated 1.13 (1.07e1.18) <0.001
Poorly differentiated 1.31 (1.24e1.39) <0.001
Undifferentiated 1.46 (1.30e1.64) <0.001
Unknown 1.11 (1.02e1.21) 0.018
*Adjusted for all variables shown as well as registry. Cut point for age, yearof diagnosis, and tumor size was based on the shape of the association ofeach variable and survival on univariable analysis.
1094 Gleisner et al Lymph Node Ratio J Am Coll Surg

in survival within the same N category ranging from7.6% to 23.6% at 5 years and 7.0% to 19.0% at 10 years(Fig. 3).Survival in patients with stage III colon cancer was also
examined according to different nodal sampling sizes (ie,TNLE < 12 and TNLE � 12) stratified by N1 vs N2disease (Fig. 4A). Survival estimates according to N statuswere generally better for those with TNLE � 12,
supporting the notion that classification based on the Nstage can be inaccurate in the presence of smaller samples.Survival estimates were then also assessed according toLNR stratified by TNLE < 12 and TNLE � 12(Fig. 4B). Although LNR had prognostic impact in boththe low and high TNLE groups, there were importantdifferences in these subgroups. Specifically, when theLNR was low (ie, 0.10 and 0.20), the estimated survival
Table 3. Characteristics of the Models Describing the Relationship Between the Total Number of Lymph Nodes Examined,the Number of Positive Nodes, and Mortality after Resected Colon Cancer, Adjusted for Other Clinical and DemographicVariables
Model Log-likelihood df chi-square* p Value AIC C-statistic
1- Clinical and demographicvariables þ TNLE linear þNMLN linear �389023.6 45 778137.3 0.724 (0.721e0.726)
2- Model 1þ TNLE RCS(4 knots) þ NMLN RCS(3 knots) �388806.6 51 434.12 <0.00001 777715.2 0.729 (0.726e0.731)
3- Model 2 þ TNLE linear xNMLN linear �388788.6 52 36.05 <0.00001 777681.1 0.730 (0.728e0.733)
4- Model 3 þ TNLE RCS xNMLN linear �388776.4 54 24.24 <0.00001 777660.9 0.730 (0.728e0.733)
5- Model 3 þ NMLN RCS xTNLE linear �388784.8 53 7.57 0.006 777675.5 0.730 (0.728e0.733)
6- Model 4 þ NMLN RCS xTNLE linear þ NMLN RCS xTNLE RCS �388774.9 57 3.09 0.3779 777663.8 0.730 (0.728e0.733)
7- Model 1 þ NMLN �10 þNMLN >10 þ NNLN�10 þNNLN�10*NNLN�10 þ 25>NNLN>10 �388778.9 52 777661.9 0.730 (0.728e0.733)
Clinical and demographic variables included: age, sex, race, year of diagnosis, tumor site, tumor size, T stage, histologic grade, and registry.*Likelihood ratio test: model 2 vs 1; model 3 vs 2; models 4 and 5 vs 3; model 6 vs model 4.AIC, Akaike information criterion; df, degrees of freedom; NMLN, number of positive lymph nodes; NNLN, number of negative lymph nodes; RCS,restricted cubic splines; TNLE, total number of lymph nodes examined.
Figure 1. Predicted risk of death (hazard ratio) according to the total number of lymph nodes examined and the number of metastatic lymphnodes, adjusted for other risk factors. (A) A simpler model accounted for nonlinearity with the inclusion of restricted cubic splines for the totalnodes examined (3 knots) and the positive nodes (4 knots). (B) The best-fitted model accounted for the presence of interaction between the 2variables in addition to nonlinearity. *Adjusted by age, sex, race, year of diagnosis, tumor site, tumor size, T stage, histologic grade, andregistry.
Vol. 217, No. 6, December 2013 Gleisner et al Lymph Node Ratio 1095

was similar for those with TNLE < 12 vs TNLE � 12.However, when the LNR was high (ie, 0.50 and 1.0),survival was worse among patients with TNLE � 12.These findings were compatible with the previous findingsfrom model 4, which showed an increasing HR withincreasing TNLE for those patients with LNR > 0.50
(Fig. 2). Last, survival estimates were compared accordingto the N score (Fig. 4C). Differently than the N stage andthe LNR, the N score provided prognostication that wasindependent of the TNLE. The model used to determinethe N score in the development set had good performancein the validation set (Figs. 4C and 5), resulting in an excel-lent agreement between observed and predicted 5-yearsurvival (correlation coefficient 0.99).
DISCUSSIONThe assessment of lymph nodes around the time ofsurgery for colorectal cancer has important staging, prog-nostic, and therapeutic implications. Multiple random-ized clinical trials have demonstrated the survival benefitof adjuvant systemic chemotherapy for stage III patientswith colorectal cancer.23 As such, accurate assessment ofLN status has been a major focus of consensus guidelines,as well as quality outcomes initiatives for colorectalsurgery.8,24 Although data on LN metastasis have tradi-tionally been reported either as a binary outcome (N0vs N1) or as the absolute number of metastatic LNs,more recently, LNR has been proposed as a superiormeans to report LN status.14-18 Our group and othershave argued that LNR is more accurate because it takesinto account both the TNLE and the NMLNdeach ofwhich has been shown to be important.3,25,26 Previousstudies on LNR, however, have failed to adequately char-acterize the complex relationship between the TNLE andNMLN and its impact on survival after resection of coloncancer. Specifically, given that NMLN and TNLE are notindependent variables because the chance of finding an
print&web4C=FPO
Figure 3. Unadjusted Kaplan-Meier survival estimates for patientswith stage III colon cancer in the validation sample according to theAmerican Joint Committee on Cancer N stage and the number ofnegative nodes (NNLN); NNLN � 3, solid line vs NNLN> 10, dashedline. Survival time measured from date of surgery.
Figure 2. Hazard ratio according to the number of total lymph nodes examined (TNLE) for different numbers of metastatic lymph nodes (solidlines) and for different lymph node ratios (LNR) (dashed lines). The hazard ratio markedly increases for the number of total lymph nodesexamined from <10 to 20 nodes among patients with the same number of metastatic lymph nodes; the cutoff increases as the numbers ofmetastatic lymph nodes increase. (A) The hazard ratio also varies considerably for a given LNR, especially for LNR >50%, and increases asthe number of total lymph nodes examined increases. (B) Hazard ratio plotted according to the number of negative nodes. The hazard ratiomarkedly increases when �10 negative lymph nodes are identified, regardless of the numbers of metastatic lymph nodes.
1096 Gleisner et al Lymph Node Ratio J Am Coll Surg

LN metastasis is dependent to some degree on TNLE,more sophisticated statistical methodology is needed toexamine the relationship between these 2 variables.Because of this, previous studies may have overestimatednot only the “value added” of LNR, but also underappre-ciated the prognostic heterogeneity within similar LNRcategories. This study is important because we examinedmore rigorously the impact of TNLE, NMLN, and LNRon survival after colon resection. To do this, we evaluatedvarious statistical models that treated both TNLE andNMLN as continuous variables and included terms inthe models to assess for nonlinearity and interaction.Given that such modeling strategies require large samplesizes, we chose to take advantage of the SEER database.We confirmed previously published data noting that
a lower TNLE was associated with an increased risk ofdeath. The association between the TNLE and survivalhad been previously described using categorical cutoffvalues that varied from 6 to 18 nodes, and mostcommonly 12.3 Unlike other studies, our study alsoexamined TNLE as a continuous variable and stratifiedthe analysis based on LN status (ie, N0 vs N1 vs N2).By adopting this approach, we gained additional informa-tion provided through evaluation of the actual shape ofthe association, which, in turn, improved the availableprognostic information while also reducing confound-ing.27,28 In adopting this approach, we noted that the
prognostic impact of TNLE differed according towhether the patient had LN metastasis or not. Specifi-cally, although patients with no lymph metastasis hada decrease in the risk of death for each additional LNexamined up to a total of 25, the effect of TNLE variedaccording to the NMLN among patients with lymphnode metastasis. However, when TNLE was substitutedfor NNLN, the effect on survival was independent ofthe NMLN, with a decrease in the risk of death foreach additional negative LN found up to 10 negativeLNs, after which the effect was negligible. These findingsconfirm and further characterize the previously reportedindependent effect of the NNLN on survival of patientswith colon cancer.29 The reason for the difference inhow TNLE affects prognosis among N0 vs patientswith LN metastasis is probably multifactorial. Scott andGrace7 reported that >90% patients with nodal metas-tases were found to have at least 1 LN metastasis after13 LNs were evaluated.7 Baxter and colleagues11 similarlyreported that the odds of identifying an LN metastasisincreased when up to 13 LNs were examined, but actuallydeclined after that. Our data expand on this past workand demonstrate that the impact of TNLE on prognosisis not constant, but rather varies based on underlying LNstatus. Our data therefore suggest that different TNLE“targets” may be warranted in patients with and withoutLN metastasis.
Figure 4. Unadjusted Kaplan-Meier survival estimates for patients with stage III colon cancer in the validation sample according to the nodalsample size (total number of lymph nodes examined [TNLE] < 12, gray line vs TNLE � 12, black line) and stratified by the (A) American JointCommittee on Cancer N stage, (B) the lymph node ratio (LNR), and (C) by the N score (*predicted, based on the number of positive andnegative lymph nodes, adjusted for other clinical and demographic variables [model 7]). The predicted survival function according to the Nscore is also shown (dashed). Survival was consistently lower for patients with TNLE < 12 when categorized by the N stage and independentof the TNLE when categorized by the N score. Although survival was similar regardless of the TNLE when the LNR was low, it was markedlyworse for those with “adequate sample size” and LNR of 50% to 100%.
Vol. 217, No. 6, December 2013 Gleisner et al Lymph Node Ratio 1097

Perhaps more interestingly, we noted significantheterogeneity in the hazard of death for patients withcomparable LNR. The LNR has recently been proposedas a better predictor of survival after surgery for severaldifferent gastrointestinal malignancies.14-18 By takinginto account information on both TNLE and NMLN,LNR has been argued to be a “better” prognostic markerthan either TNLE or NMLN alone. In addition, previousinvestigators have argued that by combining TNLE andNMLN into a composite ratio, patients with similarlong-term prognosis can be grouped more accuratelyand homogeneously.14-18 In fact, based on the differencesseen in survival among patients stratified by LNR, theincorporation of LNR into the American JointCommittee on Cancer TNM staging system has beensuggested.18 This study is important because it demon-strates that LNR may not accurately categorize patientsinto homogeneous risk groups. Rather, we found thatsignificant heterogeneity can exist among patients catego-rized into any one LNR. Although LNR may account fordifferences in the nodal sample size when NMLN is lowrelative to TNLE (ie, low LNRs), significant bias mayexist at higher LNRs (ie, LNR 0.50 to 1.00). Specifically,we showed that survival of patients within the same LNRis worse for patients with larger, “more adequate” samplesizes, or higher TNLE. In fact, we quantified this vari-ability and showed that the hazard of death can vary by
more than 3-fold within the same LNR. Given thatLNR is a direct function of TNLE and NMLN, andgiven that TNLE is independently associated with animproved survival, the worse survival of patients witha high LNR is most likely explained by the excessmortality risk associated with NMLN. For example, forpatients with LNR ¼ 1.0, those patients included inthe low TNLE group (ie, “inadequate sampling”), allwill have fewer than 12 NMLN (range 1 NMLN/1TNLE to 11 NMLN/11 TNLE); in contrast, patientswith LNR ¼ 1.0 in the high TNLE group (ie, “adequatesampling”) will all by definition have more than 12NMLN, thereby helping to explain why patients withLNR ¼ 1.0 and TNLE � 12 had a worse prognosis.Collectively, these data suggest that the LNR does notproperly represent the prognostic significance of theNMLN relative to TNLE among patients with stage IIIcolon cancer.In an attempt to identify a more accurate tool to define
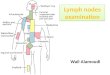
the impact of lymph node status and TNLE on overallsurvival, we constructed a model-based score taking intoaccount the complex, nonlinear, independent relationshipbetween TNLE and NMLN and survival. The “N score”was developed based on empirical data using a “develop-ment” subset of the data. The N score should thereforeprovide more accurate prognostic information. We vali-dated the N score in a “validation” subset of the data.Importantly, when we evaluated performance of the Nscore in the validation subset we found that the accuracywas excellent. Although survival predictions variedconsiderably based on LNR relative to TNLE, the Nscore accurately predicted survival when compared withactual observed survival (correlation coefficient of 0.99).As such, although not as intuitive or “simple” as LNR,the N score may be a more accurate tool to predictsurvival, as well as a better mechanism to categorizepatients into more homogeneous prognostic groups aftersurgery for colon adenocarcinoma. In order to facilitateits clinical use, the N score could also be further simpli-fied, in a trade-off between utility and precision. As anexample, the contribution of more than 10 NMLNand/or NNLN could be excluded because this corre-sponds to a small proportion of the observations.Our study has several limitations. Because the SEER
database does not provide information on disease-freesurvival, results were reported based on overall survivalonly. In addition, previous studies have shown that age,tumor size, and T stage can be associated withTNLE.30,31 To account for this, we adjusted for thesefactors in our multivariable models that assessed theimpact of TNLE and NMLN on survival. Despite doingthis, residual confounding may exist. For example, other
Figure 5. Observed 5-year survival rate vs expected 5-year survivalrate as predicted by the N score model (model 7) in the validationcohort, showing adequate concordance (r ¼ 0.99). Each dotrepresents 1/30th of the data. *Based on the N score model(model 7), which included the number of positive and negativelymph nodes, adjusted for other clinical and demographic variables.Hazard function ¼ clinical and demographic variables þ NMLN�10þNMLN >10 þ NNLN �10 þ NNLN �10 d NNLN �10 þ25>NNLN>10. NMLN, number of metastatic lymph nodes; NNLN,number of negative nodes.
1098 Gleisner et al Lymph Node Ratio J Am Coll Surg

unmeasured factors associated with “tumor biology” mayhave influenced differences in survival associated withTNLE. For example, DNA microsatellite instability hasbeen associated with higher retrieval of LNs.32,33 Highernumbers of LNs in such cases may be related to an activeimmune response to tumor antigens, which could resultin improved survival.34 Finally, TNLE may have beenassociated with some “nonbiologic” factor that mighthave influenced outcomes. For example, higher TNLEcould be a marker of higher adherence to practice guide-lines and better overall care, although recent studies wereunable to confirm this association.12,35 Retrieval andcounting of LNs is also not standardized among differentinstitutions. Fat clearing can increase the yield of LNsretrieved, but is labor intensive. The definition ofa “countable” LN also varies among pathologists, withdiscrepancies on reporting nonpalpable nodes seen onlyon microscopic evaluation and the requirement ofa capsule for lymphoid aggregates to be counted asLNs. Because we do not have information on thedifferent reasons for the variation in the LN yield amongpatients, we cannot make inferences on the decision touse a minimal of 12 TNLE as a quality of care measure-ment. The decision to choose 12 TNLE as a cutoff foradequate sampling was largely aimed at minimizingunderstaging and differences in survival exclusively basedon stage migration from N0 to N1. Therefore, as a qualityof care measurement, it largely applies to those patientswith no LN metastasis. In turn, TNLE may be a betterquality measurement for institutions rather than for indi-vidual patients. As a prognostic factor, the effect of theTNLE on survival had no strong threshold that suggestsa natural cutoff. Among those with N0 disease, forexample, any arbitrary number between 1 and 25 willdivide these patients into those with a better or worseprognosis, provided there are enough patients in eachgroup. Rather than using a unique cutoff and dichotomi-zation, categorization into 3 or more groups of NNLNexamined or the use of a summarizing variable such asthe N score would be more appropriate for prognostica-tion related to the TNLE.
CONCLUSIONSIn conclusion, although TNLE was associated with long-term survival, the effect of TNLE was different accordingto the presence of metastatic LNs. Patients with no lymphmetastasis had a decrease in the risk of death for each addi-tional LN examined up to a total of 25; the effect of TNLEwas negligible after 10 negative LNs were identified amongpatients with LN metastasis. Perhaps more interestingly,we also demonstrated that LNR does not appropriately
represent the relationship between the TNLE, NMLN,and survival. In fact, patients in the same LNR categorycould have a hazard of death that varied up to 3-fold. Assuch, data presented herein seriously call into questionthe adoption of LNR as a universal means to stratifypatients with regard to LN status. Rather, the proposedN score model, while not as simple, takes into accountthe complex relationship of TNLE and NMLN and, inturn, may better predict survival among patients aftersurgery for colon adenocarcinoma.
Author Contributions
Study conception and design: Gleisner, PawlikAcquisition of data: Gleisner, PawlikAnalysis and interpretation of data: Gleisner, Mogal,Dodson, Efron, Gearhart, Wick, Lidor, Herman,Pawlik
Drafting of manuscript: Gleisner, PawlikCritical revision: Gleisner, Mogal, Dodson, Efron,Gearhart, Wick, Lidor, Herman, Pawlik
REFERENCES
1. Mammen JM, James LE, Molloy M, et al. The relationship oflymph node dissection and colon cancer survival in theVeterans Affairs Central Cancer Registry. Am J Surg 2007;194:349e354.
2. Moore J, Hyman N, Callas P, et al. Staging error does notexplain the relationship between the number of lymph nodesin a colon cancer specimen and survival. Surgery 2010;147:358e365.
3. Chang GJ, Rodriguez-Bigas MA, Skibber JM, et al. Lymphnode evaluation and survival after curative resection of coloncancer: systematic review. J Natl Cancer Inst 2007;99:433e441.
4. Fielding LP, Arsenault PA, Chapuis PH, et al. Clinicopatholog-ical staging for colorectal cancer: an International Documenta-tion System (IDS) and an International ComprehensiveAnatomical Terminology (ICAT). J Gastroenterol Hepatol1991;6:325e344.
5. Pickren JW. Current concepts in cancer. Nodal clearance anddetection. JAMA 1975;231:969e971.
6. Cawthorn SJ, Gibbs NM, Marks CG. Clearance technique forthe detection of lymph nodes in colorectal cancer. Br J Surg1986;73:58e60.
7. Scott KW, Grace RH. Detection of lymph node metastases incolorectal carcinoma before and after fat clearance. Br J Surg1989;76:1165e1167.
8. Nelson H, Petrelli N, Carlin A, et al. Guidelines 2000 forcolon and rectal cancer surgery. J Natl Cancer Inst 2001;93:583e596.
9. Feinstein AR, Sosin DM, Wells CK. The Will Rogersphenomenon. Stage migration and new diagnostic techniquesas a source of misleading statistics for survival in cancer.N Engl J Med 1985;312:1604e1608.
10. Parsons HM, Tuttle TM, Kuntz KM, et al. Associationbetween lymph node evaluation for colon cancer and nodepositivity over the past 20 years. JAMA 2011;306:1089e1097.
Vol. 217, No. 6, December 2013 Gleisner et al Lymph Node Ratio 1099

11. Baxter NN, Ricciardi R, Simunovic M, et al. An evaluation ofthe relationship between lymph node number and staging inpT3 colon cancer using population-based data. Dis ColonRectum 2010;53:65e70.
12. Parsons HM, Tuttle TM, Kuntz KM, et al. Quality of carealong the cancer continuum: does receiving adequate lymphnode evaluation for colon cancer lead to comprehensive post-surgical care? J Am Coll Surg 2012;215:400e411.
13. Shia J, Wang H, Nash GM, et al. Lymph node staging incolorectal cancer: revisiting the benchmark of at least 12lymph nodes in R0 resection. J Am Coll Surg 2012;214:348e355.
14. Chen SL, Steele SR, Eberhardt J, et al. Lymph node ratio asa quality and prognostic indicator in stage III colon cancer.Ann Surg 2011;253:82e87.
15. Berger AC, Sigurdson ER, LeVoyer T, et al. Colon cancersurvival is associated with decreasing ratio of metastatic toexamined lymph nodes. J Clin Oncol 2005;23:8706e8712.
16. Lee HY, Choi HJ, Park KJ, et al. Prognostic significance ofmetastatic lymph node ratio in node-positive colon carcinoma.Ann Surg Oncol 2007;14:1712e1717.
17. Rosenberg R, Friederichs J, Schuster T, et al. Prognosis ofpatients with colorectal cancer is associated with lymph noderatio: a single-center analysis of 3,026 patients over a 25-yeartime period. Ann Surg 2008;248:968e978.
18. Wang J, Hassett JM, Dayton MT, et al. Lymph node ratio:role in the staging of node-positive colon cancer. Ann SurgOncol 2008;15:1600e1608.
19. Inoue K, Nakane Y, Iiyama H, et al. The superiority of ratio-based lymph node staging in gastric carcinoma. Ann SurgOncol 2002;9:27e34.
20. Kong SH, Lee HJ, Ahn HS, et al. Stage migration effect onsurvival in gastric cancer surgery with extended lymphadenec-tomy: the reappraisal of positive lymph node ratio as a properN-staging. Ann Surg 2012;255:50e58.
21. Wang J, Dang P, Raut CP, et al. Comparison of a lymph noderatio-based staging system with the 7th AJCC System forGastric Cancer: analysis of 18,043 patients from the SEERDatabase. Ann Surg 2012;255:478e485.
22. Collett D. Modelling Survival Data in Medical Research. 2nded. Boca Raton, FL: Chapman & Hall/CRC; 2003.
23. Cunningham D, Atkin W, Lenz HJ, et al. Colorectal cancer.Lancet 2010;375:1030e1047.
24. National Quality Forum Endorsed Commission on CancerMeasures for Quality of Cancer Care for Breast and ColorectalCancers. Available at: http://www.facs.org/cancer/qualitymeasures.html. Accessed February 25, 2013.
25. Cohen AM, Tremiterra S, Candela F, et al. Prognosis of node-positive colon cancer. Cancer 1991;67:1859e1861.
26. Gunderson LL, Jessup JM, Sargent DJ, et al. Revised TN cate-gorization for colon cancer based on national survivaloutcomes data. J Clin Oncol 2010;28:264e271.
27. Desquilbet L, Mariotti F. Dose-response analyses usingrestricted cubic spline functions in public health research.Stat Med 2010;29:1037e1057.
28. Becher H. The concept of residual confounding in regressionmodels and some applications. Stat Med 1992;11:1747e1758.
29. Johnson PM, Porter GA, Ricciardi R, et al. Increasing negativelymph node count is independently associated with improvedlong-term survival in stage IIIB and IIIC colon cancer. J ClinOncol 2006;24:3570e3575.
30. Steele SR, Chen SL, Stojadinovic A, et al. The impact of ageon quality measure adherence in colon cancer. J Am CollSurg 2011;213:95e103; discussion 104e105.
31. Chou JF, Row D, Gonen M, et al. Clinical and pathologicfactors that predict lymph node yield from surgical specimensin colorectal cancer: a population-based study. Cancer 2010;116:2560e2570.
32. Eveno C, Nemeth J, Soliman H, et al. Association betweena high number of isolated lymph nodes in T1 to T4 N0M0colorectal cancer and the microsatellite instability phenotype.Arch Surg 2010;145:12e17.
33. Soreide K, Nedrebo BS, Soreide JA, et al. Lymph node harvestin colon cancer: influence of microsatellite instability andproximal tumor location. World J Surg 2009;33:2695e2703.
34. Schwitalle Y, Kloor M, Eiermann S, et al. Immune responseagainst frameshift-induced neopeptides in HNPCC patientsand healthy HNPCC mutation carriers. Gastroenterology2008;134:988e997.
35. Wong SL, Ji H, Hollenbeck BK, et al. Hospital lymph nodeexamination rates and survival after resection for colon cancer.JAMA 2007;298:2149e2154.
1100 Gleisner et al Lymph Node Ratio J Am Coll Surg