StatePeter
of theM. Som,
ArtMD
Lymph
Nodes
of the
Neck
Index terms: Lymphatic system, CT, 276.1211 . Lymphatic system,
diseases #{149} Lymphatic systern, flow dynamics #{149} Lymphatic
system, MR studies, 276.1214 #{149} Lymphatic system, neoplasms,
276.375 #{149} Neck, neoplasms, 27.37 Radiology 1987;
165:593-600
ciated why? find and, one pose sues
with the worst prognosis and Finally (d), Can the radiologist
the so-called occult primary tumor so, how often and where does
concentrate such a search? The purof this article is to address
these isand answer these questions.
racic duct In adults, and ded neck in fat.
or are
right lymphatic all lymph nodes entirely or in
teleologically
duct (4). in the head part embedthis fat
Although
T
detailed and informed evaluation of the cervical lymph nodes may
represent one of the most challenging problems that a radiologist
faces today. The apparent difficulty of the task arises because
many imagers are unfamiliar with the anatomy of the head and neck
and thus are unsure where to initiate their search for these myriad
nodes. Once a lymph node is identified, the radiologist must then
determine the most accurate nomenclature to use in describing the
findings to the clinician. Just as important, the radiologist must
determine the criteria to be used in evaluating whether a node is
pathologic and also the sensitivity of these criteria. The
importance of clinical correlation and a sense of the impact that
the radiologists findings have on the patients management are often
lost in the pure mechanics of evaluating images. Several questions
that address these issues should be asked during evaluation: (a)
Can the radiologist identify clinically occult nodes and, if so,
how often and what may this mean to patient prognosis and
treatment? (b) What is the impact on patient survival of extranodal
spread, and can it be accurately diagnosed on images? (c) Do
diseased lymph nodes in all of the various anatomic locations of
the neck have the same prognostic significance and, if not, which
nodes are assoHE
HISTORICAL
PERSPECTIVE
Computed tomography (CT) as a diagnostic tool has been
clinically available for just over a decade and has been used
specifically to evaluate cervical lymph nodes only since 1981 (1).
Before that time, the radiologist could offer little effective aid
to the clinician evaluating disease of these nodes. The only
pertinent radiographic examination was lymphangiography, and this
procedure was associated failure, tremely with a high primarily
small frequency due lymphatics in of technical exarea most to
deep-lying, the
may provide a good medium for the smooth and easy motion of the
muscles, vessels, and nerves, it also provides an outlining matrix
for the cervical lymph nodes and allows CT and MR to depict these
nodes well. Only two areas in the head and neck have no direct
lymphatics: (a) The orbit virtually devoid of lymphatics and (b)
muscles do not have lymphatics; rather,their lymph drains in the
fascial planes
is
between vessels
muscles and around that supply them (4).
the
blood
ANATOMY NOMENCLATUREThe classification
AND
of cervical
lymph
nodesdifferent
is complicatedsystems and
by thethe
use of severalloose in-
commonly used for injection of contrast material: the
retroauricular region (2). In addition, these studies were fraught
with interpretive difficulties, primarily relating to the inability
to distinguish malignant nodal from reactive nodal filling defects.
Proximal metastatic nodal disease near the injection site could
prevent visualization of distal lymph nodes. Finally, previous
surgery, disease, or irradiation could alter or disrupt the usual
lymphatic pathways, leading to either a nondiagnostic or a
misleading lymphangiogram (2, 3). With the advent of CT, a
noninvasive modality became available that allowed consistent
identification of most pathologic cervical nodes, and it is not
surprising that cervical lymphangiography has been virtually
abandoned.
rather
termixing lar node5-12). nodes Of in and are system
of specific names for a particufrom one system to another (2,the
the approximately body, about 300 800 lymph are of them
locatedfifth body
in theone-sixth located
neck.in
Thus,of all either
between
onethe
the nodes in side of the (4).
neck,tion
making
developmentvery complex
of a classificadi-
The cervical lymph nodes are often vided into four or five
groups, all ofwhich Most are systems continuous are based with on
each the other. work of
Rouviere sion. Any minology
(8), as is the following alternate, commonly will be pointed
out.
discusused ter-
Rouviere
described
a lymphoid
collar
OVERVIEWIn the overall schematic of the lymphatic system, the
lymphatic vessels commence as lymphatic capillaries in the soft
tissues and extend as a closed system to larger vessels that pass
into lymph nodes. The lymph then passes again in a closed network,
usually to other nodes and then eventually to the neck veins via
the thoracic duct. Thus all lymphatic flow filters through at least
one node, and usually several nodes, before it reaches the tho-
of nodes, the pericervical ring, that encircles the neck at the
junction of the head and neck. The nodes in this collar group
include the occipital, mastoid, parotid, facial, retropharyngeal,
submaxillary, sub-
mental,and ing lateral chains
and
sublingual
nodes.
Anterior
cervical groups are descendthat extend from this collar
From the Departments of Radiology (1234) and Otolaryngology,
Mount Sinai Medical Center, City University of New York, One
Gustave L. Levy P1., New York, NY 10029-6574. Received September 9,
1987; accepted September 14. Address reprint requests to the
author. RSNA, 1987
down along the front and sides of the neck, respectively (Fig.
1) (8). The most clinically important lymph nodes in
theconsideration of head and neck cancer are
the submaxillary, submental, yngeal, and lateral
cervicalfollowing nodal groups. is a brief description
retrophargroups. Theof all the
593
1.
2.
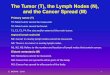
Figures 1, 2. (1) Diagram of the neck in the left anterior
oblique projection with a transverse slice made near the level of
the floor of the mouth or junction of the head and neck. Component
nodes from six cervical chains (occipital, mastoid, parotid,
submaxillary, facial, and submental) form an outer collar of lymph
nodes at this level; these palpable nodes are supplemented by the
more centrally placed retropharyngeal and sublingual nodes.
Descending from this collar are anterior and lateral cervical
groups of nodes. (2) Diagram of the head and neck in the left
anterior oblique projection demonstrates the palpable cervical node
chains and their classic names. Any commonly used alternate names
and the number of nodes in each chain are given in parentheses. The
clinically important retropharyngeal nodes are not illustrated in
this diagram.
The
occipital
nodes
junction
of the
upper
are situated posterior
at the portion
The
facial follow
nodes
are course and
situated
in the
sub-
of
cutaneouseral, maxillary
tissuesthe artery
of thethe
faceof the
and,external
in genfacial
the neck and the lower vault. There are three group, they drain
the
lateral cranial to ten nodes in this occipital region and
upper lips, cheek, nose, anterior nasal fossae, most of the
gums, teeth, palate, antenor portion of the tongue, medial
portion
anterior
of the eyelids,gual glands,
submandibularand the floor
andof the
sublinmouth.
vein.group, mid
Therewhich portion
are fivedrains of the
to tenthe face and,
nodeseyelids, rarely,
in thischeek, the
directcessory The
flowchain mastoid
primarilyof the nodes
intolateral
the spinalcervical
acnodes.
Their lymph drains into the internal jugular chain of the
lateral cervical nodes.Although these nodes almost may always
clinically be distin-
lie just behind the ear. There are one to four nodes and they
drain the parotid region, parietal area, and skin of the auricle,
and their lymph flows into the inferior parotid nodes and superior
internal jugular chain of the lateral cervical nodes. The nuchal
izodes, which were not described by Rouviere, are a small separate
group of one to three nodes that lie under the origin of the
trapezius muscle tendon and extend downward and parallel to
themidline. They typically become palpable
gums and palate. The into the submandibular The
retropharyngeal
facial nodes drain nodes. nodes are separated
mimicgland,
a massthey can
in the submandibular MR.lie in the superficial submental to
the
into
median
and
lateralnear the posterior
groups.midline to the
The
me-
dial group lies usually directly
and is upper
guished with CT and The submental nodestriangle of the neck,
in patients with infectious mononucleosis (13). The parotid
nodes are situated both superficial to the gland and within the
gland tissue. They are commonly referred to as either
extraglandular or intraglandular and include seven to 19 nodes
(12). These nodes may be confused both clinically and on CT and MR
images with parotid sive gland and tumors. varied They territory
drain including an extenthe
pharynx near the level of the second cervical vertebra. These
nodes can, however, occur as low as the level of the greater cornua
of the hyoid bone. There usually are only one or two nodes in this
inconstant group. The lateral group, consisting of one to three
nodes, is situated near the lateral aspect of the posterior
pharyngeal wall, overlying the longus capitus and longus coli
muscles. These nodes can extend along the entire length of the
phar-
mylohyoid nor belliesare one
muscle of the
and between the antedigastric muscles. Therenodes in this
group,
to eight
which
drains
the chin,floor Their
lowerof the lymph
lip,
cheeks,and into
anterior gingiva, tip of the tongue.
mouth, drains
forehead and temporal regions, portions of the mid and lateral
parts of the face, the auricle and external auditory canal, the
eustachian tube, portions of the posterior part of the cheek,
buccal mucous membrane, gums, and the parotid gland itself. Overall
the most common area to drain into these nodes is the skin, and
thus the most common tumors to metastasize to them are melanomas
and squamous cell carcinomas (3). The lymph from these nodes flows
via a variety of local pathways to the internal jugular chain of
the lateral cervical nodes.
ynx and are often enlarged in newborn infants with a pharyngeal
infection. The lateral retropharyngeal nodes lie medial to the
carotid artery, and this anatomic relationship may help distinguish
such nodes from other retrostyloid parapharyngeal space masses. As
a group, the retropharyngeal nodes primarily drain the nasopharynx
and oropharynx; however, they also drain the palate, nasal fossae,
paranasal sinuses, and middle ear.Their ternal nodes. lymph jugular
drains chain into the superior inof the lateral cervical
The submandibular (submaxillary) nodes are situated in the
submandibular triangle of the neck, lateral to the anterior belly
of the digastric muscle and near thesubmandibular six nodes in this
gland. group, There which are three drains to the
the submandibular nodes and internal jugular chain of the
lateral cervical nodes. The sublingual nodes are inconsistent and
lie in a lateral group along the anterior lingual vessels and in a
medial group between the genioglossus muscles. They drain the
tongue and floor of the mouth. They probably should not be strictly
grouped as lymph nodes, but rather as small lymph nodules located
along the collecting lymphatic trunks of the tongue and sublingual
glands (12). Their lymph drains into the submandibular and
submental nodes and the internal jugular chain of the lateral
cervical nodes. The anterior cervical nodes lie in the infrahyoid
portion of the neck, between the two carotid sheaths. There are two
divisions of this group. The anterior (superficial) jugular chain
follows the course of the anterior jugular vein and lies in the
superficial fascia of the neck, overlying the strap muscles. These
one to four small, inconstant nodes drain the skin and muscles of
the anterior portion of theneck, and their lymph drains into
the
lateral
portion
of the chin,
the
lower
and
594
#{149}
Radiology
December
1987
the
nodes
of Virchow
(Trosier
or
signal
nodes). They may receive metastatic implants from tumors
originating in the abdominal and thoracic cavities (7). The
terminations of these chains differslightly on each side. First,
the respective
chains form jugular lymphatic trunks. On the right side this
trunk enters either the right lymphatic duct, the subclavian
vein,or the internal jugular vein. On the left
side the jugular lymphatic trunk terminates either in the arch
of the thoracic duct or directly into the subclavian or internal
jugular veins. Since these nodes lie outside the carotid sheath,
the internal carotid artery,
commonjugular
carotidvein fat in should the
artery,
and
thebe
internalsharply space,
normally
outlinedby the
on CT and
MR scans,
silhouetted
nasopharyngeal
Figure
3.
Diagram
of the head
and
neck
in
and neck malignancies (4). They provide the major drainage for
all of the other nodal chains. These nodes have been grouped
according to location. The superf icial group contains one to four
nodes andfollows the course of the external jugular
visceral space, and the posterior triangle. The spinal accessory
(posterior triangle) chain of nodes follows the course of the
spinal accessory nerve in the posterior tnangle of the neck. There
are four to 20nodes in this group. The most superior
the left anterior oblique projection. The palpable nodes are
indicated with use of a simplified nomenclature of roman numerals
I-
VII (see Table
1). The clinically
important
retropharyngeal nodes are not included in this system and must
be referred to separately. The internal jugular vein is lateral to
the carotid artery (A) and parallels the course of the
sternocleidomastoid muscle, while the
carotid artery neck. Becausethis vein
runs more vertically in the of this, under the skull base
to the artery, while in it lies anterior to the artery. The two
bellies of the digastric muscle and the omohyoid muscle have also
been drawn as reference points.
is posterior
the root
of the neck
thoracic duct or anterior mediastinal nodes on the left side and
into the lowest internal jugular chain or highest intrathoracic
node on the right side. The juxtavisceral chain of the anterior
cervical nodes lies in relationship to the larynx, thyroid gland,
and tracheoesophageal grooves. One of the pretracheal nodes, the
Delphian node, lies on the cricothyroid membrane and receives lymph
from the
vein, lying superficial to the sternocleidomastoid muscle. The
deep group is divided into three subgroups: the internal jugular
(deep cervical), the spinal accessory (posterior triangle), and the
transverse cervical (supraclavicular) chains. The internal jugular
(deep cervical) chain lies close to the internal jugular vein. Just
under the skull base, these nodes become inseparable from the
highest lymph nodes of the posterior triangle chain. Most of the 15
to 40 nodes in the deep cervical chain are concentrated below the
level where the posterior belly of the digastric muscle crosses the
vein and above the level where the omohyoid muscle traverses the
system. This latter muscle divides the nodal chain into two
clinically important groups: the superior (upper) or supraomohyoid
nodes and the infraomohyoid
nodes blend with the highest nodes of the internal jugular
chain, but while the internal jugular nodes descend almost
vertically in the neck, the posterior tniangle nodes descend
obliquely downward and postenolatenally in the neck. Thesenodes
drain the occipital and mastoid
nodes, the panietal and occipital regions of the scalp, the
nape, lateral portions of the neck, and the shoulder. Their
lymphdrains tions primarily into the transverse cervichain.
cal chain,with
butthe
thereinternal
are alsojugular
communica-
The transverse cervical nodes follow the course
(supraclavicular) of the transverse
cervical vessels. The one to ten nodes in this group primarily
connect the distal posterior triangle chain with the internal
jugular chain and the central neck veins.
The
transverse
cervical
nodes
also
receive
subglottic larynx. Thus, when this node enlarged, subglottic
disease is present. The juxtavisceral nodes have been subdivided
into prelaryngeal, prethyroid, pretracheal, and laterotracheal
groups. There are six to 16 nodes in this category,with most (two
to nine nodes) in the tra-
is
(inferior) nodes. The superior group of nodes lies anterolateral
to the vein, while the infraomohyoid nodes may be either anterior,
medial, or posterior to the vein. The deep cervical nodes are
arranged either in a single series or in two or three roughly
parallel, interconnecting rows that are side by side. They drain
the parotid, submandibular, submental, retropharyngeal, and some
anterior cervical nodes. The nodes caudal to the level ofthe
crossing of the omohyoid muscle also
lymph from the subclavicular skin of the anterolateral
portion
nodes, the of the
neck, and the upper anterior chest wall. They drain in a manner
similar to the internal jugular nodes. These complex relationships
are summarized in Figure 2. Because of the varia-
tions in terminology, a simplified nomenclature was suggested in
1981 (14) (Fig. 3, Table 1). This clinicoanatomic scheme divides
the clinically palpable cervical nodes into seven groups or levels,
eachdesignated not classify by a roman numeral. the pathologically
It does important
cheoesophageal grooves. The highest nodes in the
tracheoesophageal grooves may lie directly behind the posterior
thyroid lobes; when in this location, thesenodes MR may scans be
with confused either on both CT nodule and or a thyroid
receive lymph from the arm and the superficial aspect of the
thorax. A single node in the deep cervical chain, which isusually
larger than the adjacent nodes, is
retropharyngeal
nodes,
which
are
not
parathyroid adenoma. This nodal chain drains the supraglottic
and infraglottic larynx, pyriform sinuses, thyroid gland, trachea,
and esophagus. Their lymphdrains in the same manner as that of
the
situated near the junction of the posterior belly of the
digastric muscle and the internal jugular vein; it is called the
jugulodigastric, sentinel, or tonsillar node. It receives lymph
from the tonsil, neighboring mucous membranes, and the
submandibular nodes. Similarly, at the level where the omohyoid
muscle crosses the internal jugular vein is the juguloomohyoid cent
node, nodes. which is larger than It receives all of the the
adjalymph
easily identified by the clinician. Using this system, the
radiologist can specifically identify a particular node seen on a
scan (e.g., a high, intermediate,
or lowalso be
levelreferred
III node).
Level
I nodes(submental)
can
to as medial
or lateral (submaxillary) allows a more precisethe radiographic
retropharyngeal CT or MR scans,
in location. This correlation betweenfindings. identified be
referred If on
and clinical nodes are they should
anterior ly. The primary
jugular
chain
described
previousup the in head
lateral cervical nodes make nodes of clinical interest
from the or nodes
tongue. Among the in the deep cervical
most chain
inferiare
to as such, being located at a specific tomic reference level as
seen on the ages (i.e., C-i, C-2, etc.).
anaim-
Volume
165
Number
3
Radiology.
595
a.
b.
C.
d.
e.
f.
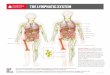
Figure 4. (a) Transverse spin-echo, proton density-weighted MR
image of the upper portion of the neck demonstrates bilaterally
enlarged occipital nodes (0) and multiple bilateral parotid nodes
(P) in this patient with sarcoidosis. Repetition time (TR) = 1,800
msec, echo delay time (TE) = 27 msec, 0.5 T. (b) Axial CT scan
reveals bilateral parotid nodes (P) and posterior triangle (spinal
accessory) (level V) nodes (S) in this patient with sarcoidosis.
(c) Axial CT scan reveals both a medial and lateral retropharyngeal
node (R) on the right side of this patient with acquired
immunodeficiency syndrome. (d) Axial CT scan reveals bilateral
internal jugular chain nodes (I) (level II) in the jugulodigastric
region of the neck. The right node measures i cm in diameter and
must be considered normal (hyperplastic). The left node measures
1.75 cm in diameter and is pathologic in this patient with
carcinoma of the supraglottic larynx. SM = submandibular gland. (e)
Axial CT scan reveals two left submandibular nodes (sni) (level I)
in this patient with lymphoma. SM = submandibular gland. (f) Axial
CT scan reveals bilateral lower-neck posterior triangle (spinal
accessory) nodes (5) (level V) in this patient with lymphoma.
Since poorly logically used cervical
normal
lymph
nodes
are
often
seen on scans, if seen at all, pathoenlarged lymph nodes will be
to illustrate nodes just some of the important (Fig. 4).
discussed
the entire neck ternal auditorytop of the
from canal
the level of the ex(skull base) to the
can be given initially trated drip administeredThis latter
technique
andallows
the concenthereafter.scanning
manubrium.
CT is performed with the patients chin slightly elevated. A
gantry angle of 00 is used, and 5-mm-thick contiguous scans be are
obtained after throughout the
IMAGINGThere are at least
PROTOCOLtwo approaches to
areashould
of interest.obtained
If possible,
the
scans
to be started immediately, with no time lost during contrast
material administration. Magnetic resonance (MR) imaging protocols
are more varied, dependingin unit part on being the used. magnet In
nodes. 5 mm strength general, and transverse the
administration
imaging the neck: With one, only the area suspected of being
pathologic is imaged, while with the other, the entire neck is
imaged. The former approach provides short examinationtimes.
However, in patients with ma-
of contrast material because these images will help in the
differentiation between vessels and nodes and, in somecases,
tissues. administered between The pathologic contrast as a drip
material of 150 and normal is usually mL of a
imagescervical nesses
are
most
useful
forSection are
depictingthicksince optimal,
lymph of about
lignancy outsideIn addition, metastasize tween
there of theto the skull
may be occult disease clinically localized area.most the base
primary neck and efficacious are the tumors located root of that
bethe
concentrated iodinated agent (e.g., Conray [Mallinckrodt, St.
Louis] 600 mg/mL); scanning is initiated when one-third of the
bottle (50 mL) hasbeen 50 mL given. of Alternately, contrast
material a bolus (e.g., of Hy25-
thicker sections may obscure small nodes. Because of time
constraints, only the area of interest is usually imaged; however,
with newer, faster imaging techniques and new software, thesetime
limitations may become less of a
neck.lignancy
Therefore,it is more
in patients
withto
mascan
paque
50 [Winthrop-Breon,
New
York])
factor. Ti-weighted images usually good differentiation
between
provide the inter-
596.
Radiology
December
1987
5.Figures 5, 6. (5) Axial CT scan reveals two necrotic
6.nodes in the right side of the neck. One
region of the internal jugular chain (I) (level II), and one is
in the posterior triangle (5) (level V) of this patient with
carcinoma. Both nodes are enlarged and have necrotic regions with
irregular, nodular walls. (6) Axial CT scan reveals a necrotic,
smooth-walled cystic mass in the right posterior triangle (level V)
in this patient with metastatic papillary thyroid carcinoma. This
is too far posterior in the neck to be a branchial cleftcyst of
this size.
is in the jugulodigastric
mediate-signal-intensity lymph nodes and the
high-signal-intensity fat. A similar, although less clear,
distinction can be seen on proton density-weighted (mixed) images.
On strongly T2weighted images, the pathologic nodes tend to become
bright in intensity, whereas the surrounding fat now has an
intermediate-intensity signal. On the T2-weighted studies, focal
areas of high signal intensity may be seen in nodes, and these may
represent sites oftumor necrosis.
The quality of the image depends most on the signal-to-noise
ratio, which in turn depends on the surface coil used. At present,
a variety of coils are being used by different manufacturers and
individuals, and no one technique has been determined to be better
than the others. Pathologically correlated studies must be done
before optimal imaging sequences and coil designs can be
determined.
CRITERIA FOR CERVICALOnce knowledge ture and the locationslymph
tained, velop nodes the criteria next for on
EVALUATING NODESabout nomenclaof cervicalhas been step when obis
to dea node
images important deciding
is pathologic. The nodes in the upper portion of the neck tend
to be larger than those the lower portion; this is especially true
of the submandibular and upper supraomohyoid nodes of the internal
jugular chain (8, 12, 15). These nodes
in
become enlarged due to a benign reactive hyperplasia that is in
response to the common inflammatory episodes that so often involve
the teeth, gums, tonsils, and pharynx. Results of several clinical
series with pathologic correlation have suggested that a clinically
positive (metastatic) node should be defined as being greater than
1 cm in diameter, spherical rather than flat or ovoid, and harder
than an uninvolved node (4, 16, 17). Other authors have indicated
that, especially for the submandibular and internal jugular chain
nodes, normal nodes are usually 1.5 cm in diameter or less; nodes
in the other cervical chains are normally smaller than 1 cm in
diameter (12, 15, 18, 19). It should be noted that most cervical
lymph nodes are ovoid or lima bean shaped, and the determination of
nodal size is based on the greatest nodal diameter. Thus, to
correlate imaging findings with these clinical studies, contiguous
images may have to be examined in some patients in order to
determine accurately the greatest diameter of a node whose longest
dimension is parallel to the craniocaudal axis. The smallest-sized
nodes detected with palpation were approximately 0.5 cm for
superficial nodes and 1 cm for deeper nodes (17). On the basis of
these studies, the most reasonable size criteria to use when
evaluating cervical lymph nodes in the submandibular (level 1) and
jugulodigastric regions of the internal jugular chain (low level
II, high level III) are that any node in these regions larger than
1.5 cm in diameter must be
considered abnormal, while for the remaining nodes in the neck a
diameter of more than 1 cm should be considered abnormal (17, 20).
On the basis of these criteria, about 80% of enlarged nodes are
truly metastatic and 20% are enlarged due to benign hyperplasia;
these statistics are similar to those reported by clinicians (17,
21, 22). The larger the size by which a node is considered
abnormal, the fewer false-positive findings will be reported;
however, as the number of false-positive findings decreases, the
number of false-negative findings will increase. Because of this,
in large cancer centers where the patient population is biased
toward cancer, the smaller 1-cm-diameter criterion is often used
for all nodes, to raise the diagnostic level of suspicion. This is
usually done with the proviso that before such a borderline lymph
node is called metastatic, it must be spherical rather than ovoid.
It is known that cancer cells initially enter the lymph node via
the afferent lymphatics and lodge in the reticular meshwork of the
marginal sinuses of the nodal cortex. Proliferation of the
malignant cells then results in invasion of the nodal medulla,
extensive neoplastic invasion, blockage of the flow of lymph, and
propagation of cancer cells to other nodal chains. Eventually the
nodal medulla undergoes necrosis. Although this may occur within a
brief period of time, metastatic nodal necrosis is a biologically
late event in the evolution of the tumor in the lymph node (4, 23).
Both CT and MR imaging can be used to detect nodal necrosis, even
in nonenlarged nodes. This further increases the sensitivity of the
overall nodal evaluation, for now both necrosis and nodal size are
used as criteria.
Any node with central necrosis, regardless of size, must be
considered pathologic. At CT, this necrosis usually appears as a
central area of low attenuation (10-18 HU) with a surrounding
irregular, nodular wall (1, 18) (Fig. 5). The nodal wall can,
however, be smooth or uniform, simulating a benign process. This
latter appearance ismost often associated with metastatic
papillary thyroid carcinoma rather than with squamous cell
carcinoma (Fig. 6). Fatty nodal replacement can occur in
postinflammatory and postirradiation nodes (18). This replacement
usually occurs in a peripheral or noncentral location within the
node. Although any measurement of the attenuation of such a small
area is fraught with volume averaging errors, these regions usually
measure near 0 HU andthus are at a lower attenuation than
metastatic necrosis Although there relevant correlation
(18). is little statistically between patholog-
Volume
165
Number
3
Radiology
#{149} 597
a.
b.
C.
Figure 7. (a) Axial contrast material-enhanced CT scan reveals
two adjacent necrotic nodes in the right jugulodigastric region of
the internal jugular chain (level II). The nodes have enhancing,
unsharp rims that suggest extracapsular invasion in this patient
with pharyngeal carcinoma. (b) Spin-echo, proton density-weighted
MR image of the neck near the same level as a reveals the enlarged
right nodal mass. However, it is not evident that there are two
conglomerate nodes rather than one large node. TR = 2,000 msec, TE
= 30 msec, 0.5 1. (C) Spin-echo 12-weighted MR image, paired with b
(TR = 2,000 msec, TE = 80 msec), reveals high signal intensity in
the right nodal mass, suggesting necrosis. The capsular margins are
also unsharp, suggesting extracapsular invasion.
ic and MR findings at this time, there initial evidence to
suggest that areas high T2 signal intensity within alymph node may
correspond to sites
is ofof
tumor necrosis, and that MR imaging may become a sensitive
technique for the evaluation of these metastatic nodes (Fig. 7). In
all patients presenting with cervical adenopathy, there is the
possibility that a node, whether cavitated or not, will be
inflammatory in origin. In mostbut guish not all between instances,
history and physi-
cal examination andious
canan the
be used node.
to distinAn insida non-
inflammatory-related
a metastatichistory,
lymphabsence
of pain,
tender mass, and fixation all indicate a malignant lesion. Even
so, there will be a few cases in which both the clinician and the
radiologist cannot distinguish between the two possibilities; in
these cases, only the pathologist can resolve the issue. Some
further CT findings that can aid the radiologist in
distinguishingbenign from malignant disease include
(a) the presence of a thick, irregular zone of enhancement
around a necroticcentral matory area, process which indicates or an
abscessed inflam(abscess
node-especially tuberculosis-or an infected branchial cleft
cyst); (b) the presence of a thin, enhancing rim with one or more
focal areas of nodularity(3, 24), which node indicates with
capsular a malignant invasion; lymph
(c) the whichcess,
presence indicatessince most
of an enhancing an inflammatorytumor nodes have
node, proan
attenuation equal to or less than that of muscle; (d) the
presence of nodes some of which enhance, some of which are of
muscle density, and some of which are of a lower attenuation than
muscle. These varied attenuations suggest agranulomatous process
(Fig. 8).
Calcifications within cervical lymph nodes are unusual. Most
often these calcific deposits are found with old granulomatous
disease (scrofula). Metastatic tumoral calcifications are uncommon,
and the most likely primary neoplasm is papillary thyroid carcinoma
(Fig. 9). Healed, irradiated metastatic carcinomatous and
lymphomatous nodes may in rare cases calcify. In addition, from a
clinical and pathological perspective, about 5% of metastatic nodes
will be clinically occult but will be detected by CT (18). These
nodes lie primarily deep to the sternocleidomastoid muscle or in
areas that are not accessible at routine examination, such as the
retropharyngeal or tracheoesophageal regions. Thus, imaging
techniques make the staging of metastatic nodes more accurate than
if clinical examination is used alone. The advantage of imaging
over palpation is also demonstrated when an obvious conglomerate
mass of nodes seen on images is erroneously interpreted by the
clinician as a solitary node. This distinction can influence the
staging of the cervical nodes if the clinician believes that such a
mass is less than 3 cm in diameter (25). The occurrence of
extranodal tumor extension is an ominous prognostic sign and is
associated with about a 50% decreased survival compared with the
survival in patients with tumor confined to the lymph nodes (26).
Although it used to be assumed that lymph nodes determined at
physical examination to be smaller than 3 cm in diameter did not
have extracapsular spread, it is known today that such extranodal
tumor extension occurs in 23% of nodes smaller than 1 cm, 53% of
nodes 2-3 cm, and 74% of nodes greater than 3 cm. Overall,
extranodal spread occurs in 60% of nodes less than 3 cm in
Figure
8.
Axial
contrast-enhanced
CT scan
reveals multiple posterior triangle (level V) and internal
jugular chain (level III) nodes in the left side of the neck. Some
of these nodes enhance more than do the adjacent muscles, one or
two are about the same at-
tenuation, and one or two have areas of lower attenuation. There
is also a small, enhancing right internal jugular chain node (level
III) (arrow) in this patient with tuberculosis.
diameter (26, 27). On CT images, extranodal spread is correlated
with an unsharp or poorly defined nodal border that may or may not
enhance. There also may be associated obliteration of the adjacent
fat planes (1, 3). These findings are more indicative of metastatic
disease if there is no history of prior surgery, irradiation, or
recent infection, all of which can cause similar imaging findings
(28).
598
#{149}
Radiology
December
1987
extracapsular spread, of nodal immunoreactivity, of the precise
tumor site, and of the histologic characteristics of the tumor
(32). These systems are currently based on clinical findings.
However, there is hope that imaging will soon be a necessary part
of this staging. If scanning is
used to complement clinical examination, the following staging
conversions can occur: NO will become Ni neck, Ni will become N2
neck, Ni will becomeN3c neck, or NO will become N3c neck.
of patients with head and neck cancer, it was found that the
number of deaths increased from distant metastases, decreased from
uncontrolled tumor, decreased from fatal complications of
treatment, and increased from unrelated nonmalignant disease. The
frequency of a second malignancy as a cause of death remained
constant at 14% (36).Thus, it appears we are seeing a change
Clearly, imaging state-of-the-art
is necessary to the evaluation of cancer.
CLINICALThe presence node in a patient tive tract cancer
Invasioninous
PERSPECTIVEof a metastatic with upper is an ominousof the
cervical aerodigesproglocation
in the evolution of head and neck cancers, with distant
metastases starting to become a serious treatment consideration; it
is clear that the frequency of such distant metastases is greater
in patients with metastatic disease of the cervical nodes (26). The
location of a metastatic node in the neck, regardless of the site
of theprimary tumor, may have a certain
of the
carotidAlthough
arteryin
hasmost
omsur-
nostic
sign.
Regardless
implications.
of thesingle
primarymetastatic
tumor,node
thein
presencethe ipsilateral
of a
casesrounding
effacementthe artery
of the
fat planesarterial
signifies
portionsurvival
of thein half.
neck
cuts
the
expectedaffect-
invasion, this is not always true (1, 28). Ultrasound has been
employed to define better the true cases of carotid artery
invasion, and although use of this technique can reduce the number
of false-positive diagnoses made on thebasis still ologist of a few
(29). CT imaging cases In that general, alone, will there defy a
cautious the are radira-
A contralateral
diologic diagnosis of probable arterial invasion will usually be
correct and will not effectively influence the treatment planning
for these patients, whousually have more advanced disease.
ed node also reduces the expected survival by 50%. Thus, a
patient with bilateral cervical metastases has only one quarter the
expected survival he or she would have had if there were no
metastatic nodes (33-35). The presence of extranodal tumor spread
is the best prognosticator of local treatment failure and is also
associated with a 50% decreased survival (3335).
At present, it is not possible to identify microscopic tumor
implants in a normal-sized noncavitated node by means of any
imaging technique. Similarly, although an educated guess can often
be made about the nature of a pathologic area in an abnormal node
based on its imaging appearance, no steadfast rules exist and
histologic findings sometimes prove any of theserules to be in
error.
Once the lymph nodes become obstructed, there may no longer be
an orderly progression of disease down the lymphatic chains into
the vascular system. Tumor cells may bypass the obstructed ginal
medulla sinuses, or by they means may of enter the marthe
prognostic value. As an example, the mere presence of a
metastatic level V node suggests a 19% worse 5-year survival
compared with survival in patients who have metastatic nodes in any
site other than the posterior triangle. Similarly, metastatic level
IV nodes have an associated grave prognosis because most of them
are metastases from a primary tumor located below the clavicle.
About 2.8% of intrathoracic and intraabdominal malignancies will
spread to these nodes (7). Similarly, if a primary tumor of the
head and neck spreads to level IV nodes, more proximal nodes are
probably already involved, and the patient has either a
biologically aggressive tumor or a faradvanced malignancy. The
preferred sites of metastasis for the various primary tumors of the
head and neck have been thoroughly studied (3, 16). Although most
of the neoplasms metastasize to level II and III
blood stream within the node. This phenomenon appears to account
for the skip-type metastases that occur in some patients. On the
other hand, lymphatic-venous shunting has been found in patients
with nonobstructedlymphatics, and account metastases and argues
this for against intercommunicathe confused in the some concept
patpafound tion tern tients may of
CANCER
STAGING
SYSTEMS
nodes, some conclusions can be drawn from these analyses (Table
3). Tumors that have the highest frequency of metastasizing at
clinical presentation, the highest frequency of bilateral nodal
involvement, and the highest frequencies of posterior triangle
adenopathy all arise from Waldeyer ring and, in particular, the
nasopharynx (23). Since thisregion can be examined in physician
detail when
There are two major TNM (tumor, node, metastases)
classifications currently in use for the staging of head and neck
cancers. The one more generally accepted in the United States was
developed by the American Joint Committee on Cancer (AJCC). The
other system was developed by the International Union Against
Cancer (UICC). Although both systems correlate well with one
another, the AJCC system may be more discriminative for nodal
disease (Table 2) (30, 31). At present,however, cized nodal for
both not location systems addressing in reference have the been
issues both to critiof the
that metastases are strictly confined to one or another system
(except, perhaps, early in the evolution of the disease (26). In
recent years, there has been better control of local and regional
cancer, and while patients are living somewhat longer, they are
exhibiting the development of distant metastases. This may, in
fact, only be the unmasking of thenatural history of head and neck
cancer
thegist
entiremay be
neckthe
is imaged,first
the
radioloto local-
primary portions
tumor and to the of chains within
chains or the neck, of
with successfully treated local and regional disease, and it may
be more correct to view head and neck cancer as a systemic disease
rather than as a localregional process, as it has been
traditionally viewed (26). In a recent study
ize the primary tumor in a patient presenting clinically with
cervical metastases. This is especially true in the 4.7% of
patients who present with an occult primary tumor and in whom
imaging enables identification of as many as 25% of these
clinically undiagnosed tumors (3, 20, 23, 37, 38). In addition, it
is generally believed that when metastases are found at nodal
levels not expected of a particular primary tumor, this neoplasm is
more biologically aggressive than normal (16, 26). Thus, the
radiologist shouldbecome familiar with the statistically
Volume
165
Number
3
Radiology
#{149} 599
expected nodal metastases for each of the primary tumors of the
head and neck. Evidence suggests performance of an open biopsy on a
neck node will decrease the patients survival unless definitive
surgery is performed without delay (26). This has prompted the
increased use of the skinny-needle biopsy procedure, with or
without imaging guidance (38-40). In fact, new needle materials are
being developed that reduce imaging artifacts and make
imaging-guided biopsies more practical (41). A limiting factor in
this procedure is lack of access to an expert cytologist; however,
this problem appears to be diminishing, since interest in this
technique has grown. Today, physicians at most institutions will
perform a skinny-needle biopsy before surgically violating a neck
for a diagnostic procedure. Even newer approaches are being
investigated in which, by the use of thinneedle monitors, in vivo
oxygen tension is being monitored to help the clinician evaluate
the presence of tumor or the effectiveness of therapy (42). New
techniques will continue to evolve in the quest to solve the
problems of head and neck cancer.
Table Nodal
3
Metastases
in Patients
with
Head
and Neck
CancerPercentage of Percentage ofPatients Initially Who Present
Patients with Bilateral Metastatic Nodes
Site
of Primary
Nodal
Levels
Most
Carcinoma Oral portion of tongue Floor of mouthRetromolar
trigone
Commonly I, II, IIII, II
Involved
with
Metastases34-65 30-59 39-56
11.8 7.8 8.8 253L8 20.2
anterior fascial Soft palateNasopharynx
pillar
1, II, III II II, Ill, IV,II, 111, I, II, III, IV, II, III,
IV,
37-56V V V V (22.3%) (10.9%) (9.0%) (8.4%) 86-90 50-71
Oropharynx Tonsillar
fossa
58-7652-72
139
Hypopharyn.x Base of tongue Supraglottic larynxNote-Data in
table obtained
II, III, IV, II, Ill, IVfrom references
V (6.7%)
50-8331-54
21.322.5
17, 18, and
24.
7.
8.
Hollingshead WH. Anatomy for surgeons. 1, The head and neck. New
York: Hoeber-Harper, 1954; 488-494. Rouviere H. Lymphatic system of
the head
Vol.
26.
Collins
SL.
Controversies
in management
of
and
cancer of the neck. In: Thawley eds. Comprehensive management
neck tumors. Vol. 2. Philadelphia:27. 1987; Snow 1386-1443. GB,
Annyas AA, Van Slooten
SE, Panje WR, of head and Saunders,EA, Bartelink
neck.tern.
In: AnatomyTobias MJ
of the(trans.).
humanAnn Arbor,
lymphaticMich.:
sysEd-
9.
wards Brothers, 1938; 5-28. Last RJ. Anatomy regional
H, Hart and applied. 6th ed.28.
AA.
Prognostic
factors
of neck7:185-192. tomography
node
meof
10
11.
12.
Edinburgh: Churchill-Livingstone, 1978; 376378, 443-444.
Montgomery WW. Surgery of the upper respiratory system.
Philadelphia: Lea & Febiger, 1971; 75-87. Trotter HA. The
surgical anatomy of the lymphatics of the head and neck. Ann Otol
Rhinol Laryngol 1930; 39384-397. Feind CR. The head and neck In:
Haagensen
tastasis. Clin Otolaryngol 1982; Som PM, Biller HF. Computed
the neck in the neck dissectionology 1983;
postoperative patient: and the myocutaneous
radical flap.
Radi-
148:157-160.
29.
Hajek PC, Salomonowitz E, Turk R, Tscholarkoff D, Kumpan W,
Czembirek H. Lymph nodes of the neck: evaluation with US. Radiology
1986; I 58:739-742.Black RJ, Gluckman JL, Shumrick DA. Staging
30.
CD, Feind CR, Herter FP, Slanetz CA, Weinberg JA. eds. The
lymphatics in cancer. Philadelphia: Saunders, 1972; 60-208.13.
Kuisk of the H. Development. lymphatic system. structure, In: Kuisk
and function H, ed. Tech-
systems
for cancerbetween 8:305-312. node
of theAJC
headand
andUICC.
neckClin
region:Otolar-
comparison yngol 1983;
CONCLUSIONClearly, imaging today plays an essential role in the
evaluation of disease in the cervical lymph nodes and should be
part of any thorough workup of patients with head and neck cancer.
With the continued advance of techniques and the growing interest
in head and neck imaging, it is only reasonable to expect that, in
the future, imaging will have an even greater impact on patient
management. #{149} Acknowledgments:I thank Hugh D. Curtin, M.D.,
William P. Dillon, M.D., and R. Thomas Bergeron, M.D., for their
advice and editorialcomments script. in helping me prepare this
manu-
31.
Johnsvical
ME, Neallymph
DA, Cantrellmetastasis:
RN. LaryngolPatel MF,
Staging 1984;Harvey
of cerof two
comparison
niquepretation.
of lymphographySt. Louis: neck Green,
and RH,
principles1971; 5-14.
of interB. Surgical32.
systems.332. Rapidis
AnnAD,
OtolLangdon
RhinolJD,
93:330PW.
14.
Shah
JP, Strong
E, Spiro
Vikram
15.
grand rounds, futurepossibilities Mancuso AA,
dissection: current status and Clin Bull 1981; 11:25-33.
Harnsberger HR. Muraki AS. Ste-
vens MH. Computed and retropharyngeal
tomography lymph nodes
of cervical normal anatoin staganatomy. Ra-
33.
16.
my. variants of normal, and application ing head and neck
cancer. I. Normal diology 1983; 148:709-714. Lindberg R.
Distribution ofcervical
34.lymph node 35.
metastases from upper respiratory17.
squamous cell carcinoma of the and digestive tracts. Cancer
STNMP: a new system for the clinico-pathological classification
and identification of intraoral carcinomata. Cancer 1977;
39:204-209. Farr HW, Goldfarb PM, Farr CM. Epidermoid carcinoma of
the mouth and pharynx at Memorial Sloan Kettering Cancer Center
1965 to 1969. Am Surg 1980; 140:563-567. Spiro RH. The management
of neck nodes in head and neck cancer: a surgeons view. Bull NY
Acad Med 1985; 61:629-637.Batsakis JG. Tumors of the head and neck:
clini-
18.
19.
References1. Mancuso AA, Macen D, Rice D, Hanafee WN. CT of
cervical lymph node cancer. AJR 1981; I36:381-385. Kuisk H.
Cervical lymphography. In: Kuisk H. ed. Technique of lymphography
and principles of interpretation. St. Louis: Green, 1971; 156-162.
20.
1972; 29:1446-1449. Sako K, Pradier RN, Marchetta FC, Pickren
JW. Fallibility of palpation in the diagnosis of metastasis to
cervical nodes. Surg Gynecol Obstet 1964; 1 18:989-990. Mancuso AA,
Harnsberger HR. Muraki AS, Stevens MA. Computed tomography of
cervical and retropharyngeal lymph nodes: normal anatomy, variants
of normal, and application in staging head and neck cancer. II.
Pathology. Radiology 1983; 148:715-723. Jinkins JR. Computed
tomography of the craniocervical lymphatic system: anatomical and
functional considerations Neuroradiology 1987; 29:317-326. Friedman
M, Shelton V. Mafee M, Bellity P. Skolnik E. Metastatic neck
diseases: evaluation by
cal and pathological considerations. more: Williams &
Wilkins, 1979;250.
2d ed Balti144-176, 240progress?HR.
36.37,
Goepfert
H.
Are1984; Mancuso
we making
any
Arch
Otolaryngol Muraki AS,
110:562-563. AA, Harnsberger
38.
39.
Metastatic cervical adenopathy from tumors of unknown origin:
the role of CT. Radiology 1984; 152:749-753. Gatenby RA, Mulhern CB
Jr., Strawitz J, Moldofsky PJ. Comparison of clinical and computed
tomographic staging of head and neck tumors. AJNR 1985; 6:399-401.
Gatenby RA, Mulhern CB Jr., Richter MP, Moldofsky PJ. CT-guided
biopsy for the detectionand staging of tumors of the head and
neck.
computed21.
tomography.
Arch
Otolaryngol
1984;SE. CerviLaryngoAA.
40.
AJNR 1984; zornoza J.Clause ME,
5:287-289. PercutaneousWallace ed. 5, eds.
lymphLymphatic
node
biopsy.imaging,
In: scm-
2.
1 10:443-447. Cinberg JZ, Silver CE, Molnar cal cysts: cancer
until proven
JJ, yogI otherwise.HR. Mancuso
lymphography,tigraphy. 2d 1985; 496-510.
computedBaltimore:
tomography,Williams
and& Wilkins.
3.
ReedeS, eds.
DL, Bergeronlymph Lymphatic
RT.nodes. Imaging:
ComputedIn: Clouse lymphography,
tomographyME. Wallace com22.
scopeStevens
1982;MH,
92:27-30.Harnsberger
of cervical
41.
putedmore:
tomography,Williams
and& Wilkins,
scintigraphy.1985; 472-495.
2d ed. Balti23.
Computed tomography staging and management cer. Arch
OtolaryngolSom PM. An approach
of cervical lymph nodes: of head and neck can1985; 11:735-739.to
tumors of patients. of the In: San head and
42.
Lufkin R, Teresi L, Hanafee W. New needle for MR-guided
aspiration cytology of the head and neck. AJR 1987; 149:380-382.
Gatenby RA, Coia LR, Richter MP, et al Oxygentension in human
tumors: in vivo mapping using
4.
5. 6.
Schuller DE. Management of cervical metastasis in head and neck
cancer, no. 82200. Washington, D.C.: American Academy of
Otolaryngology, Head and Neck Surgery Foundation, 1982. Paff GH.
Anatomy of the head and neck Philadelphia: Saunders, 1973: 221-228.
Taillens JP. Les ad#{233}nopathies cervicales essai dune
classification #{233}tiologique des ad#{233}nites enfonction de
leur localisation Suisse anatomo-topogra-
neck:staging
the
roleand
of computedfollow-up
tomography radiology.
in theMargulis
CT-guided
probes.
Radiology
1985;
156:211-214.
AR. Gooding
CA,
eds.
Diagnosticof California RT. Cervical
San
24.
Francisco: University 1985; 347-352. Reede DL. Bergeron
Francisco,
tuberculous
adenitis:25.
CT manifestations.
Radiology
1985;of
phique. 280.
Rev
Med
Romande
1962;
82:259-
14:701-704. American Joint Committee on Cancer. Staging cancer
of head and neck sites and of melanoma. Chicago: Lippincott,
1980.
600
.
Radiology
December
1987