Embed Size (px)
Citation preview

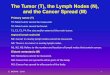
HISTOLOGY AND PATHOLOGY OF LYMPH NODES
Presented by Dr. Anjum Baker
II MDS postgraduateDept. of Oral Pathology & Microbiology, VIDS&RC
SEMINAR#8

Contents•Introduction•Overview of Lymphoid organs•Embryology of lymph nodes•Anatomy of head and neck nodes•Lymphatic drainage of oral cavity•Clinical examination of head and neck nodes•Histology of Lymph nodes including cytology•Pathology of lymph nodesoInfectionsoReactive hyperplasiasoLymphoid neoplasmsoOthers

INTRODUCTION•Lymphoid system is a part of the hematopoietic system represented by thymus, lymph nodes and spleen
•Lymph nodes form a part of the immune system as well as the circulatory system as it collects and drains lymph and are distributed along the course of the larger lymphatic vessels.
•Lymph originates as blood plasma, in tissue capillary bed, plasma leaves the circulatory system to become interstitial fluid.
• 90% of interstitial fluid is returned to capillary bed and drains via venous channels.Remaining 10% is drained via lymphatic system and makes up the lymph

LYMPHOID ORGANS•CENTRAL/PRIMARY•Where new lymphocytes are produced
•Bone marrow•Thymus
•PERIPHERAL/SECONDARY
•Where lymphocytes respond to antigens
•Lymph nodes•Spleen•Tonsils•Mucosa/skin associated lymphoid tissue (MALT)

• EMBRYOLOGY• Develops from lateral plate
mesoderm• Lymphatic sacs develop
from endothelial outgrowths of large central veins
• Sacs are invaded by mesenchymal cells that proliferate and aggregate
• Ist trimester end- foci of lymphoblasts
• 2nd trimester end-Organisation into cortex, medulla and primary follicles

ANATOMY OF H&N NODES•Distributed in 3 regions•1. peripheral nodesi. circular chain/cervical collar/horizontal
superficial ringii. deep inner circle/ horizontal deep ring•2. Deep cervical nodes/vertical chain
•Waldeyer’s ring

PRINCIPAL H&N NODESRouviere in 1938 divided the nearly 300 lymph nodes of head and neck into 10 principal groups
•SUPRAHYOID•1. Occipital •2. Mastoid•3. Parotid•4. Submandibular•5. Facial •6. Submental•7. Sublingual•8. Retropharyngeal•9. Anterior cervical•10. Lateral cervical
•INFRAHYOID•1. Anterior cervical•A)Juxtrvisceral•B) prelayngeal•C) Pretracheal•D) prethyroid•E) Lateral tracheal•2. Lateral cervical•A) Deep •B) Superficial

WALDEYER’S RING•Immunosurveillence organs of head and neck
•Palatine tonsils•Lingual tonsils•Tubal tonsil•Phayngeal tonsil

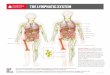
LYMPHATIC DRAINAGE

CLINICAL EXAMINATION

CLINICAL FINDINGSFINDING INTERPRETATION
Firm,tender,enlarged,warm Inflammation
Firm to fluctuant, nontender,enlarged,mobile,
Chronic inflammation/chronic abscess(TB,HIV etc)
Tensely filled balloon/grape Acute abscess
Nontender,enlarged,rubbery consistency
Post infection
Firm,nontender,matted,fixed,slowly enlarging
Malignancy
Diffuse bilateral involvement Systemic malignancy
Localised involvement Localised malignancy
Posterior cervical lymph node enlargement
Upper respiratory tract infection

•SURGICAL DISSECTION

HISTOLOGY OF LYMPH NODES•CAPSULE •OUTER CORTEX•INNER MEDULLA



•PRIMARY FOLLICLES•In the absence of immune stimulation
•SECONDARY FOLLICLES OR GERMINAL CENTERS
•In the presence of immune stimulation.

CELLS OF LYMPH NODESA.SMALL LYMPHOCYTES T/B cells Effector/memory Lineage- by
location in node (Lymphocyte homing)
Clumped chromatin- non activated
Stage of maturation-IHC/molecular techniques

B. GERMINAL CENTRE CELLS•Replicating and post-replicating B cells
• I)Noncleaved cells, small and large•Replicating populations- expanding antigen responsive cells.•Round nuclei but larger than resting small lymphocyte•Open or vesicular chromatin•Recognizable nucleoli.
•Nucleus clear -->genetic material unwound for replication. •Size, large or small compared nucleus of macrophage.
•2)Small cleaved cells- ( CENTROCYTES)•Nonreplicating population•Post mitotic memory or plasma cell precursors•Clumped chromatin • Irregular folded and cleaved nuclear profiles

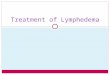
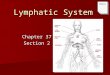
REACTIVE GERMINAL CENTRE
MZ
LZ
DZ


3.IMMUNOBLASTS
•Replicating large cells found outside the germinal
centers.
•May be of B or T cell type
•Have nuclear characteristics of replicating
lymphocytes- Vesicular chromatin ,Nucleoli

4. ACCESSORY CELLSI) Antigen processing cells
• Interdigitating reticulin cells- T cell paracortex
•Dendritic reticulin cells- B cell germinal centers
•Process and present antigen to B and T lymphocytes
• Invisible in normal lymph node
2) Macrophages
Phagoctytic cells of lymph node
Tingible body macrophages of germinal centers
Medullary and subcapsular sinus macrophages-
Abundant pale cytoplasm
Oval nucleus, single small nucleolus

PATHOLOGY OF LYMPH NODES•Infections•Reactive hyperplasias•Malignant lymphomas•Metastatic tumors•Others

INFECTIONS•SPECIFICi. Bacterial- TB, syphilis, brucellosisii. Viral- infectious mononucleosis,PGL OF
HIV,LGViii. Fungal- histoplasmosis,
blastomycosis,coccidomycosisiv. Parasitic- Filariasis,toxoplasmosis
• NONSPECIFICi. Acuteii. Chronic

BACTERIAL INFECTIONSCommon Features•Increase in no of Germinal centres•Hyperplasia of paracortical T cell zones•Granulomatous lesion –caseous /non caseous•Identification of causative organism is only by culture/serology.

TUBERCULAR LYMPHADENITIS•The characteristic morphological element is the tuberculous granuloma (caseating tubercule) which maybe confluent.
•This consists of Langhan’s giant cells surrounded by epithelioid cells , T cell lymphocytes and fibroblasts.
•Granulomatous tubercules eventually develop central caseous necrosis and tend to become confluent, replacing the lymphoid tissue.
•Stages of Tubercular Lymphadenitis -•Lymphadenitis•Periadenitis•Cold abscess•'Collar stud' abscess•Sinus•Syphilitic lymphadenitis- Similar presentation but rare.


ACUTE NONSPECIFIC LYMPHADENITIS
•Prominent large reactive germinal centres•Numerous mitotc figures•Macrophages with particulate debris•Pyogenic infection- neutrophils•Necrosis at centre of follicle•Severe infections- acute inflammatory cell infiltrate with effacement of LN architecture
•Less severe infections- scattered neutrophil infiltrate in follicles and accumulation in lymphoid sinuses
•Hyperplasia of endothelial cell lining sinuses


CHRONIC NONSPECIFIC LYMPHADENITIS
•Germinal centres in secondary follicles•Chronic inflammatory cells-Macrophages, plasma cells and eosinophils.
•Necrosis of entire follicles•Fibrosis•Thickened sinus walls•Effacement of LN architecture


Infectious Mononucleosis•EBV infection in young adults- lymphadenopathy•Periperal blood lymphocytosis•Diagnosis-Serology•H/P•Marked paracortical hyperplasia•Early stages- follicular hyperplasia• Increased population of small lymphocytes, plasmacytoid lymphocytes,immunoblasts,R-S cells, histiocytes and plasma cells
•Foci of coagulative necrosis•Late Stages- effacement of architecture ,sometimes only residual follicles/patent sinuses can be identified
•DD- Lymphomas• IHC- CD45+ (immunoblasts), CD15-(R-S Cells)


HIV INFECTION Persistent generalized lymphadenopathy H/P Initial marked reactive follicular hyperplasia Large bizzare germinal centres, Minimal/absent mantle zone Follicle lysis- small lymphocytes infiltrate GC Marked monocytoid B cell reaction in sinuses Paracortical regions are not prominent Chronic condition Involution of LN Lymphocyte depletion Only follicular dendritic cells remain Plasma cells, histiocytes and vascular network remains Wide patent sinuses Later stages- malignant neoplasms, increased histiocytes, MAC infections


REACTIVE HYPERPLASIAS•3 PROMINENT PATTERNS1. Follicular hyperplasia2. Paracortical hyperplasia3. Sinus histiocytosis

A. Follicular Hyperplasia•Increase in no and size of germinal centres,•may involve paracortex and medullary areas•Seen in- •collagen vascular disorders•Systemic toxoplasmosis•Syphilis


B. Paracortical Hyperplasia•Increase in interfollicular elements• small compressed follicles•Increased subcortical infiltrates•Seen in•SLE•Viral infections( low grade)•Drug reaction


C. Sinus Histiocytosis•Expansion of medullary sinus histiocytes•Selective proliferation of histiocytes•Expanded patent sinuses•Seen in-•Malignancy adjacent to lymph nodes•Chronic Infections


LYMPHOMAS•Malignant neoplasms of lymphoid origin•Divided into Hodgkin’s and Non-Hodgkin’s types•All HL and 2/3rd of NHL occur in lymph nodes•Lymphoid neoplasms show some degree of T or B cell differentiation
•Associated with immune system abnormalities•Neoplastic cells can recapitulate behavior of normal counterparts

CLASSIFICATION•Based on prognosis

WORKING FORMULATION• Low grade
• ML, small lymphocytic• ML, follicular small cleaved cell• ML, follicular, mixed small and large cell
• Intermediate grade:
• ML, follicular, large cell• ML, diffuse, small cleaved cell• ML, diffuse, mixed small and large cell• ML, diffuse, large cell
• High grade
• ML, immunoblastic• ML, lymphoblastic• ML, small non-cleaved cell (Burkitt's vs non-
Burkitt's)
• Miscellaneous (mycosis fungoides, true histiocytic, etc.)
From 1982-1994, the classification used in the United States Based on:
The observed clinical history of 1200 patients.Microsopic examination alone, utilizing
Loss of normal nodal architecture The dominant cytologic cell type observed under the microscopePresence or absence of "follicularity" - mimicking of normal lymphoid follicle formation

CLASSIFICATION- REAL/WHO 2008•REAL/WHO is a "disease” oriented rather than purely morphology
oriented classification, based on:
•Cell lineage: B vs T vs NK vs Histiocytic
•Stage of maturation of the presumed normal counterpart.
• Includes immunologic and molecular criteria in addition to purely
morphologic criteria of WF
•Each disease entity may have differing grades of aggressiveness
•Greatly expanded the list of entities; includes leukemias of
lymphoid origin

B-Cell Neoplasms T/NK-Cell Neoplasms Hodgkin's LymphomaPrecursor B-cell lymphoblasticleukemia/lymphoma
Precursor T cell lymphoblasticleukemia/lymphoma
Lymphocyte predominance,nodular
Peripheral B-cell neoplasms Peripheral T-cell and NK-cellneoplasms
Classical HL
B-cell CLL/SLL Predominantlyleukemic/disseminated
Lymphocyte rich classical HL
B-cell prolymphocytic leukemia T-cell prolymphocytic leukemia Nodular sclerosisLymphoplasmacytic lymphoma T-cell large granular lymphocytic
(LGL) leukemia Mixed cellularity
Mantle cell lymphoma NK cell leukemia Lymphocyte dep letionFollicular lymphoma Adult T-cell leukemia/lymphoma Unclassifiable classical HLExtranoda l marginal zone B-cell lymphoma, MALT type (+/-monocytoid B cells)
Predominantly nodalAngioimmunoblastic T-celllymphoma
Nodal marginal zone B-celllymphoma (+/-monocytoid Bcells)
Peripheral T-cell lymphomaunspecified
Splenic marginal zone B-celllymphoma (+/-villouslymphocytes)
Anaplastic large cell lymphoma,T/null-cellPredominantly extranodal
Hairy cell leukemia Mycosis fungoidesDiffuse large B-cell lymphoma Sezary syndrome
Burkitt lymphoma Primary cutaneous (CD30+ T- celllymphoproliferative disorders)
Plasma cell myeloma Subcutaneous panniculitis-like T-cell lymphoma
Plasmacytoma NK/T cell lymphoma, nasal andnasal-typeEnteropathy -type intestinal T-celllymphomaHepatosplenic T-cell lymphoma g/d (gamma/delta) a/b (alpha/beta )

MAJOR LYMPHOID NEOPLASMS OF LYMPH NODES• i. Mantle cells/Mantle zone – Mantle cell lymphomas• Ii. Germinal centre Follicular lymphomas Burkitt’s lymphomas DLBCL HLiii. Marginal zone DLBCL Marginal zone lymphomas Small lymphocytic lymphoma Chronic lymphocytic leukemiaiv. Peripheral T cells Peripheral T cell lymphomasV. Paracortical regions – Anaplastic large cell lymphomas



CLINICAL FEATURES•Lymphadenopathy•Pain +/-•Weight loss >10% body weight•Fever>38^C•Night sweats•Malaise•Pruritis•Frequent Infections
‘B symptoms”

FNAC OF LYMPHOMAS•Indications• for metastasis•recurrences and deep seated lymphomas •C/I• for primary lymphomas

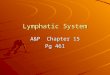
LYMPHOMA REACTIVE HYPERPLASIA
K/L K/L

METASTATIC SCC
LYMPHOMA
CYTOKERATIN

FNAC EVALUATION•Quick stain –cytomorphology••Flow/immunocytochemistry••Proliferation Indexes••Cytogenetics
http://www.mayoclinic.org/cond/lymphoma/fnac/con-20035937

MANTLE CELL LYMPHOMA•DEFINITION•CD5+ B cell malignant lymphoma with chromosomal translocation t(11:14), rearranged Bcl-1 gene, Cyclin D1 overexpression and cytologic features intermediate between small lymphocytic lymphoma and follicular lymphoma.
•SYNONYMS•Intermediate lymphocytic lymphoma/centrocytic lymphoma/SC cell lymphoma
•ORIGIN•Primary Follicles•Mantle zone of secondary follicles

C/F•60-63 YRS
•M:F=2:1 TO 5:1
•Generalised lymphadenopathy
•B symptoms-Weight loss/fever/night sweats
•Early dissemination- most cases late stage with spleen & BM involvement during diagnosis
•Extranodal sites-Waldeyer’s ring, SG,spleen,GIT
•Intermediate grade lymphoma

H/P•Small to med sized lymphocytes with irregular nuclear contours, condensed chromatin, inconspicuous nucleoli and scanty cytoplasm
•Nucleus not as round as SLL nor as cleaved as FL•SLL and F type cells <30%•Immunoblasts – rare/absent•Moderate mitotic rate•Venules with hyalinised walls•Non neoplastic plasma cells•Epitheloid histiocytes


VARIANTS•Mantle zone•Nodular•Diffuse•Blastic

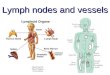
MANTLE ZONE PATTERN

NODULAR PATTERN

DIFFUSE PATTERN

BLASTIC VARIANT

IHC•B cell markers•CD5, CD43•Cyclin D1•Bcl-1Rx & PrognosisSurgery,Chemotherapy, RadiationVery poor prognosis in case of- Increased proliferation rate P53 mutation P16 inactivation Blastic variantMedian survival time- 3-4 yrs

FOLLICULAR LYMPHOMA•DEFINITION•Lymphomas composed of cleaved and non cleaved B cells recapitulating the germinal centres of lymphoid follicles and growing in a nodular pattern
•SYNONYMS•Nodular lymphosarcoma/Germinal centre lymphoma/Nodular lymphoma/Brill Symmer’s disease
•ORIGIN•Naïve B cells of germinal centre

C/F•Most common lymphoma after DLBCL•Tumor of old age•No male predominance as in other lymphomas•Indolent disease, insidious onset•Cervical and inguinal LN are most common sites•Late Diagnosis with dissemination into BM,Liver,GIT

H/P•Obliteration of normal LN architecture by nodules of uniform size and shape involving cortex and medulla
•Involvement of perinodal fibroadipose tissue•Total/ partial occupation of LN with nodules which sometimes lack mantle zone-blurring of borders
•Closely packed nodules with little uninvolved tissue between them
•Monotonous monoclonal population•Also forms nodular pattern if it metastasizes to other site.



GRADING•Grade I- predominant small cleaved cell type•Grade II- mixed small cleaved and large cell•Grade III- predominant large cell type
AGGRESSIVE TRANSFORMATIONTo aggressive diffuse lymphomas usually after 6 months or more of initial diagnosisCan transform to DLBCL,BL,Diffuse mixed lymphoma or immunoblastic lymphoma

Signet ring lymphomas•Rare variant of FL•Nodular/combined nodular and diffuse pattern•Signet ring cells•Intracytoplasmic inclusions- IIIr to Russel bodies c/d Dutcher bodies

IHC for FLB cell markers-CD19,CD20,CD22,CD79Bcl-2 overexpressionCD5-
Rx & Prognosis Responsive to radiation and chemotherapyRemission for avg of 19 yearsTendency for aggressive transformation

BURKITT’S LYMPHOMA•Non Hodgkin’s B cell lymphoma of small noncleaved cell type, associated with EBV infection
•Ist lymphoma in which cytogenetic abnormality was detected
•Variants•Burkitt’s•Non Burkitt’s•Endemic to Africa•Associated EBV infection in 90% cases•Increased incidence in AIDS

Pathogenesis•Immortalisation of EBV in B lymphocytes of infected patients
•Continuous stimulation of lymphocytes by EBV bearing B cells
•Reciprocal chromosomal translocation 8:14
•Rapid tumor growth with increased growth fraction and short doubling time

C/F•Mean age – 7 years•M:F=2:1•Jaw/ orbital bone -60% cases•LN- abdominal followed by cervical•AIDS associated – CNS involvement

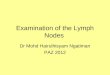
HP/F•Starry sky appearance- monomorphic neoplastic lymphoid cells interspersed with histiocytes
•Tumor cells with uniform size-smaller than centroblasts, larger than lymphocytes
•Thin rim of basophilic cytoplasm,small lipd vacuoles•Increased mitosis- 4% of tumor cells•Doubling time of 24-48 hrs•Cellular necrosis,phagocytic histiocytes


Non Burkitt’s variant•Lacks monotony of BL•Lesser TBM•Less evident starry sky pattern•Moderate pleomorphism

IHC• IgM with Kappa & Lambda chains•B cell markers +•EBV demonstration in situ
RX & PROGNOSIS•Usually poor prognosis•Cyclophosphamide+Methotrexate-Good regression

DIFFUSE LARGE B CELL LYMPHOMA•Heterogenous group of neoplasms characterized by a diffuse proliferation of large neoplastic B lymphoid cells, with nuclear size at least twice that of a small lymphocyte.
• Some are of follicle centre cell origin. It is unclear which combination of positivity for CD10, bcl-2 & bcl- 6and t(14;18) may indicate derivation from a follicle centre cell, either de novo or by transformation.
•Most common lymphoma•Male predominance•Mean age 60 years•Genetics- Dysregulation of bcl-6, t(14:18) translocation•Rapidly enlarging mass, aggressive•Common site- Waldeyer’s ring, oropharyngeal lymphoid tissue

H/P•Large cell size-4-5 times diameter of normal lymphocytes
•Diffuse pattern•Round/oval nucleus which appears vesicular•Anaplastic tumors may contain MNGC resembling RS cells


IHC•CD19+,CD20+•CD10,Bcl-6- variable expression
Rx & PROGNOSIS•Rapidly fatal without treatment•Chemotherapy-complete remission in 60% to 80% cases
•Adjuvant therapy with anti CD20 antibody- good response to Rx

MARGINAL ZONE LYMPHOMA•DEFINITION
•Heterogenous group of B cell tumors that arise within lymph nodes, spleen or extranodal tissues.
May arise in SG of sjogren’s syndrome pts, thyroid of pts with Hashimoto’s thyroiditis

H/P
Architectural effacement by atypical centrocyte like cells that infiltrate around reactive B cell follicles in a marginal zone distribution and spread to interfollicular area
May have a pattern resembling Follicular Lymphoma
Monocytoid B cells, Small lymphocytes, plasma cells, centroblasts and immunoblasts in small numbers.



IHC•B cell markers+, Bcl-10+•CD11, Bcl-2 –
•RX AND PROGNOSIS•Chemotherapy and Radiotherapy•Good remission rates-92%

SMALL LYMPHOCYTIC LYMPHOMA/ CHRONIC LYMPHOCYTIC LEUKEMIA
•SML & CLL differ only in the amount of peripheral blood lymphocytosis
•CLL- absolute lymphocyte count >5000/cu.mm
•Less common in Asians
•Mutation of Ig genes
•C/F
•B symptoms
• Ig spike

H/P•Diffuse effacement of LN by small lymphocytes
•Round to irregular nuclei
•Scanty cytoplasm
•Mitotically active cells aggregate at proliferation centres- mostly large lymphocytes- pathognomic feature
•‘Smudge cells” in peripheral smears



IHC•B cell markers+•CD5+
•Rx & Prognosis•Chemotherapy and radiotherapy•CLL- Bone marrow transplant•Intermediate grade neoplasm•Good remission rates

HODGKIN’S LYMPHOMA•DEFINITION
•A lymphoma characterized by a heterogenous cellularity comprising a minority of specific neoplastic cells and a majority of reactive non-neoplastic cells
•C/F
•Age-bimodal distribution;b/w 15-34 yrs & 54 yrs
•M>F
•Less common than NHLs in HIV pts
•Etiology-EBV infection is implicated as R-S cells are EBV+ in 40% to 50% cases

•Cervical and supraclavicular nodes are commonly involved
•Usually contiguous spread
•Non contiguous spread in case of vessel invasion
•Enlarged LN- non painful, non tender
•Immune deficiency symptoms
•B symptoms


CLASSIFICATIONS

HP/F•Cell types
•1. Non neoplastic cells
•Represent immune reaction to neoplastic cellular component
•Lymphocytes with small round nucleus and rare mitoses is predominant
•Majority are CD4+ T cells
•Occasional histiocytes, fibroblasts, immunoblasts, plasma cells, neutrophils and eosinophils are seen
•Eosinophils-constant and characteristic component of NS & MC types- ‘eosinophilic microabscesses’
•Epitheloid granulomas in 10% cases
•Increased no of epitheloid cells in MC type

•2. Neoplastic cells
•Reed Sternberg cells are pathognomic
•Typical cells are 20-60 Microns in dm
•Variable amount of cytoplasm
•Large nuclei with thick nuclear membrane
•2 nuclei- mirror image
•Single prominent eosinophilic nucleolus –owl eye app
•May show multipolar mitoses
•Mononucleated cells with prominent eosinophilc nucleolus-’Hodgkin cell”
•Constitute 1-3% of tumor volume

Origin of RS cells-Theories•1.Transformation of histiocytes/RE cells•Capacity for phagocytosis•CD21+•Fc receptors present•2.From immunoblasts•Ig gene rearrangements in RS cells•CD15+,CD20+•3.Somatic mutation in GC cells•4.EBV RNA identified in some RS cells

RS cell variants•Hodgkins cell- mononuclear•Lacunar variant•Mummified variant•Anaplastic variant•L H cells-pop corn cells

NODULAR SCLEROSIS TYPE•Most common especially in Young women
•Diagnostic criteria•Lacunar cells- single/sheets
•Sclerosis- defining feature- broad interconnecting bands of collagen-originate from capsule and divide LN into nodules of varying sizes and shapes
•RS cells in variable numbers
•Phases- cellular phase to fibrotic phase
•Syncytial Variant of NS -Extreme form of cellular phase-Numerous RS cells and Hodgkin’s cells arranged in clusters and sheets, Central necrosis-Resembles melanoma/metastatic carcinoma


LYMPHOCYTE RICH•Few RS cells and HC within a mass of lymphocytes and only few eosinophils and neutrophils
• Incidence-6%
•Diagnostic-
•<5RScells/hpf
•Bad prognosis
•Survival 2-3 yrs
Post diagnosis

MIXED CELLULARITY•Heterogenous cell population- lymphocytes, plasma cells,histiocytes,eosinophils, HC,Rs cells with Moderate to diffuse fibrosis
•Common in young/elderly/AIDS pts
•Involves whole/large areas of LN
•Total loss of architecture
•Foci of necrosis
•Diagnostic criteria
•5-15 RS & HC/hpf

LYMPHOCYTE DEPLETION
•Most aggressive form of HL, worst prognosis
•Older pts
•Short median survival(4-5 months posr diagnosis)
•Subtypes-
•1. Diffuse Fibrosis
•2. Reticular
•Diagnostic criteria
•RS & HC >15 cells/hpf

Diffuse Fibrosis•Develops spontaneously or as a result of radiation or chemotherapy
•Poorly cellular structureless LN architecture•Normal parenchyma replaced by fibrous tissue, scattered RS cells/residual lymphocytes
•Spindle cells•Bizzare RS cells •Reticular subtype•Hypercellular•Normal LN architecture obliterated by pleomorphic RS cells/variants
•Eosinophils,neutrophils,macrophages•Foci of necrosis, minimal fibrosis•Characteristic capsule/perinodal invasion


NODULAR LYMPHOCYTE PREDOMINANT •Also c/d paragranuloma
•Nodular lymphoproliferation with clinicopathological features of both HL and low grade B cell lymphoma
•2-6% of HL
•Aggressive Transformation to DLBCL has been reported
•Good prognosis
•2 patterns

1. NodularLN architecture replaced by large lymphocytic nodules, larger than seen in reactive follicles/FL and composed entirely of small lymphocytesLH cells-variant of RS cells with vesiculated multilobate nucleus- popcorn cellsEpitheloid cells ,histiocytes 20% cases- enlarged follicles with increased B cells of mantle zone type-progressive transformation of Germinal centres (PTGC zones-pathognomic)2.Diffuse- Rarely seenLH cells scattered without nodule formation


IHC•RS cells & variants-•CD15+,CD30+•CD45-,CD20-,EMA-, B cell markers-•LP nodular type-•LH cells- CD45+, B cell markers+
•TREATMENT •Surgery ,Chemotherapy,Radiotherapy

UNCLASSIFIABLE LYMPHOMAS•Cannot be defined by combine morphologic, immunohistochemical and genetic investigations

PRIMARY NONHEMATOLYMPHOID TUMORS OF LN•A. Stromal•Hemorrhagic spindle cell tumor•Angiomyolipoma•lymphangiomyoma•Intranodal leiomyoma•Inflammatory pseudotumor
•B. Vascular•Kaposi’s sarcoma•Hemangioma, epithelioid hemangioendothelioma,and angiosarcoma
•Lymphangioma
•C. Benign Epithelial and nevus inclusions- no atypia

METASTATIC NEOPLASMS IN LN
•Most common metastatic tumor in H&N region- SCC
•Others-Malignant melanoma, Thyroid Ca,
•Emreyonic small cell Ca, Adenocarcinoma,
•Renal clear cell Ca.
•HN Sarcomas almost always metastasize to LN
•The metastatic tumor often starts as isolated cellular clusters in the subcapsular sinuses, with gradual replacement of the nodal parenchyma. may be accompanied by a desmoplastic reaction or inflammatory reaction including granuloma formation.
•Discrete metastasis – IHC panel
•Treatment modalities depend on nature of primary tumor

REFERENCES•Chaurasia.Human Anatomy vol3.4th Ed. CBS India•Ham A W., Cormack DH. Ham's Histology. Philadelphia: Lippincott, 1987.•Elmore SA. Histopathology of the Lymph Nodes. Toxicol Pathol. 2006 ; 34(5): 425–454.
• Ioachim HL, Mederios JL. Ioachim’s Lymph node pathology.4th Ed.Lippicott Willians & Wilkins. Philadelphia;2009
•Gnepp DR. Diagnostic Surgical Pathology of Head and Neck.Elseiver Saunders.Philadelphia 2011
•www.pathologyoutlines.com•Kumar, Abbas,Aster.Robbins & Cotran Pathologic Basis of Disease,Vol1.Elseiver Saunders.India;2014
•Robbin’s atlas of pathology.Elseiver Saunders.Massachusetts.2005•Yamaguchi et al. De Novo CD5+ Diffuse Large B-Cell Lymphoma: Results Of A Detailed Clinicopathological Review In 120 Patients. Haematologica August 2008 93: 1195-1202
•Fletcher. Diagnostic Histopathology of tumors.Elseiver Saunders;Philadelphia.2013