Embed Size (px)
Citation preview
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Supported by an independent educational grant from Lundbeck, Inc.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.2
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
This is a CME certified activity.To earn credit for this activity visit:
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Target AudienceThis activity is intended for neurologists, primary care providers, cardiologists, nurses, and pharmacists who care for patients with autonomic disturbances.
GoalThe goal of this activity is to improve physicians’ knowledge and competency in diagnosing and designing appropriate treatment regimens for patients with neurogenic orthostatic hypotension (nOH).
Learning ObjectivesUpon completion of this activity, participants will be able to:1. Identify patients at higher risk for nOH and list the factors that elevate risk2. Discuss the diagnostic criteria and patient presentation for nOH3. Evaluate the evidence for available and emerging treatments for nOH to integrate new therapies into patient management strategies
Credits AvailablePhysicians - maximum of 0.50 AMA PRA Category 1 Credit(s)™
Accreditation StatementsFor Physicians Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
Medscape, LLC designates this enduring material for a maximum of 0.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Instructions for Participation and CreditThere are no fees for participating in or receiving credit for this online educational activity. For information on applicability and acceptance of continuing education credit for this activity, please consult your professional licensing board. This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity online during the valid credit period that is noted on the title page. To receive AMA PRA Category 1 Credit™, you must receive a minimum score of 75% on the post-test. Follow these steps to earn CME/CE credit*:1. Read the target audience, learning objectives, and author disclosures.2. Study the educational content online or printed out.3. Online, choose the best answer to each test question. To receive a certificate, you must receive a passing score as designated at the top of the test. We encourage you to complete the Activity Evaluation to provide feedback for future programming.
CME Released: 12/04/2014; Valid for credit through 12/04/2015

www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.3
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannot alter it. Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time period you can print out the tally as well as the certificates from the CME/CE Tracker. *The credit that you receive is based on your user profile.
Hardware/Software RequirementsTo access activities, users will need:· A computer with an Internet connection.· Internet Explorer 8.x or higher, the latest versions of Firefox or Safari, or any other W3C standards compliant browser.· Adobe Flash Player and/or an HTML5 capable browser may be required for video or audio playback.· Occasionally other additional software may be required such as PowerPoint or Adobe Acrobat Reader.
Faculty and DisclosuresAs an organization accredited by the ACCME, Medscape, LLC, requires everyone who is in a position to control the content of an education activity to disclose all relevant financial relationships with any commercial interest. The ACCME defines “relevant financial relationships” as financial relationships in any amount, occurring within the past 12 months, including financial relationships of a spouse or life partner, that could create a conflict of interest.
Medscape, LLC, encourages Authors to identify investigational products or off-label uses of products regulated by the US Food and Drug Administration, at first mention and where appropriate in the content.
Robert A. Hauser, MD, MBA
Professor of Neurology, Molecular Pharmacology, and Physiology; Director, USF Health Byrd Parkinson’s Disease and Movement Disorders Center of Excellence, National Parkinson Foundation Center of Excellence, Tampa, Florida
Disclosure: Robert Hauser, MD, MBA, has disclosed the following relevant financial relationships: Served as an advisor or consultant for: AbbVie Inc.; Allergan, Inc.; Auspex Pharmaceuticals; AstraZeneca Pharmaceuticals LP; Biotie Therapies Corp; Ceregene; Chelsea Therapeutics, Inc.; Cleveland Clinic; GE Healthcare; Gerson Lehrman Group; GLG Pharma, LLC; HealthLogiX; IMPAX Laboratories, Inc.; Indus Pharma; Ipsen; Lilly; Lundbeck, Inc.; Merck & Co., Inc.; Merck Sharp & Dohme Corp.; Noven Pharmaceuticals, Inc.; Pfizer Inc; Pricespective; Strakan Pharmaceuticals Ltd; Targacept, Inc.; Teva Neuroscience, Inc.; Teva Pharmaceuticals USA; UCB Pharma, Inc.; Upsher-Smith Laboratories, Inc.; US WorldMeds, LLC; XenoPort, Inc.; Zambon Company SpA Dr Hauser does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States. Dr Hauser does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.

Pg.4
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Horacio Kaufmann, MD
Professor of Neurology and Medicine; Director, Dysautonomia Center, New York University Langone Medical Center, New York, New York
Disclosure: Horacio Kaufmann, MD, has disclosed the following relevant financial relationships: Served as an advisor or consultant for: Lundbeck, Inc. Dr Kaufmann does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States. Dr Kaufmann does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.
William B. White, MD
Professor and Division Chief, Pat and Jim Calhoun Cardiology Center, University of Connecticut Health Center, Farmington, Connecticut
Disclosure: William B. White, MD, has disclosed the following relevant financial relationships: Served as an advisor or consultant for: AstraZeneca Pharmaceuticals LP; Roche; Takeda Pharmaceuticals North America, Inc. Dr White does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States. Dr White does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.
EditorRonald K. Miller, PhDScientific Director, Medscape, LLC
Disclosure: Ronald K. Miller, PhD, has disclosed no relevant financial relationships.
CME ReviewerNafeez Zawahir, MDCME Clinical Director, Medscape, LLC
Disclosure: Nafeez Zawahir, MD, has disclosed no relevant financial relationships.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.5
Robert A. Hauser, MD, MBA: Hello. I’m Robert Hauser from the University of South Florida Parkinson’s Disease and Movement Disorder Center of Excellence in Tampa. Thank you for joining this program on neurogenic orthostatic hypotension (nOH). We will be discussing various features of nOH, including its clinical presentation, important diagnostic considerations, and treatment strategies past and present.

Pg.6
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Dr Hauser: Joining me today are 2 experts in the field, Horacio Kaufmann from New York University in New York City and William White from the Calhoun Cardiology Center, University of Connecticut Health Center in Farmington. Welcome, gentlemen.
William B. White, MD: Thanks. Nice to see you.
Horacio Kaufmann, MD: Thank you, Bob. Nice to see you.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.7
Dr Hauser: Neurogenic orthostatic hypotension is a disorder of noradrenergic neurotransmission. It’s most familiar presentation is lightheadedness or even syncope on standing. We know that the basic mechanism is impaired norepinephrine release from postganglionic sympathetic nerve terminals, resulting in a decrease in blood pressure (BP) and reduced blood flow to vital organs, especially the brain, when one stands. Orthostatic hypotension (OH) is defined as a fall in systolic BP of at least 20 mm Hg or in diastolic BP of at least 10 mm Hg within 3 minutes of standing. Symptoms may include lightheadedness, dizziness, weakness, fatigue, vision changes, poor concentration, head and neck pain, and difficulty standing.[1] It could be due to an underlying neurologic condition or other factors. To get the conversation going, Billy, what are the non-neurologic causes of OH?

Pg.8
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Dr White: I actually think that is much more common than neurologic causes of hypotension on standing. We get this as a consult in the hospital all the time. The most common thing is clearly volume depletion, whether it was from a previous gastrointestinal bleed or an illness or basically poor fluid intake in an elderly person. Of course, other things to consider are does the person possibly have hypoadrenalism or Addison disease? Hypocorticalism? Are they possibly taking a drug that they forgot they were taking that lowers BP and causes orthostasis? Finally, do they have problems with cardiac function where they might have a little heart failure and cannot mount a good BP rise?[2]
Dr Hauser: In my office, the most common thing I see is actually antihypertensive medications. Horacio, what about causes of nOH?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.9
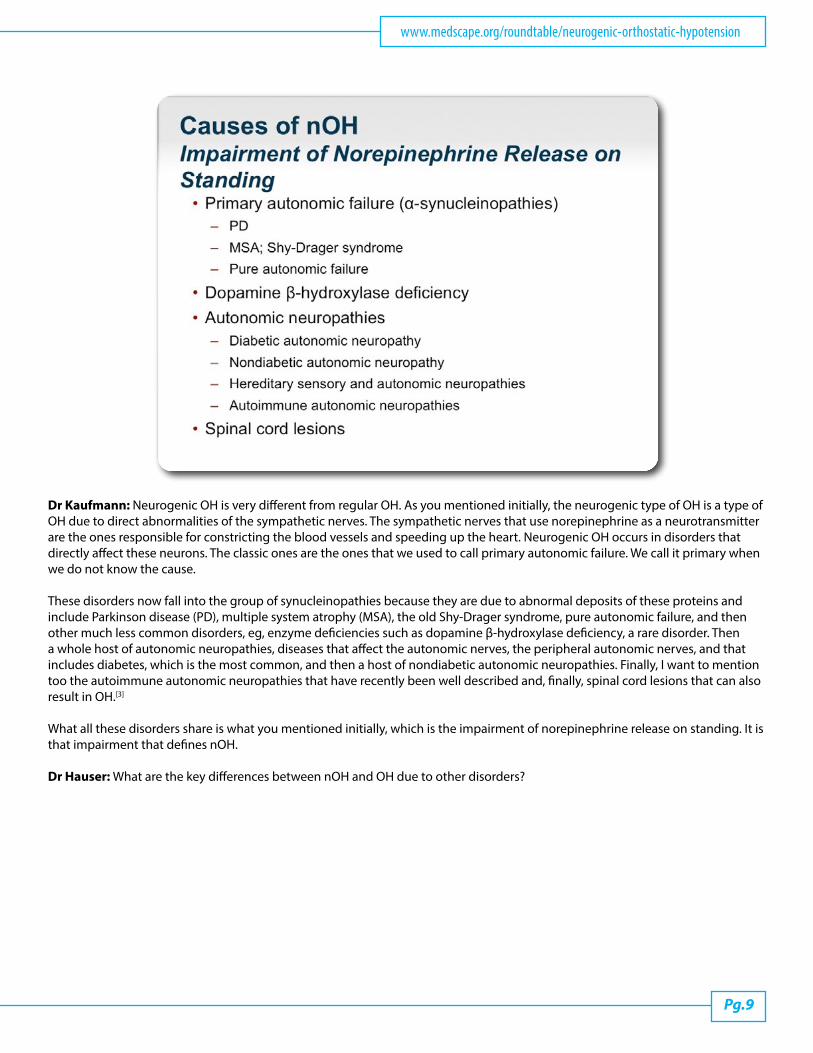
Dr Kaufmann: Neurogenic OH is very different from regular OH. As you mentioned initially, the neurogenic type of OH is a type of OH due to direct abnormalities of the sympathetic nerves. The sympathetic nerves that use norepinephrine as a neurotransmitter are the ones responsible for constricting the blood vessels and speeding up the heart. Neurogenic OH occurs in disorders that directly affect these neurons. The classic ones are the ones that we used to call primary autonomic failure. We call it primary when we do not know the cause.
These disorders now fall into the group of synucleinopathies because they are due to abnormal deposits of these proteins and include Parkinson disease (PD), multiple system atrophy (MSA), the old Shy-Drager syndrome, pure autonomic failure, and then other much less common disorders, eg, enzyme deficiencies such as dopamine β-hydroxylase deficiency, a rare disorder. Then a whole host of autonomic neuropathies, diseases that affect the autonomic nerves, the peripheral autonomic nerves, and that includes diabetes, which is the most common, and then a host of nondiabetic autonomic neuropathies. Finally, I want to mention too the autoimmune autonomic neuropathies that have recently been well described and, finally, spinal cord lesions that can also result in OH.[3]
What all these disorders share is what you mentioned initially, which is the impairment of norepinephrine release on standing. It is that impairment that defines nOH.
Dr Hauser: What are the key differences between nOH and OH due to other disorders?
Pg.10
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Dr White: Horacio did a nice job of outlining the neurogenic causes. It really comes down to what to do to try to potentially rule it out. One of the things that we do in the office is to evaluate the BP supine vs standing. Typically, it is a little more common in nOH to have supine hypertension. It is also more common to have a lower-than-expected rise in heart rate on standing if you have a drop in BP because if somebody is volume depleted or taking a vasodilator, it is very common to get reflex sympathetic tachycardia in the upright position. Of course, the absence of any neurologic diseases, such as PD, diabetes, and so forth, also makes you think of a non-neurologic cause of the OH.
Dr Hauser: The supine hypertension may be there, but it may not be in nOH, as well as the lack of increase in heart rate when you stand up. Those things may help, but they might not be there.
Dr White: That is correct. It is not a 100% phenomena, but it leads you to be more thoughtful of that.
Dr Hauser: Could you say a few more words about supine hypertension? Is that part and parcel of nOH or is it part of the disorder?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.11
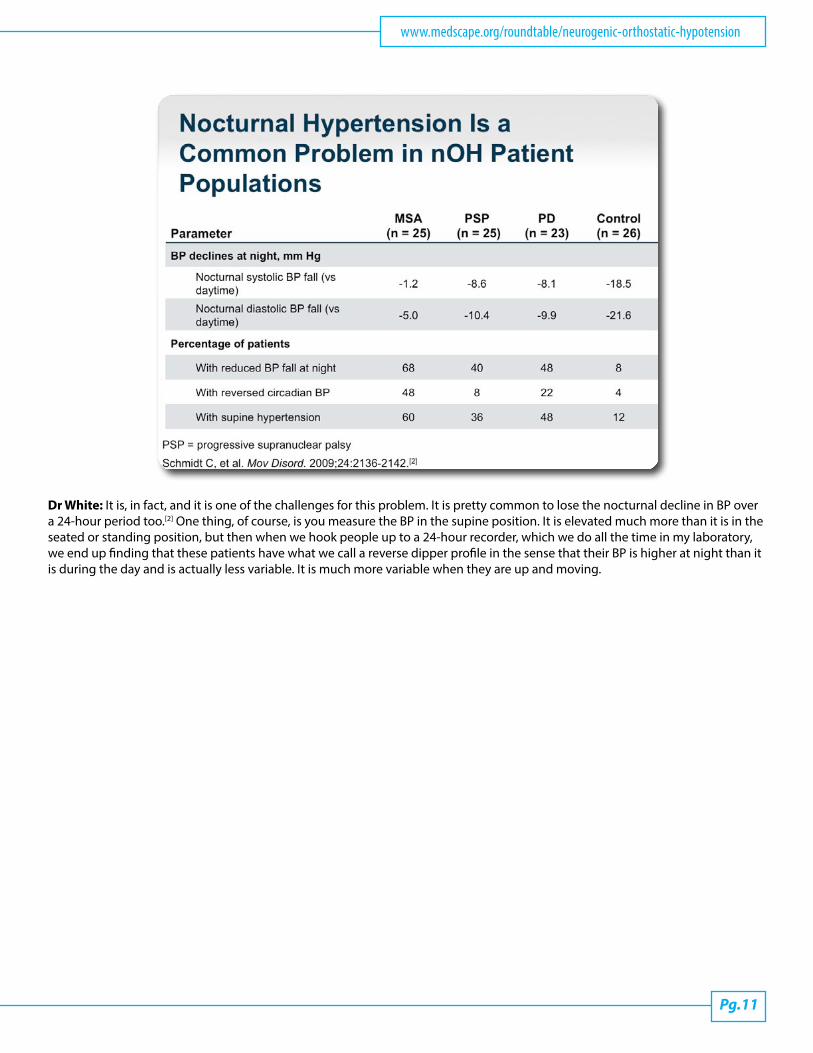
Dr White: It is, in fact, and it is one of the challenges for this problem. It is pretty common to lose the nocturnal decline in BP over a 24-hour period too.[2] One thing, of course, is you measure the BP in the supine position. It is elevated much more than it is in the seated or standing position, but then when we hook people up to a 24-hour recorder, which we do all the time in my laboratory, we end up finding that these patients have what we call a reverse dipper profile in the sense that their BP is higher at night than it is during the day and is actually less variable. It is much more variable when they are up and moving.
Pg.12
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
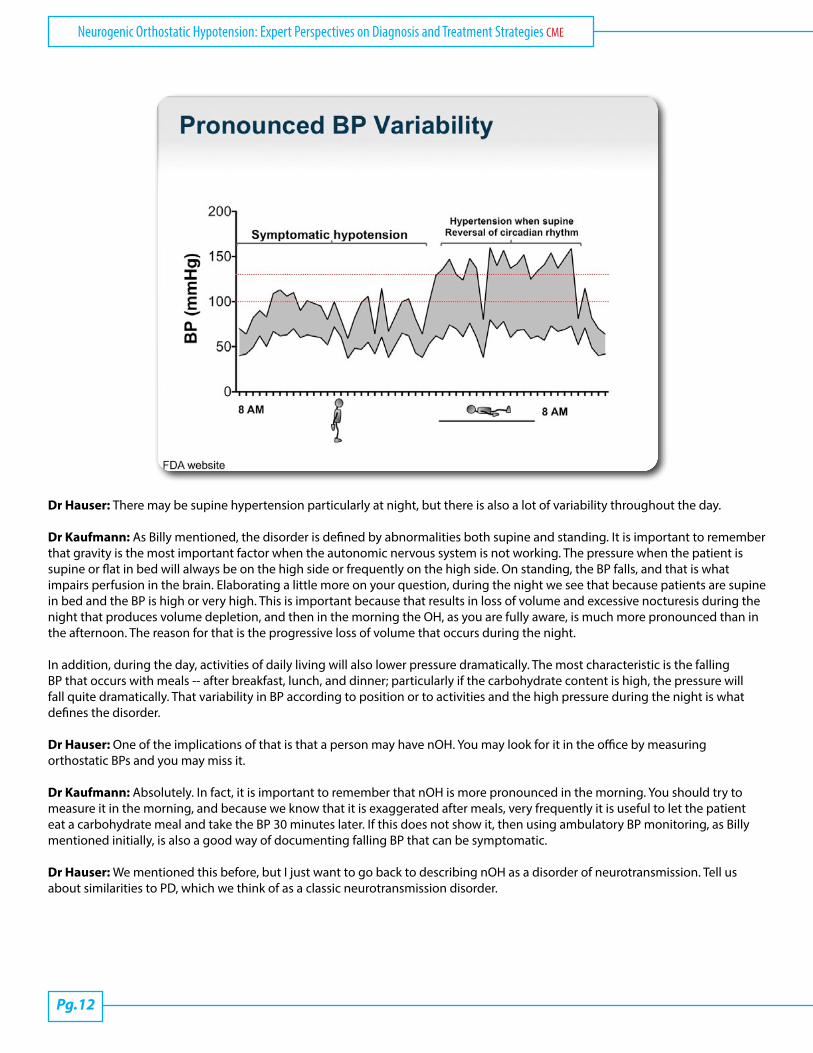
Dr Hauser: There may be supine hypertension particularly at night, but there is also a lot of variability throughout the day.
Dr Kaufmann: As Billy mentioned, the disorder is defined by abnormalities both supine and standing. It is important to remember that gravity is the most important factor when the autonomic nervous system is not working. The pressure when the patient is supine or flat in bed will always be on the high side or frequently on the high side. On standing, the BP falls, and that is what impairs perfusion in the brain. Elaborating a little more on your question, during the night we see that because patients are supine in bed and the BP is high or very high. This is important because that results in loss of volume and excessive nocturesis during the night that produces volume depletion, and then in the morning the OH, as you are fully aware, is much more pronounced than in the afternoon. The reason for that is the progressive loss of volume that occurs during the night.
In addition, during the day, activities of daily living will also lower pressure dramatically. The most characteristic is the falling BP that occurs with meals -- after breakfast, lunch, and dinner; particularly if the carbohydrate content is high, the pressure will fall quite dramatically. That variability in BP according to position or to activities and the high pressure during the night is what defines the disorder.
Dr Hauser: One of the implications of that is that a person may have nOH. You may look for it in the office by measuring orthostatic BPs and you may miss it.
Dr Kaufmann: Absolutely. In fact, it is important to remember that nOH is more pronounced in the morning. You should try to measure it in the morning, and because we know that it is exaggerated after meals, very frequently it is useful to let the patient eat a carbohydrate meal and take the BP 30 minutes later. If this does not show it, then using ambulatory BP monitoring, as Billy mentioned initially, is also a good way of documenting falling BP that can be symptomatic.
Dr Hauser: We mentioned this before, but I just want to go back to describing nOH as a disorder of neurotransmission. Tell us about similarities to PD, which we think of as a classic neurotransmission disorder.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.13
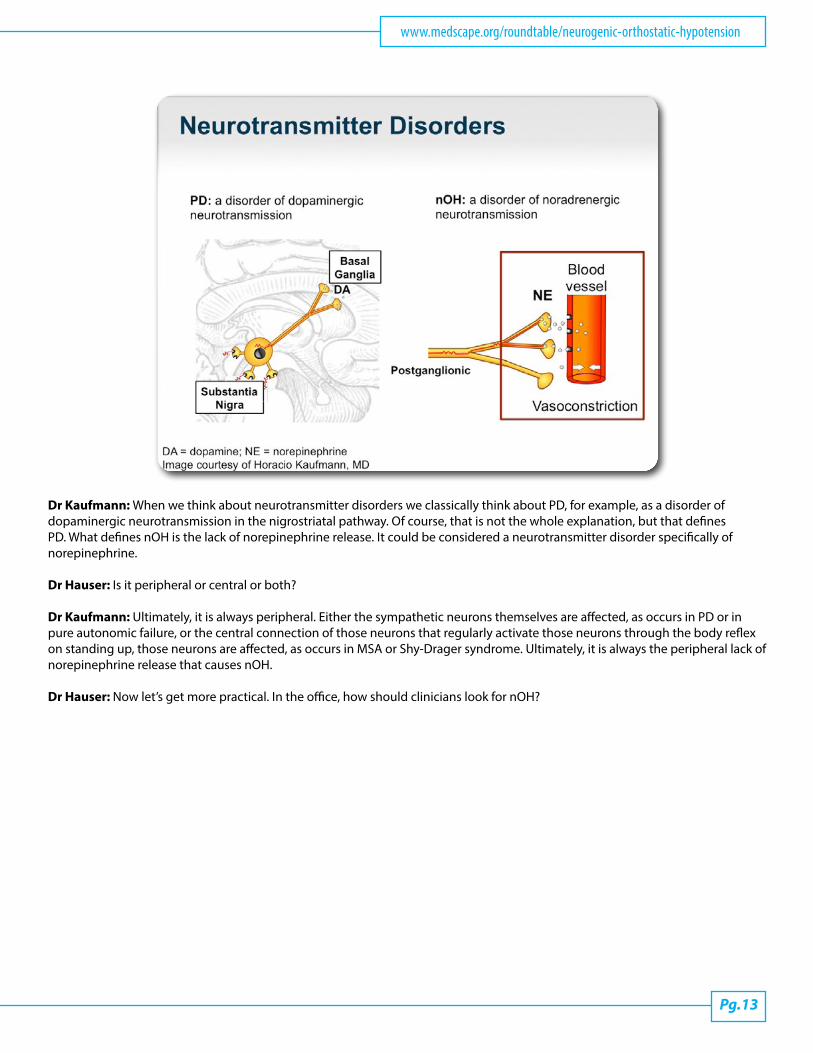
Dr Kaufmann: When we think about neurotransmitter disorders we classically think about PD, for example, as a disorder of dopaminergic neurotransmission in the nigrostriatal pathway. Of course, that is not the whole explanation, but that defines PD. What defines nOH is the lack of norepinephrine release. It could be considered a neurotransmitter disorder specifically of norepinephrine.
Dr Hauser: Is it peripheral or central or both?
Dr Kaufmann: Ultimately, it is always peripheral. Either the sympathetic neurons themselves are affected, as occurs in PD or in pure autonomic failure, or the central connection of those neurons that regularly activate those neurons through the body reflex on standing up, those neurons are affected, as occurs in MSA or Shy-Drager syndrome. Ultimately, it is always the peripheral lack of norepinephrine release that causes nOH.
Dr Hauser: Now let’s get more practical. In the office, how should clinicians look for nOH?
Pg.14
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
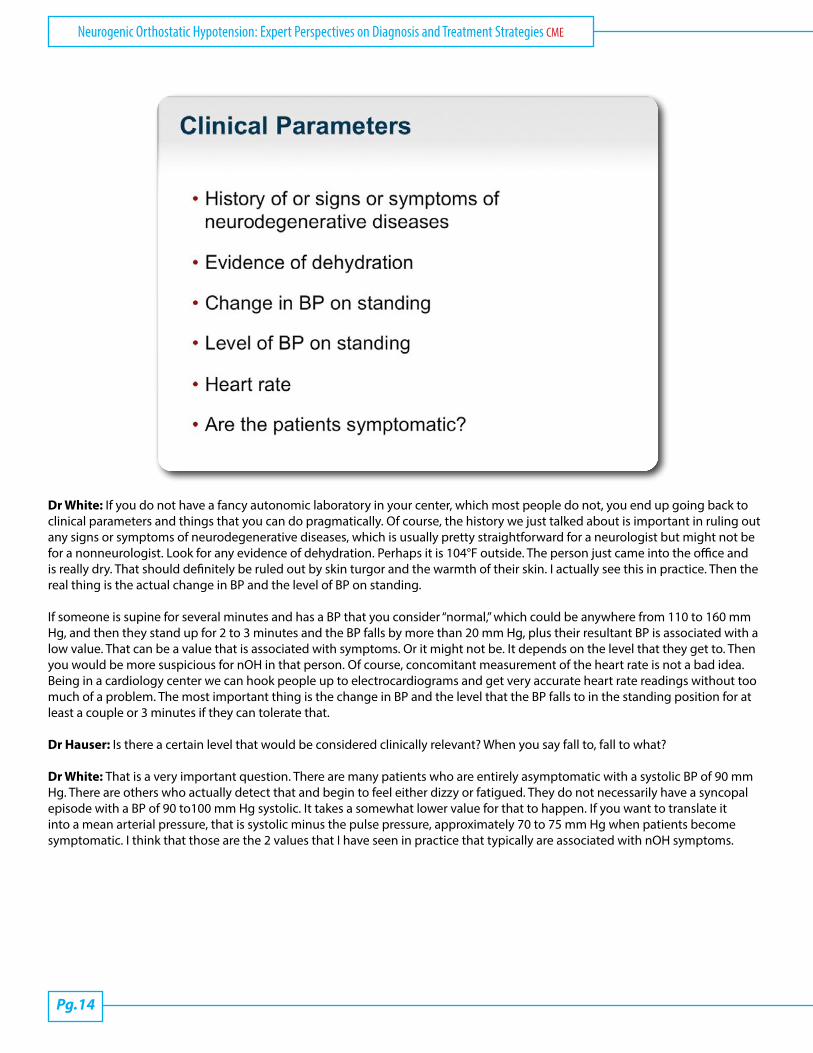
Dr White: If you do not have a fancy autonomic laboratory in your center, which most people do not, you end up going back to clinical parameters and things that you can do pragmatically. Of course, the history we just talked about is important in ruling out any signs or symptoms of neurodegenerative diseases, which is usually pretty straightforward for a neurologist but might not be for a nonneurologist. Look for any evidence of dehydration. Perhaps it is 104°F outside. The person just came into the office and is really dry. That should definitely be ruled out by skin turgor and the warmth of their skin. I actually see this in practice. Then the real thing is the actual change in BP and the level of BP on standing.
If someone is supine for several minutes and has a BP that you consider “normal,” which could be anywhere from 110 to 160 mm Hg, and then they stand up for 2 to 3 minutes and the BP falls by more than 20 mm Hg, plus their resultant BP is associated with a low value. That can be a value that is associated with symptoms. Or it might not be. It depends on the level that they get to. Then you would be more suspicious for nOH in that person. Of course, concomitant measurement of the heart rate is not a bad idea. Being in a cardiology center we can hook people up to electrocardiograms and get very accurate heart rate readings without too much of a problem. The most important thing is the change in BP and the level that the BP falls to in the standing position for at least a couple or 3 minutes if they can tolerate that.
Dr Hauser: Is there a certain level that would be considered clinically relevant? When you say fall to, fall to what?
Dr White: That is a very important question. There are many patients who are entirely asymptomatic with a systolic BP of 90 mm Hg. There are others who actually detect that and begin to feel either dizzy or fatigued. They do not necessarily have a syncopal episode with a BP of 90 to100 mm Hg systolic. It takes a somewhat lower value for that to happen. If you want to translate it into a mean arterial pressure, that is systolic minus the pulse pressure, approximately 70 to 75 mm Hg when patients become symptomatic. I think that those are the 2 values that I have seen in practice that typically are associated with nOH symptoms.

www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.15
Dr Kaufmann: I would emphasize that the most important thing is to measure the BP standing. Measure BP supine, wait 3 minutes, and then measure BP standing. That is perhaps what we should emphasize the most to our neurologic colleagues. Not to only take it supine but take it standing. I fully agree that it is very important not only to consider the drop in BP but also to consider the actual level of BP standing. In other words, the crucial thing is not how much it falls but how low it goes. We recently did a study that is going to come out soon showing similar numbers to what Billy is mentioning. We found that 75 mm Hg of mean BP standing nicely separated patients with and without symptoms. These were all patients with PD. Meaning, if the BP was lower than 75 mm Hg when standing, the patients had symptoms and that may be a good indication to think seriously about treatment.
There are 2 things to consider: diagnosis and treatment. For diagnosis, falling pressure is important. For treatment, it is the actual level of BP standing. That falling pressure can tell you that the patient may eventually develop a neurodegenerative disease. Neurologists are quite aware of the need to identify premotor degenerative diseases. Not infrequently, patients with MSA may have a period in which only the falling BP is what is symptomatic. Many times, identifying that falling BP as a premotor stage of a neurodegenerative disease is important, and for that the 20 mm Hg drop is crucial.
Dr Hauser: I will usually ask patients about symptoms that could be related to nOH, and only if I hear of those, if they get lightheaded when they get up, that is when I do orthostatic BPs. Am I missing the boat there? Do I really need to do it more often than that?
Dr Kaufmann: You are probably right in most cases. There are many patients, particularly with PD, who may have nonspecific symptoms and may not be able to recognize that those symptoms only occur when he or she is standing and are due to nOH. To be on the safe side, it is a good idea for either you or your nurse to measure the BP when the patient is standing because the reverse can also happen and you may think that symptoms that occur only when standing are due to nOH. In fact, they may be due to just garden-variety motor problems in PD. It is important to measure their BP standing.
Dr Hauser: When you say standing, do you mean supine and standing or can I just do it standing?
Dr Kaufmann: If you have to choose 1, I would choose standing.
Dr Hauser: Let’s move on to current treatment options, options that have been around for a long time now. There are some nonpharmacologic treatment options. Billy, can you tell us about those?
Pg.16
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
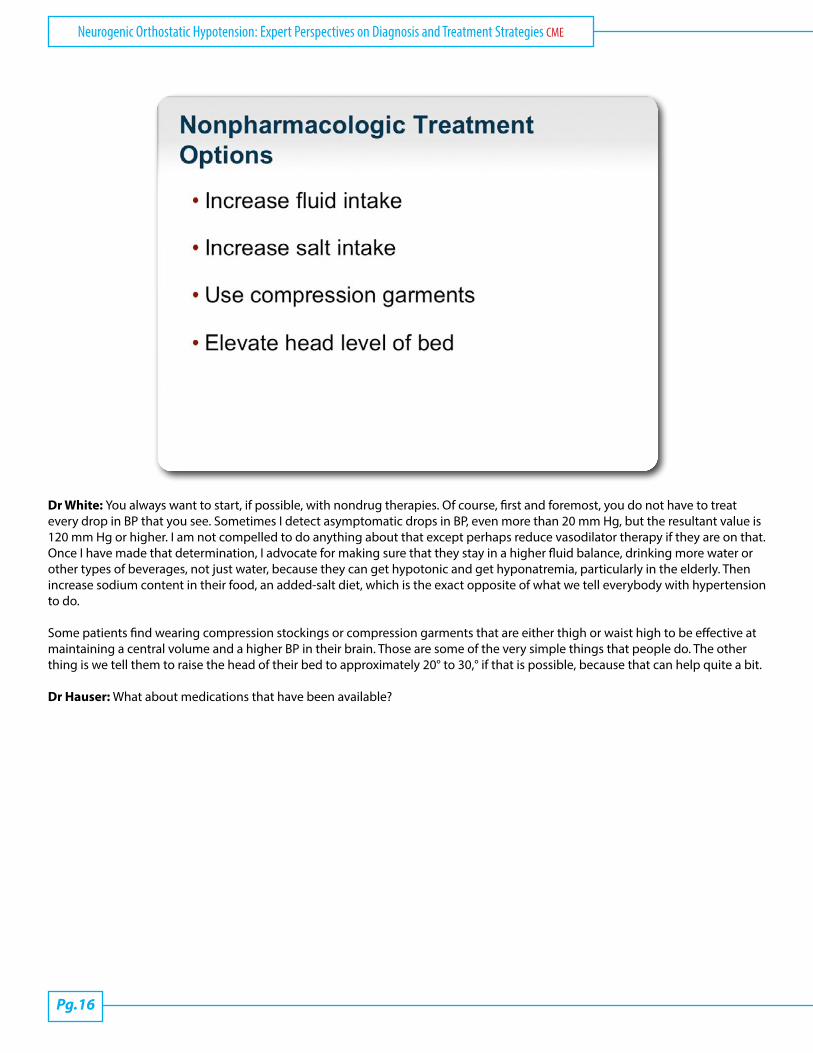
Dr White: You always want to start, if possible, with nondrug therapies. Of course, first and foremost, you do not have to treat every drop in BP that you see. Sometimes I detect asymptomatic drops in BP, even more than 20 mm Hg, but the resultant value is 120 mm Hg or higher. I am not compelled to do anything about that except perhaps reduce vasodilator therapy if they are on that. Once I have made that determination, I advocate for making sure that they stay in a higher fluid balance, drinking more water or other types of beverages, not just water, because they can get hypotonic and get hyponatremia, particularly in the elderly. Then increase sodium content in their food, an added-salt diet, which is the exact opposite of what we tell everybody with hypertension to do.
Some patients find wearing compression stockings or compression garments that are either thigh or waist high to be effective at maintaining a central volume and a higher BP in their brain. Those are some of the very simple things that people do. The other thing is we tell them to raise the head of their bed to approximately 20° to 30,° if that is possible, because that can help quite a bit.
Dr Hauser: What about medications that have been available?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.17
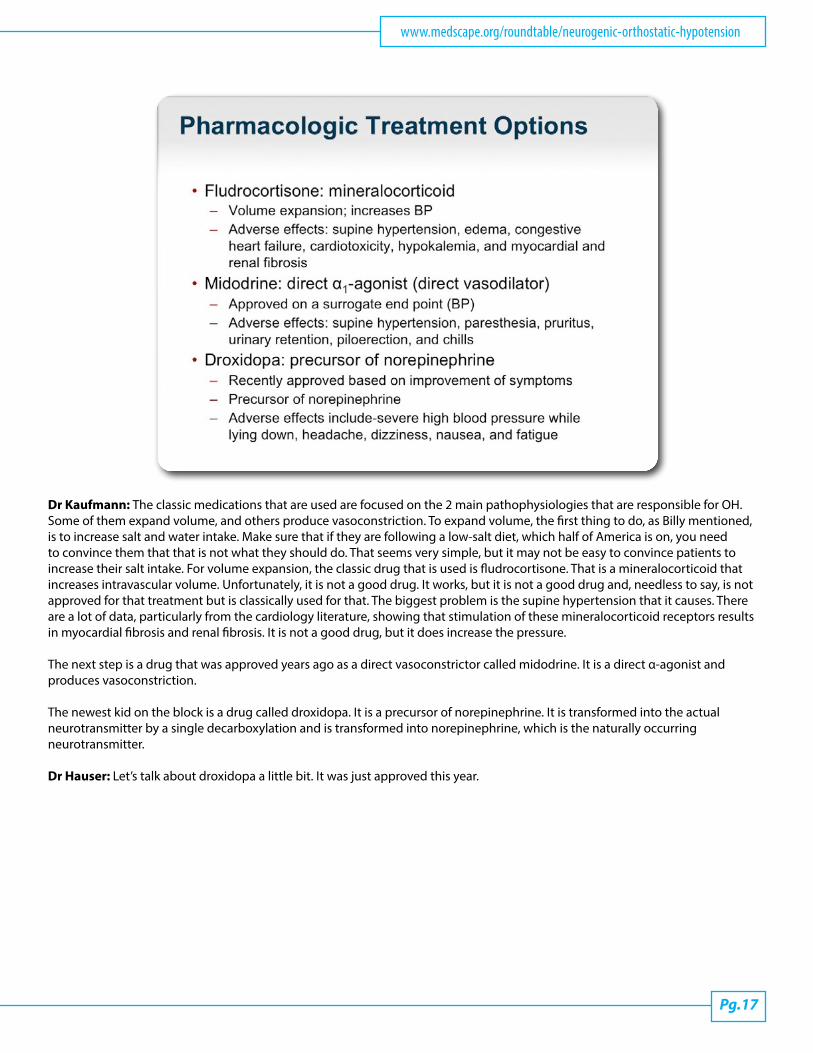
Dr Kaufmann: The classic medications that are used are focused on the 2 main pathophysiologies that are responsible for OH. Some of them expand volume, and others produce vasoconstriction. To expand volume, the first thing to do, as Billy mentioned, is to increase salt and water intake. Make sure that if they are following a low-salt diet, which half of America is on, you need to convince them that that is not what they should do. That seems very simple, but it may not be easy to convince patients to increase their salt intake. For volume expansion, the classic drug that is used is fludrocortisone. That is a mineralocorticoid that increases intravascular volume. Unfortunately, it is not a good drug. It works, but it is not a good drug and, needless to say, is not approved for that treatment but is classically used for that. The biggest problem is the supine hypertension that it causes. There are a lot of data, particularly from the cardiology literature, showing that stimulation of these mineralocorticoid receptors results in myocardial fibrosis and renal fibrosis. It is not a good drug, but it does increase the pressure.
The next step is a drug that was approved years ago as a direct vasoconstrictor called midodrine. It is a direct α-agonist and produces vasoconstriction.
The newest kid on the block is a drug called droxidopa. It is a precursor of norepinephrine. It is transformed into the actual neurotransmitter by a single decarboxylation and is transformed into norepinephrine, which is the naturally occurring neurotransmitter.
Dr Hauser: Let’s talk about droxidopa a little bit. It was just approved this year.
Pg.18
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
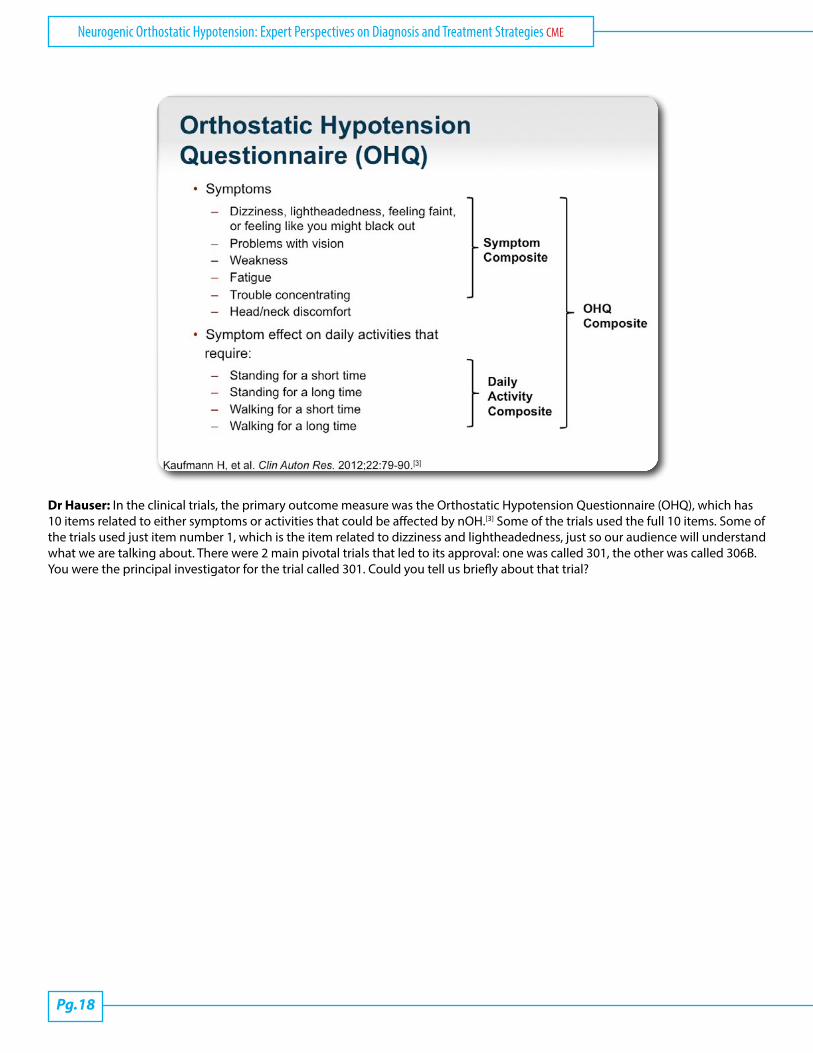
Dr Hauser: In the clinical trials, the primary outcome measure was the Orthostatic Hypotension Questionnaire (OHQ), which has 10 items related to either symptoms or activities that could be affected by nOH.[3] Some of the trials used the full 10 items. Some of the trials used just item number 1, which is the item related to dizziness and lightheadedness, just so our audience will understand what we are talking about. There were 2 main pivotal trials that led to its approval: one was called 301, the other was called 306B. You were the principal investigator for the trial called 301. Could you tell us briefly about that trial?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.19
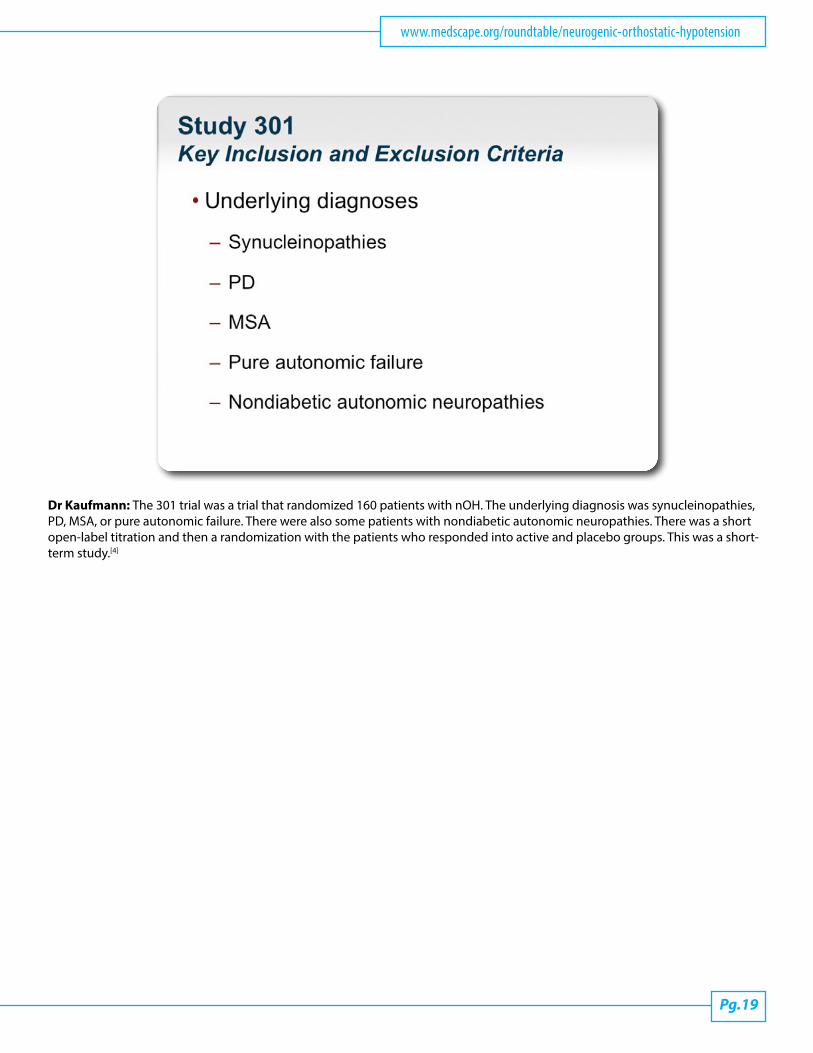
Dr Kaufmann: The 301 trial was a trial that randomized 160 patients with nOH. The underlying diagnosis was synucleinopathies, PD, MSA, or pure autonomic failure. There were also some patients with nondiabetic autonomic neuropathies. There was a short open-label titration and then a randomization with the patients who responded into active and placebo groups. This was a short-term study.[4]
Pg.20
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
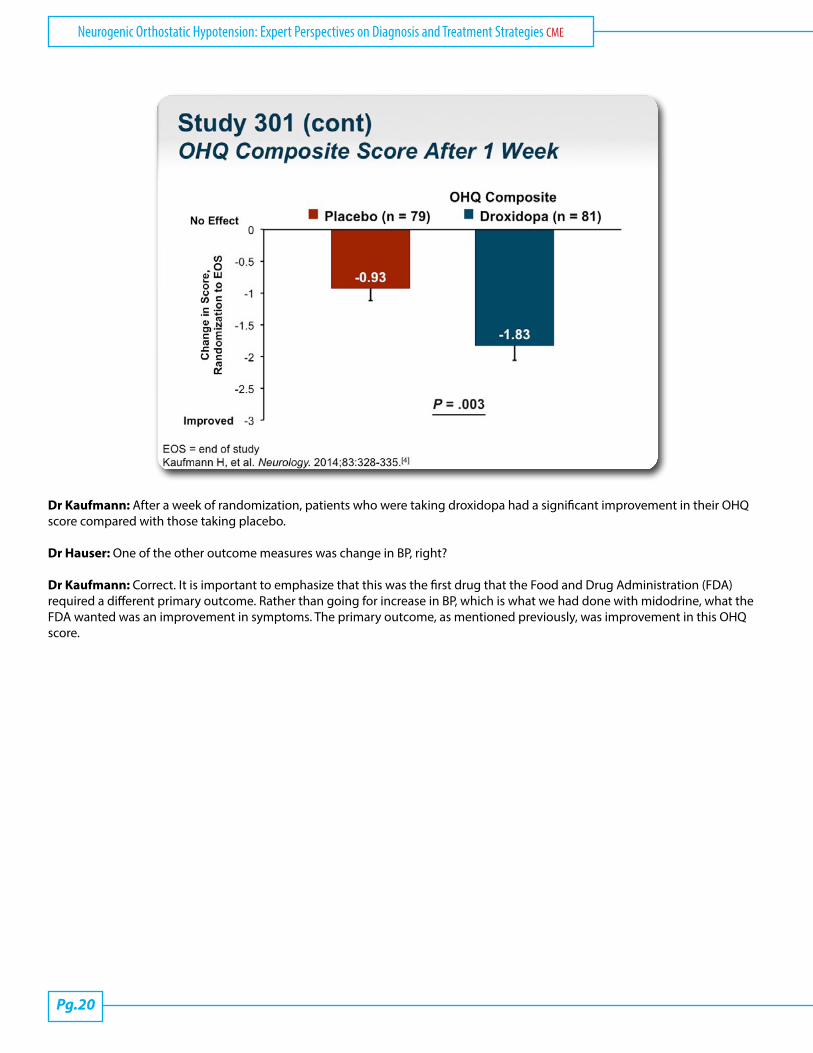
Dr Kaufmann: After a week of randomization, patients who were taking droxidopa had a significant improvement in their OHQ score compared with those taking placebo.
Dr Hauser: One of the other outcome measures was change in BP, right?
Dr Kaufmann: Correct. It is important to emphasize that this was the first drug that the Food and Drug Administration (FDA) required a different primary outcome. Rather than going for increase in BP, which is what we had done with midodrine, what the FDA wanted was an improvement in symptoms. The primary outcome, as mentioned previously, was improvement in this OHQ score.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.21
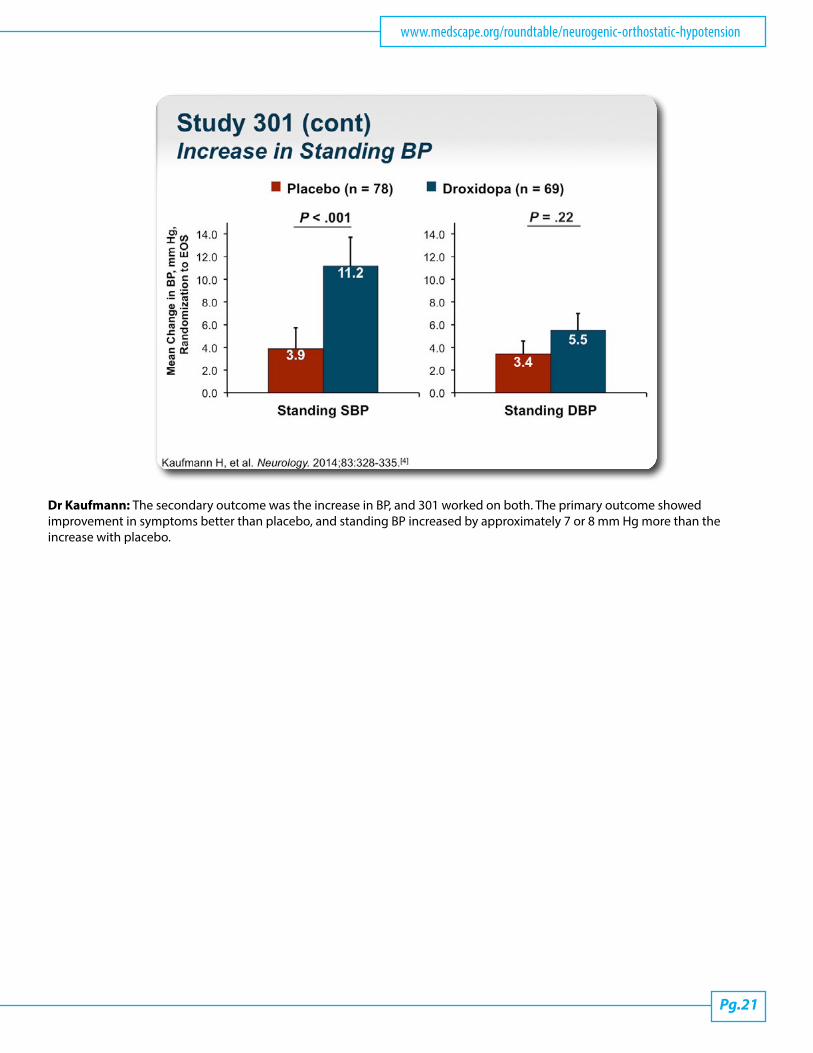
Dr Kaufmann: The secondary outcome was the increase in BP, and 301 worked on both. The primary outcome showed improvement in symptoms better than placebo, and standing BP increased by approximately 7 or 8 mm Hg more than the increase with placebo.
Pg.22
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
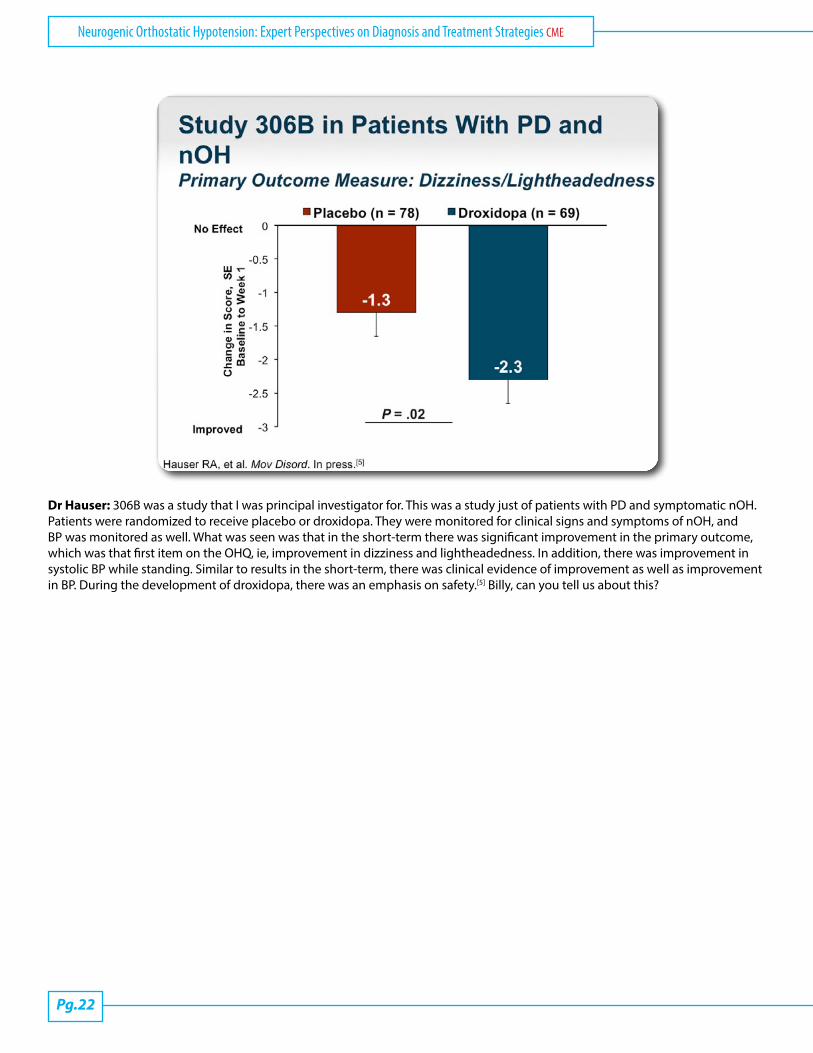
Dr Hauser: 306B was a study that I was principal investigator for. This was a study just of patients with PD and symptomatic nOH. Patients were randomized to receive placebo or droxidopa. They were monitored for clinical signs and symptoms of nOH, and BP was monitored as well. What was seen was that in the short-term there was significant improvement in the primary outcome, which was that first item on the OHQ, ie, improvement in dizziness and lightheadedness. In addition, there was improvement in systolic BP while standing. Similar to results in the short-term, there was clinical evidence of improvement as well as improvement in BP. During the development of droxidopa, there was an emphasis on safety.[5] Billy, can you tell us about this?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.23
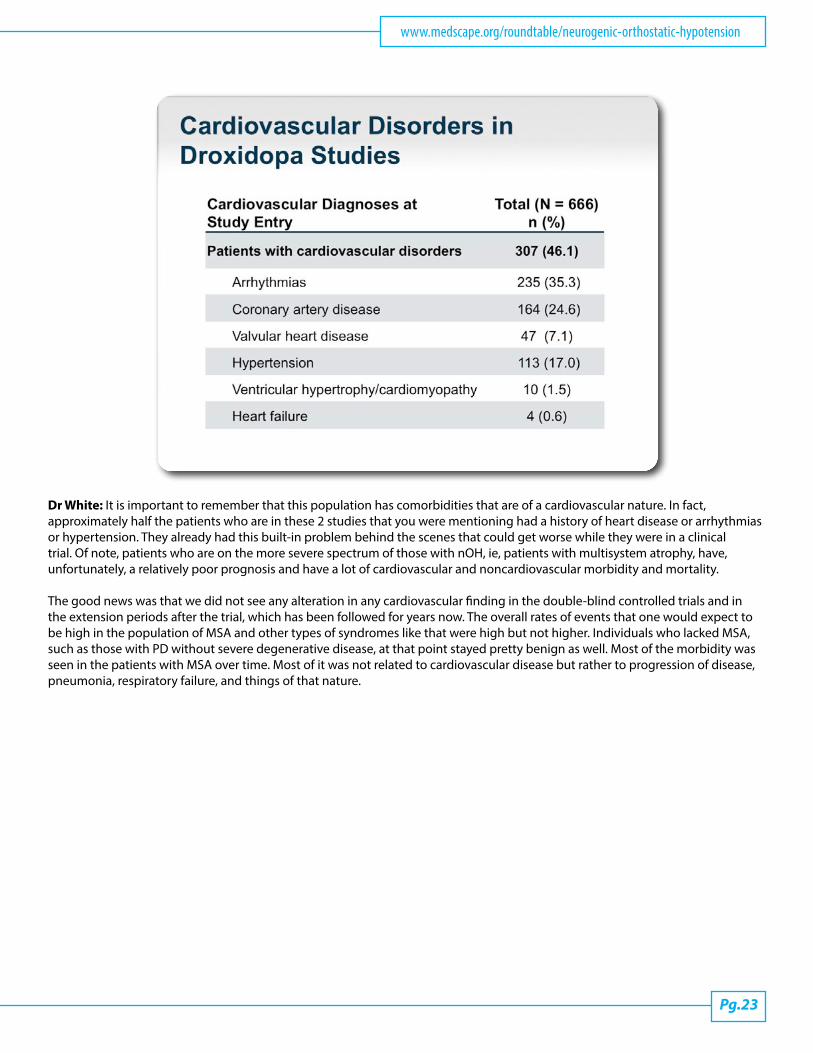
Dr White: It is important to remember that this population has comorbidities that are of a cardiovascular nature. In fact, approximately half the patients who are in these 2 studies that you were mentioning had a history of heart disease or arrhythmias or hypertension. They already had this built-in problem behind the scenes that could get worse while they were in a clinical trial. Of note, patients who are on the more severe spectrum of those with nOH, ie, patients with multisystem atrophy, have, unfortunately, a relatively poor prognosis and have a lot of cardiovascular and noncardiovascular morbidity and mortality.
The good news was that we did not see any alteration in any cardiovascular finding in the double-blind controlled trials and in the extension periods after the trial, which has been followed for years now. The overall rates of events that one would expect to be high in the population of MSA and other types of syndromes like that were high but not higher. Individuals who lacked MSA, such as those with PD without severe degenerative disease, at that point stayed pretty benign as well. Most of the morbidity was seen in the patients with MSA over time. Most of it was not related to cardiovascular disease but rather to progression of disease, pneumonia, respiratory failure, and things of that nature.
Pg.24
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
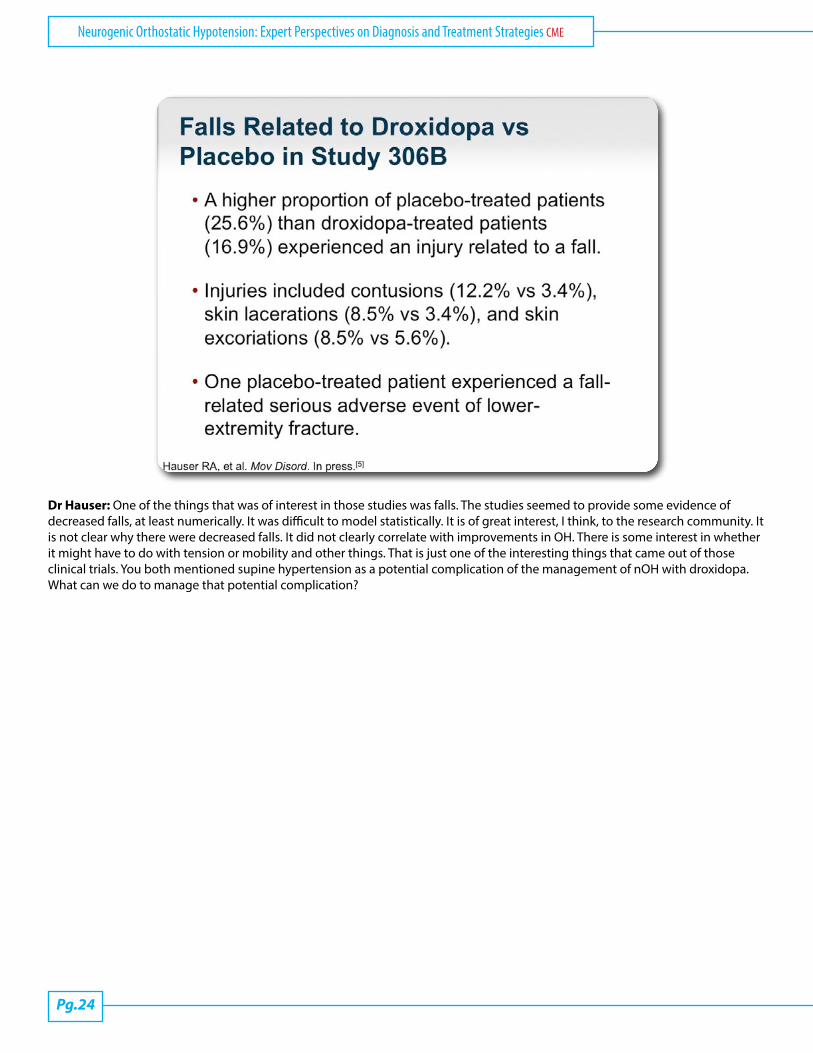
Dr Hauser: One of the things that was of interest in those studies was falls. The studies seemed to provide some evidence of decreased falls, at least numerically. It was difficult to model statistically. It is of great interest, I think, to the research community. It is not clear why there were decreased falls. It did not clearly correlate with improvements in OH. There is some interest in whether it might have to do with tension or mobility and other things. That is just one of the interesting things that came out of those clinical trials. You both mentioned supine hypertension as a potential complication of the management of nOH with droxidopa. What can we do to manage that potential complication?
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.25
Dr White: I get consulted for this problem on a regular basis. It is a tough thing to do actually. It is a clinical challenge because on the one hand you are giving a pressor agent that improves the quality of life of patients, makes them less dizzy and lightheaded during the daytime, and improves their standing BP, all the things that you want from the drug. Occasionally, the consequences are also negative if the BP when they are supine goes up. Of course, in this population it already happens. In fact, we did not see a dramatic increase in supine hypertension with droxidopa relative to placebo. It was more in the mild to moderate increases. I typically would treat that with avoiding giving the drug too late at night so that they are not taking it right before they are going to be supine anyway, and in the worst case scenario, using a small dose of a short-acting antihypertensive drug to mitigate the hypertension that is developing when they are supine. Particularly if there is a benefit that is being obtained, I am not going to stop the drug because of a BP elevation when they are in the supine position.

Pg.26
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Dr Hauser: Droxidopa is now approved, and it is available to treat such patients. I just want to mention a few key points on the label. It is indicated for the treatment of symptomatic nOH, so we do not just treat BP changes.[6] Number 2, it is important to evaluate efficacy and that means evaluating ongoing efficacy, but it is also important to monitor for supine hypertension. If the BP is too high when patients are supine, treat it or make other changes to avoid that potential problem.
I have a few frequently asked questions. Can it be used with fludrocortisone and midodrine?
Dr White: We have no information on the concomitant use of droxidopa with midodrine. In fact, in the studies, patients could not continue taking midodrine if they were going to start taking droxidopa. Considering that they are both vasoconstrictors, that was considered potentially a safety issue or certainly a confounder in the ability to understand what droxidopa was doing vs what midodrine might be doing. On the other hand, a volume expander, such as fludrocortisone, salt, stockings, all those things are probably reasonable background therapy for patients who would be considered initiated on droxidopa, and it would be appropriate to use it in combination with those other therapies.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.27
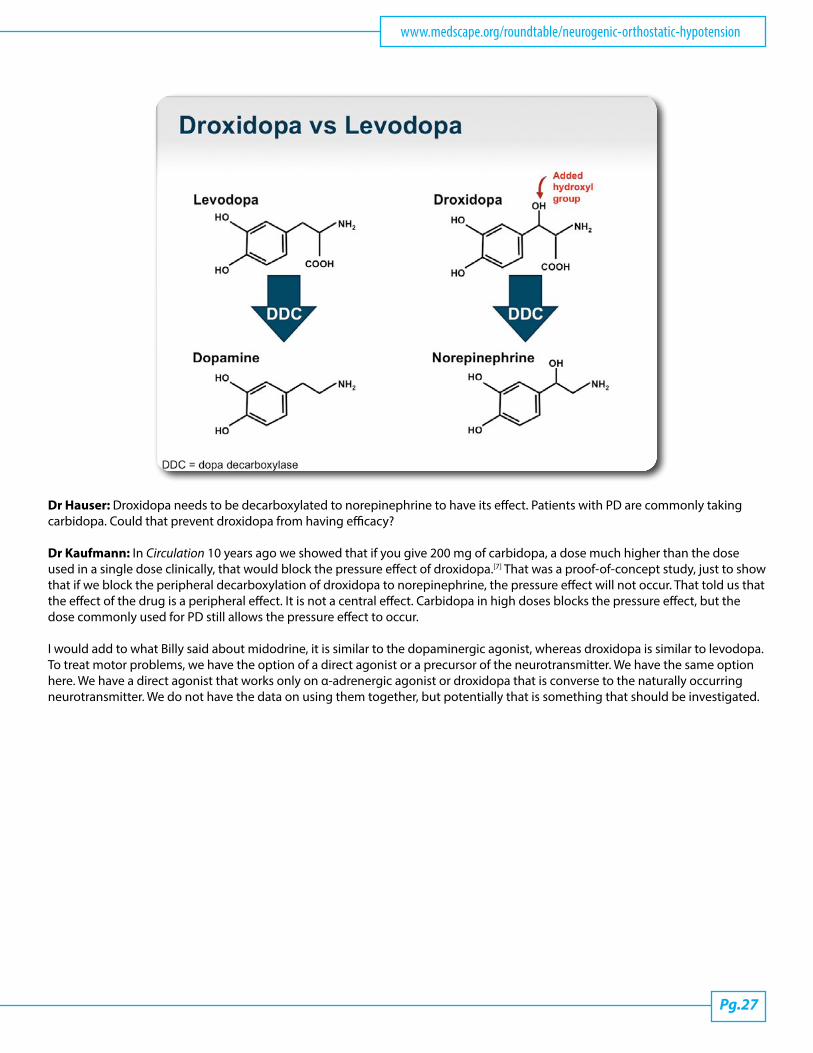
Dr Hauser: Droxidopa needs to be decarboxylated to norepinephrine to have its effect. Patients with PD are commonly taking carbidopa. Could that prevent droxidopa from having efficacy?
Dr Kaufmann: In Circulation 10 years ago we showed that if you give 200 mg of carbidopa, a dose much higher than the dose used in a single dose clinically, that would block the pressure effect of droxidopa.[7] That was a proof-of-concept study, just to show that if we block the peripheral decarboxylation of droxidopa to norepinephrine, the pressure effect will not occur. That told us that the effect of the drug is a peripheral effect. It is not a central effect. Carbidopa in high doses blocks the pressure effect, but the dose commonly used for PD still allows the pressure effect to occur.
I would add to what Billy said about midodrine, it is similar to the dopaminergic agonist, whereas droxidopa is similar to levodopa. To treat motor problems, we have the option of a direct agonist or a precursor of the neurotransmitter. We have the same option here. We have a direct agonist that works only on α-adrenergic agonist or droxidopa that is converse to the naturally occurring neurotransmitter. We do not have the data on using them together, but potentially that is something that should be investigated.
Pg.28
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
Dr Hauser: Maybe evaluated in the future. OK. Great. Just an overall summary then for droxidopa. Droxidopa at doses of 100 to 600 mg 3 times a day results in clinical improvements that translate into meaningful benefits for patients with nOH. It seems to have an acceptable safety profile, especially considering that some patients have potentially disabling features from that disorder, but it is important to monitor its ongoing efficacy and potential adverse effects, especially the supine hypertension.
With that, I would like to thank you, gentlemen, for joining me in the discussion today. Thank you, Dr Kaufmann. Thank you, Dr White.
www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.29
Thank you to the audience for joining us today. Please be sure to click on the Earn CME Credit link to take the CME posttest and evaluation.
This transcript has been edited for style and clarity.
This is a CME certified activity. To earn credit for this activity visit: www.medscape.org/roundtable/neurogenic-orthostatic-hypotension
Pg.30
Neurogenic Orthostatic Hypotension: Expert Perspectives on Diagnosis and Treatment Strategies CME
References1. The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. Neurology. 1996;46:1470.2. Schmidt C, Berg D, Herting, et al. Loss of nocturnal blood pressure fall in various extrapyramidal syndromes. Mov Disord. 2009;24:2136-2142. Abstract3. Kaufmann H, Malamut R, Norcliffe-Kaufmann L, et al. The Orthostatic Hypotension Questionnaire (OHQ): validation of a novel symptom assessment scale. Clin Auton Res. 2012;22:79-90. Abstract4. Kaufmann H, Freeman R, Biaggioni I, et al. Droxidopa for neurogenic orthostatic hypotension. Neurology. 2014;83:328-335 Abstract5. Hauser R; Isaacson S, Lisk JP, et al. Droxidopa for the short-term treatment of symptomatic neurogenic orthoststic hypotension in Parkinson Disease (nOH306B) Mov Disord. In press.6. Northera™ [package insert]. Deerfield, IL: Lundbeck NA Ltd; 2014.7. Kaufmann H, Saadia D, Voustianiouk A, et al. Norepinephrine precursor therapy in neurogenic orthostatic hypotension. Circulation. 2003;108:724-728. Abstract
AbbreviationsBP = blood pressure DA = dopamine DDC = dopa decarboxylase EOS = end of study FDA = Food and Drug Administration MSA = multiple system atrophy NE = norepinephrine nOH = neurogenic orthostatic hypotension OH = orthostatic hypotension OHQ = Orthostatic Hypotension Questionnaire PD = Parkinson disease PSP = progressive supranuclear palsy
DisclaimerThe educational activity presented above may involve simulated case-based scenarios. The patients depicted in these scenarios are fictitious and no association with any actual patient is intended or should be inferred.
The material presented here does not necessarily reflect the views of Medscape, LLC, or companies that support educational programming on medscape.org. These materials may discuss therapeutic products that have not been approved by the US Food and Drug Administration and off-label uses of approved products. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or employing any therapies described in this educational activity.
Medscape Education © Medscape, LLC