Embed Size (px)
DESCRIPTION
case 1
Citation preview
case records of the massachusetts general hospital
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121136
Founded by Richard C. CabotNancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., EditorJo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate EditorSally H. Ebeling, Assistant Editor Emily K. McDonald, Assistant Editor
Case 29-2012: A 49-Year-Old Man with Pain and Cranial-Nerve Palsies after Treatment
of Oral CancerLori J. Wirth, M.D., Scott R. Plotkin, M.D., Ph.D., Kevin S. Emerick, M.D.,
Mary Elizabeth Cunnane, M.D., and William C. Faquin, M.D., Ph.D.
From the Departments of Medical Oncol-ogy (L.J.W.), Neurology (S.R.P.), Surgery (K.S.E.), and Pathology (W.C.F.), Massa-chusetts General Hospital; the Depart-ments of Otolaryngology (K.S.E.) and Radiology (M.E.C.), Massachusetts Eye and Ear Infirmary; and the Departments of Medicine (L.J.W.), Neurology (S.R.P.), Otology and Laryngology (K.S.E.), Radi-ology (M.E.C.), and Pathology (W.C.F.), Harvard Medical School — all in Boston.
N Engl J Med 2012;367:1136-47.
DOI: 10.1056/NEJMcpc1104565Copyright © 2012 Massachusetts Medical Society.
Pr esen tation of C a se
Dr. Mikael L. Rinne: A 49-year-old man was admitted to this hospital because of fever, pain, and cranial-nerve deficits after treatment of squamous-cell cancer of the oral cavity.
Approximately 9 months before admission, a painful ulcer developed on the right side of the floor of the mouth. Imaging studies performed at another institution revealed an enhancing lesion in the floor of the mouth; a biopsy specimen of the lesion revealed poorly differentiated squamous-cell carcinoma. The patient had a history of depression and alcoholism and had spent time in halfway houses; he had stopped drinking alcohol 3 months earlier. He had smoked cigarettes (70 pack-years) but had stopped smoking after the diagnosis of oral cancer; he did not use illicit drugs. Four months before admission, right hemiglossectomy, resection of the right side of the floor of the mouth, bilateral modified radical neck dissection, and reconstruction were performed at the Massachusetts Eye and Ear Infirmary. Patho-logical examination of the tissue revealed a large (stage T4), invasive, poorly differ-entiated squamous-cell carcinoma, with extensive lymphovascular and focal peri-neural invasion, bilateral lymph-node metastases (stage N2c), and positive margins. After surgery, dental extractions were performed in anticipation of radiation, and a submental abscess developed, which resolved after antibiotic therapy and inci-sion and drainage. Radiation therapy (66 Gy, over a period of 6 weeks) and concur-rent chemotherapy (paclitaxel and carboplatin) were administered. Throughout the treatment, the patient reported severe pain in the radiation field that required narcotic analgesia.
Four days after the completion of radiotherapy, pain developed around the right eye and forehead, with ptosis and diplopia, and the temperature rose to 38.3°C. The patient was admitted to another hospital. Cultures of the blood and urine were sterile. Computed tomography (CT) of the head and neck reportedly showed post-treatment changes but no fluid collection within the surgical bed or the neck. During the next 4 days, pain worsened and complete right ophthalmoplegia developed. In
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1137
addition, the examination revealed sensation to light touch and cold were reduced in the distribu-tions of the first (ophthalmic) and second (maxil-lary) branches of the fifth cranial nerve (V1 and V2) on the right side and of the mandibular branch (V3) bilaterally. On the sixth day, CT of the head reportedly revealed an area of slightly decreased enhancement in the right cavernous sinus that measured 1.2 cm in diameter and was centered on the right internal carotid artery. Lumbar puncture was performed. Analysis of the cerebrospinal f luid (CSF) is shown in Table 1; testing for Lyme disease, herpes simplex virus (HSV), and syphilis (by the Venereal Disease Re-search Laboratory test) and examination for malig-nant cells were negative. Cultures were sterile. Ceftazidime was administered.
During the next week, left ophthalmoplegia and bilateral facial swelling developed; the pa-tient reported severe generalized facial pain. On the 12th day, magnetic resonance imaging (MRI) of the head reportedly revealed signal abnormal-ity in the foramina and infratemporal fossa at the base of the skull, extensive enhancement and sig-nal abnormality in the sphenoid sinus (features consistent with inflammation), and multiple den-sities in the cerebellum that were consistent with infarcts. He was transferred to this hospital on the 13th day. Medications on transfer included ceftazi-dime, gabapentin, dalteparin, hydromorphone, lorazepam, methylphenidate, metoclopramide, mirtazapine, posaconazole, thiamine, and ny-statin suspension.
On examination, the patient was cachectic. The blood pressure was 134/68 mm Hg, the pulse 96 beats per minute, the temperature 37.5°C, the respiratory rate 20 breaths per minute, and the oxygen saturation 93% while he was breathing ambient air. Surgical scars and changes second-ary to radiation were seen on the skin of the neck, with an eschar on the upper neck. He re-ported severe pain on palpation of the orbits, temples, and forehead. On neurologic examina-tion, he was intermittently drowsy and inatten-tive but was oriented to self and location. There was complete ptosis of the left eyelid and incom-plete ptosis of the right eyelid, with 2 mm of corneal exposure. Pupils were 6 mm in diameter and unresponsive to light. Passive head turning did not produce eye movements in the opposite direction (doll’s-eye maneuver). Strength was normal. Sensory examination and gait testing
were not performed because of fluctuating at-tentiveness.
The red-cell indexes, the platelet count, and tests of renal and liver function were normal, as were the blood levels of glucose, total protein, al-bumin, globulin, phosphorus, magnesium, and calcium; other test results are shown in Table 1. Lumbar puncture was performed, and testing for HSV was negative; results of analysis of the CSF are shown in Table 1. Cultures of the blood, urine, and CSF were sterile. The administration of vancomycin, meropenem, and liposomal am-photericin B was begun. Packed red cells were transfused.
During the next 2 days, the patient became increasingly confused and obtunded, without new focal findings on examination. The blood levels of lactate and ammonia were normal. MRI of the brain was suboptimal because of motion. There were abnormal signal and enhancement in the central skull base, from the greater wing of the sphenoid to the left infratemporal fossa, the pterygopalatine fossa, the vidian canal, and the foramen rotundum bilaterally; enlargement and enhancement of the cavernous sinuses bilater-ally; and thickening and enhancement of the dura of the anterior and middle cranial fossa. There were multiple foci of restricted diffusion in the brain parenchyma, features consistent with subacute infarcts. On the second day, the temperature rose to 39.3°C. The administration of clindamycin and filgrastim was begun. A transthoracic echocardiogram showed a patent foramen ovale, with no evidence of valvular le-sions.
On the third day, the patient became intermit-tently agitated and was transferred to the medi-cal intensive care unit, where he was sedated, and the trachea was intubated to permit additional imaging. Laboratory-test results are shown in Table 1. MRI of the brain performed with the administration of gadolinium revealed enhance-ment surrounding multiple foci of restricted diffusion, a feature consistent with the evolution of subacute infarcts, and a new focus of restricted diffusion in the right thalamus; enhancement and thickening of the dura, cavernous sinuses, and skull-base foramina were unchanged. On the fourth day, transesophageal echocardiography showed no valvular vegetations or intracardiac thrombus.
A diagnostic procedure was performed.
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121138
Differ en ti a l Di agnosis
Dr. Lori J. Wirth: All discussants are aware of the diagnosis in this case. This 49-year-old man with a history of tobacco and alcohol abuse presented with fever and progressive bilateral cranial-nerve palsies shortly after completing treatment for a locally advanced squamous-cell carcinoma of the oral tongue, defined as the portion of the tongue anterior to the circumvallate papillae. The differ-ential diagnosis centered on an infectious process (a complication of treatment) and recurrent can-cer. I will begin by reviewing the rationale for his initial treatment and then will focus on the dif-ferential diagnosis of his current presentation.
Management of Squamous-cell carcinoma of the head and neck
Most squamous-cell carcinomas of the head and neck are locally advanced at the time of diagnosis and require multidisciplinary treatment.1 The lo-cation of the cancer is integral to the under-standing of its natural history and the develop-ment of a multidisciplinary treatment approach. This patient had cancer of the oral tongue, one of the most common subsites of squamous-cell car-cinoma of the head and neck,2 which is best ap-proached with surgery first, in view of the surgical accessibility of the oral cavity and current tech-niques for resection and reconstruction that yield good speech and swallowing outcomes.1 There-
Table 1. Laboratory Data.*
VariableReference Range,
Adults†On Admission, Other Hospital
On Admission, This Hospital 3rd Day 4th Day
Blood
Hematocrit (%) 41.0–53.0 25.5 25.3 25.3 25.5
Hemoglobin (g/dl) 13.5–17.5 8.9 8.9 9.2 9.1
White-cell count (per mm3) 4500–11,000 2000, with toxic granulations
2100 5200 11,600
Differential count (%)
Neutrophils 40–70 43 64 71 73
Band forms 0–10 28 6 13 19
Lymphocytes 22–44 5 13 2 2
Monocytes 4–11 19 14 11 6
Eosinophils 0–8 3 0 2 0
Basophils 0–3 0 0 1 0
Myelocytes 0 1 0 0 0
Metamyelocytes 0 1 3 0 0
Activated partial-thromboplastin time (sec) 21.0–33.0 35.1 33.5
Prothrombin time (sec) 11.0–13.7 13.4 14.4 15.3
International normalized ratio for prothrombin time
1.0 1.2 1.3
Sodium (mmol/liter) 135–145 121 126 123 120
Potassium (mmol/liter) 3.4–4.8 3.9 4.9 3.8 3.7
Chloride (mmol/liter) 100–108 83 88 90 87
Carbon dioxide (mmol/liter) 23.0–31.9 29 27.2 25.1 24.5
Thyrotropin (μU/ml) 0.40–5.00 0.03 0.11
Free thyroxine (ng/dl) 0.9–1.8 0.7 (ref 0.6–1.6) <0.4
Total triiodothyronine (ng/dl) 60–181 53
Cortisol (μg/dl)
Random 5–15, between 12 p.m. and 8 p.m.
9.8
90 min after cosyntropin 22.5
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1139
fore, this patient underwent hemiglossectomy, free-flap reconstruction, and bilateral selective neck dissection (dissection of the regions that are most likely to contain involved nodes).
May we review the pathological specimen?Dr. William C. Faquin: Gross examination of the
specimen from the partial glossectomy revealed a firm, tan tumor, 4.3 cm in diameter, involving the soft tissue of the tongue and extending to multiple soft-tissue margins (Fig. 1A). Micro-scopical evaluation showed a predominantly non-keratinizing, poorly differentiated squamous-cell carcinoma extensively invading the lingual skele-tal muscle, the salivary gland, and the soft tissues of the floor of mouth and base of tongue (Fig. 1B). Focally, there was evidence of squamous dysplasia and squamous-cell carcinoma in situ within the overlying lingual mucosa. Multiple foci of lymphatic and venous invasion by squamous-cell carcinoma were present (Fig. 1C); perineural invasion was identified (Fig. 1D), and tumor ex-tended along large nerve bundles (Fig. 1E). Re-
sults of immunohistochemical analysis showed that the carcinoma was strongly positive for p16 and focally positive for BCL2. Expression of p16 is a strong predictor of human papillomavirus (HPV) positivity; therefore, testing for HPV was performed by in situ hybridization, and the re-sults were positive. This carcinoma is not charac-teristic of HPV-related squamous-cell carcino-mas of the head and neck, which tend to occur in the oropharynx and typically do not have the extensive lymphovascular and perineural inva-sion seen in this case. Expression of BCL2 is an adverse prognostic factor in squamous-cell car-cinomas of the head and neck.
Bilateral neck dissection revealed metastatic squamous-cell carcinoma in 8 of 57 lymph nodes, including focal extranodal extension into the soft tissue of the right side of the neck to level IV. Therefore, the final pathological stage is T4N2c, according to the American Joint Committee on Cancer staging system.
Dr. Wirth: The finding of HPV in this locally
Table 1. (Continued.)
VariableReference Range,
Adults†On Admission, Other Hospital
On Admission, This Hospital 3rd Day 4th Day
Cerebrospinal fluid
Color Colorless Colorless Colorless
Turbidity Clear Clear Clear
Xanthochromia None None
Red-cell count (per mm3)
Tube 1 0 11 11
Tube 3 or 4 0 1 8
White-cell count (per mm3)
Tube 1 0–5 3 1
Tube 3 or 4 0–5 0 1
Differential count, tube 1 (%)
Neutrophils 0 7
Band forms 0 4
Lymphocytes 0 44
Monocytes 0 45
Protein (mg/dl) 5–55 48 75
Glucose (mg/dl) 50–75 56 55
* To convert the values for free thyroxine to picomoles per liter, multiply by 12.87. To convert the values for total triiodothyronine to nano-moles per liter, multiply by 0.01536. To convert the values for cortisol to nanomoles per liter, multiply by 27.59. To convert the values for glucose to millimoles per liter, multiply by 0.05551. Ref denotes reference range at the other hospital.
† Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Massachusetts General Hospital are for adults who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121140
advanced cancer was unexpected. HPV, particularly type 16, is most often associated with squamous-cell carcinomas of the oropharynx.3 Patients with HPV-positive squamous-cell carcinoma of the head and neck tend to be younger and have had less exposure to tobacco and alcohol than those with classic (HPV-negative) squamous-cell carcinoma of the head and neck. Most important, patients with HPV-positive tumors have a better progno-
sis than do patients with HPV-negative tumors, in part because HPV-positive tumors tend to be sensitive to both chemotherapy and radiation.4
Risk of Recurrence of Squamous-cell carcinoma of the Head and Neck
Features that confer a high risk of recurrence of squamous-cell carcinomas of the head and neck include positive or close margins, nodal metasta-
A B
DC
E
Figure 1. Specimen from Partial Glossectomy.
Panel A shows extensive involvement of the tongue by nonkeratinizing squamous-cell carcinoma, which on micro-scopical examination can be seen invading the lingual skeletal muscle (Panel B, hematoxylin and eosin). There is extensive lymphovascular invasion (Panel C, hematoxylin and eosin) and perineural invasion by squamous-cell carcinoma (Panel D, hematoxylin and eosin), as well as extension along large nerve bundles (Panel E, hematoxylin and eosin).
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1141
sis with extranodal spread, two or more involved lymph nodes, invasion of the soft tissues of the neck or skin, and perineural invasion.5-7 High-risk features in this case were positive margins, perineural invasion, and multiple nodal metasta-ses with extranodal spread, as well as the pa-tient’s history of tobacco and alcohol use. Since this patient’s risk factors include both positive margins and extracapsular spread, there are clear indications for adjuvant platinum-based chemoradiotherapy, which improves locoregion-al control and survival outcomes as compared with radiotherapy alone.8-10 Surgery was there-fore followed by chemoradiation in this patient.
Four days after completion of chemoradio-therapy, right-eyelid weakness, diplopia, and right-sided facial and neck pain developed. On examination, the patient had mucositis, derma-titis, and pain in the radiation field, as expected after chemoradiation, as well as exquisite ten-derness to palpation of the forehead, orbits, and face. We had to determine whether this was an infectious process or locally recurrent cancer.
Recurrent Squamous-Cell CarcinomaThe median time to recurrence of squamous-cell carcinoma of the head and neck after the com-pletion of treatment is 8 to 9 months, so if this is a case of recurrence, it is unusually early.11 Before the current era of chemoradiotherapy, when ra-diotherapy alone was the mainstay of adjuvant treatment, recurrence of carcinoma was most of-ten locoregional, whereas now, with patients at high risk for recurrence receiving chemoradio-therapy, distant metastasis is more frequent. For primary tumors in the oral cavity, locoregional recurrence can occur within the cavity, the cervi-cal nodes, or along the paths of the 5th, 9th, and 12th cranial nerves.12 When a patient with squa-mous-cell carcinoma of the head and neck has pain in the head and neck region, recurrent dis-ease is always a concern, since this type of cancer can be neurotropic, as it was in this case. When squamous-cell carcinoma of the head and neck involves the 5th cranial nerve, typical findings are pain or numbness in the distribution of the affected branches. Examination of the head and neck in this patient was limited by mucositis and dermatitis; nevertheless, there was no evidence of recurrent tumor in the oral cavity or the neck on physical examination, which included fiber-optic laryngoscopic examination. The tenderness to palpation was puzzling in the absence of any
other gross abnormality and suggested involve-ment of the 5th cranial nerve by cancer.
May we review the imaging studies?Dr. Mary Elizabeth Cunnane: MRI performed on
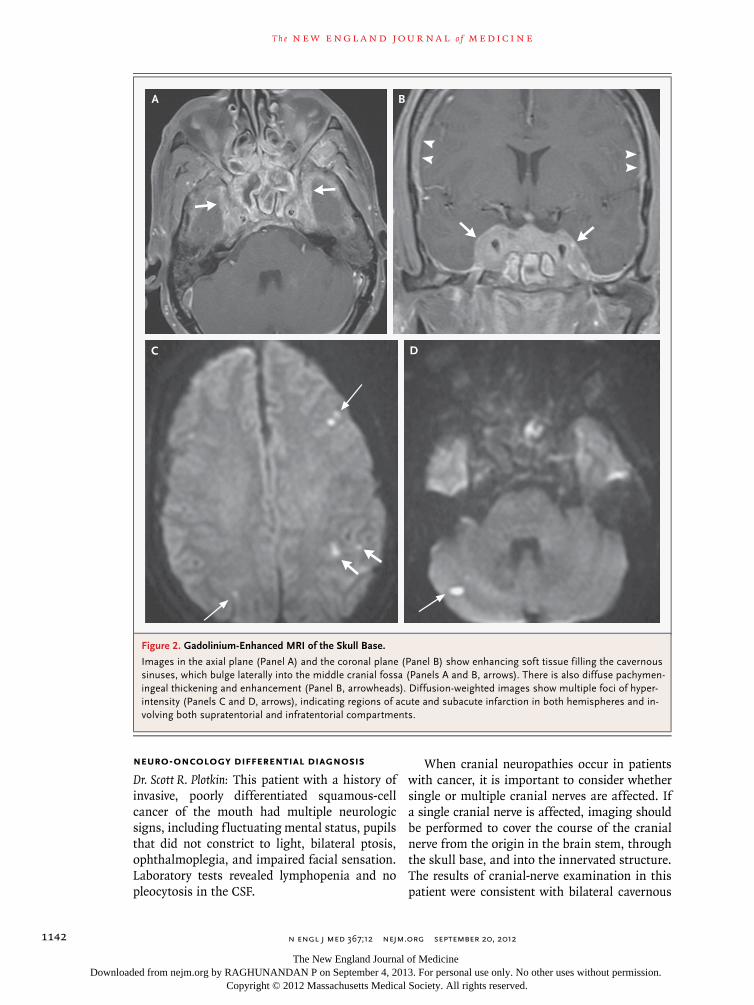
admission reveals marked dural thickening and enhancement and abnormal soft tissue involving the sella and the bilateral cavernous sinuses (Fig. 2A and 2B). Signal abnormality and enhance-ment involve the skull base bilaterally, and on the left, abnormal tissue involves the dura of the middle cranial fossa, the greater wing of the sphenoid, and the inferotemporal fossa. Diffu-sion-weighted images (Fig. 2C and 2D) show multiple regions of restricted diffusion bilater-ally and in the territory of both anterior and posterior circulation. Some of these infarcts show enhancement, and others do not, suggest-ing a mixture of acute and subacute strokes.
Dr. Wirth: Once the radiographic images were available, recurrent squamous-cell carcinoma of the head and neck was considered as a possible diagnosis; however, contrary to this possibility were the fever, the timing of the process (im-mediately on completion of chemoradiotherapy), and the pattern of extensive bilateral involve-ment of the base of the skull and the dura on imaging. With a primary tumor in the lateral oral cavity, mucosal recurrence would be ex-pected in the ipsilateral oral cavity or pharyn-geal wall, and bilateral involvement of the base of the skull, dura, and brain parenchyma would be highly atypical.
Infectious ProcessesMajor considerations were opportunistic infec-tions arising in an immunocompromised pa-tient, such as sinonasal aspergillosis or mucor-mycosis. Intracranial tuberculoma involving the skull base was considered because of the risk fac-tors of alcoholism and time spent in halfway houses. We also considered the development of subacute bacterial endocarditis after the sub-mental abscess, causing septic emboli to the lungs and brain and, possibly, osteomyelitis of the skull base. Despite sterile cultures of the blood and CSF and an absence of vegetations on the echocardiogram, we treated the patient for conventional bacterial pathogens and fungi, to avoid missing a treatable infection. We also re-quested neuro-oncology and otolaryngology con-sultation for advice regarding further diagnostic considerations, including the need for definitive tissue diagnosis.
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121142
Neuro-Oncology Differential Diagnosis
Dr. Scott R. Plotkin: This patient with a history of invasive, poorly differentiated squamous-cell cancer of the mouth had multiple neurologic signs, including fluctuating mental status, pupils that did not constrict to light, bilateral ptosis, ophthalmoplegia, and impaired facial sensation. Laboratory tests revealed lymphopenia and no pleocytosis in the CSF.
When cranial neuropathies occur in patients with cancer, it is important to consider whether single or multiple cranial nerves are affected. If a single cranial nerve is affected, imaging should be performed to cover the course of the cranial nerve from the origin in the brain stem, through the skull base, and into the innervated structure. The results of cranial-nerve examination in this patient were consistent with bilateral cavernous
A B
DC
Figure 2. Gadolinium-Enhanced MRI of the Skull Base.
Images in the axial plane (Panel A) and the coronal plane (Panel B) show enhancing soft tissue filling the cavernous sinuses, which bulge laterally into the middle cranial fossa (Panels A and B, arrows). There is also diffuse pachymen-ingeal thickening and enhancement (Panel B, arrowheads). Diffusion-weighted images show multiple foci of hyper-intensity (Panels C and D, arrows), indicating regions of acute and subacute infarction in both hemispheres and in-volving both supratentorial and infratentorial compartments.
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1143
sinus syndrome (deficits of the third through sixth cranial nerves) and optic neuropathy. The identification of bilateral cavernous sinus syn-drome should focus attention to the skull base, and it indicates a process that involves the skull base diffusely. There are several possible causes of multiple cranial neuropathies.
Wernicke’s EncephalopathyWernicke’s encephalopathy is caused by thiamine deficiency and is characterized by fluctuation of attentiveness, oculomotor abnormalities, and gait difficulty.13 This patient’s history of alcoholism and his impaired feeding due to treatment of his oral cancer raises concern for decreased nutri-tional intake. However, in view of the presence of a mass lesion in the skull base, this diagnosis was not considered further.
InfectionThis patient is at increased risk for infection be-cause of his history of submental abscess, chemoradiation, and lymphopenia. Fever and al-tered mental status are cardinal features of men-ingitis, and infections that involve the basal me-ninges may lead to cranial neuropathies. The presence of lymphopenia raises concern for un-common pathogens such as listeria, mucormyco-sis, and tuberculosis, particularly in patients with malnutrition.14 Facial infections, such as the submental abscess in this patient, increase the risk of cavernous sinus thrombosis, which may be manifested with fever, headaches, pro-ptosis, and ocular motor palsies. A skull-base infection could also explain the subacute embol-ic strokes involving the distribution of the ca-rotid and vertebral arteries bilaterally, since en-docarditis from disseminated infection can cause embolic strokes, as can direct vascular in-vasion.15
CancerLeptomeningeal involvement occurs in about 5% of patients with metastatic cancer.16 The hall-mark manifestation of this condition is focal neurologic deficits involving the cranial and spi-nal nerves; symptoms often include headache, difficulty walking, and bowel or bladder dys-function.17 Perineural spread of squamous-cell carcinoma of the head and neck has been report-ed, with extension of the tumor into the skull base along the cranial nerves.18-20 In this patient,
there was perineural invasion associated with the primary tumor but no radiographic evidence of extension of the tumor to the skull base.
SummaryWe believed that the most likely diagnosis in this case was an infection involving the skull base. Less likely was the possibility of direct extension of the tumor into the skull base. We recommend-ed a biopsy to establish a histologic diagnosis.
Approaches to biopsy
Dr. Kevin S. Emerick: A tissue biopsy was required in this case to distinguish between cancer and infection. The anatomical location of concern presented challenges in obtaining a specimen.
Image-Guided Fine-Needle BiopsyMasses or lesions in anatomically sensitive areas or areas with limited access, such as this one, can be approached with image-guided fine-nee-dle biopsy. Biopsy specimens of intracranial and even skull-base lesions can be obtained in this manner; however, biopsies of skull-base lesions are typically limited to lesions located more lat-erally than this one. The proximity to major vas-cular structures and critical cranial nerves and the limited accessibility of the lesion prevented an image-guided biopsy from being reliably per-formed.
Neurosurgical ApproachesOpen approaches to biopsy were considered by the neurosurgical and otolaryngologic teams. There are numerous neurosurgical approaches to this area, but they all involve a craniotomy and often a large amount of brain retraction that would not have been well tolerated by this pa-tient. In some instances, extensive soft-tissue or bone dissections through the infratemporal fos-sa or temporal bone are needed to gain access to the craniotomy site, increasing the surgical time for an already critically ill patient. Therefore, we decided against a neurosurgical approach.
Endoscopic Transsphenoidal BiopsyTwo pathways to this lesion were then consid-ered. The first was an endoscopic transsphenoi-dal approach, commonly used for chronic rhino-sinusitis. This approach has been enhanced by image-guided systems that provide additional anatomical definition and location confirma-
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121144
tion.21 However, in this case, the tissue needed for diagnosis was not in the sphenoid sinus but in the cavernous sinus. Studies of cadavers have documented the ability to reach the cavernous sinus with modifications of the traditional endo-scopic approaches to the sphenoid22; however, ex-perience with clinical applications is limited.23 The biggest problem with this approach is the difficulty controlling bleeding. Acquiring enough tissue for examination would undoubtedly have caused extensive bleeding that would have been very difficult to control with this approach.
Biopsy of the Infratemporal FossaThe central skull base communicates laterally with the infratemporal fossa. Because of imag-ing studies in this patient suggesting that the process had spread into the infratemporal fossa, approaches to the infratemporal fossa were con-sidered. Several approaches have been described and are commonly used, depending on the type of resection being performed.24-26 In this case, since only a biopsy specimen was needed and re-constructive procedures were not anticipated, a very direct approach to the infratemporal fossa was ultimately chosen as the best path to the abnormal area.
An invasive fungal infection was a diagnostic consideration in this case. Although cultures had been negative, the diagnosis of invasive fun-gal infections cannot be made on the basis of fluid cultures or swabs and requires tissue bi-opsy. An infection involving cavernous sinuses would most likely also involve the sphenoid si-nus, since the lateral wall of the sphenoid sinus is the medial wall of the cavernous sinus. Infec-tion in the other paranasal sinuses could also lead to infection in the cavernous sinus, as could a soft-tissue infection of the nose or periorbital region. Since the sphenoid sinus was the prob-able source of any infection, this area was also targeted for biopsy.
An incision was made near the lateral can-thus and extended laterally to allow access to the infratemporal fossa at the anterior edge of the temporalis muscle and along the lateral wall of the orbit. Dissection of the medial and anterior aspects of the infratemporal fossa revealed an infiltrative process; a biopsy specimen was ob-tained and sent for frozen-section examination. Examination of the initial frozen section sug-
gested squamous-cell carcinoma. Even though the frozen-section examination of the infratem-poral fossa suggested cancer, we could not rule out the potential for two separate processes. Therefore, we performed an image-guided trans-nasal endoscopic biopsy of the sphenoid sinus through the anterior and posterior ethmoid si-nuses. Frozen-section examination revealed no fungi, but intravascular tumor was present.
Clinic a l Di agnosis
Squamous-cell carcinoma involving the skull base or an opportunistic infection.
Discussion of M a nagemen t
Dr. Wirth: This patient had rapidly progressive squamous-cell carcinoma of the oral cavity, with extensive involvement of the base of the skull and dura. We wondered whether he had hematoge-nous metastasis to the brain parenchyma, which would explain the subacute infarcts seen on MRI. His condition continued to deteriorate. Palliative radiation was precluded because of tumor im-mediately adjacent to the field of his recent radio-therapy. Palliative chemotherapy is also preclud-ed in a patient who is moribund from a solid tumor. Discussions with the patient’s family led to a change in the focus of care to maximizing his comfort at the end of his life. He was extu-bated under sedation with fentanyl and loraze-pam on hospital day 12 and died 35 minutes lat-er. Consent for postmortem examination was obtained.
Pathol o gic a l Discussion
Dr. Faquin: Biopsy specimens of the infratemporal fossa and the ethmoid, maxillary, and sphenoid sinuses showed extensive, invasive, nonkeratiniz-ing squamous-cell carcinoma with multifocal lymphovascular invasion (Fig. 3A).
Postmortem examination revealed metastatic squamous-cell carcinoma in the lungs, liver, stomach, thyroid, heart, jejunum, ileum, left ad-renal gland, base of the skull, and cervical spine (Fig. 3B). Neuropathological evaluation showed squamous-cell carcinoma extending from one cavernous sinus into the other through the pitu-itary gland (Fig. 3C) and also extending along
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1145
the trigeminal nerve and through the trigeminal ganglion (Fig. 3D). There was extensive dural involvement by squamous-cell carcinoma, with-out leptomeningeal involvement (Fig. 3E). Mac-rophage-rich infarcts were present in the cere-
bellum and right frontal lobe (Fig. 3F), but no tumors or thrombi were identified and there was no evidence of vasculitis.
Dr. Wirth: Fortunately, we do not see this pat-tern of rapidly progressive squamous-cell carci-
A B
DC
FE
Figure 3. Infratemporal Biopsy and Autopsy Examination (Hematoxylin and Eosin).
A biopsy specimen of the infratemporal fossa shows invasive squamous-cell carcinoma (Panel A). Postmortem examination shows metastatic squamous-cell carcinoma in the lung (Panel B), the pituitary gland (Panel C), the trigeminal ganglion (Panel D), and the dura (Panel E). There is an infarct in the right frontal lobe (Panel F, arrows) but no evidence of parenchymal or intravascular cancer. (Panels C through F, courtesy of Dr. Matthew P. Frosch, Neuropathology.)
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;12 nejm.org september 20, 20121146
noma of the head and neck very often. An im-portant lesson is that pain in a patient with a history of cancer usually does signal recurrent cancer. Although imaging studies can be useful in distinguishing between cancer and infection, in most cases a tissue biopsy is essential, espe-cially when the differential diagnosis includes an untreatable fatal cancer. Once the diagnosis is known, a rational decision can be made either to pursue aggressive treatment for infection or to change the focus of care to optimizing the patient’s comfort at the end of life.
Dr. Plotkin: The presentation with strokes is the most difficult part of this case to explain. We did an extensive workup for stroke, but we were not able to perform a hypercoagulable workup, so we could not definitively rule out a hyperco-agulable state.
A Physician: It is interesting in view of the ex-tensive dural involvement that examination of the CSF was negative. How often do you see this?
Dr. Plotkin: Patients with dural spread of can-cer often have concurrent leptomeningeal or brain involvement. Results of laboratory tests of the CSF are normal in approximately 15% of patients with leptomeningeal metastases. This
percentage is probably higher in patients with isolated dural disease. Although the lumbar-puncture results were initially confusing, we believe the cancer spread to the skull base by migrating up cranial-nerve fascicles, rather than by disseminating through the CSF.
A nat omic a l Di agnoses
Squamous-cell carcinoma of the tongue and floor of the mouth, with metastatic disease to the lungs, liver, stomach, thyroid, heart, jejunum, il-eum, left adrenal gland, base of the skull, cervi-cal spine, trigeminal nerve and ganglion, cavern-ous sinuses, pituitary gland, and dura mater.
Infarcts in the cerebellum and right frontal lobe.This case was presented at Neurology Grand Rounds.Dr. Wirth reports receiving consulting fees from Bayer, Boeh-
ringer Ingelheim, Exelexis, and Acceleron; Dr. Plotkin, grant support to his institution from Pfizer; Dr. Faquin, payment for expert opinions in legal cases concerning thyroid cancer and royalties from Springer; and Dr. Cunnane, payment from World-Care Clinical for interpreting results of imaging studies for clini-cal trials. No other potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
We thank Dr. Matthew P. Frosch for the neuropathological examination and images.
References
1. Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet 2008;371:1695-709.2. Curado MP, Hashibe M. Recent changes in the epidemiology of head and neck cancer. Curr Opin Oncol 2009;21: 194-200.3. Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for hu-man papillomavirus-related and -unre-lated oral squamous cell carcinomas in the United States. J Clin Oncol 2008;26: 612-9.4. Chung CH, Gillison ML. Human pap-illomavirus in head and neck cancer: its role in pathogenesis and clinical implica-tions. Clin Cancer Res 2009;15:6758-62.5. Peters LJ, Goepfert H, Ang KK, et al. Evaluation of the dose for postoperative radiation therapy of head and neck can-cer: first report of a prospective random-ized trial. Int J Radiat Oncol Biol Phys 1993;26:3-11.6. Huang DT, Johnson CR, Schmidt-Ull-rich R, Grimes M. Postoperative radio-therapy in head and neck carcinoma with extracapsular lymph node extension and/or positive resection margins: a compara-tive study. Int J Radiat Oncol Biol Phys 1992;23:737-42.
7. Langendijk JA, Slotman BJ, van der Waal I, Doornaert P, Berkof J, Leemans CR. Risk-group definition by recursive partitioning analysis of patients with squamous cell head and neck carcinoma treated with surgery and postoperative radiotherapy. Cancer 2005;104:1408-17.8. Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with or with-out concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004;350:1945-52.9. Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004;350:1937-44.10. Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative ra-diation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Head Neck 2005;27:843-50.11. Hall SF, Groome PA, Rothwell D. Time to first relapse as an outcome and a predictor of survival in patients with squamous cell carcinoma of the head and neck. Laryngoscope 2000;110:2041-6.12. Yovino S, Settle K, Taylor R, et al.
Patterns of failure among patients with squamous cell carcinoma of the head and neck who obtain a complete re-sponse to chemoradiotherapy. Head Neck 2010;32:46-52.13. Sechi G, Serra A. Wernicke’s encepha-lopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol 2007;6:442-55.14. Central nervous system infections. In: DeAngelis LM, Posner JB. Neurologic complications of cancer. 2nd ed. New York: Oxford University Press, 2009:369-417.15. Rogers LR. Cerebrovascular compli-cations in cancer patients. Neurol Clin 2003;21:167-92.16. Beauchesne P. Intrathecal chemother-apy for treatment of leptomeningeal dis-semination of metastatic tumours. Lancet Oncol 2010;11:871-9.17. Leptomeningeal metastases. In: DeAn-gelis LM, Posner JB. Neurologic complica-tions of cancer. 2nd ed. New York: Oxford University Press, 2009:240-81.18. Lin C, Tripcony L, Keller J, et al. Peri-neural infiltration of cutaneous squa-mous cell carcinoma and basal cell car-cinoma without clinical features. Int J Radiat Oncol Biol Phys 2012;82:334-40.
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 367;12 nejm.org september 20, 2012 1147
19. Fagan JJ, Collins B, Barnes L, D’Amico F, Myers EN, Johnson JT. Perineural inva-sion in squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg 1998;124:637-40.20. Zhu JJ, Padillo O, Duff J, Hsi BL, Fletcher JA, Querfurth H. Cavernous sinus and leptomeningeal metastases arising from a squamous cell carcinoma of the face: case report. Neurosurgery 2004;54: 492-8.21. Reardon EJ. The impact of image-
guidance systems on sinus surgery. Oto-laryngol Clin North Am 2005;38:515- 25.22. Abuzayed B, Tanriover N, Gazioglu N, Ozlen F, Cetin G, Akar Z. Endoscopic anatomy and approaches of the cavernous sinus: cadaver study. Surg Radiol Anat 2010;32:499-508.23. Sung A, Bergsneider M, Wang MB. Transnasal endoscopic surgery of the cav-ernous sinus for tissue diagnosis. Laryn-goscope 2010;120:282-4.
24. Tiwari R, Quak J, Egeler S, et al. Tu-mors of the infratemporal fossa. Skull Base Surg 2000;10:1-9.25. Mansour OI, Carrau RL, Snyderman CH, Kassam AB. Preauricular infratem-poral fossa surgical approach: modifica-tions of the technique and surgical indi-cations. Skull Base 2004;14:143-51.26. Mishra A. Transorbital approach to infratemporal fossa: novel technique. J Laryngol Otol 2011;125:638-42.Copyright © 2012 Massachusetts Medical Society.
Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
The New England Journal of Medicine Downloaded from nejm.org by RAGHUNANDAN P on September 4, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.