Embed Size (px)
DESCRIPTION
bedah
Citation preview

case records of the massachusetts general hospital
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 364;4 nejm.org january 27, 2011362
Founded by Richard C. CabotNancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate EditorJo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate EditorSally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor
From the Division of Surgical Oncology, the Department of Surgery ( J.C.C.), the Division of Medical Oncology, Depart-ment of Medicine (J.W.C.), and the De-partments of Radiology (D.V.S.) and Pa-thology (L.R.Z.), Massachusetts General Hospital, Boston; the Department of Sur-gical Oncology, M.D. Anderson Hospital, and the Department of Surgery, Univer-sity of Texas Medical School — both in Houston (S.A.C.); and the Departments of Surgery ( J.C.C.), Medicine (J.W.C.), Ra-diology (D.V.S.), and Pathology (L.R.Z.), Harvard Medical School, Boston.
N Engl J Med 2011;364:362-70.Copyright © 2011 Massachusetts Medical Society.
Pr esen tation of C a se
Dr. Serguei Melnitchouk (Surgery): A 58-year-old woman was seen in the multidisci-plinary gastrointestinal oncology clinic of this hospital because of a mass in the liver.
The patient had been well until 2 weeks earlier, when severe, sharp pain devel-oped suddenly in the right upper quadrant. The pain did not radiate, and there was no nausea, vomiting, or food intolerance. During the day, the pain (which she rated at up to 7 on a scale of 0 to 10, with 10 indicating the most severe pain) was intermittent and increased with moving or coughing. That evening, she went to the emergency department of her local hospital and was admitted. Ultrasonogra-phy of the abdomen showed a mass, 11 cm in diameter, in the right lobe of the liver. Computed tomography (CT) of the chest, with the administration of contrast material, revealed subsegmental (discoid) atelectasis in the apical and posterior basal segments of the lower lobe of the right lung. CT of the abdomen revealed an area of hypodensity, 7.8 cm by 5.3 cm by 11 cm, in the right hepatic lobe, abutting the gallbladder. The lesion showed slight heterogeneous enhancement, less than that of the surrounding liver; no neovascularity during the arterial phase; and no discrete central scar. There was a hypodense lesion (4 mm in diameter) in the lateral aspect of the right kidney and a small hiatal hernia. Cytologic examination of a specimen from a fine-needle aspiration biopsy of the liver mass revealed small, malignant cells that expressed pancytokeratin and synaptophysin and had focal positivity for cytokeratin 7 and no expression of chromogranin, cytokeratin 20, or thyroid transcription factor 1 (TTF-1). The findings were thought to be consistent with small-cell carcinoma but did not indicate a site of origin. The patient was discharged home on the fourth day, with pain medications.
Two weeks later, the patient was seen at this hospital. She reported pain (rated at 2 out of 10) in her right upper abdomen and back, with no weight loss, night sweats, or change of appetite, and a persistent cough that she had had for years that was unchanged. She had diabetes mellitus type 2, hyperlipidemia, hyperten-sion, glaucoma, arthritis, scoliosis, irritable bowel symptoms, and multiple epi-sodes of bronchitis and pneumonia; previous operations included a tonsillectomy, adenoidectomy, sinus surgery, and a hysterectomy for a prolapsed uterus. Medica-
Case 3-2011: A 58-Year-Old Woman with a Mass in the Liver
James C. Cusack, Jr., M.D., Jeffrey W. Clark, M.D., Steven A. Curley, M.D., Dushyant V. Sahani, M.D., and Lawrence R. Zukerberg, M.D.
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 364;4 nejm.org january 27, 2011 363
tions included lisinopril and timolol, and loraz-epam and oxycodone as needed for pain. She was allergic to sulfa drugs, penicillin, and cephalo-sporins. She was divorced, lived with relatives, and worked in an office. She did not smoke, drink alcohol, or use illicit drugs. Her mother had Alzheimer’s disease, her father had died of colon cancer and end-stage renal disease, and a sister had had bilateral breast cancer in her 40s.
On examination, the blood pressure was 190/97 mm Hg, and the other vital signs were normal. The abdomen was soft and slightly ten-der in the right upper quadrant at the liver edge; there was no hepatomegaly, splenomegaly or abdominal distention. The remainder of the physical examination was normal. Magnetic resonance imaging (MRI) of the liver with the administration of gadolinium revealed a lesion in the right lobe, 9.4 cm by 12.3 cm by 8.5 cm, with heterogeneous enhancement. Another le-sion, 5 mm in diameter, in segment seven was consistent with a possible metastasis, and mul-tiple small lesions in the right lobe were thought to be hemangiomata.
The plasma cortisol level was 23.5 μg per deciliter (648 nmol per liter) (reference range, 5 to 15 μg per deciliter [138 to 414 nmol per liter], from noon to 8 p.m.) and the vasoactive intestinal polypeptide was 32 pg per milliliter (reference range, <75). Single-photon-emission CT (SPECT), performed 1 day after the administration of 237 MBq of indium-111–labeled pentetreotide, re-vealed a large region of decreased pentetreotide uptake in the right hepatic lobe that correspond-ed to the mass seen on the previous MRI; no other areas of abnormal activity were visualized in the liver or spine.
Additional diagnostic tests were performed, and a management decision was made.
Differ en ti a l Di agnosis
Dr. Jeffrey W. Clark: May we review the imaging studies?
Dr. Dushyant V. Sahani: CT of the abdomen re-vealed a large mass within the right hepatic lobe. The mass abutted the right margin of the gallbladder and was partially exophytic off the inferior margin of the liver (Fig. 1A). The mass showed slight heterogeneous enhancement with no neovascularity during the arterial phase and no discrete central scar. There was no evidence of biliary obstruction or evidence of a primary
tumor elsewhere in the abdomen or pelvis. MRI of the liver (Fig. 1B) confirmed a heterogeneous-ly enhancing mass in the right lobe that showed
A
B
C
Figure1.ImagingStudiesatPresentation.
A contrast-enhanced CT image of the liver (Panel A; horizontal bar masks text present in the original im-age) shows a large, minimally enhancing mass in the right lobe (arrow), with no biliary obstruction. The corre-sponding MRI image confirms the presence of the large mass (Panel B, arrow) that was seen on CT and also reveals an additional lesion (Panel C, arrow) in seg-ment four.
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 364;4 nejm.org january 27, 2011364
avid enhancement in the arterial phase; an addi-tional 5-mm lesion in segment seven showed features that were similar to those of the domi-nant mass (Fig. 1C). The liver parenchyma showed no cirrhosis or other chronic liver diseases.
The features seen on CT and MRI are sugges-tive of a diagnosis of a metastatic malignant tu-mor. Primary liver tumors such as cholangiocar-cinoma or hepatocellular carcinoma are unlikely in the absence of biliary obstruction or vascular encasement and in the absence of cirrhosis.
Dr. Clark: I am aware of the diagnosis in this case. This patient presented with metastatic can-cer from an unknown primary site; such cancers account for approximately 2% of all cancers, a percentage that continues to fall with improve-ments in diagnostic approaches.1 Cancers of un-known primary site fall into several pathological categories. The most common are adenocarcino-mas; neuroendocrine carcinomas, which this patient has, account for less than 5% of meta-static cancers from an unknown primary site.
Neuroendocrine carcinomas of unknown primary site
Neuroendocrine carcinomas can be divided into well-differentiated or moderately differentiated tumors, which are biologically relatively indo-lent, and poorly differentiated neuroendocrine carcinomas, which are more aggressive.2 Before deciding on treatment it will be important to re-view the pathology to determine whether this tumor is well, moderately, or poorly differentiat-ed, and, if possible, the primary site.
Patients with well-differentiated or moder-ately differentiated neuroendocrine carcinomas (most commonly carcinoid tumors or pancreatic endocrine tumors) may present with liver metas-tases,3 but they often have symptoms that are related to the release of substances such as sero-tonin, glucagon, or insulin, which this patient did not have. If this patient has a metastatic well-differentiated or moderately differentiated neu-roendocrine carcinoma, treatment options would include careful observation (if the tumor is pro-gressing slowly) and long-acting octreotide or its analogues (used for patients who are symptom-atic or to delay tumor progression in asymptom-atic patients).4 Other options include interferon, temozolomide (or dacarbazine), fluorouracil (or capecitabine), streptozocin, bevacizumab, newer agents such as sunitinib,2-5 hepatic arterial em-bolization, radiofrequency ablation, and surgical
resection of metastatic disease confined to the liver, especially if the primary tumor can also be resected.3
Patients with poorly differentiated neuroen-docrine carcinomas, in contrast, frequently pre-sent with multiple metastatic sites, including multiple lymph nodes, and are unlikely to have symptoms that are caused by the release of hor-mones.2,3 The lung is the most common site of origin for small-cell carcinomas, so a chest CT should be performed, as it was in this case. Less than 5% of small-cell carcinomas are extrapul-monary.6 They can arise in many sites, including the gastrointestinal tract, bladder, prostate, ova-ries, cervix, and salivary gland. Poorly differenti-ated neuroendocrine tumors, which this patient is reported to have, tend to have a high response rate to platinum-based chemotherapy (e.g., cis-platin or carboplatin plus etoposide or irinote-can)1-3; although the majority of patients will ultimately have a relapse, a small percentage can have a durable complete response. We would be likely to offer this patient such treatment.1,2
This patient’s liver-biopsy specimen was re-viewed at this hospital, and I will ask Dr. Zuker-berg to show us the slides. The imaging studies showed no evidence of a primary cancer in the lung. The patient had presented with pain in the right upper quadrant; although it was consistent with pain from a liver lesion, it was described as slightly below the edge of the liver and therefore raised the possibility of a process in the right colon or distal small bowel. The patient also had a family history of colon cancer and, at 58 years of age, had never had a colonoscopy. For this reason, I recommended that she undergo a colo-noscopy. A large cecal mass was found, and a biopsy specimen was obtained.
Dr . Jeffr e y W. Cl a r k’s Di agnosis
Poorly differentiated neuroendocrine carcinoma, metastatic to the liver, possibly arising in the colon.
Pathol o gic a l Discussion
Dr. Lawrence R. Zukerberg: The specimen from the fine-needle aspiration biopsy of the liver mass shows a very cellular specimen, with clumps of neoplastic cells admixed with blood (Fig. 2). The neoplastic cells are tightly packed and range from small to medium size, with a high nuclear-
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 364;4 nejm.org january 27, 2011 365
to-cytoplasmic ratio and scant pink cytoplasm. The nuclei are oval with fine chromatin and small nucleoli. Numerous mitoses are seen. Im-munohistochemical staining (Fig. 2, inset) shows that the tumor cells are positive for cytokeratin and synaptophysin and negative for cytokeratin 7, cytokeratin 20, and TTF-1. The findings are those of a poorly differentiated neuroendocrine carcinoma (small-cell carcinoma). A biopsy spec-imen of the cecal mass showed a villous adeno-ma, with no evidence of small-cell carcinoma.
Discussion of M a nagemen t
Dr. James C. Cusack, Jr.: This patient had the rare occurrence of what appeared to be neuroendo-crine cancer arising in a colonic polyp (although we had not yet confirmed the primary site of dis-ease). The surgeon had two decisions to make: whether to resect the primary tumor before che-motherapy was begun and whether to resect the metastatic tumor after chemotherapy. In making these decisions, we drew on both our experience and the literature on the management of the more common situation of metastatic adenocar-cinoma of the colon.
Surgical management of the primary tumor
In this patient with metastatic colon cancer, the role of surgery in the management of the pri-mary tumor should be addressed before systemic chemotherapy is begun, preferably by a surgeon and a medical oncologist working together as a multidisciplinary team. If both systemic therapy and surgery are likely to be included in the treat-ment plan, the treating team must decide wheth-er to leave the primary tumor in place during systemic chemotherapy or to resect it to avoid potential tumor-related and treatment-related complications. The decision regarding the man-agement of the primary colonic tumor must take into consideration the risk of complications re-lated to the primary tumor that may occur dur-ing the course of treatment, as well as the risks and benefits of a major surgical intervention to remove the primary tumor. In addition, the ex-tent of metastatic disease is important, in terms of both the number of organ systems involved and the distribution of metastatic disease in any one organ system. For the patient with a solitary metastasis to the liver, I might recommend a combined colectomy and wedge resection of the liver before systemic therapy.7 However, this pa-
tient appears to have multiple liver lesions that are not currently resectable.
A review of the literature suggested that in 20 to 30% of patients with metastatic colon cancer who receive chemotherapy, complications develop that involve the primary tumor and ultimately require surgical intervention.8 However, one re-cent retrospective study of asymptomatic patients with colon cancer who were treated with a regi-men of either folinic acid (leucovorin), fluoro-uracil, and oxaliplatin (known as FOLFOX) or folinic acid (leu covorin), fluorouracil, and irino-tecan (FOLFIRI), with or without bevacizumab, showed that complications related to the pri-mary tumor developed in only 11% of the pa-tients, and only 7% required surgical interven-tion.8 These complications may be related to progression of the primary tumor or may result from changes of the primary tumor in response to systemic chemotherapy; the most common complications are intestinal obstruction and per-foration. The rationale for resecting the primary tumor is to avoid such complications and the complications that may arise from an emergency operation on a patient who is receiving chemo-therapy (e.g., neutropenia leading to infection) or problems with wound healing in a patient receiving bevacizumab.
The disadvantages of resecting the primary tumor include a delay in the initiation of chemo-
Figure2.SpecimenfromaFine-NeedleAspirationBiopsyoftheLiver.
The aspirate shows blood and cohesive clusters of small, tightly packed cells with oval nuclei and fine chromatin, features that are typical of high-grade neu-roendocrine carcinoma (small-cell carcinoma) (Papani-colaou stain). Immunohistochemical staining (inset) shows that the cytoplasm is positive for synaptophysin, which confirms the diagnosis of neuroendocrine car-cinoma.
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 364;4 nejm.org january 27, 2011366
therapy, the addition of a potentially unnecessary procedure to the treatment plan, an increase in the treatment-related costs and risks to the pa-tient, and the lack of evidence of a survival ad-vantage in those who have undergone resection of the primary tumor.
Features that were unique to this case and in-fluenced our initial treatment recommendations included our inability to clearly define the pri-mary site of the metastatic tumor, although we suspected that it was the colon. In addition, be-cause this was a poorly differentiated neuroen-docrine cancer, rather than a typical adenocarci-noma, we were unsure how it would respond to systemic chemotherapy. Initial staging studies suggested that the liver involvement was pre-dominantly in the right lobe. However, the portal vein appeared to be involved at its bifurcation and the left lobe most likely had small, difficult-to-delineate metastases. Therefore, we elected to perform an exploratory laparotomy and to resect the colonic tumor before the initiation of sys-temic chemotherapy. At the time of surgery, we noted that 90% of the right lobe of the liver had metastatic involvement; the left lobe of the liver also had metastatic involvement, which was con-firmed by biopsy. In addition, the patient was noted to have ascites.
Pathol o gic a l Discussion
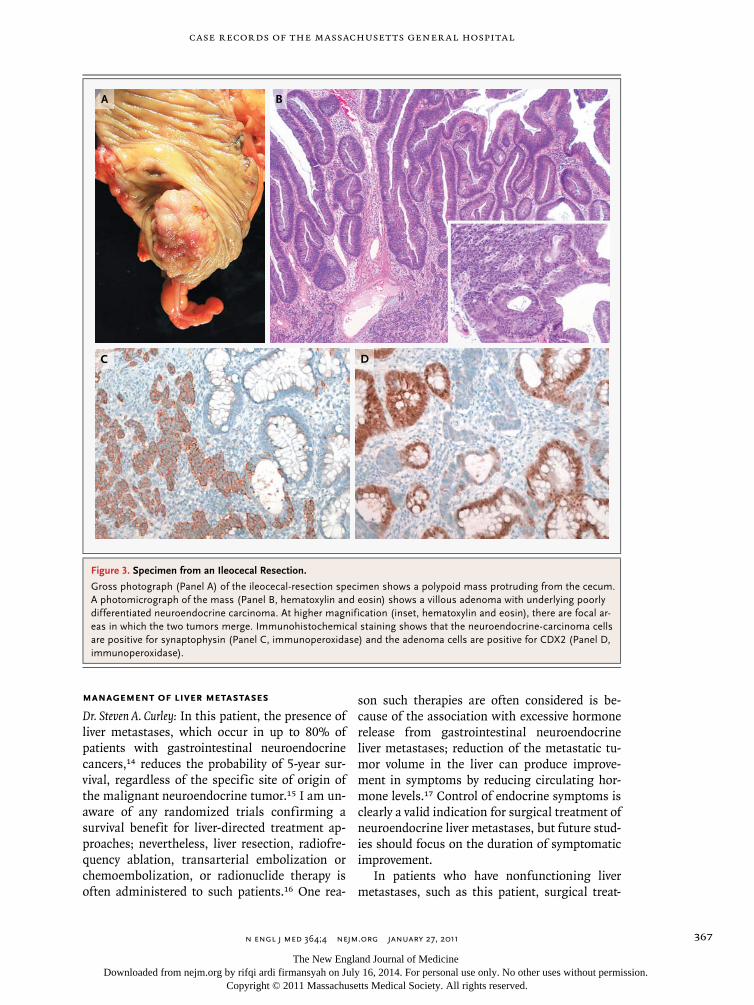
Dr. Zukerberg: The specimen from the ileocecal re-section consisted of a 3-cm segment of ileum and a 5-cm segment of cecum. A 4.1-cm polypoid exophytic mass protruded from the cecal mucosa (Fig. 3A). Microscopical examination showed a villous adenoma of the mucosal surface and an underlying poorly differentiated neoplasm (Fig. 3B). At higher magnification, it was evident that the poorly differentiated component of the tu-mor was a poorly differentiated neuroendocrine carcinoma with an appearance that was similar to that seen in the liver-biopsy specimen (Fig. 3B, inset). Although a majority of the poorly differ-entiated carcinoma appears separate from the adenoma, foci of apparent transition are seen. The neuroendocrine carcinoma infiltrated to the peritoneal surface, and there was extensive inva-sion of the vessels.
The cancer cells were positive for cytokeratin and synaptophysin (Fig. 3C), similarly to the liver tumor. CDX2, a marker of intestinal differentia-
tion, was expressed by the adenoma cells but not by the carcinoma (Fig. 3D). Fifteen lymph nodes were free of metastatic involvement. The biopsy specimen from the left lobe of the liver obtained at the time of surgery showed metastatic poorly differentiated neuroendocrine carcinoma.
The pathological diagnosis is a poorly dif-ferentiated neuroendocrine carcinoma, arising in a tubulovillous adenoma (tumor–node–metas-tasis pathologic stage T4bN0M1). Neuroendo-crine carcinomas of the gastrointestinal tract are rare, but the colorectal region is the second-most-common gastrointestinal site after the esophagus. In the colorectal region, the most common site is the rectum, followed by the ce-cum and then other sites within the colon.9,10 Neuroendocrine carcinomas may have mixed his-topathological features, as in this case, including areas of adenocarcinoma or squamous-cell car-cinoma, or they may be pure small-cell carcino-mas.11 Neuroendocrine carcinoma arising in a villous adenoma is extremely rare but has been reported.12,13
Discussion of M a nagemen t
Dr. Clark: This patient has a poorly differentiated neuroendocrine carcinoma of the colon. These cancers usually present with metastatic disease, with the most common site being liver, although it can also spread to distant lymph nodes, lungs, or bones. The most common presentation is ab-dominal pain, as we saw in this patient, followed by melena or obstruction. In general, patients with these tumors have a poor prognosis, with a median survival of 6 to 12 months and an overall 1-year survival of approximately 15%.9,10
We treated this patient with a regimen of cisplatin and etoposide, with a plan for 1 year of treatment. Peripheral neuropathy developed and progressed despite the substitution of carbopla-tin, so she received etoposide alone for her last cycle. As she completed her chemotherapy, we began treatment with octreotide, in hopes of suppressing any residual tumor. Octreotide has minimal toxic effects, and the results of a ran-domized study showed that it conferred a bene-fit with respect to progression-free survival in patients with well-differentiated neuroendocrine carcinoma.4 The peripheral neuropathy gradu-ally improved, and she described her quality of life as excellent.
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.
case records of the massachusetts gener al hospital
n engl j med 364;4 nejm.org january 27, 2011 367
Management of liver metastases
Dr. Steven A. Curley: In this patient, the presence of liver metastases, which occur in up to 80% of patients with gastrointestinal neuroendocrine cancers,14 reduces the probability of 5-year sur-vival, regardless of the specific site of origin of the malignant neuroendocrine tumor.15 I am un-aware of any randomized trials confirming a survival benefit for liver-directed treatment ap-proaches; nevertheless, liver resection, radiofre-quency ablation, transarterial embolization or chemoembolization, or radionuclide therapy is often administered to such patients.16 One rea-
son such therapies are often considered is be-cause of the association with excessive hormone release from gastrointestinal neuroendocrine liver metastases; reduction of the metastatic tu-mor volume in the liver can produce improve-ment in symptoms by reducing circulating hor-mone levels.17 Control of endocrine symptoms is clearly a valid indication for surgical treatment of neuroendocrine liver metastases, but future stud-ies should focus on the duration of symptomatic improvement.
In patients who have nonfunctioning liver metastases, such as this patient, surgical treat-
A B
DC
Figure3.SpecimenfromanIleocecalResection.
Gross photograph (Panel A) of the ileocecal-resection specimen shows a polypoid mass protruding from the cecum. A photomicrograph of the mass (Panel B, hematoxylin and eosin) shows a villous adenoma with underlying poorly differentiated neuroendocrine carcinoma. At higher magnification (inset, hematoxylin and eosin), there are focal ar-eas in which the two tumors merge. Immunohistochemical staining shows that the neuroendocrine-carcinoma cells are positive for synaptophysin (Panel C, immunoperoxidase) and the adenoma cells are positive for CDX2 (Panel D, immunoperoxidase).
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 364;4 nejm.org january 27, 2011368
ment is more often considered for potentially curative intent. Despite the apparent absence of prospective, randomized, controlled trials com-paring resection with other treatments for these patients, there are data demonstrating 5-year survival rates of 61 to 70%, with 10-year survival rates of 35% after resection.16 Radiofrequency ablation has also been used to treat patients with unresectable or multiple neuroendocrine liver metastases, but the long-term survival in this group is more difficult to assess.18 Some small studies have suggested 5-year survival rates as high as 56%, but these studies involved carefully selected patients, and these data can-not be applied as a general statement to all patients with liver metastases from gastrointes-tinal neuroendocrine cancers.16 Adjuvant treat-ments such as transarterial chemoembolization
or radionuclide therapy (yttrium-90 microspheres) led to better survival rates than did liver resec-tion alone in a nonrandomized study.19
Reducing the size of liver metastases with neoadjuvant therapy can make initially unresect-able disease in the liver, such as this patient has, resectable. I know of no data regarding the out-comes of patients who have had downsizing of their neuroendocrine liver metastatic disease with systemic chemotherapy; nonetheless, it is certainly possible that such a response followed by liver resection could lead to an improvement in long-term survival rates. If this patient’s liver metastases show a response to chemotherapy, I would propose the resection of any residual tu-mor that could be safely removed.
Dr. Cusack: In developing a surgical treatment plan for this patient, we first determined the extent of liver disease remaining after chemo-therapy.
Dr. Sahani: CT performed shortly before the initiation of chemotherapy revealed substantially more tumor burden in the liver than the initial images showed (Fig. 4A). However, after the completion of chemotherapy, CT scans showed substantial reduction in the size of the masses in the liver (Fig. 4B). Examination with com-bined positron-emission tomography (PET) and CT revealed an absence of metabolic activity in the remaining liver lesions and no evidence of PET-avid lesions elsewhere in the body.
Dr. Cusack: The patient had a dramatic re-sponse to chemotherapy. Curative resection would require an extended right hepatectomy and partial resection of the remaining left lat-eral segment of the liver. To assess the regenera-tive capacity of the liver, we performed emboli-zation of the right portal vein and measured the degree of hypertrophy over time in the remain-ing left lateral segment, where two small foci of metastatic disease remained.
Dr. Sahani: MRI examination before and 3 months after right portal-vein embolization (Fig. 1 of the Supplementary Appendix, available with the full text of this article at NEJM.org) confirmed the reduction in tumor burden and the absence of new disease. The volume of the left lobe, estimated from the MRI images, showed a 5% increase after embolization of the right portal vein, from 1196.7 ml to 1264.7 ml.
Dr. Cusack: On the basis of these results, we felt confident proceeding with a staged liver resec-
A
B
Figure4.ImagingStudiesbeforeandafterChemo-therapy.
An axial image from contrast-enhanced CT before the initiation of chemotherapy (Panel A) reveals an in-crease in the size of the dominant mass (arrow) and new lesions (arrowheads) in the liver. A CT image after completion of chemotherapy (Panel B) shows a marked reduction in the tumor burden (arrow).
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 364;4 nejm.org january 27, 2011 369
tion. I performed an extended right hepatectomy, and I examined the left lobe of the liver, where we identified two residual scars, in segments two and three (one anteriorly and one posteriorly). We were able to resect the tumor in the right lobe and in segment four and clear the margins. Three months later, the patient had no evidence of cancer outside the liver, and we removed the remaining tumor from the left lobe of the liver.
Dr. Zukerberg: Resection of a portion (14 cm by 13 cm by 7 cm) of the right lobe of liver showed a 1.2-cm firm, well-circumscribed mass that did not extend to the resection margins. Sections showed metastatic, poorly differentiated neuro-endocrine carcinoma with areas of necrosis and fibrosis. Numerous embolic particles were pres-ent in portal vessels and had an associated his-tiocytic reaction with giant cells. The surround-ing liver parenchyma showed collapse, fibrosis, and inflammation secondary to the embolic treatment, but the rest of the liver, away from the embolized areas, looked normal. The subse-quent resection from the left lobe of the liver showed only scar with no residual cancer.
Dr. Clark: The patient did well after the surgi-cal resections, which were completed 20 months after her initial presentation. We continued maintenance therapy with octreotide. Unfortu-nately, 3 months after the second liver resection, right-sided chest and abdominal pain developed, and imaging studies showed recurrent disease in the liver, chest, ribs, and vertebrae. At this point, we had a long discussion with the patient about whether to proceed with chemotherapy or move to supportive care. She had a very strong wish to
live as long as possible, to be with her grandchil-dren, and opted to proceed with chemotherapy, even though the likelihood of prolonged benefit was small. The tumor progressed despite the initiation of chemotherapy with FOLFIRI plus bevacizumab (which we chose because of the association of her neuroendocrine carcinoma with a villous adenoma and because of the re-ported activity of irinotecan and fluorouracil in neuroendocrine carcinomas1-3) and subsequently a trial of etoposide as a single agent. At that point, she made the decision to move to hospice care. The patient died 2 years 3 months after the initial diagnosis.
The patient was sure that the aggressive ap-proach to her disease was worthwhile. Neverthe-less, we need to do a better job of identifying which patients with poorly differentiated neuro-endocrine tumors might derive long-term bene-fits from aggressive treatment. We hope that better molecular genetic characterization of these tumors will help in such identification and will also help to define better treatments for patients such as this one.
A nat omic a l Di agnosis
Poorly differentiated neuroendocrine carci-noma arising in a tubulovillous adenoma of the cecum, with metastasis to the liver.
This case was presented at the postgraduate course Advances in Cancer Management for the Surgeon, 2009, sponsored by the Department of Continuing Education, Harvard Medical School.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References1. Varadhachary GR, Greco FA. Over-view of patient management and future directions in unknown primary carcino-ma. Semin Oncol 2009;36:75-80.2. Spigel DR, Hainsworth JD, Greco FA. Neuroendocrine carcinoma of unknown primary site. Semin Oncol 2009;36:52-9.3. Clark OH, Benson AB III, Berlin JD, et al. NCCN clinical practice guidelines in oncology: neuroendocrine tumors. J Natl Compr Canc Netw 2009;7:712-47.4. Rinke A, Müller HH, Schade-Brittinger C, et al. Placebo-controlled, double-blind, prospective, randomized study on the ef-fect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin On-col 2009;27:4656-63.5. Chan JA, Kulke MH. Progress in the
treatment of neuroendocrine tumors. Curr Oncol Rep 2009;11:193-9.6. Lobins R, Floyd J. Small cell carcino-ma of unknown primary. Semin Oncol 2007;34:39-42.7. Martin R, Paty P, Fong Y, et al. Simul-taneous liver and colorectal resections are safe for synchronous colorectal liver me-tastasis. J Am Coll Surg 2003;197:233-42.8. Poultsides GA, Servais EL, Saltz LB, et al. Outcome of primary tumor in patients with synchronous stage IV colorectal can-cer receiving combination chemotherapy without surgery as initial treatment. J Clin Oncol 2009;27:3379-84.9. Bernick PE, Klimstra DS, Shia J, et al. Neuroendocrine carcinomas of the colon and rectum. Dis Colon Rectum 2004;47: 163-9.10. Cebrian J, Larach SW, Ferrara A, et al.
Small-cell carcinoma of the rectum: report of two cases. Dis Colon Rectum 1999;42: 274-7.11. Li AF, Li AC, Hsu CY, Li WY, Hsu HS, Chen JY. Small cell carcinomas in gastro-intestinal tract: immunohistochemical and clinicopathological features. J Clin Pathol 2010;63:620-5.12. Ispas C, Yu J, Tarantino DR, Lara JF. Pathologic quiz case: a 44-year-old woman with a tubulovillous adenoma of the colon and liver and bone lesions: small cell (neuroendocrine) carcinoma of the colon with metastasis and an associated, overly-ing villous adenoma. Arch Pathol Lab Med 2005;129:412-4.13. Vilor M, Tsutsumi Y, Osamura RY, et al. Small cell neuroendocrine carcinoma of the rectum. Pathol Int 1995;45:605-9.14. Mignon M. Natural history of neuro-
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.

n engl j med 364;4 nejm.org january 27, 2011370
case records of the massachusetts gener al hospital
endocrine enteropancreatic tumors. Diges-tion 2000;62:Suppl 1:51-8.15. Scigliano S, Lebtahi R, Maire F, et al. Clinical and imaging follow-up after ex-haustive liver resection of endocrine me-tastases: a 15-year monocentric experi-ence. Endocr Relat Cancer 2009;16:977-90.16. Gurusamy KS, Ramamoorthy R, Sharma D, Davidson BR. Liver resection versus other treatments for neuroendo-
crine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev 2009;2:CD007060.17. Norton JA, Warren RS, Kelly MG, Zuraek MB, Jensen RT. Aggressive surgery for metastatic liver neuroendocrine tu-mors. Surgery 2003;134:1057-65.18. Elias D, Goéré D, Leroux G, et al. Combined liver surgery and RFA for pa-tients with gastroenteropancreatic endo-
crine tumors presenting with more than 15 metastases to the liver. Eur J Surg On-col 2009;35:1092-7.19. Landry CS, Scoggins CR, McMasters KM, Martin RC II. Management of he-patic metastasis of gastrointestinal carci-noid tumors. J Surg Oncol 2008;97:253-8.Copyright © 2011 Massachusetts Medical Society.
Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
The New England Journal of Medicine Downloaded from nejm.org by rifqi ardi firmansyah on July 16, 2014. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.





























