-
7/27/2019 Nej m Cpc 1103562
1/12
case records of themassachusetts general hospital
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 366;4 nejm.org january 26, 2012 361
Founded by Richard C. CabotNancy Lee Harris, m.d., Editor Eric
S. Rosenberg, m.d., Associate EditorJo-Anne O. Shepard,
m.d.,Associate Editor Alice M. Cort, m.d.,Associate EditorSally H.
Ebeling,Assistant Editor Christine C. Peters, Assistant Editor
Case 3-2012: A Newborn Boy with Vomiting,Diarrhea, and Abdominal
Distention
Elliot Melendez, M.D., Allan M. Goldstein, M.D.,Pallavi Sagar,
M.D., and Kamran Badizadegan, M.D.
From the Department of Pediatrics, Chil-drens Hospital (E.M.);
the Departmentsof Pediatrics (E.M.), Surgery (A.M.G.), Radi-ology
(P.S.), and Pathology (K.B.), Massa-chusetts General Hospital; and
the Depart-ments of Pediatrics (E.M.), Surgery (A.M.G.),Radiology
(P.S.), and Pathology (K.B.), Har-vard Medical School all in
Boston.
N Engl J Med 2012;366:361-72.Copyright 2012 Massachusetts
Medical Society.
Presentation of Case
Dr. Rebecca C. Bell (Pediatrics): A 6-day-old boy was admitted
to this hospital becauseof vomiting, diarrhea, and abdominal
distention.
The patient was born at another hospital to a teenaged
primigravida by vaginaldelivery after a full-term, uncomplicated
gestation. The mother had received pre-natal care; she had no
history of sexually transmitted infections, and prenatalscreening
tests were negative. Meconium was present at delivery. The
patientsbirth weight was 4.3 kg (95th percentile), and the 1-minute
and 5-minute Apgarscores were 7 and 9, respectively. Breast-feeding
was initiated. The newborn passedtwo stools on the second day (the
first at 30 hours of age). The next day, he report-edly had one
loose, green stool. He was discharged home at 50 hours of age.
Helived with his mother and her parents. When he was 3 and 4 days
of age, he vom-ited yellow-green emesis on several occasions. He
was otherwise well and breast-feeding regularly. At 3 a.m. on the
day of admission, he became fussy and did notcomplete his normal
feeding. Between 3 a.m. and 9 a.m., approximately six epi-sodes of
vomiting (initially breast milk, followed by mucus) occurred, with
in-creasingly foul-smelling emesis. Diarrhea developed, and urine
output decreased.Later that morning, he became less active;
abdominal distention developed, andhe stopped voiding. He was taken
to a clinic affiliated with this hospital. On ex-amination, he
appeared tired, with intermittent grunting. The rectal
temperaturewas 38.0C. The abdomen was distended and tender, with
hypoactive bowel sounds;stool was positive for occult blood. He was
transported by ambulance to the emer-
gency department of this hospital.On examination, the patient
appeared alert and slightly uncomfortable. The tem-perature was
37.2C, the pulse 160 beats per minute, the respiratory rate 30
breathsper minute, and the oxygen saturation 100% while he was
breathing ambient air.The weight was 3.9 kg. The abdomen was
distended, soft, and tympanic, with de-creased bowel sounds. There
were small, bilateral noncommunicating hydroceles.The remainder of
the examination was normal. A stool specimen showed no occultblood.
Urinalysis revealed clear orange urine, with a specific gravity
greater than1.030, pH 6.5, nitrites, 1+ urobilinogen, 3+ bilirubin,
2+ albumin, and trace whitecells, blood, glucose, and ketones.
Urinalysis also revealed 0 to 2 red cells, 3 to 5 white
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
2/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 366;4 nejm.org january 26, 2012362
Table 1. Laboratory Data.*
VariableReference Range,
Age-Adjusted On Admission 2nd Hospital Day 3rd Hospital Day
Hematocrit (%) 45.067.0 66.0 (manual) 62.6 48.8
Hemoglobin (g/dl) 14.522.5 21.0 16.3
White-cell count (per mm3) 940034,000 14,300 7000 6200
Differential count (%)
Neutrophils 5362 29 24 18 (ref 3048)
Band forms 010 19 1
Lymphocytes 2134 32 53 61 (ref 4081)
Monocytes 411 15 17 18
Eosinophils 08 4 0
Basophils 03 1 2
Metamyelocytes 0 5 1
Platelet count (per mm3) 150,000450,000 179,000 157,000
65,000
Sodium (mmol/liter) 135145 138 136 140
Potassium (mmol/liter) 4.05.6 7.1 (hemolyzed) 3.5 3.5
Chloride (mmol/liter) 98106 113 110 110
Carbon dioxide (mmol/liter) 19.022.0 17.1 22.5
Urea nitrogen (mg/dl) 520 46 34 19
Creatinine (mg/dl) 0.301.00 0.60 0.43
Glucose (mg/dl) 60100 141 185 124Bilirubin (mg/dl)
Total 2.015.0 0.7 0.8
Direct 0.53.5 0.1 0.1
Protein (g/dl)
Total 6.08.3 3.2 3.3
Albumin 3.35.0 1.6 1.9
Globulin 2.64.1 1.6 1.4
cells, moderate bacteria, and a few squamous andrenal tubular
cells per high-power field. Ampicil-lin, gentamicin, and boluses of
normal saline wereadministered. Other test results are shown
inTable 1. Radiographs of the abdomen showeddilated loops of bowel
in the lower abdomen,which were suggestive of distal bowel
obstruc-
tion. There was no free air. An upper gastro-intestinal series
showed severe gastroesophagealreflux without evidence of
malrotation. An en-ema administered with a water-soluble
contrastagent revealed free flow of contrast material,with a long
segment of narrowing involving therectum and distal sigmoid colon
and proximaldistention of the descending colon. No stricturewas
identif ied. Rectal examination performed
after the enema did not reveal blood or mucus.After the enema,
the patient passed multiple non-bloody stools, and the abdominal
distentiondecreased.
Seven hours after arrival in the emergency de-partment, the
temperature rose to 38.7C; acet-aminophen was administered. Lumbar
puncture
was performed; analysis of cerebrospinal fluid isshown in Table
2. Acyclovir was administered.The patient was admitted to the
pediatric service.Shortly after admission, the temperature rose
to39.1C and the pulse to 179 beats per minute, withpoor capillary
refill. He was transferred to thepediatric intensive care unit.
Vancomycin andadditional crystalloid were administered
intrave-nously. During the first day, increasing abdomi-
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
3/12
case records of the massachusetts general hospital
n engl j med 366;4 nejm.org january 26, 2012 363
nal distention, poor perfusion (as evidenced bycool
extremities), and respiratory failure devel-oped. A nasogastric
tube was placed.
A continuous infusion of dopamine followedby norepinephrine was
administered, and the tra-chea was intubated. Transthoracic
echocardiogra-phy revealed a patent foramen ovale, a smallpatent
ductus arteriosus with left-to-right shunt-
ing, and normal ventricular function. Stoolsbecame positive for
occult blood, and perianalexcoriation developed. Serum levels of
lactate,aspartate aminotransferase, and alkaline phos-phatase were
normal; other test results are shownin Table 1. A repeat abdominal
radiographshowed multiple distended loops of small bowelcontaining
residual contrast material and relativedecompression of the large
bowel. Surgical con-sultants inserted a femoral central venous
cathe-
ter and a radial arterial catheter. The administra-tion of
ampicillin was stopped, and meropenemwas begun; pressors were
adjusted to maintain amean arterial pressure between 50 and 60 mm
Hg.
Urine obtained by catheter on admission wascultured and grew few
nonhemolytic streptococci(1000 to 10,000 colonies per milliliter;
the strep-tococci were consistent with viridans group
streptococci and were thought to be a contami-nant); a blood
culture was sterile. Screening ofnasal specimens for respiratory
viruses and en-terovirus and of stool cultures for enteric
patho-gens and enterovirus was negative. On the thirdday, serum
levels of lactate, magnesium, andionic calcium were normal; other
test results areshown in Table 1. Bicarbonate and immune globu-lin
were administered intravenously. Total paren-teral nutrition was
begun.
Table 1. (Continued.)
VariableReference Range,
Age-Adjusted On Admission 2nd Hospital Day 3rd Hospital Day
Phosphorus (mg/dl) 4.59.0 3.0
Calcium (mg/dl) 8.510.5 7.3
Alanine aminotransferase (U/liter) 1055 88 65
d-Dimer (ng/ml)
-
7/27/2019 Nej m Cpc 1103562
4/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 366;4 nejm.org january 26, 2012364
Table 2. Analysis of Cerebrospinal and Peritoneal Fluid.*
Variable Cerebrospinal Fluid Peritoneal Fluid
Reference Range Day of Admission Reference Range 6th Day
Color and turbidity Colorless, clear Colorless, clear Yellow,
clear Yellow, slightly turbid
White-cell count (per mm3) 01000 1130 (11% neutrophils, 1%
bandforms, 81% lymphocytes, 1%
monocytes, 6% plasma cells)
Tube 1 030 37 (29% lymphocytes, 71% mono-cytes)
Tube 4 030 11 (2% neutrophils, 21% lympho-cytes, 73% monocytes,
4%macrophage or lining cells)
Red-cell count (per mm3) 0 1585
Tube 1 0 21
Tube 4 0 0
Glucose (mg/dl) 5075 120
Protein (mg/dl) 555 48 Not defined 2200
Sodium (mmol/liter) Not defined 139Potassium (mmol/liter) Not
defined 3.2
Chloride (mmol/liter) Not defined 105
Carbon dioxide (mmol/liter) Not defined 32.2
Lactate dehydrogenase (U/liter) Not defined 140
Amylase (U/liter) Not defined
-
7/27/2019 Nej m Cpc 1103562
5/12
case records of the massachusetts general hospital
n engl j med 366;4 nejm.org january 26, 2012 365
and results of renal- and hepatic-function testsimproved.
Acyclovir and vancomycin were stopped,and furosemide was
administered for gradualdiuresis.
During the second week, the patients vitalsigns and clinical
condition gradually stabi-lized. Gentamicin and dopamine were
stopped,
norepinephrine was weaned, and gradual diure-sis continued.
On the 14th day, a diagnostic procedure wasperformed.
Differential Diagnosis
Evaluation and Management of Neonatal Sepsis
Dr. Elliot Melendez: All discussants are aware of thediagnosis
in this case. This 6-day-old boy presentedwith signs of sepsis.
Although viruses are themost common infectious cause of fever in
infants,
the prevalence of urinary-tract infection, bacte-remia, and
meningitis in patients less than 28 daysold is between 8.8% and
13.3%.1,2 For this reason,cultures from urine, blood, and
cerebrospinal fluidwere obtained. The most common bacterial
patho-gens are group B streptococci, Escherichia coli, andListeria
monocytogenes: thus, the administration ofbroad-spectrum
antibiotics was initiated. Herpessimplex virus, a dangerous but
potentially treat-able virus, was considered, and the
administrationof acyclovir was initiated. Stool was reported
asheme-positive in the clinic; it was heme-negativewhen the patient
arrived at this hospital, but be-cause of the abdominal distention,
an abdominalsource was considered. If bloody diarrhea is pres-ent,
stool cultures for enteric bacterial pathogensmust be sent.
Appropriately, the neonate was ad-mitted for observation and
continuation of anti-biotics pending culture results. On admission,
hewas recognized as having respiratory distress andcardiovascular
dysfunction, as evidenced by poorcapillary refill. He was
transferred to the pediat-ric intensive care unit, where
respiratory failure
subsequently developed, and his condition metthe consensus
definition of severe sepsis.3
Severe sepsis with shock is associated withan imbalance between
oxygen delivery and de-mand. The treatment strategy to correct this
im-balance is referred to as early goal-directed thera-py. Rivers
et al.4 found that in adults a sepsisalgorithm with targeted goals
in managementcan reduce mortality rates among patients withsevere
sepsis and shock. Unfortunately, in pedi-
atrics, there are very little data on the use of
earlygoal-directed therapy beyond aggressive fluid ad-ministration.
Nevertheless, the principles of earlygoal-directed therapy are the
same for both chil-dren and adults.
Oxygen was administered to improve oxygendelivery. If there are
signs of respiratory insuf-
ficiency, early endotracheal intubation should beconsidered, as
it was in this neonate. The historysuggested the presence of
absolute hypovolemia,probably due to increased insensible water
lossesfrom fever and tachypnea, as well as vomiting,diarrhea, and
poor oral intake. Aggressive fluidresuscitation was given in the
form of 0.9% salinein boluses of 20 ml per kilogram of body
weightover a period of 5 to 10 minutes and repeatedas long as signs
and symptoms of shock per-sisted. Ringers lactate would also have
beenacceptable. After the administration of 60 ml per
kilogram, vasopressor therapy should be admin-istered if the
blood pressure remains low; how-ever, more fluid can safely be
given as long asthere is no evidence of heart failure or
volumeoverload.
Children are more likely than adults to havecardiac dysfunction
in severe sepsis or shock,with 58% having low cardiac output and
highsystemic vascular resistance and 22% having bothlow cardiac
output and low systemic vascular re-sistance.5 As a result, because
of its vasopressiveand inotropic properties, the administration
ofdopamine was begun in this patient. The use ofsubsequent agents
should depend on the clinicalresponse and the predominant
hemodynamicderangement. Because this patient had persis-tent shock
with vasodilatation (warm shock),norepinephrine was subsequently
added. Oncethe neonate was receiving dopamine and norepi-nephrine,
an echocardiogram was obtained, whichruled out congenital heart
disease.
Adequate control of fever can reduce meta-bolic activity and
oxygen demand. Since some
children have tachypnea or agitation, early con-trol of the
airway with sedation and analgesia,as was performed in this
patient, can also bebeneficial. Finally, prompt empirical
treatmentof infection can reduce the metabolic demand bythe
inflamed tissue.
Finally, a search should continue for a poten-tial source of
infection that can be controlled.Patients with infected indwelling
foreign objects,such as central catheters, should have these
objects
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
6/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 366;4 nejm.org january 26, 2012366
removed. Patients with necrotic wounds shouldundergo dbridement.
Abscesses should be drained,preferably by minimally invasive
techniques. Inthis patient, who had progression of
abdominaldistention and development of bloody stools,
anintraabdominal source of infection was likely,and we requested
surgical consultation to assist
with further evaluation and treatment.
Bilious emesis, liquid stools, and abdominal
distention in a neonate
Dr. Allan M. Goldstein: This neonate presented withbilious
emesis, liquid stools, and abdominal dis-tention. In the
differential diagnosis of a poten-tial intraabdominal process in
this newborn, life-threatening conditions need to be considered
first.
Intestinal Malrotation
Bilious emesis in newborns immediately raises
concern for intestinal malrotation with midgutvolvulus, a
condition requiring prompt treatment.Abdominal distention and
heme-positive diar-rhea, as in this patient, can occur in
malrotationwith intestinal ischemia. A timely upper
gastro-intestinal series should be performed to rule
outmalrotation.
Necrotizing Enterocolitis
Necrotizing enterocolitis typically occurs in pre-mature
neonates, although 10% of cases occur infull-term neonates.6 The
onset of necrotizing en-terocolitis in premature neonates is often
delayed,but in full-term neonates it can develop within thefirst
week of life.6 Necrotizing enterocolitis is un-likely in this
patient because of the absence of pneu-matosis intestinalis on
abdominal radiographs.
Enterocolitis Associated with Hirschsprungs Disease
Enterocolitis associated with Hirschsprungs dis-ease
(Hirschsprungs-associated enterocolitis) isa critical diagnosis
that fits this newborns pre-sentation. Patients with Hirschsprungs
disease,
a congenital intestinal neuropathy characterizedby the absence
of ganglion cells extending fromthe rectum proximally for a
variable distance, pre-sent with failure to pass meconium within 48
hoursafter birth and often progress to abdominal dis-tention and
vomiting.7 In healthy newborns, 94 to99% pass meconium by 24 hours,
and 100% by48 hours.8,9 In newborns with Hirschsprungs dis-ease,
only 6% pass meconium by 24 hours,7 and37 to 54% by 48 hours7,10
This patient first passed
meconium at 30 hours of life, a finding consis-tent with
Hirschsprungs disease. Vomiting, dis-tention, loose stools, and
fever occur, as in thispatient, when Hirschsprungs disease is
compli-cated by enterocolitis. In children with knownHirschsprungs
disease, enterocolitis is the mostserious complication. Even in
infants and neonates
without known Hirschsprungs disease, the diag-nosis should be
considered, since up to 12% of pa-tients who are ultimately found
to have Hirsch-sprungs disease present with
enterocolitis.11,12Infectious gastroenteritis, allergic colitis
(allergyto milk protein), and metabolic disorders arealso possible
in this patient but should be consid-ered only after the critical
diagnoses of Hirsch-sprungs disease and enterocolitis have
beenruled out.
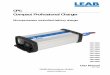
May we review the imaging studies?Dr. Pallavi Sagar: Radiographs
of the abdomen
taken with the patient in the supine and decubi-tus positions
(Fig. 1A and 1B, respectively) re-veal dilated loops of bowel with
airliquid levelsin the right abdomen, as well as a
small-caliberrectum. These findings are worrisome for ob-struction
of the distal bowel. There is no free airor pneumatosis. An upper
gastrointestinal series(Fig. 1C) shows severe, spontaneous
gastroesoph-ageal reflux. There is no evidence of malrotation.An
enema administered with a water-soluble con-trast agent (Fig. 1D)
reveals free flow of contrastmaterial from the rectum to the
ascending colonwithout evidence of a stricture. There is narrow-ing
of a long segment that has an irregularmucosal outline and involves
the rectum anddistal sigmoid colon, with reversal of the
recto-sigmoid index and a funnel-like transition into adilated
proximal sigmoid and descending colon.The transverse colon and
ascending colon arealso dilated. These findings are worrisome
fordistal bowel obstruction secondary to Hirsch-sprungs disease.
The irregular mucosal outlinemay represent dyskinetic contractions
of the
aganglionic segment or colitis.An abdominal ultrasonogram
obtained onthe fifth hospital day (Fig. 1E) shows abundantascites
with multiple internal septations, fea-tures of concern for
peritonitis. Overall, thesefeatures suggest distal bowel
obstruction, mostlikely due to Hirschsprungs disease, with
colitisand peritonitis.
Dr. Goldstein: The findings on a barium enemaexamination a
contracted rectosigmoid with a
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
7/12
case records of the massachusetts general hospital
n engl j med 366;4 nejm.org january 26, 2012 367
dilated descending colon are characteristic ofHirschsprungs
disease, and the sawtooth patternof irregularity in the rectal
mucosa is of concern
for enterocolitis. These clinical and radiographicfeatures all
point to the diagnosis of Hirsch-sprungs disease with
Hirschsprungs-associatedenterocolitis. Prompt recognition and early
treat-ment are essential. A definitive diagnosis ofHirschsprungs
disease requires examination ofa rectal-biopsy specimen to confirm
agangliono-sis. However, because of the acute inflammationin this
patient, performing the biopsy needs tobe deferred until the
inflammation subsides,
and treatment must be initiated on the basis ofa presumptive
diagnosis.
The incidence of enterocolitis in patients with
Hirschsprungs disease varies widely, from 17% to34%,11-14 partly
because of a lack of a standardizeddefinition. Patients with
Hirschsprungs-associ-ated enterocolitis can present with symptoms
rang-ing from mild abdominal distention with diar-rhea to septic
shock, as in this patient.11,15,16
Lethargy and bloody stools can occur. Even milddiarrhea and
abdominal distention in a patient withHirschsprungs disease or in a
neonate such as thisone, with delayed passage of meconium,
should
A B
DC E
Figure 1. Radiographic and Ultrasound Images of the Abdomen.
Supine (Panel A) and left lateral decubitus (Panel B) views show
dilated loops of bowel with airliquid levels and
without evidence of rectal air, features suggestive of distal
bowel obstruction. There is severe spontaneous gastro-esophageal
reflux to the cervical esophagus (Panel C, arrow). An enema
administered with a water-soluble contrast
agent (Panel D) reveals narrowing of the rectum and sigmoid
(arrow) with funnel transition to the descending colon(arrowhead).
Mucosal irregularity of the narrowed segment suggests dyskinetic
irregular contractions or colitis. An
abdominal ultrasonogram (Panel E) shows ascites with internal
septations (arrow) that are suggestive of peritonitis.
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
8/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 366;4 nejm.org january 26, 2012368
prompt consideration of Hirschsprungs-associatedenterocolitis in
order to avoid a delay in treatmentand the associated
complications. Hirschsprungs-associated enterocolitis remains the
leadingcause of death in patients with Hirschsprungsdisease,
although with increased awareness,earlier diagnosis, and improved
management,
the mortality rate associated with the disease hasdecreased from
33%15 to approximately 1%.13
Management of Hirschsprungs-Associated Enterocolitis
Mild cases of Hirschsprungs-associated entero-colitis can be
treated with oral metronidazoleand rectal dilatation to relax the
anal sphincterand allow the passage of stool. This patient
pre-sented with severe enterocolitis, which
requireshospitalization, bowel rest, and broad-spectrumantibiotics
that target bowel flora.13 Rectal irriga-tion twice daily with 30
to 50 ml of warm saline
applied through a flexible rectal catheter untilthe eff luent is
clear, performed to evacuate stoolfrom the colon, is an important
component oftreatment.15 Rectal irrigations or dilatations,which
could have decreased the severity and du-ration of this patients
illness, were not per-formed. In patients whose condition does
notimprove with these measures, colostomy or ileos-tomy can be
life-saving. This newborns condi-tion ultimately improved with
aggressive medicalsupport, and he did not require diversion.
After the enterocolitis resolves in this patient,tissue obtained
by rectal suction biopsy shouldbe examined to confirm the diagnosis
ofHirschsprungs disease, and then definitive sur-gery should be
planned to remove the agangli-onic bowel. Despite definitive
surgery, this pa-tient is at risk for recurrence of
enterocolitis.Recurrence occurs in 10 to 42% of patients;
thereasons are unclear.13,16-19 Trisomy 21 has beenidentified as a
risk factor for Hirschsprungs-associated enterocolitis,12,20 as
have long-segmentaganglionosis,11,14 prior enterocolitis,11,14 and
anas-
tomotic stricture.21,22
Most important, the patientsfamily must be made aware of the
early signs ofenterocolitis and the importance of seekingprompt
evaluation, and clinicians need to remainvigilant for this devastat
ing Hirschsprungs-related complication.
Dr. Elliot Melendezs Diagnosis
Severe sepsis most likely due to an intraabdominalsource.
Dr. Alla n M. Goldsteins
Diagnosis
Hirschsprungs disease complicated by entero-colitis.
Pathological Discussion
Dr. Kamran Badizadegan: The first diagnostic pro-cedure was a
suction biopsy that was performedto obtain rectal tissue.
Alternative surgical pro-cedures, such as deep mucosal or
full-thicknessrectal biopsies, may also be performed but oftenare
not because of the increased risk of complica-tions. The diagnosis
of Hirschsprungs diseaserequires an adequate volume of the
submucosa toconfirm the absence of ganglion cells. In thiscase, the
specimen was small, yielding fewerthan 25 consecutive 5-m sections
with super-
ficial submucosa (Fig. 2A). Criteria for specimenadequacy vary,
although a mucosal-biopsy speci-men measuring 2 to 3 mm in diameter
and 1 mmin depth is generally considered adequate for di-agnosis.23
The diagnosis of Hirschsprungs dis-ease is confirmed by the absence
of ganglioncells on at least 75 consecutive 5-m sections
oftissue.23 Thus, although no ganglion cells wereidentif ied, the
small specimen precluded defini-tive evaluation for Hirschsprungs
disease. A re-peat biopsy was therefore recommended, and anadequate
specimen was obtained (Fig. 2B), withno identifiable ganglion cells
in 90 consecutivesections, a f inding consistent with
Hirschsprungsdisease.
Ideal specimen size and technical quality arenot always
achieved; therefore, the diagnosis ofHirschsprungs disease is often
supported bysecondary or ancillary criteria, such as analysisof
submucosal nerve fibers, histochemical stain-ing for
acetylcholinesterase, and immunostainingfor calretinin.
Hypertrophic submucosal nervesmeasuring more than 40 m in diameter
are
highly characteristic of Hirschsprungs disease.24
Although it is assumed that this f inding representscompensatory
hypertrophy of extrinsic nerves inthe absence of intrinsic neurons,
data to supportthis hypothesis are lacking. Support of the
diag-nosis in this case was provided by identification
ofhypertrophic submucosal nerves (Fig. 2B). His-tochemical staining
for acetylcholinesterase onfrozen sections of mucosal-biopsy
specimens inHirschsprungs disease often reveals the presenceof
abnormal acetylcholinesterase-positive neurites
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
9/12
case records of the massachusetts general hospital
n engl j med 366;4 nejm.org january 26, 2012 369
within the muscularis mucosae and has long beenan invaluable
ancillary technique. In this case, weidentified abnormal
acetylcholinesterase-positiveneurites on a frozen-section slide
(Fig. 2C).
Studies published after this patients diagnosiswas established
indicate that the absence ofcalretinin-positive mucosal neurites on
immuno-histochemical staining of paraffin sections is ahighly
sensitive marker for Hirschsprungs dis-ease.25,26 Calretinin is a
calcium-binding proteinthat is normally expressed in cholinergic
nerves;it is not known why calretinin-positive mucosalneurites are
absent in Hirschsprungs diseaseand abnormal
acetylcholinesterase-positive neu-rites are present.
Retrospectively, the original
suction-biopsy specimen was immunostainedfor calretinin and
shows complete absence ofcalretinin-positive neurites (Fig. 2D and
2E). Theavailability of this stain may permit the diag-
nosis of Hirschsprungs disease on specimensthat were previously
considered inadequate.25,26
There was no evidence of active colitis on eitherbiopsy.
Discussion of M anagement
Dr. Goldstein: The biopsy in this case confirmedthe diagnosis of
Hirschsprungs disease. Defini-tive management requires resection of
the agan-glionic segment of colon, bringing normally in-
A B
DC E
Figure 2. Suction-Biopsy Specimens of Rectal Tissue.
The original rectal tissue obtained with the use of a
suction-biopsy instrument (Panel A, hematoxylin and eosin) did
not show ganglion cells, but the biopsy specimen was considered
too small for definitive diagnosis of Hirschsprungsdisease.
However, a specimen from the repeat suction biopsy (Panel B,
hematoxylin and eosin) contained ample sub-
mucosa with no ganglion cells on more than 90 serial sections
and markedly hypertrophic nerves (arrowheads). In
addition, histochemical staining for acetylcholinesterase on an
accompanying frozen-section slide (Panel C) highlightedthickened
and irregular neurites within the lamina propria and the muscularis
mucosae (arrowheads), supporting thediagnosis of Hirschsprungs
disease. The original biopsy specimen (Panel A) was retrospectively
immunostained for
calretinin (Panel D) and showed a complete absence of
calretinin-positive elements, a feature consistent with
thisdiagnosis (immunoperoxidase stain for calretinin). Normal
expression of calretinin-positive neurites is highlighted
in a control specimen (Panel E, arrows; immunoperoxidase stain
for calretinin). The solid bar represents 200 m inPanels A and B,
and 50 m in Panels C, D, and E.
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
10/12
-
7/27/2019 Nej m Cpc 1103562
11/12
case records of the massachusetts general hospital
n engl j med 366;4 nejm.org january 26, 2012 371
disease, whose intestinal tracts seem particularlysensitive to
any perturbations. It is often difficultto determine whether the
symptoms are due togastroenteritis or enterocolitis. However, it is
bet-ter to assume that it is enterocolitis and treat
withantibiotics and rectal irrigations or dilatations,since
enterocolitis can progress rapidly, as was
seen in this newborn. This case emphasizes that,even after the
aganglionic colon has been re-moved, one must remain vigilant for
the diagno-sis of enterocolitis, since the risk persists.
Dr. Nancy Lee Harris(Pathology): Dr. Cronin, youare this
patients pediatrician. Would you tell ushow he is doing?
Dr. Rebecca M. Cronin (Pediatrics): This patientis now 2 years
old and is doing well medically,despite all his hospital
admissions. The pri-mary care of a patient such as this one with
achronic medical illness requires educating the
family about the potential complications of thisillness and the
potential for recurrence. Althoughthe patients mother is very
young, she has doneremarkably well caring for him and has
broughthim promptly to medical attention when neces-sary. One issue
this family has had to deal withis behavioral problems. Chronically
ill and fre-quently hospitalized children are often seen
asvulnerable, and it is hard for parents to consis-tently and
appropriately discipline them. Forexample, toilet training for this
patient is goingto require consistent limit setting. Since
lifelongconstipation is a serious possible consequenceof
Hirschsprungs disease, establishing goodbowel habits will be
important to his overallhealth. We have involved child life
specialists
and early intervention specialists, who can helpwith developing
good skills for parenting illchildren.
Dr. Harris: Are these parents at risk for havinganother affected
child?
Dr. Goldstein: Hirschsprungs disease is a multi-factorial
disorder with complex inheritance.
The risk to a subsequent sibling is higher if theaffected child
is female or has long-segmentdisease. In this case, which involved
a boy withshort-segment aganglionosis, the risk of Hirsch-sprungs
disease in a sibling is only 3 to 5%.Because of the low penetrance
associated witha single gene mutation in nonsyndromic
Hirsch-sprungs disease, the utility of genetic testingcurrently is
limited.
Dr. Harris: Is there an algorithm in the neonatalunits that
would lead one to raise the questionof Hirschsprungs disease early
in the course?
Dr. Goldstein: The possibility of Hirschsprungsdisease should at
least be considered in a full-term neonate who does not pass a
first meco-nium stool within 24 hours after birth.
Anatomical Di agnosis
Hirschsprungs disease with enterocolitis.
This case was discussed at Pediatric Grand Rounds.Disclosure
forms provided by the authors are available with
the full text of this article at NEJM.org.Dr. Badizadegan is
currently at Nemours Childrens Hospital,
Orlando, FL.We thank Ian Michelow, M.D. (Pediatric Infect ious
Diseases),
Phoebe Yager, M.D. (Pediatr ic Intensive Care), and Daniel
Ryan,M.D. (Pediatric Surgery), for assistance with preparing the
casehistory; and Lindsay P. Carter, M.D. (Pediatrics), for helping
toorganize the conference.
References
1. Bachur RG, Harper MB. Predictivemodel for serious bacterial
infectionsamong infants younger than 3 months ofage. Pediatrics
2001;108:311-6.2. Baker MD, Bell LM. Unpredictabilityof serious
bacterial illness in febrile in-fants from birth to 1 month of age.
Arch
Pediatr Adolesc Med 1999;153:508-11.3. Goldstein B, Giroir B,
Randolph A.International pediatric sepsis consensusconference:
definitions for sepsis and or-gan dysfunction in pediatrics.
Pediatr CritCare Med 2005;6:2-8.4. Rivers E, Nguyen B, Havstad S,
et al.Early goal-directed therapy in the treat-ment of severe
sepsis and septic shock.N Engl J Med 2001;345:1368-77.5. Ceneviva
G, Paschall JA, Maffei F,
Carcillo JA. Hemodynamic support influid-refractory pediatric
septic shock.Pediatrics 1998;102(2):e19.6. Ostlie DJ, Spilde TL, St
Peter SD, et al.Necrotizing enterocolitis in full-term in-fants. J
Pediatr Surg 2003;38:1039-42.7. Swenson O, Sherman JO, Fisher
JH.
Diagnosis of congenital megacolon: ananalysis of 501 patients. J
Pediatr Surg1973;8:587-94.8. Sherry SN, Kramer I. The time of
pas-sage of the first stool and first urine bythe newborn infant. J
Pediatr 1955;46:158-9.9. Clark DA. Times of first void and
firststool in 500 newborns. Pediatrics 1977;60:457-9.10. Polley TZ,
Coran AG. Hirschsprungs
disease in the newborn: an 11-year experi-ence. Pediatr Surg Int
1986;1:80-3.11. Elhalaby EA, Coran AG, Blane CE,Hirschl RB,
Teitelbaum DH. Enterocolitisassociated with Hirschsprungs disease:
aclinical-radiological characterization basedon 168 patients. J
Pediatr Surg 1995;30:
76-83.12. Menezes M, Puri P. Long-term out-come of patients with
enterocolitis com-plicating Hirschsprungs disease. PediatrSurg Int
2006;22:316-8.13. Suita S, Taguchi T, Ieiri S, Nakatsuji
T.Hirschsprungs disease in Japan: analysisof 3852 patients based on
a nationwidesurvey in 30 years. J Pediatr Surg 2005;40:197-201.14.
Pini Prato A, Gentilino V, Giunta C, et al.
The New England Journal of Medicine
Downloaded from nejm.org on October 23, 2012. For personal use
only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights
reserved.
-
7/27/2019 Nej m Cpc 1103562
12/12