Embed Size (px)
Citation preview

British JaurnalofPIastic Surguy (1989), 42,263-265 0 1989 The Trustees of British Association of Plastic Surgeons
0007-1226!89/0042-0263/$10.00
Modified gluteus maximus V-Y advancement flaps
A. J. HEYWOOD and A. A. QUABA
Department of Plastic Surgery, Bangour General Hospital, Broxburn, West Lothian
Summary-A modified method is presented for the closure of wounds using gluteus maximus V-Y advancement flaps. Extra tissue is included in each flap by extending the corners of its advancing edge. The extra tissue is utilised to aid closure by using a combination of rotation and transposition in addition to advancement. This modification is illustrated and examples of its clinical use described.
The V-Y advancement flap is an established reconstructive procedure whose use has recently been extended by better understanding of the blood supply to the skin (Ramirez et al., 1984, 1987; McGraw and Arnold, 1986).
The majority of surgical defects are roughly circular or oval, and widest across the centre. Using V-Y flaps, closure across the centre depends upon the amount of advancement which can be achieved, and wide defects may be a source of difficulty. Inclusion of extra tissue in the flaps, to whatever extent the blood supply permits, is of no value in obtaining closure across the centre if the flaps are simply advanced. For sacral defects we have used modified gluteus maximus V-Y advancement flaps, incorporating extra tissue in the flaps and introduc- ing other movements in addition to advancement. A similar technique has also been employed in the head and neck.
Method
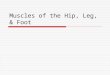
The flaps are designed to include extra tissue in the form of “horns” at the corners of the advancing edge, and undermined at the level of the gluteus maximus muscle surface so as to leave each attached only by its middle third, around which it may then be rotated (Fig. 1A).
Pure advancement of the flaps may lead to tension across the line of closure along the middle sections of the advancing edges (Fig. 1B). To avoid this tension and to utilise the extra tissue in the horns, the flaps are first rotated so that one horn of each flap meets the mid point of the advancing edge of the other. The two remaining horns, and the apices of the flaps, are then transposed to fill the remaining sections of the defect (Fig. 1C).
Closure results in a Z-shaped suture line across the middle of the defect (Fig. 1D).
Fig. 1
Figure l-(A) Flap design with attachment to pedicle retained in middle third. (B) Advancement alone fails to make optimum use of flap tissue. (C) Flaps advanced and rotated. Arrows indicate direction of transpositions. (D) Lines of final closure.
263

264 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 2
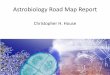
Figure 2-A sacral pressure ulcer in a patient with disseminated sclerosis. (A) Defect created by excision of the ulcer. (B) Flaps elevated, showing undermining of the flap on the right. (C) Flaps brought together under tension using pure advancement. (D) Flaps brought together easily by advancement with rotation (E) Flaps sutured in position without tension.

MODIFIED GLUTEUS MAXIMUS V-Y ADVANCEMENT FLAPS 245
Clinical applications
A clinical example of the technique is shown in Figure 2. It has been used successfully in seven similar cases, six of them pressure ulcers and one a large skin tumour. The same technique of flap design and movement has also been used in two instances in the head and neck, where the design was of a “random” pattern with respect to blood supply in contrast with the musculocutaneous perforators upon which the gluteus maximus flap is based. No part of any flap was lost.
Discussion
For V-Y flaps, the size of defect which can be closed by advancement alone depends on the amount of stretch in the skin and other tissues of the flap, and on the mobility of the tissues upon which the flap is based. The former can be increased by undermining of the flap and division of inelastic attachments such as fascia, the safe extent of which is dictated by the blood supply. Mobility of underlying tissues has been increased by various means. Barron and Emmett (1965) described V-Y skin flaps which are in reality island transposition flaps. Chan (1988) recently described a long unfolding subcutaneous pedicle applicable in the head and neck. Where a flap derives its blood supply from musculocutaneous perforating vessels, as in the gluteus maximus and hamstring musculo- cutaneous flaps, increased mobility has been achieved by detachment of the muscle origin or
in the sacral and head and neck regions, and may be applicable elsewhere.
Acknowledgement
The authors are grateful to the Department of Medical Illustration, Bangour General Hospital, for providing the illustrations.
References
Barron, J. N. and Emmett, A. J. J. (1965). Subcutaneous pedicle flaps. British Journal of Plastic Surgery, 18, 5 1.
Chan, S. T. S. (1988). A technique of undermining a V-Y subcutaneous island flap to maximise advancement British Journal of Plastic Surgery, 41.62.
Fisher, J., Arnold, P. G., Waldorf, G. and Woods, J. E. (1983). The gluteus maximus musculocutaneous V-Y advancement flap for large sacral defects. Annals ofPlastic Surgery, 11, 517.
Hurteau, J. E., Bostwick, J., Nahai, F., Hester, R. and Jurklewicz, M. J. (1981). Advancement of hamstring musculocutaneous flap for coverage of ischial pressure sores. Plastic and Reconstructive Surgery, 68,539.
McGraw, J. B. and Arnold, P. G. (1986). Atlas of Muscle and Musculocutaneous Flaps. Norfolk, Virginia: Hampton Press Publishing Co.
Ramirez, 0. M., Hurwitz, D. J. and Futrell, J. W. (1984). The expansive gluteus maximus flap. Plastic and Reconstructive Surgery, 74, 757.
Ramirez, 0. M., Swartz, W. M. and Futrell, J. W. (1987). The gluteus maximus muscle: experimental and clinical consider- ations relevant to reconstruction in ambulatory patients. British Journal of Plastic Surgery, 40, 1.
Scheflan, M. D., Nahai, F. and Bostwick, J. (1981). Gluteus maximus island musculocutaneous flap for closure of sacral and ischial ulcers. Plastic and Reconstructive Surgery, 68,533.
The Authors insertion (Hurteau et al., 1981; Scheflan et al., 1981; Fisher et al., 1983).
A. J. Heywood, FRCSEd, SHO in Plastic Surgery
The technique described here, while requiring A. A. Quaba, FRCSEd (Plast.), Consultant Plastic Surgeon
moderate undermining to allow advancement, does Department of Plastic Surgery, Bangour General Hospital,
not require muscle detachments or other modifica- Broxburn, West Lothian, EH52 6LR.
tions of the tissue pedicle. Rather, it involves only Requests for reprints to Mr Heywood at the above address.
extension of the cutaneous part of the flap and p adjustment of its final orientation. It has been used
aper received 2nd September 1988. Accepted 30 September 1988.