Embed Size (px)
Citation preview

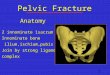
ITB Syndrome

Normal Anatomy
• Origin– Gluteus Maximus– Gluteus Medius– Tensor Fascia Latae– Ilium
• Insertion– Lateral Femoral Condyle– Tibial Infracondylar Tubercle

Normal Anatomy
• Continuation of TFL tendon
• Thickened aspect of lateral fascia
• Non-contractile structure

Pathology
• Friction of ITB against femoral epicondyle with repeated flexion and extension
• Compression of distal ITB against lateral femoral condyle
• Irritation of lateral structures– Fat– Connective tissue– ITB Bursa

Mechanism of Injury
• ITB Compression
• “Impingement Zone”– 30 degrees– Eccentric TFL – Eccentric Glute Max– Stance phase
• Repetitive movement– Long distance running– Cycling– Hill walking

Mechanism of Injury
• Posterior fibre irritation
• Irritation of Lateral Synovial recess
• Periosteum inflammation
• Insufficient recovery

Classification
• Compression– Lateral structures
• ITB itself• Lateral condyle
• Tissue Irritation– Synovial recess– Bursa– Cyst
• ?Inflammation presence in condition
• ?Anterior-Posterior movement or “snapping”
Lavine, 2010

Associated Pathologies
• PFPS
• Lateral ligament injury
• Bursitis

Subjective
• Lateral knee pains
• Increase throughout activity
• Some pain on bending activities
• Increases with repetition
• Can have swelling
• ?Tightness sensation

Objective - Knee
• Observation– Local swelling– Increased Q –angle– Valgus– Anterior pelvic tilt
• ROM– Full ROM– Pain at 30 degrees
flexion

Objective - Knee
• Squat/Single Leg Squat– Pain at 30 degrees– Weight shift– Valgus
• Palpation– Distal ITB tenderness– Lateral condyle tenderness– ITB tension

Objective - Hip
• Decreased abductor strength
• Contralateral Pelvic Drop
• Dynamic Knee Valgus
Fredericson et al, 2000

Objective - Foot
• Excessive calcaneal eversion
• Lack of supination
• Tibial Internal Rotation
Ferber et al, 2010

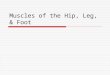
Special Tests
Ober’s & Modified Ober’s Test– Side lying– Fix pelvis– Take hip into extension– Release hip– Positive if does not pass
midline
Noble Compression Test– Patient supine– Flex knee to 90 degrees– Add compression– Extend knee– Symptoms approx 30
degrees

Further Investigation
• MRI

Management
• Reduce pain
• Reduce insertional compression
• Correct imbalances
• Improve kinetic chain function

Conservative - Management
McNichol et al, 1981
• 94% improvement conservative treatment
• NSAIDs– 0-7 days with treatment
• Cryotherapy– Pain relief Schwellnus et al, 1991

Conservative - Management
• Tissue Release
– Foam rolling• TFL• Adductors
– Soft tissue techniques• Massage• Not DTF• Not Stretching
Schwellnus et al, 1992
Chaudry et al, 2008

Conservative - Management
• Muscle Activation– Clam shells– Hip abductions
• Strengthening– Band Walks– Hip thrusts– Tibialis posterior
Cambridge et al, 2012

Conservative - Management
• Biomechanics– Movement patterns
• Single leg squat• FMS
– Gait assessment/re-education• Stride width• Cadence
– Footwear• Orthotics• Ramp angles

Conservative - Management
• Adjuncts– Acupuncture
– Electrotherapy
– Supports
– Taping

Conservative Management
1. Reduce pain, swelling2. Prepare tissues3. Restore Normal ROM4. Activate muscles5. Correct Movement Patterns

Surgical - Management
• Lateral Release– Transect posterior half– Bursa removal– Release of lateral retinaculum
• Injection– Corticosteroid• 30% improvement
Gunter & Schwellnus, 2004
Drogset et al, 1999

References• Cambridge ED, Sidorkewicz N, Ikeda DM, McGill SM. (2012). Progressive hip rehabilitation: the effects of
resistance band placement on gluteal activation during two common exercises. Clin Biomech. 27(7); 719-24
• Chaudry H, Schleip R, Zhiming J, Bukiet B, Maney M, Findley T. (2008). Three-Dimensional mathematical model for deformation of human fasciae in manual therapy. J Am Osteopath Assoc. 108; 379-390
• Drogset JO, Rossvoll I. Grontvedt T. (1999). Surgical treatment of iliotibial band friction syndrome. A retrospective study of 45 patients. Scand J Med Sci Sports. 9; 296-298
• Ellis R, Hing W, Reid D. (2007). Iliotibial band friction syndrome – A systematic review. Manual Therapy. 12; 200-208
• Ferber R, Noehren B, Hamill J, Davis I. (2010). Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. Journal of Orthopaedic & Sports Physical Therapy. 40(2); 52-60
• Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. (2000). Hip abductor weakness in distance runners with iliotibial band syndrome. Clinical Journal of Sports Medicine. 10(3); 169-175

References• Gunter P, Schwellnus M. (2004). Local corticosteroid injection in iliotibial band friction
syndrome in runners: a randomised controlled trial. British Journal of Sports Medicine. 38; 269–72
• Lavine R. (2010). Iliotibial band friction syndrome. Curr Rev Musculoskelet Med. 3; 18-22
• McNicol K, Taunton J, Clement D. (1981). Iliotibial tract friction syndrome in athletes. Canadian Journal of Applied Sport Science. 6(2);76–80
• Schwellnus M, Theunissen L, Noakes T, Reinach S. (1991). Anti-inflammatory and combined anti-inflammatory/analgesic medication in the early management of iliotibial band friction syndrome. South African Medical Journal. 79; 602–6
• Schwellnus M, Mackintosh L, Mee J. (1992). Deep transverse frictions in the treatment of iliotibial band friction syndrome in athletes: a clinical trial. Physiotherapy. 78(8); 564–8