Embed Size (px)
Citation preview

lable at ScienceDirect
Clinical Oncology 23 (2011) 587e600
Contents lists avai
Clinical Oncology
journal homepage: www.elsevier .com/locate/c lon
Overview
Metastatic Triple-negative Breast Cancer
E.A. Rakha *, S. Chan y*Department of Pathology, Nottingham University Hospitals NHS Trust, Nottingham, UKyDepartment of Clinical Oncology, Nottingham University Hospitals NHS Trust, Nottingham, UK
Received 19 November 2010; received in revised form 25 January 2011; accepted 27 January 2011
Abstract
The triple-negative class (oestrogen receptor-negative, progesterone receptor-negative andhumanepidermal growth factor receptor2 [HER2]-negative) comprisesabout 15%of breast cancer. It is associatedwith a poor prognosis comparedwith tumours that arepositive for hormone receptors orHER2. Despite being sensitive tochemotherapy,manywomenwithmetastatic triple-negative breast cancer (TNBC) relapse quickly, and commonly develop visceralmetastasis, including lung, liverand brainmetastasis. TNBC hasmolecular features that overlapwith breast cancer in BRCA1 germlinemutation carriers and with those of the basal-like molecularclass of tumours. Furthermore, tumours with the triple-negative phenotype have specific features and express markers that are potential therapeutic targets, forexample an impaired DNA repairmechanism and increased expression of proliferation and basal-associatedmarkers. The presence of these features has importantimplications for clinical practice and for the design of clinical trials looking at novel therapies. Targeted agents that are currently being investigated include poly(ADP-ribose) polymerase inhibitors, epidermal growth factor receptor inhibitors and anti-angiogenic compounds. Here we discuss the epidemiology, morpho-logical and molecular spectrum of TNBC, the clinical significance of this important class of breast cancer and the current treatment options.� 2011 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Key words: Breast cancer; metastasis; prognosis; targeted therapy; triple negative
Statement of Search Strategies Used andSources of Information
Literature including PubMed, Medline and the Cochranelibrary were searched for articles from 2000 to 2010 pub-lished in the English language. The key words used for thesearch were ‘breast cancer’, ‘basal’, ‘triple negative’,‘molecular profile’, ‘therapy’ and ‘outcome’. Publicationsbefore 2000 or published in another language were alsoconsidered if they were commonly referenced or highlyregarded older publications. The search also included thereference list for these articles and selected additionalarticles and web pages that were judged to be relevant.
Introduction
Breast cancer is a heterogeneous disease with variedmorphological appearance, molecular features, behaviour
Author for correspondence: E.A. Rakha, Department of Pathology,Nottingham University Hospitals NHS Trust, Nottingham City HospitalCampus, Hucknall Road, Nottingham NG5 1PB, UK. Tel: þ44-115-9691169;Fax: þ44-115-9627768.
E-mail address: [email protected] (E.A. Rakha).
0936-6555/$36.00 � 2011 The Royal College of Radiologists. Published by Elsevidoi:10.1016/j.clon.2011.03.013
and response to therapy. However, it has become clear thatpatients with apparently similar features may vary in theiroutcomes [1e3]. In an attempt to subdivide patients intoclearly defined categories that can be used to supportmanagement decisions, various well-established prognosticfactors have been combined to constitute prognostic indices[4]. Subgrouping based on molecular biomarkers such ashormone receptor (HR) has the advantage of avoiding thesubjectivity inherent in histopathology. Currently, expres-sion of HR, i.e. oestrogen receptors (ER) and progesteronereceptors (PR), and human epidermal growth factorreceptor 2 (HER2) play an important part in breast cancerclassification, at least partly because they predict theresponse to treatment [5e7]. ER-positive (ERþ) tumoursaccount for up to 65% of breast tumours in womenaged< 50 years, and 80% in older women [8]. PR-positive(PRþ) tumours account for about 60% of breast cancers [9].
Tumours that are HRþ and HER2-negative (HER2e)comprise the largest proportion of breast cancer and havea better prognosis and response to hormone therapy than theother HR/HER2 subgroups [10,11]. HRþ/HER2þ tumoursaccount for about 6% of breast cancers [12]. Preclinical andclinical data suggest that HER2 overexpression in HRþtumours confers resistance to hormonal treatment and
er Ltd. All rights reserved.

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600588
specific chemotherapeutic agents [10,13]. Tumours withouteither HR or HER2 expression are referred to as triple-negative breast cancer (TNBC). They have a poor prognosisin terms of disease-free and overall survival [1,6,14] andcurrently there is a lack of targeted therapies for this group ofpatients. There is an overlap between the molecular profilesand clinical/pathological features of TNBC and basal-like andBRCA1-associated cancers [15]. Furthermore, it has beenreported that sporadic TNBC shows BRCA1 protein dysfunc-tion despite the lack of BRCA1 germline mutation [16], whichmay provide therapeutic opportunities that have been triedsuccessfully in BRCA1-deficient tumours, for example, poly(ADP-ribose) polymerase (PARP) inhibitors [17,18].
Although there is a 60e90% overlap between TNBC andbasal-like breast cancer, and both terms are sometimes usedinterchangeably [18], it is important to recognise that thetriple-negative designation is based on clinical assays forER, PR and HER2, whereas basal-like is a molecularphenotype initially defined using gene expression profiling(cDNA microarrays) [3,19,20]. In most studies, the immu-nohistochemical (IHC) definition of basal-like tumoursrelies on the expression of one or more basal marker (e.g.CK5/6, CK14, epidermal growth factor receptor [EGFR]) withor without the HRe/HER2ephenotype [3].
Here we focus on the epidemiology, features, prognosis,metastatic patterns and current and future therapeuticstrategies for patients diagnosed with TNBC. Throughout,we use the term ‘triple-negative’when studies used clinicalassays for definition and ‘basal-like’ when expressionmicroarrays or IHC methodology using basal-associatedmarkers were used.
Epidemiology of Triple-negative BreastCancer
TNBC accounts for 10e20% of all breast cancer[6,14,21,22], depending on the thresholds for ERþ and PRþand the HER2 assessment method, as well as the age groups,racial groups and tumour grade/type/stage in differentstudy cohorts. The reported prevalence of TNBC may bechanged slightly in the future in light of amendments to thedefinition of HER2 and HR positivity in guidelines from theAmerican Society of Clinical Oncology and the College ofAmerican Pathologists [23,24].
TNBC is more prevalent in non-white African womenthan in the overall population [21,25]. It is also more prev-alent than other types of breast cancer in premenopausalwomen under the age of 50 years [5,21]. However, in linewith the prevalence of breast cancer overall, most TNBC isdetected in postmenopausal women aged 50þ years [2,26].
Diagnostic Features of Triple-negativeBreast Cancer
Imaging Features
Compared with other molecular classes of breast cancer,there is a low detection rate of TNBC bymammography [14].
Indeed, in breast screening, basal-like cancer often presentsas an interval cancer (i.e. between routine mammograms)[27]. The most frequent mammographic features diagnosticof TNBC, compared with other breast cancer subtypes, arecircumscribed mass (without spiculated margins), uni-focality and absence of microcalcifications [28].
On ultrasound, basal-like breast cancer is less likely tohave an echogenic halo, comparedwith other breast cancers[29]. Using magnetic resonance imaging, most TNBC is ofmass-type, with typical malignant signal enhancementkinetics [30], rim enhancement, persistent enhancementpattern and very high intratumoral signal intensity [31]. Ina study using F-18 fluorodeoxyglucose (FDG)-positronemission tomography imaging, all patients with TNBC(n¼ 18) had areas with focally enhanced uptake of FDG; theinvestigators suggested that FDG-positron emissiontomography can detect TNBC with 100% sensitivity [32].
Clinicopathological Features
TNBC has several characteristic aggressive clinicopatho-logical features, including young age at onset and largetumour size [5,30]. Its histological hallmarks include highgrade, high proliferative activity, focal areas of necrosis,absence of infiltrative margin, absence of gland formation,presence of central scar/fibrotic foci and prominent lym-phoplasmacytic inflammatory infiltrate [5,21,26,33].However, most of the histological features of TNBC are notspecific, and are observed in other high-grade HRetumours. Although TNBC constitutes 25e30% of grade 3tumours, 77e90% of TNBC is grade 3 [6,22,26,34]. MostTNBC (80e93%) is poorly differentiated ductal carcinoma ofno special type [6,25,26]. Invasive lobular carcinoma (thesecond most common type of breast cancer) comprises1e2% of TNBC [26]. Almost all cases of typical medullarycarcinomas show the triple-negative phenotype, and theyconstitute z2% of TNBC [26]. Most atypical medullarybreast cancer and cancers arising in women who carry theBRCA1 mutation show the triple-negative phenotype.
TNBC often lacks association with vascular invasion, oran overt in situ component [3,28,35]. However, whena triple-negative tumour is associated with ductal carci-noma in situ (DCIS), it is usually of high nuclear grade [26].The low frequency of association between TNBC and DCISmay be explained by the rapid progression of TNBC toinvasive cancer and/or obliteration of the DCIS precursor bythe rapidly growing invasive component [36].
The reported association between TNBC and lymph nodestage varies between different studies; some investigatorshave reported no association [3,37], whereas others haveassociated TNBC with node negativity [38e40] or positivity[14]. Most studies have reported an association betweenTNBC and large primary tumours [30], and this wouldsuggest that TNBC may have rapid growth rates [36,41].
Most TNBC express proteins characteristic of basal breastepithelial cells or those associated with proliferation andpoor prognosis. It has been reported that 50e80% of TNBCexpress basal cytokeratins (CK5/6, CK14 and CK17), EGFR,P-cadherin andvimentin [3,42]. Othermarkers include c-Kit,

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600 589
nestin, osteonectin, caveolins 1 and 2, aB crystallin andlaminin [3]. p53 IHC expression or TP53 gene mutation areseen in a high proportion of TNBC [43e45], as are alterationsof the pRB and p16 G1/S cell cycle checkpoint [46,47].Aminority of TNBCharbours EGFR gene amplification [48] oraneusomy [49].
Molecular Features
Collectively, the gene expression profile of basal-liketumours provides a myriad of candidate genes that maycontribute to their aggressive phenotype. Although basal-like cancer and TNBC are not synonymous, there arenumerousmolecular similarities and overlap between them[50]. Furthermore, most TNBC have the basal-like pheno-type [50]; similarly, most tumours expressing ‘basal’markers are TNBC [7,51]. However, a proportion of basal-likecancers lack a triple-negative phenotype and vice versa,23 and 28%, respectively, according to Bertucci et al. [51].
TNBC and basal-like cancers are believed to havea greater degree of genetic instability, compared with otherbreast cancer subtypes; they show the highest frequency ofDNA losses and gains, but less frequently have high-levelgains/amplifications [52,53]. Wang et al. [54] found loss ofheterozygosity (a marker for genomic instability) ata higher level in basal-like breast cancer than in othermolecular subtypes. Furthermore, chromosome region5q11, close to a number of DNA repair and checkpoint genes,was lost in 100% of basal-like cancers and never in othersubtypes [54]. This pattern of genomic change may suggesta defect in DNA double-strand break repair mechanisms.
One of the functions of the BRCA1 gene is DNA damagerepair, and in its absence, the cell becomes dependent onerror-prone methods of DNA double-strand break repair[5,55]. Accordingly, loss of a functional BRCA1 genepromotes chromosomal instability and often results incarcinogenesis [5]. Women with germline mutations ofBRCA1 are highly susceptible to breast cancer [56], andabout 70e90% display the triple-negative/basal-likephenotype [57]. Possible deficits in DNA repair have impli-cations for the response to therapy d not only to currentagents, but also to novel targeted therapies that use thisdeficiency in tumour cells for therapeutic gain.
Role as Prognostic Marker
There are disproportionate numbers of disease recur-rences and breast cancer deaths in TNBC, compared withother breast cancer subtypes, particularly in the first 3e5years after diagnosis [1,6,14]. TNBC also has a specificpattern of timing and site of recurrences [14,25]. Distantrecurrence in TNBC is rarely preceded by local recurrence[14]. There is a rapid progression from distant recurrence todeath. Interestingly, the risk of recurrence beyond 5 yearsafter diagnosis is 50% less when compared with similarearly HRþ breast cancer [58].
Despite having a poor prognosis overall, TNBC is hetero-geneous with respect to individual patient outcomes [6,38].
Some rare tumour types have a triple-negative phenotype,but anexcellentprognosis (e.g. adenoid cystic carcinomaandsecretory carcinomas [59,60]). There are also some types ofTNBC that do not express basal markers, and are classified aseither normal breast-like or null phenotype [2,5].
Metastatic Triple-negative Breast Cancer
Metastatic breast cancer (MBC) is not curable, and theprimary goal of therapy is restoration of quality of life [61].Decisions about systemic treatment of women with MBCare often based on ER, PR and HER2 status, as well asspecific patient and other tumour factors, such as sites ofmetastasis and symptoms. The age at initial diagnosis, HRstatus and site of metastasis are the most relevant factorsfor predicting survival from the time of metastasis [62].
TNBC has a propensity for visceralmetastasis to brain andlung, rather than lymph nodes, bone or liver [25,63]. Thismay be due to the propensity of TNBC for haematogenousrather than lymphatic spreaddwehaveobserved that TNBCis associated with an increased microvascular density, butnotwith lymphovascular densitywhen comparedwith non-TNBC (Rakha E, unpublished data).
Current Therapeutic Options
Chemotherapy
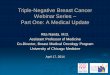
To date, chemotherapy remains the only systemic ther-apeutic option for TNBC in either the adjuvant or metastaticsetting [5,21] and various chemotherapy trials are ongoing(Table 1). The prognosis after standard chemotherapyremains poor, even for small, lymph node-negative TNBC[64,65]. The efficacy of anthracycline-based regimens inTNBC remains controversial. A meta-analysis of four studiesshowed that patients with TNBC experienced a 23%reduction in the risk of disease relapse when treated withan anthracycline-containing regimen as opposed tocyclophosphamideþmethotrexateþ 5-fluorouracil [66].However, in a retrospective analysis of the MA5 trial ofcyclophosphamideþ epirubicinþ 5-fluorouracil versuscyclophosphamideþmethotrexateþ 5-fluorouracil adju-vant chemotherapy, the test for interaction between basal-like class and treatment arm reached only borderlinesignificance [67], suggesting that these patients may notderive a particular benefit from anthracyclines.
Rodriguez-Pinilla et al. [68] showed that TNBC witha defective DNA repair gene expression pattern was signif-icantly associated with anthracycline response and taxaneresistance, and concluded that defective DNA repair geneexpression signature may be useful to identify TNBC that issensitive to anthracyclines and resistant to taxane-basedchemotherapy. Moreover, preclinical and clinical studiesindicate that tumours with BRCA1 dysfunction are sensitiveto agents that cause DNA damage, such as platinum agents(cisplatin and carboplatin) [69]. In a recent study of neo-adjuvant single-agent cisplatin versus non-platinum

Table 1Clinical trials in triple-negative breast cancer
Trial name Study phaseand design
Totalenrolment
Condition Definitionof triple-negativebreastcancer
Primary aim No. arms Th py Outcomemeasures
Start andexpectedcompletiondates
Chemotherapy aloneCarboplatinor docetaxelchemotherapyfor advancedgenetic breastcancer(BRCA trial).
IIRandomised
148 MetastaticBRCA carrierbreast cancer
BRCAmutationcarrierbreastcancer
To determine ifcarboplatin isbetter thandocetaxel forgenetic breastcancer that hascome back afterchemotherapy
2(2 : 1assignment,uncontrolled)
Ca platinor cetaxel
Tolerability,responserate, time toprogression
September2005September2009
Triple-negativebreast cancer trial
IIIRandomised
370e450 Metastatic orrecurrentlocallyadvancedbreast cancer
Triplenegative
To determinewhether there isgreater activityfor carboplatinthan a taxane standardof care (docetaxel)in women with triple-negative breast cancer
2(parallelassignment,uncontrolled)
Ca platin(ar A) anddo axel(ar B)
Overall survival,progression-freesurvival, timeto progression,toxicity, time totreatment failure
January2008January2014
Neoadjuvantplatinum-basedchemoradiationtherapy forlocally advancedtriple-negativebreast cancer
IINon-randomised
53 Primary locallyadvanced/non-metastatictriple-negativebreast cancer
Triplenegative
To determine theresponse toplatinum-basedchemotherapy(cisplatin or carboplatin)given withradiation therapybefore surgery
1 Pla um-basedch otherapy,rad tion,su ry
Clinical responserate, pathologicalcompleteresponse,time to diseaseprogression,overall survival
October2010November2015
Targeted therapy with or without chemotherapyA phase II studyof standardchemotherapy plusBSI-201(a PARPinhibitor) inthe neoadjuvanttreatment oftriple-negativebreast cancer
II 36 Stage IeIIIAdisease
Triplenegative
To investigate whetherthe neoadjuvantcombination ofgemcitabine,carboplatin, andBSI-201 will causea high percentage of triple-negative breast cancerpatients to achievea pathological completeresponse before surgery
1 (single groupassignmentcomparedwith historicalcontrol)
Sta ardch otherapy(ge citabineplucar platin)plu BSI-201,iv, weekcy s
Pathologicalcompleteresponse
December2008May 2012
E.A.Rakha,S.Chan
/ClinicalO
ncology23
(2011)587
e600
590
erarbodo
rbomcetm
tinemiarge
ndemmsbos3cle

Study to assessthe efficacy andsafety of a PARPinhibitor for thetreatment ofBRCA-positiveadvanced breastcancer (ICEBERG 1)
IINon-randomised
54 Advancedbreast cancerwith no brainmetastasis
PositiveBRCA1or BRCA2status
To assess the efficacyand safety of KU0059436 in patientswith advanced BRCA1or BRCA2-associatedbreast cancer
1 (non-comparative)
KU 0059436given orallytwice daily
Tumourresponse rate,clinical benefitrate, drugsafety/tolerability
June 2007February2009
Study to assess thesafety andtolerabilityof a PARP inhibitorin combinationwith carboplatin
INon-randomised
160(includingovariancancerpatients)
Breast cancer inpatients who havenot received morethan two previousplatinumebasedchemotherapycourses
Triplenegative
To identify a safe andtolerable dose ofKU-0059436 thatcan be given incombination withcarboplatin and/orpaclitaxelchemotherapy
3(1:carboplatinþKU-0059436; 2:paclitaxelþKU-0059436; 3:paclitaxel,carboplatinþKU-0059436)
Oral KU-0059436in combinationwith paclitaxel/carboplatinaccording todifferent arms
Drug toxicity/tolerability
June 2007March 2013
A study of dasatinib(BMS-354825) inpatients withadvanced’tripleenegative’breast cancer
IINon-randomised
44 Recurrent,locally advancedor metastaticbreast cancer
Triplenegative
To estimate theobjective responserate of dasatinib andobtain preliminarypharmacogenomicsdata
1 (single groupassignment,uncontrolled)
Dasatinib(oral, twicedaily)
Overallresponse rate,disease controlrate,progression-free survival,responseduration
December2006December2008
Cetuximab andcisplatin in thetreatment oftriple-negativemetastatic breastcancer (BALI-1)
IIRandomised
180 Metastaticbreast cancer
Triplenegative
To assessthe overallresponse
2 (parallelassignment,active control)
Anti-EGFR(cetuximab)combined withcisplatin andcisplatin alone
Progression-freesurvival, overallsurvival, time toresponse
June 2007June 2010
Cetuximab andcarbo for ER/PR/HER2enegativebreast cancer
IIRandomised
100 Metastaticbreast cancer
Triplenegative
To assessthe overallresponse rateto cetuximabalone and incombinationwith cetuximab pluscarboplatin
2 (parallelassignment,uncontrolled)
Anti-EGFRcetuximabalone(group A)and incombinationwithcarboplatin(group B)
Overallresponse rate,progression-freesurvival, overallsurvival, effectsof EGFRinhibition
December2006December2015
Cediranib andolaparib incombination forrecurrent ovarianor triple-negativebreast cancer
I and IINon-randomised
90 ovarianand breastcancers
Recurrenttriple-negativebreast cancer
Triplenegative
To assessthe safety ofthe combinationof cediranib andolaparib and thehighest safedoses of thesetwo drugs
1(single groupassignment,uncontrolled)
Cediranib andolaparib orallyin combinationand comparedto each drugwhen usedalone
Drug toxicity/tolerability andprogression-freesurvival andoverall survival
November2009October2014
(continued on next page)
E.A.Rakha,S.Chan
/ClinicalO
ncology23
(2011)587
e600
591
Table 1 (continued)
Trial name Study phaseand design
Totalenrolment
Condition Definitionof triple-negativebreastcancer
Primary aim No. arms Therapy Outcomemeasures
Start andexpectedcompletiondates
Combined treatmentof cetuximab andpaclitaxel inbasalelikebreast cancer
I and IINon-Randomised
25 Metastaticbreast cancer
Triplenegative
To assess theefficacy ofcombinedanti-EGFRcetuximaband weeklytaxol
1(single groupassignment,uncontrolled)
Anti-EGFR(Erbitux;cetuximab)with weeklytaxolchemotherapy
Tolerability,response rate,tumour markerstumour sizechemotherapy
November2006September2009
Cediranib maleateand olaparib intreating patientswith recurrentovarian epithelialcancer, fallopiantube cancer,peritoneal cancer,or recurrenttriple-negativebreast cancer
I and IIRandomised
114ovarianand breastcancers
Recurrenttriple-negativebreast cancer(phase I only)
Triplenegative
To assess thesafety andefficacyof thecombinationof cediranibmaleate andolaparib
2(parallelassignment,uncontrolled)
Arm I: patientsreceive oralcediranibmaleate oncedaily on days1e28.Arm II: patientsreceive oralcediranibmaleateonce daily andoral olaparibtwice dailyon days 1e28.
Drug toxicity/tolerability andprogression-freesurvival andoverall survival
March 2010May 2010
EndoTAG-1 intriplereceptorenegativebreast cancerpatients
IIRandomised
143 Metastatic orrelapsed breastcancer
Triplenegative
To assess theefficacy, safetyand tolerabilityof EndoTAG-1alone and incombination
3 EndoTAG-1and paclitaxel(combinationtherapy) andEndoTAG-1(monotherapy)in comparisonwith paclitaxel(control group)
4-monthprogression-freesurvival,survival rate,tumourresponse
January2007December2010
Abraxane,bevacizumaband carboplatinin triple-negativemetastaticbreast cancer(NCI CTCAE)
IINon-randomised
70 Metastaticbreast cancer
Triplenegative
To assessthe effect ofcombination ofweekly abraxaneand carboplatinplus bi-weeklybevacizumab
1(single groupassignment,and historicalcontrol)
Abraxane,bevacizumaband carboplatin
Progression-free survival,safety andtolerabilityof combinationtherapy
May 2007May 2009
E.A.Rakha,S.Chan
/ClinicalO
ncology23
(2011)587
e600
592

Preoperativecisplatin andbevacizumabin ERe, PRe,Her-2ebreastcancer
IINon-randomised
40 Primarynon-metastaticbreast cancer
Triplenegative
To assessthe effect ofcisplatin incombinationwith bevacizumabbefore surgery,and then standardchemotherapyplus bevacizumabafter surgery intriple-negativebreast cancer
1 Preoperativetherapy withcisplatin (iv,on day 1 of thecycle (onceevery3 weeks) for4 cycles) andbevacizumab(iv, on day 1 ofthe cycle (onceevery 3 weeks)for 3 cycles)
Pathologicalcompleteresponse,clinicalresponserate
September2007September2010
Oestrogen fortripleenegativebreast cancer(NCT01083641)
IINon-randomised
39 Metastaticbreastcancer
Triplenegative
(To determinethe effectivenessof oestradioltreatmentfor metastatictriple-negativebreast cancer)
1 High-doseestradiol(10 mgoral threetimes daily)
Tumourobjectiveresponserate
January2010January2012
Bevacizumaband abraxaneas second-linetherapy intriple-negativemetastaticbreast cancer
IINon-randomised
37 Metastaticbreastcancer
Triplenegative
To determinethe effect ofaddingbevacizumabto abraxaneas second-linetherapy
2(single groupassignmentand activecontrol)
Bevacizumaband abraxane
Progression-freesurvival, overallresponse rate,toxicity
May 2007December2011
Study ofSU011248versuschemotherapyfor patientswith previouslytreated triplereceptorenegativebreast cancer
IIRandomised
200 Previouslytreatedmetastatic orlocallyrecurrenttriple-negativebreast cancer
Triplenegative
To compareprogression-freesurvival forSU011248versus standardof care therapyin patients withpreviouslytreated,advancedtriple-negativebreast cancer
2 A:Experimentalarm:intervention:drug:SU011248(sunitinib)orallyB: Activecomparatorarm:intervention:drug:chemotherapy(The choice ofchemotherapywas at thediscretion ofthe investigatorwithin thelimits specified)
Progression-free survival,objectiveresponserate andoverallsurvival
January2006May 2010
(continued on next page)
E.A.Rakha,S.Chan
/ClinicalO
ncology23
(2011)587
e600
593

Table 1 (continued)
Trial name Study phaseand design
Totalenrolment
Condition Definitionof triple-negativebreastcancer
Primary aim No. arms Therapy Outcomemeasures
Start andexpectedcompletiondates
Neoadjuvantsunitinib withpaclitaxel/carboplatin inpatients withtriple-negativebreast cancer
I and IINon-randomised
53 Locallyadvancedtriple-negativebreast cancer
Triplenegative
To evaluate thecombination ofsunitinib pluspaclitaxel andcarboplatin asneoadjuvanttreatmentfor locallyadvancedtriple-negativebreast cancer
1 Systemictherapyinterventions:Drugs:chemotherapypaclitaxel/carboplatin(intravenous)Drug: sunitinib(oral)
To determinethe maximumtolerated dose,pathologicalcomplete responsesafety and efficacyof the combinationof sunitinib/paclitaxel/carboplatinwhen usedas neoadjuvanttreatment fortriple-negativebreast cancer
January2009June 2010
Erlotinib pluschemotherapyfor treatmentof triple-negativebreast cancer
IINon-randomised
30 Stage II andIII triple-negativebreast cancer withno prior therapy
Triplenegative
To assess thepathologicalcompleteresponse withfour to six cyclesof neoadjuvantchemotherapyand pulse erlotinib
1(single groupassignmentand activecontrol)
Neoadjuvantcarboplatin/docetaxel �plus erlotiniband then,12 monthsof maintenanceerlotinib
Pathologicalcompleteresponse,regimensafety/toxicity
July 2007June 2011
Paclitaxel followedby FEC versuspaclitaxel andRAD001 followedby FEC In womenWith breast cancer
IIRandomised
50 Stage IIA(T1N1) to IIICnoneinflammatorybreast cancer
Triplenegative
To assess thedifferencebetweenstandardneoadjuvantchemotherapyversus thecombinationwith RAD001
2(1: paclitaxelþFEC; 2:paclitaxelþRAD001þ FEC)
Neoadjuvantpaclitaxelfollowed byFEC versus thecombination ofpaclitaxel,and RAD001(oral 30 mgweekly on days1, 8, and 15 for12 cycles)followed by FEC
Molecularchanges(inhibition/activation)of the PI3K/PTEN/AKTpathway,pathologicalcomplete response,overallresponserates, drug toxicity
July 2007July 2011
HER2, human epidermal growth factor receptor 2; PARP, poly (ADP-ribose) polymerase; EGFR, epidermal growth factor receptor; ER, oestrogen receptor; PR, progesterone receptorData obtained from Clinical Trials website (http://clinicaltrials.gov/ and http://www.cancerresearchuk.org/).
E.A.Rakha,S.Chan
/ClinicalO
ncology23
(2011)587
e600
594

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600 595
regimens in patients with BRCA1-associated breast cancer,the pathological complete response rate was high in thecisplatin-treated cohort (83%; 10/12 patients) and far lower inthe other aggregated regimens (16%; 14/90 patients) [70].However, this study may be limited by its small size, retro-spective nature and the difference between the two studycohorts [70]. The response rate of TNBC to platinum-basedregimens versus other cytotoxics remains to be validated.Clinical trials aiming to address the response of TNBC toplatinum agents are underway, including investigations atphase II (Platinum for Triple-Negative Metastatic BreastCancer and Evaluation of p63/p73 as a Biomarker of Responsetrial [NCT00483223] a non-randomised, single-arm trial todetermine the objective response rate in patients withmetastatic TNBC receiving platinum as first- or second-linetherapy) and phase III (Triple Negative Breast Cancer Trial[NCT00532727] a randomised, double-arm study comparingcarboplatinwith docetaxel-based standard of care inwomenwith metastatic or recurrent locally advanced TNBC).
In vitro evidence from human cell line and murinetumour models suggests that BRCA1 mutations may conferresistance to taxanes [71]. TNBC express high levels of bIII-tubulin, whose expression is correlated with resistance totaxanes. However, to date, there is no convincing clinicalevidence that TNBC is less sensitive than non-TNBC to tax-ane treatment.
Fourquet et al. [72] reporteda complete clinical response in46% (15/39) of patients with mutated BRCA1/2 treated withinduction anthracycline-containing chemotherapy and/orradiotherapy compared with 17% (7/54) of those with non-mutated tumours. A complete or major clinical responsewas observed in 74% of tumours treated with inductionchemotherapy. The overall complete or major clinicalresponse rate in tumours treatedwith induction radiotherapywas 68% (13/19). The group also found that, after inductiontreatment by either chemotherapy or radiotherapy, morebreast-conserving treatments could be carried out in muta-tion carriers than in non-carriers and they concluded thatBRCA1mutationwas the solepredictorof breast conservation.This suggests that impaired repair mechanisms related to theBRCA1/2 mutations increased the chemosensitivity andradiosensitivity of large breast cancers.
Radiotherapy
A study of 1000 patients with high-risk breast cancer,including 152 with TNBC, randomised to receive post-mastectomy radiotherapy, has suggested possible radio-resistance of the triple-negative subtype [73]. Theinvestigators concluded that this radioresistance may bea result of HRe status, a finding that will need further vali-dation ina larger series. There isalsoapossibility that thepooroutcome in TNBC patients is related to the absence of endo-crine therapy,which is known to reduce local recurrence [74].
Local Treatment
TNBC is not associated with an increased risk of locore-gional relapse after conservative surgery, compared with
other breast cancer subtypes [1]. This observation, inaddition to the well-defined border of invasion in TNBC andthe absence of association with vascular invasion orextensive in situ components [3,21,28,35] suggests thatTNBC does not warrant a more radical approach to local oraxillary surgery than other breast cancers. The potentiallyaggressive behaviour of these tumours may be betteraddressed by systemic therapy.
Future Directions for Triple-negativeBreast Cancer Treatment: Targeted Therapy
A number of targeted therapies are currently beinginvestigated in women with TNBC in the neoadjuvant andmetastatic settings (Table 1). We will discuss in some detailthe most important potential targets.
Epidermal Growth Factor Receptor
EGFR (HER1) has an important role in cell proliferation,migration and protection against apoptosis, and is associ-ated with a poor prognosis [75], including in patientstreated with anthracycline chemotherapy [76]. EGFR isexpressed at high levels in at least 20% of breast cancersoverall [75,77], but in 60e70% of patients with TNBC[78,79]. Furthermore, it is overexpressed in up to 80% ofmetaplastic carcinomas (a variant of triple-negative/basal-like breast cancer) and, of these, 34% harbour EGFR geneamplification [48]. These findings suggest that EGFRmay bea rational target for treatment of TNBC, e.g. using mono-clonal antibodies (cetuximab, panitumumab) and/orsynthetic tyrosine kinase inhibitors [80]. In an overview ofstudies of the tyrosine kinase inhibitors, erlotinib andgefitinib, as targeted treatments for breast cancer, Agrawalet al. [76] pointed out that efficacy depends on the presenceof EGFR protein in the tumour tissue. Thus, EGFR assess-ment could be used to identify patients who would prob-ably have a good response to EGFR-targeted therapy.
Because TNBC is characterised by EGFR overexpressionand DNA repair defects, and there is cytotoxic interactionbetween EGFR inhibitors and DNA cross-linking agents (e.g.platinum derivatives) [81], there may be the possibility ofan effective combination treatment for TNBC. A preclinicalstudy has shown that concurrent treatment with subop-timal doses of cetuximab significantly enhances apoptoticcell death induced by the DNA cross-linking agent cisplatin[81]. In a phase II study of irinotecan and carboplatinwith orwithout cetuximab in 78 patients with TNBC, cetuximabwas associated with a response rate of 49% compared with30% when chemotherapy was used alone [82]; however,there were no significant differences in progression-freesurvival or overall survival, and toxicity led to chemo-therapy dose reductions [82]. Based on the availableevidence, there is little reason to believe that either single-agent cetuximab or a small-molecule tyrosine kinaseinhibitor will have substantial activity in TNBC. It remainsunknown whether these agents will prove useful whencombined with chemotherapy.

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600596
Vascular Endothelial Growth Factor
Vascular endothelial growth factor (VEGF) is a potentangiogenic factor associated with a poor prognosis in breastcancer in general [83], and with shorter survival in patientswith TNBC compared with those with non-TNBC [84].Hence, blocking the action of VEGF seems to be a promisingapproach to breast cancer treatment.
Bevacizumab (Avastin), a monoclonal antibody targetingVEGF, is active in a variety of solid tumours, including breastcancer. Improvement in progression-free survival wasreported when bevacizumab was added to paclitaxelchemotherapy compared with single-agent paclitaxel alonein first-line treatment of MBC, including a subset with TNBC[85]. Although some oncologists will consider a bev-acizumab combination for first-line therapy of metastaticTNBC, the results of two placebo-controlled phase IIIrandomised trials of bevacizumab plus chemotherapy in thefrontline MBC setting (AVADO trial [62] and RIBBON 1 trial[86]) have shown an improvement in progression-freesurvival of a much smaller magnitude than seen in theE2100 study [85] even though the improvement wasstatistically significant. A significant improvement in overallsurvival was not achieved in any of these three trials. In theneoadjuvant setting, it has been reported that the additionof bevacizumab to cisplatin produces only modest resultsbut considerable toxicity [87].
In a phase II, open-label, multicentre study, sunitinibmalate, an oral multi-targeted tyrosine kinase inhibitor thatinhibits VEGF receptor, c-kit, platelet-derived growth factorreceptor and colony-stimulating factor-1 receptor, has shownmoderate activity (objective response rate 11%) as mono-therapy in 64 patients with MBC resistant to anthracyclinesand taxanes [88]. The objective response ratewas particularlyhigh among patients with triple-negative tumours (3/20;15%) or trastuzumab-treated, HER2þ tumours (3/12; 25%),compared with other phenotypic groups (1/32; 3%).
c-Myc and TOP2A Oncogenes
c-Mycencodes a proliferative DNA-binding protein thatplays an important role in induction and progression oftumours, including breast cancer. There are reports of anassociation between c-Myc amplification and tumouraggressiveness, but there is wide variability in thefrequency of the amplification and its association withtriple-negative/basal-like breast cancer [89]. c-Myc ampli-fication is reported in 53% of BRCA1-deficient breast cancer,compared with about 20% of sporadic breast cancer [90],a finding that supports a link between c-Myc and BRCA1 andimplies that c-Mycmay be an important target in basal-like/triple-negative disease. However, Rodriguez-Pinilla et al.[91] reported that c-Myc was amplified in only 4% of basal-like carcinomas and concluded that c-Myc amplification isnot associated with the basal-like phenotype.
TOP2A encodes topoisomerase IIa, and its amplification isassociated with a good response to anthracyclines, whereasdeletion may be accompanied by resistance [92]. Although
there have been many publications with regards to TOP2Aand the response to anthracyclines in breast cancer [93], thedata so far are inconclusive and TOP2A amplification isinfrequent in TNBC [94], which may limit its clinical utility.
Poly (ADP-ribose) Polymerase Inhibitors
When there is BRCA1 deficiency, other DNA repairpathways may increase in importance. Several DNA repairpathways, including base-excision repair, are dependent inpart on PARPs [21,95] d enzymes that catalyse the poly-merisation of poly (ADP-ribose) chains in target proteins[95]. Nuclear PARPs, particularly PARP1, have key roles inDNA repair and programmed cell death. PARP1 alsocontributes to the modification of histones, which leads tolocal chromatin remodelling, allowing access of DNA repairproteins to the repair site. When PARP1 is inhibited, there isaccumulation of DNA double-strand breaks that wouldnormally be repaired via homologous recombination(BRCA1-mediated) [29]. Preclinical studies have shown thatinhibition of PARP leads to selective and significant killing ofBRCA-mutated cancer cells, a phenomenon described assynthetic lethality, which is not observed in cells with intactBRCA function [17,96,97]. Consistent with these observa-tions, phase I clinical trial results of PARP inhibitors havebeen encouraging, with sustained responses in patientswith BRCA1/2-deficient breast or ovarian metastatic cancers[17,98].
High PARP1 expression is observed in BRCA1-associatedand triple-negative/basal-like breast tumours [99].However, not all TNBC is associated with BRCA1 dysfunc-tion, and it has been reported that sensitivity to PARPinhibitors is higher in cancer cells that lack the tumoursuppressor, phosphatase and tensin homolog (PTEN), thanin those with normal PTEN [100]. Both of these findingshave implications for the selection of patients with TNBC fortreatment with PARP inhibition and, therefore, these resultsrequire confirmation in other studies.
PARP1 activity increases significantly after DNA damagecaused by chemotherapy or radiotherapy [101]. Inhibition ofPARP1 has, therefore, been undergoing preclinical andclinical development as a strategy to enhance chemo-therapy- and radiotherapy-mediated cytotoxicity in humancancers. Several PARP1 inhibitors are currently in clinicaldevelopment; of these, iniparib and olaparib are at the mostadvanced developmental stage.
Recently published randomised phase II data haveshown that iniparib, delivered intravenously at a dose of5.6 mg/kg on days 1, 4, 8 and 11 (every 21 days) in additionto gemcitabineþ carboplatin in patients (n¼ 123) withmetastatic TNBC who had received no more than twoprevious lines of chemotherapy, improved the clinicalbenefit rate to 56%, compared with 34% for chemotherapyalone [99]. The overall response rate was improved from32% in the chemotherapy-only arm to 52%with the additionof iniparib, progression-free survival was improved from 3.6to 5.9 months, respectively, and overall survival wasimproved from 7.7 to 12.3 months, respectively [102]. Therisk of death was reduced by a highly significant 43% among

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600 597
patients given iniparib, compared with chemotherapyalone, with little added toxicity [102].
Another recently presented phase II trial looked at anorally active PARP inhibitor, olaparib (given at a dose of400 mg twice daily), in patients with confirmed BRCA1/2mutations and recurrent advanced breast cancer who hadfailed at least one previous chemotherapy [103]. Olaparibproduced an objective response rate of 41%, a clinicalbenefit rate of 52% and a median progression-free survivalof about 6 months. Severe toxicities were rare, with onlyone treatment discontinuation due to treatment-relatedadverse events. However, although this trial providespositive proof of concept for PARP inhibition in BRCA-defi-cient breast cancer, the magnitude of response was in factlower than that expected from other successful targetedtherapy. It is possible that the homologous recombinationpathway was still functioning in the study population, dueto secondary reversion mutation in BRCA [104]. Veliparib(ABT-888) is another oral PARP1 inhibitor, and is beingevaluated as monotherapy or in combination regimens inthe treatment of breast cancer.
The use and clinical value of the different PARP1 inhibi-tors in TNBC remain to be validated and several questionsremain to be answered, such as which subgroup of TNBC aremost likely to benefit from this therapy, what biomarkerscan predict the response to it and what are the best cyto-toxic agents to be used with PARP1 inhibitors. Clinical trialsare being designed and conducted and they are expected toanswer such questions in the near future.
Other Potential Targets
The mammalian target of rapamycin (mTOR) is a cellcycle regulator as well as an effector of the final commonpathway of PTEN/AKT, ametabolic pathway that is damagedin breast cancer [105]. When activated, mTOR promotesprotein synthesis and angiogenesis [105]. Everolimus(RAD001), an inhibitor of mTOR, is currently being evalu-ated in two phase II clinical trials in patients with TNBC(Trial of RAD001 in Triple Negative Metastatic Breast Cancer[NCT00827567] d a single-arm, non-randomised trial oforally administered RAD001 alone for the treatmentof metastatic TNBC d and Cisplatin and Paclitaxel With orWithout Everolimus in Treating Patients With Stage II orStage III Breast Cancer [NCT00930930] d a randomised,parallel-assignment, two-arm neoadjuvant study ofcisplatin and paclitaxel with or without RAD001 in patientswith locally advanced TNBC).
The Src family tyrosine kinase (STK) is overexpressed inbasal TNBC, in which it exerts a prominent role in phos-phorylating key regulators of adhesion and migration andpromoting tyrosine phosphorylation of the receptor tyro-sine kinases [106]. It has been reported that STK inhibitionattenuates cellular proliferation, survival and motility ofbasal breast cancer cell lines [106]. Dasatinib is an oral,small-molecule tyrosine kinase inhibitor that acts on STK.Preclinical studies have shown that dasatinib inhibits thegrowth of basal TNBC cell lines [107], providing the
rationale for clinical research to evaluate its use as mono-therapy or in combination regimens in the treatment ofTNBC.
Heat shock protein 90 is a cellular chaperone protein thatis widely expressed in breast cancer [108]. It facilitates thepost-translational maturation and stabilisation of a numberof conformationally labile client proteins, including RAF-1,cyclin-dependent kinase 4, AKT and other proteins thatplay a role in transducing proliferative signals [109]. Apreclinical study of the heat shock protein 90 inhibitor PU-H71 in TNBC xenografts showed an impressive response,including complete response and tumour regression,without toxicity to the host [108]; however, its use for thetreatment of human TNBC needs to be assessed in clinicaltrials. Furthermore, we and others [6], have shown thata proportion of patients with TNBC express androgenreceptors. A phase II clinical trial using the anti-androgenbicalutamide in the treatment of androgen receptor-positive TNBC is underway (Bicalutamide in TreatingPatients With Metastatic Breast Cancer [NCT00468715];a feasibility study to evaluate the use of bicalutamide for thetreatment of androgen receptor-positive, ERe, PRe MBC).
Conclusion
TNBC overlaps with BRCA1 germline mutation carriersand the basal-like molecular class of tumours. Clinicalexperience suggests that although TNBC is sensitive tochemotherapy, many women with metastatic TNBC relapsequickly. Furthermore, they are more likely to developvisceral metastasis, including brain metastasis, than othermolecular subtypes. This observation has important impli-cations for both clinical practice and clinical trial design.
Tumours with the triple-negative phenotype havespecific features that are potential therapeutic targets, e.g.they show an impaired DNA repair mechanism andincreased expression of basal-associated and proliferation-associated markers. Targets currently being investigatedinclude the DNA repair pathway, angiogenesis and EGFR.However, due to the heterogeneity of triple-negativetumours and the complexity of the molecular pathwaysinvolved in their development and progression, it ispostulated that the optimal therapeutic concept for TNBCwill eventually comprise a combination approach of cyto-toxic and targeted agents in an individual tailored pattern.At least one such combination approach d gemcitabi-neþ carboplatinþ iniparib (a PARP inhibitor)d is currentlyundergoing a phase III clinical trial.
Conflict of Interest Statement
During the preparation of this review article, the authorsreceived editorial assistance from Succinct HealthcareCommunications, Amersham, UK. This assistance, whichcomprised copy-editing and formatting, was supportedthrough an educational grant from sanofi-aventis, whichhad no input into the content.

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600598
References
[1] Haffty BG, Yang Q, Reiss M, et al. Locoregional relapse anddistant metastasis in conservatively managed triple negativeearly-stage breast cancer. J Clin Oncol 2006;24:5652e5657.
[2] Kwan ML, Kushi LH, Weltzien E, et al. Epidemiology of breastcancer subtypes in two prospective cohort studies of breastcancer survivors. Breast Cancer Res 2009;11: R31.
[3] Rakha EA, Reis-Filho JS, Ellis IO. Basal-like breast cancer:a critical review. J Clin Oncol 2008;26:2568e2581.
[4] Galea MH, Blamey RW, Elston CE, Ellis IO. The NottinghamPrognostic Index in primary breast cancer. Breast Cancer ResTreat 1992;22:207e219.
[5] Gluz O, Liedtke C, Gottschalk N, et al. Triple-negative breastcancerdcurrent status and future directions. Ann Oncol2009;20:1913e1927.
[6] Rakha EA, El-Sayed ME, Green AR, et al. Prognostic markersin triple-negative breast cancer. Cancer 2007;109:25e32.
[7] Cheang MC, Voduc D, Bajdik C, et al. Basal-like breast cancerdefined by five biomarkers has superior prognostic valuethan triple-negative phenotype. Clin Cancer Res 2008;14:1368e1376.
[8] Anderson WF, Chatterjee N, Ershler WB, Brawley OW.Estrogen receptor breast cancer phenotypes in the Surveil-lance, Epidemiology, and End Results database. Breast CancerRes Treat 2002;76:27e36.
[9] Rakha EA, El-Sayed ME, Green AR, et al. Biologic and clinicalcharacteristics of breast cancer with single hormonereceptor positive phenotype. J Clin Oncol2007;25:4772e4778.
[10] Prat A, Baselga J. The role of hormonal therapy in the manage-ment of hormonal-receptor-positive breast cancer with co-expression of HER2. Nat Clin Pract Oncol 2008;5:531e542.
[11] Kaplan HG, Malmgren JA. Impact of triple negative pheno-type on breast cancer prognosis. Breast J 2008;14:456e463.
[12] Cheang MC, Chia SK, Voduc D, et al. Ki67 index, HER2 status,and prognosis of patients with luminal B breast cancer. J NatlCancer Inst 2009;101:736e750.
[13] Azambuja E, Durbecq V, Rosa DD, et al. HER-2 over-expression/amplification and its interaction with taxane-based therapy in breast cancer. Ann Oncol 2008;19:223e232.
[14] Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breastcancer: clinical features and patterns of recurrence. ClinCancer Res 2007;13:4429e4434.
[15] Reis-Filho JS, Tutt AN. Triple negative tumours: a criticalreview. Histopathology 2008;52:108e118.
[16] Turner NC, Reis-Filho JS. Basal-like breast cancer and theBRCA1 phenotype. Oncogene 2006;25:5846e5853.
[17] Fong PC, Boss DS, Yap TA, et al. Inhibition of poly(ADP-ribose)polymerase in tumors from BRCA mutation carriers. N Engl JMed 2009;361:123e134.
[18] Al Tamimi DM, Shawarby MA, Ahmed A, et al. Proteinexpression profile and prevalence pattern of the molecularclasses of breast cancer e a Saudi population based study.BMC Cancer 2010;10:223.
[19] Sorlie T, Perou CM, Tibshirani R, et al. Gene expressionpatterns of breast carcinomas distinguish tumor subclasseswith clinical implications. Proc Natl Acad Sci USA 2001;98:10869e10874.
[20] Sorlie T, Tibshirani R, Parker J, et al. Repeated observation ofbreast tumor subtypes in independent gene expression datasets. Proc Natl Acad Sci USA 2003;100:8418e8423.
[21] Cleator S, Heller W, Coombes RC. Triple-negative breastcancer: therapeutic options. Lancet Oncol 2007;8:235e244.
[22] Carey LA, Perou CM, Livasy CA, et al. Race, breast cancersubtypes, and survival in the Carolina Breast Cancers Study.JAMA 2006;295:2492e2502.
[23] Hammond ME, Hayes DF, Dowsett M, et al. American Societyof Clinical Oncology/College of American Pathologistsguideline recommendations for immunohistochemicaltesting of estrogen and progesterone receptors in breastcancer. J Clin Oncol 2010;28:2784e2795.
[24] Wolff AC, Hammond ME, Schwartz JN, et al. AmericanSociety of Clinical Oncology/College of American Patholo-gists guideline recommendations for human epidermalgrowth factor receptor 2 testing in breast cancer. J Clin Oncol2007;25:118e145.
[25] Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologicalfeatures and sites of recurrence according to breast cancersubtype in the National Comprehensive Cancer Network(NCCN). J Clin Oncol 2009;27: abstract 543.
[26] Thike AA, Cheok PY, Jara-Lazaro AR, et al. Triple-negative breastcancer: clinicopathological characteristics and relationshipwith basal-like breast cancer.Mod Pathol 2010;23:123e133.
[27] Collett K, Stefansson IM, Eide J, et al. A basal epithelialphenotype is more frequent in interval breast cancerscompared with screen detected tumors. Cancer EpidemiolBiomarkers Prev 2005;14:1108e1112.
[28] YangWT, Dryden M, Broglio K, et al. Mammographic featuresof triple receptor-negative primary breast cancers in youngpremenopausal women. Breast Cancer Res Treat 2008;111:405e410.
[29] Au-Yong IT, Evans AJ, Taneja S, et al. Sonographic correlationswith the new molecular classification of invasive breastcancer. Eur Radiol 2009;19:2342e2348.
[30] Chen JH, Agrawal G, Feig B, et al. Triple-negative breastcancer: MRI features in 29 patients. Ann Oncol 2007;18:2042e2043.
[31] Uematsu T, Kasami M, Yuen S. Triple-negative breast cancer:correlation between MR imaging and pathologic findings.Radiology 2009;250:638e647.
[32] Basu S, Chen W, Tchou J, et al. Comparison of triple-negativeand estrogen receptor-positive/progesterone receptor-posi-tive/HER2-negative breast carcinoma using quantitativefluorine-18 fluorodeoxyglucose/positron emission tomo-graphy imaging parameters: a potentially useful method fordisease characterization. Cancer 2008;112:995e1000.
[33] Marginean F, Rakha EA, Ho BC, et al. Histological features ofmedullary carcinoma and prognosis in triple-negative basal-like carcinomas of the breast. Mod Pathol2010;23:1357e1363.
[34] Banerjee S, Reis-Filho JS, Ashley S, et al. Basal-like breastcarcinomas: clinical outcome and response to chemo-therapy. J Clin Pathol 2006;59:729e735.
[35] Hugh J, Hanson J, Cheang MC, et al. Breast cancer subtypesand response to docetaxel in node-positive breast cancer:use of an immunohistochemical definition in the BCIRG 001trial. J Clin Oncol 2009;27:1168e1176.
[36] Dabbs DJ, Chivukula M, Carter G, Bhargava R. Basal pheno-type of ductal carcinoma in situ: recognition and immuno-histologic profile. Mod Pathol 2006;19:1506e1511.
[37] Kusinska R, Potemski P, Jesionek-Kupnicka D, Kordek R.Immunohistochemical identification of basal-type cytoker-atins in invasiveductalbreast carcinomad relationwith grade,stage, estrogen receptor and HER2. Pol J Pathol2005;56:107e110.
[38] Tischkowitz M, Brunet JS, Begin LR, et al. Use of immuno-histochemical markers can refine prognosis in triple nega-tive breast cancer. BMC Cancer 2007;7:134.
E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600 599
[39] Crabb SJ, Cheang MC, Leung S, et al. Basal breast cancermolecular subtype predicts for lower incidence of axillarylymph node metastases in primary breast cancer. Clin BreastCancer 2008;8:249e256.
[40] Tan DS, Marchi�o C, Jones RL. Triple negative breast cancer:molecular profiling and prognostic impact in adjuvantanthracycline-treated patients. Breast Cancer Res Treat2008;111:24e44.
[41] Seewaldt VL, Scott V. Images in clinical medicine. Rapidprogression of basal-type breast cancer. N Engl J Med2007;356: e12.
[42] Rakha EA, Elsheikh SE, Aleskandarany MA, et al. Triple-negative breast cancer: distinguishing between basal andnonbasal subtypes. Clin Cancer Res 2009;15:2302e2310.
[43] Jumppanen M, Gruvberger-Saal S, Kauraniemi P, et al. Basal-like phenotype is not associated with patient survival inestrogen-receptor-negative breast cancers. Breast Cancer Res2007;9: R16.
[44] Shakya R, Szabolcs M, McCarthy E, et al. The basal-likemammary carcinomas induced by Brca1 or Bard1 inactiva-tion implicate the BRCA1/BARD1 heterodimer in tumorsuppression. Proc Natl Acad Sci USA 2008;105:7040e7045.
[45] Langerod A, Zhao H, Borgan O, et al. TP53 mutation statusand gene expression profiles are powerful prognosticmarkers of breast cancer. Breast Cancer Res 2007;9: R30.
[46] Subhawong AP, Subhawong T, Nassar H, et al. Most basal-likebreast carcinomas demonstrate the same Rbe/p16þ immu-nophenotype as the HPV-related poorly differentiatedsquamous cell carcinomas which they resemble morpho-logically. Am J Surg Pathol 2009;33:163e175.
[47] Gauthier ML, Berman HK, Miller C, et al. Abrogated responseto cellular stress identifies DCIS associated with subsequenttumor events and defines basal-like breast tumors. CancerCell 2007;12:479e491.
[48] Reis-Filho J, Pinheiro C, Lambros M, et al. EGFR amplificationand lack of activating mutations in metaplastic breastcarcinomas. J Pathol 2006;209:445e453.
[49] Gilbert JA, Goetz MP, Reynolds CA, et al. Molecular analysis ofmetaplastic breast carcinoma: high EGFR copy number viaaneusomy. Mol Cancer Ther 2008;7:944e951.
[50] Rakha EA, Tan DS, Foulkes WD, et al. Are triple-negativetumours and basal-like breast cancer synonymous? BreastCancer Res 2007;9:404.
[51] Bertucci F, Finetti P, Cervera N, et al. How basal are triple-negative breast cancers? Int J Cancer 2008;123:236e240.
[52] Natrajan R, Lambros MB, Rodriguez-Pinilla SM, et al. Tilingpath genomic profiling of grade 3 invasive ductal breastcancers. Clin Cancer Res 2009;15:2711e2722.
[53] Bergamaschi A, KimYH,WangP, et al. Distinct patterns ofDNAcopy number alteration are associated with different clinico-pathological features and gene-expression subtypes of breastcancer. Genes Chromosomes Cancer 2006;45:1033e1040.
[54] Wang ZC, Lin M, Wei LJ, et al. Loss of heterozygosity and itscorrelation with expression profiles in subclasses of invasivebreast cancers. Cancer Res 2004;64:64e71.
[55] McCabe N, Turner NC, Lord CJ, et al. Deficiency in the repairof DNA damage by homologous recombination and sensi-tivity to poly(ADP-ribose) polymerase inhibition. Cancer Res2006;66:8109e8115.
[56] Hedenfalk I, Duggan D, Chen Y, et al. Gene-expressionprofiles in hereditary breast cancer. N Engl J Med2001;344:539e548.
[57] Kandel MJ, Stadler Z, Masciari S, et al. Prevalence of BRCA1mutations in triple negative breast cancer (BC). J Clin Oncol2006;24: abstract 508.
[58] Nofech-Mozes S, Trudeau M, Kahn HK, et al. Patterns ofrecurrence in the basal and non-basal subtypes oftriple-negative breast cancers. Breast Cancer Res Treat2009;118:131e137.
[59] Azoulay S, Lae M, Freneaux P, et al. KIT is highly expressed inadenoid cystic carcinoma of the breast, a basal-like carci-noma associated with a favorable outcome. Mod Pathol2005;18:1623e1631.
[60] Rakha EA, Putti TC, Abd El-Rehim DM, et al. Morphologicaland immunophenotypic analysis of breast carcinomas withbasal and myoepithelial differentiation. J Pathol 2006;208:495e506.
[61] Largillier R, Ferrero JM, Doyen J, et al. Prognostic factors in1,038 women with metastatic breast cancer. Ann Oncol2008;19:2012e2019.
[62] Miles DW, Chan A, Dirix LY, et al. Phase III study of bev-acizumab plus docetaxel compared with placebo plusdocetaxel for the first-line treatment of human epidermalgrowth factor receptor 2-negative metastatic breast cancer. JClin Oncol 2010;28:3239e3247.
[63] Fulford LG, EastonDF, Reis-Filho JS, et al. Specificmorphologicalfeatures predictive for the basal phenotype in grade 3 invasiveductal carcinoma of breast. Histopathology 2006;49:22e34.
[64] De Giorgi U, Rosti G, Frassineti L, et al. High-dose chemo-therapy for triple negative breast cancer. Ann Oncol 2007;18:202e203.
[65] Kaplan HG, Malmgren JA, Atwood MK. T1N0 triple negativebreast cancer: adjuvant chemotherapy treatment and risk ofrecurrence. Breast J 2009;15:454e460.
[66] Di Leo A, Isola J, Piette F, et al. A meta-analysis of phase IIItrials evaluating the predictive value of HER2 and top-oisomerase II alpha in early breast cancer patients treatedwith CMF or anthracycline-based adjuvant therapy. BreastCancer Res Treat 2008;107: abstract 705.
[67] Cheang M, Chia SK, Tu D, et al. Anthracyclines in basal breastcancer: the NCIC-CTG trial MA5 comparing adjuvant CMF toCEF. J Clin Oncol 2009;27:519.
[68] Rodriguez-Pinilla SM, Sarrio D, Honrado E, et al. Prognosticsignificance of basal-like phenotype and fascin expression innode-negative invasive breast carcinomas. Clin Cancer Res2006;12:1533e1539.
[69] Sirohi B, Arnedos M, Popat S, et al. Platinum-based chemo-therapy in triple-negative breast cancer. Ann Oncol 2008;19:1847e1852.
[70] Byrski T, Gronwald J, Huzarski T, et al. Pathologic completeresponse rates in young women with BRCA1-positive breastcancers after neoadjuvant chemotherapy. J Clin Oncol 2010;28:375e379.
[71] Rottenberg S, Nygren AO, Pajic M, et al. Selective induction ofchemotherapy resistance of mammary tumors in a condi-tional mouse model for hereditary breast cancer. Proc NatlAcad Sci USA 2007;104:12117e12122.
[72] Fourquet A, Stoppa-Lyonnet D, Kirova YM, et al. Familialbreast cancer: clinical response to induction chemotherapyor radiotherapy related to BRCA1/2 mutations status. Am JClin Oncol 2009;32:127e131.
[73] Kyndi M, Sorensen FB, Knudsen H, et al. Estrogen receptor,progesterone receptor, HER-2, and response to post-mastectomy radiotherapy in high-risk breast cancer: theDanish Breast Cancer Cooperative Group. J Clin Oncol2008;26:1419e1426.
[74] Early Breast Cancer Trialists’ Collaborative Group (EBCTCG).Effects of chemotherapy and hormonal therapy for earlybreast cancer on recurrence and 15-year survival: an over-view of the randomised trials. Lancet 2005;365:687e717.

E.A. Rakha, S. Chan / Clinical Oncology 23 (2011) 587e600600
[75] Tsutsui S,OhnoS,MurakamiS,HachitandaY,OdaS. Prognosticvalue of epidermal growth factor receptor (EGFR) and itsrelationship to the estrogen receptor status in 1029 patientswith breast cancer. Breast Cancer Res Treat 2002;71:67e75.
[76] Agrawal A, Gutteridge E, Gee JM, et al. Overview of tyrosinekinase inhibitors in clinical breast cancer. Endocr Relat Cancer2005;12(Suppl. 1):S135e144.
[77] Kurebayashi J, Okubo S, Yamamoto Y, Sonoo H. Inhibition ofHER1 signaling pathway enhances antitumor effect ofendocrine therapy in breast cancer. Breast Cancer2004;11:38e41.
[78] Irvin Jr WJ, Carey LA. What is triple-negative breast cancer?Eur J Cancer 2008;44:2799e2805.
[79] Dogu GG, Ozkan M, Ozturk F, et al. Triple-negative breastcancer: immunohistochemical correlation with basaloidmarkers and prognostic value of survivin. Med Oncol2010;27:34e39.
[80] Mendelsohn J, Baselga J. Epidermal growth factor receptortargeting in cancer. Semin Oncol 2006;33:369e385.
[81] Oliveras-Ferraros C, Vazquez-Martin A, Lopez-Bonet E, et al.Growth and molecular interactions of the anti-EGFR anti-body cetuximab and the DNA cross-linking agent cisplatin ingefitinib-resistant MDA-MB-468 cells: new prospects in thetreatment of triple-negative/basal-like breast cancer. Int JOncol 2008;33:1165e1176.
[82] O’Shaughnessy J, Weckstein DJ, Vukelja SJ. Preliminaryresults of a randomized phase II study of weekly irinotecan/carboplatin with or without cetuximab in patients withmetastatic breast cancer. Breast Cancer Res Treat2007;106(S1):S32: abstract 308 (presentation).
[83] Eppenberger U, Kueng W, Schlaeppi JM, et al. Markers oftumor angiogenesis and proteolysis independently definehigh- and low-risk subsets of node-negative breast cancerpatients. J Clin Oncol 1998;16:3129e3136.
[84] Linderholm BK, Hellborg H, Johansson U, et al. Significantlyhigher levels of vascular endothelial growth factor (VEGF)and shorter survival times for patients with primary oper-able triple-negative breast cancer. Ann Oncol2009;20:1639e1646.
[85] Miller K, Wang M, Gralow J, et al. Paclitaxel plus bev-acizumab versus paclitaxel alone for metastatic breastcancer. N Engl J Med 2007;357:2666e2676.
[86] Robert NJ, Dieras V, Glaspy J, et al. RIBBON-1: randomized,double-blind, placebo-controlled phase III trial of chemo-therapy with or without bevacizumab (B) for first-linetreatment of HER2-negative locally recurrent or metastaticbreast cancer (MBC). ASCO Annual Meeting 2009; abstract1005.
[87] Ryan PD, Tung NM, Isakoff SJ, et al. Neoadjuvant cisplatinand bevacizumab in triple negative breast cancer (TNBC):safety and efficacy. J Clin Oncol 2009;27: abstract 551.
[88] Burstein HJ, Elias AD, Rugo HS, et al. Phase II study of sunitinibmalate, an oral multitargeted tyrosine kinase inhibitor, inpatients with metastatic breast cancer previously treatedwith an anthracycline and a taxane. J Clin Oncol2008;26:1810e1816.
[89] Aulmann S, Adler N, Rom J, et al. c-myc amplifications inprimary breast carcinomas and their local recurrences. J ClinPathol 2006;59:424e428.
[90] Grushko TA, Dignam JJ, Das S, et al. MYC is amplified inBRCA1-associated breast cancers. Clin Cancer Res 2004;10:499e507.
[91] Rodriguez-Pinilla SM, Jones RL, Lambros MB, et al. MYCamplification in breast cancer: a chromogenic in situ hybrid-isation study. J Clin Pathol 2007;60:1017e1023.
[92] Burgess DJ, Doles J, Zender L, et al. Topoisomerase levelsdetermine chemotherapy response in vitro and in vivo. ProcNatl Acad Sci USA 2008;105:9053e9058.
[93] Bouchalova K, Cizkova M, Cwiertka K, et al. Triple negativebreast cancer e current status and prospective targetedtreatment based on HER1 (EGFR), TOP2A and C-MYC geneassessment. Biomed Pap Med Fac Univ Palacky Olomouc CzechRepub 2009;153:13e17.
[94] Knoop AS, Knudsen H, Balslev E, et al. Retrospective analysisof topoisomerase IIa amplifications and deletions aspredictive markers in primary breast cancer patientsrandomly assigned to cyclophosphamide, methotrexate, andfluorouracil or cyclophosphamide, epirubicin, and fluoro-uracil: Danish Breast Cancer Cooperative Group. J Clin Oncol2005;23:7483e7490.
[95] Chalmers AJ. The potential role and application of PARPinhibitors in cancer treatment. Br Med Bull 2009;89:23e40.
[96] Farmer H, McCabe N, Lord CJ, et al. Targeting the DNA repairdefect in BRCA mutant cells as a therapeutic strategy. Nature2005;434:917e921.
[97] Bryant HE, Schultz N, Thomas HD, et al. Specific killing ofBRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 2005;434:913e917.
[98] Fong PC, Yap TA, Boss DS, et al. Poly(ADP)-ribose polymeraseinhibition: frequent durable responses in BRCA carrierovarian cancer correlating with platinum-free interval. J ClinOncol 2010;28:2512e2519.
[99] Hashimoto K, Tamura K. Breakthrough breast cancer treat-ment e PARP inhibitor, BRCA, and triple negative breastcancer. Gan To Kagaku Ryoho 2010;37:1187e1191.
[100] Mendes-Pereira AM, Martin SA, Brough R, et al. Syntheticlethal targeting of PTEN mutant cells with PARP inhibitors.EMBO Mol Med 2009;1:315e322.
[101] Ratnam K, Low JA. Current development of clinical inhibitorsof poly(ADP-ribose) polymerase in oncology. Clin Cancer Res2007;13:1383e1388.
[102] O’Shaughnessy J, Osborne C, Pippen JE, et al. Iniparib pluschemotherapy in metastatic triple-negative breast cancer. NEngl J Med 2011;364:205e214.
[103] Tutt A, Robson M, Garber JE, et al. Oral poly(ADP-ribose)polymerase inhibitor olaparib in patients with BRCA1 orBRCA2 mutations and advanced breast cancer: a proof-of-concept trial. Lancet 2010;376:235e244.
[104] Edwards SL, Brough R, Lord CJ, et al. Resistance to therapycaused by intragenic deletion in BRCA2. Nature 2008;451:1111e1115.
[105] Faivre S, Kroemer G, Raymond E. Current development ofmTOR inhibitors as anticancer agents. Nat Rev Drug Discov2006;5:671e688.
[106] Hochgrafe F, Zhang L, O’Toole SA, et al. Tyrosinephosphorylation profiling reveals the signaling networkcharacteristics of basal breast cancer cells. Cancer Res2010;70:9391e9401.
[107] Finn RS, Dering J, Ginther C, et al. Dasatinib, an orally activesmall molecule inhibitor of both the src and abl kinases,selectively inhibits growth of basal-type/"triple-negative"breast cancer cell lines growing in vitro. Breast Cancer ResTreat 2007;105:319e326.
[108] Caldas-Lopes E, Cerchietti L, Ahn JH, et al. Hsp90 inhibitorPU-H71, a multimodal inhibitor of malignancy, inducescomplete responses in triple-negative breast cancer models.Proc Natl Acad Sci USA 2009;106:8368e8373.
[109] Bagatell R, Whitesell L. Altered Hsp90 function in cancer:a unique therapeutic opportunity. Mol Cancer Ther2004;3:1021e1030.