Embed Size (px)
Citation preview
Trastuzumab in Metastatic Breast Cancer
• Teaching an old dog new tricks
• Rama Suresh, M.D.
• Fellow, Division of Hematology-Oncology
HER 2
Discovered in 1980
• Member of EGFR family
• Overexpressed in 25 to 30% of breast cancers
• Shortened survival and relative resistance to therapies
IHC
HER2 protein expression
• Grading – 0, 1+(negative)– 2+ (indeterminant) – 3+(positive)
• Low volume labs correlate poorly with the reference labs (JNCI 2002;94: 852-854 and 855-857)
FISH
HER2 gene overexpression
• PathVysion HER2 DNA probe– positive if HER2 to CEP17 is> 2
• Gold standard
• Results are similar with IHC 3+
• Indicated when IHC 2+ or aggressive tumor with IHC 0+/1+
Trastuzumab
• Binds to the EC domain of HER2
• FDA approved (1998)
• Only in IHC 3+ or FISH +
Dosage
• Loading 4mg/kg over 90min – weekly 2mg/kg over 30min
• Half life 30days (Washington CB, Clin Pharmacol Ther 2002;71:12.Abstract)
• Loading 8mg/kg maintenance – 6mg/kg q 3wks – Gelmon (ASCO 2001;20:271 Abstract)
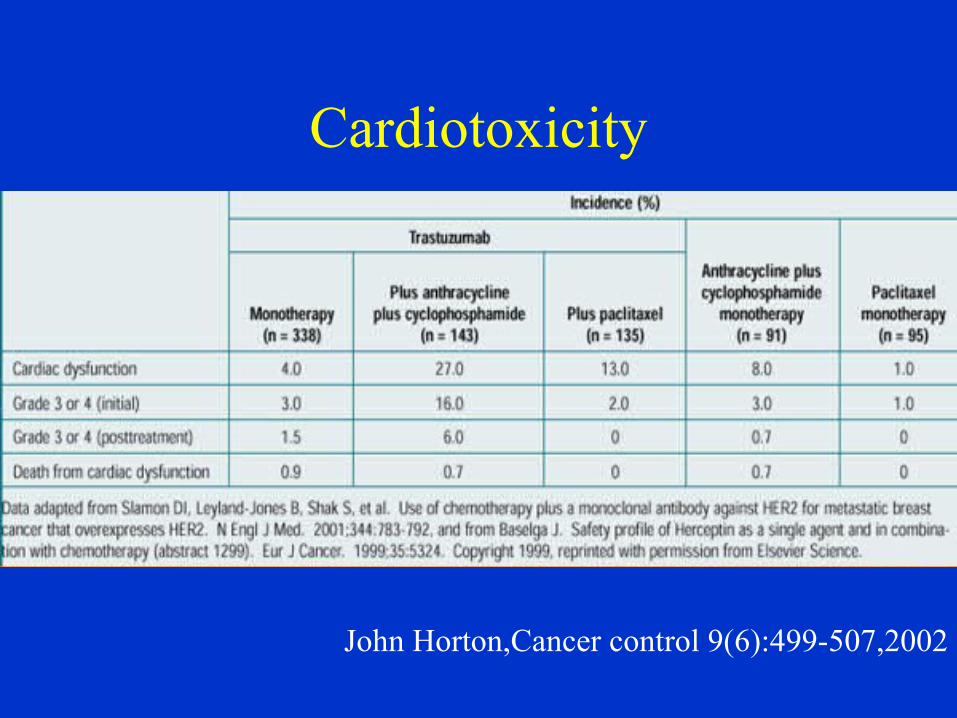
Cardiotoxicity
John Horton,Cancer control 9(6):499-507,2002
Other toxicity
• Infusion reaction 40%– Fever,chills, nausea, vomiting, body pain, rigors,
Headache, dizziness, rash, hypotension
• Diarrhea 25%
• Grade 3 hematological toxicity <1%• Anaphylaxis/pulmonary events• Glomerulopathy
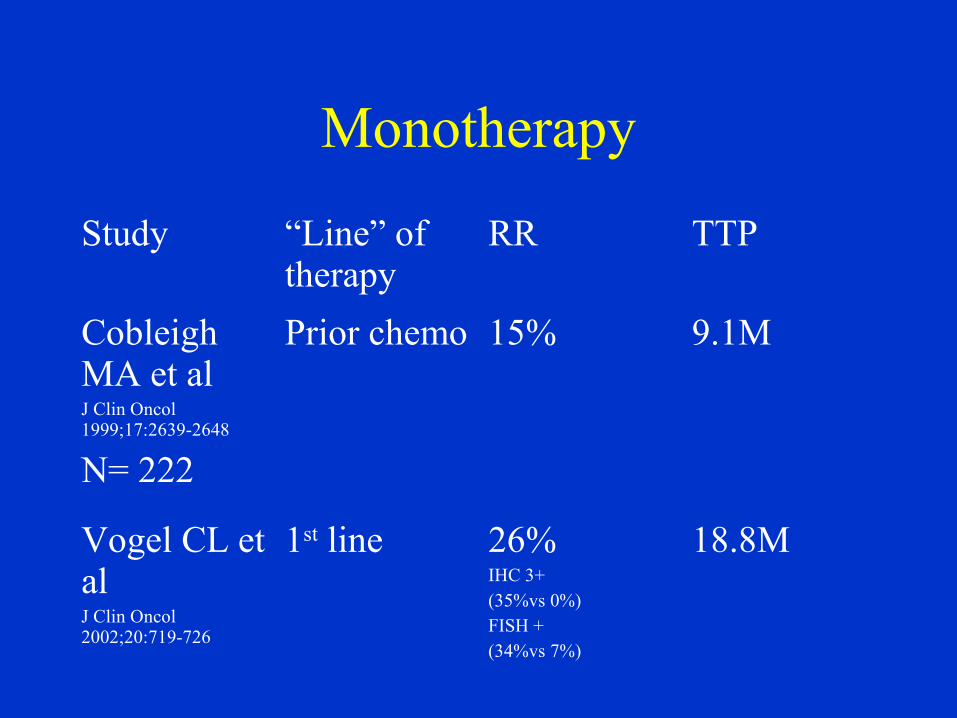
Monotherapy
Study “Line” of therapy
RR TTP
Cobleigh MA et alJ Clin Oncol 1999;17:2639-2648
N= 222
Prior chemo 15% 9.1M
Vogel CL et alJ Clin Oncol 2002;20:719-726
1st line 26%IHC 3+ (35%vs 0%)FISH + (34%vs 7%)
18.8M

Interaction of Trastuzumab with chemotherapy in cell lines
Interaction Agent
Synergy Cisplatin, Carboplatin, DocetaxelVinorelbine, Etoposide, Thiotepa, XRTPaclitaxel, Doxorubicin
Addition Vinblastine, Methotrexate
Antagonism 5-FU
Nabholtz et al,Clinical Breast Cancer3S2:75-79,Oct 2002Based on articles of Pegram, Oncogene1999 and Konecny, Breast Cancer Res Treat 1999
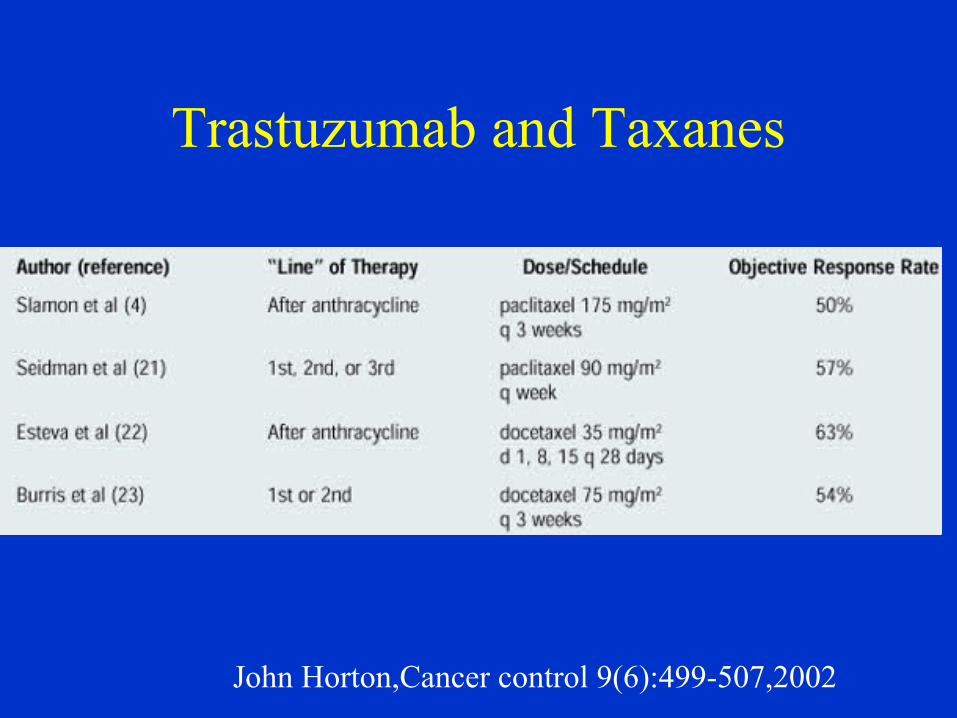
Trastuzumab and Taxanes
John Horton,Cancer control 9(6):499-507,2002
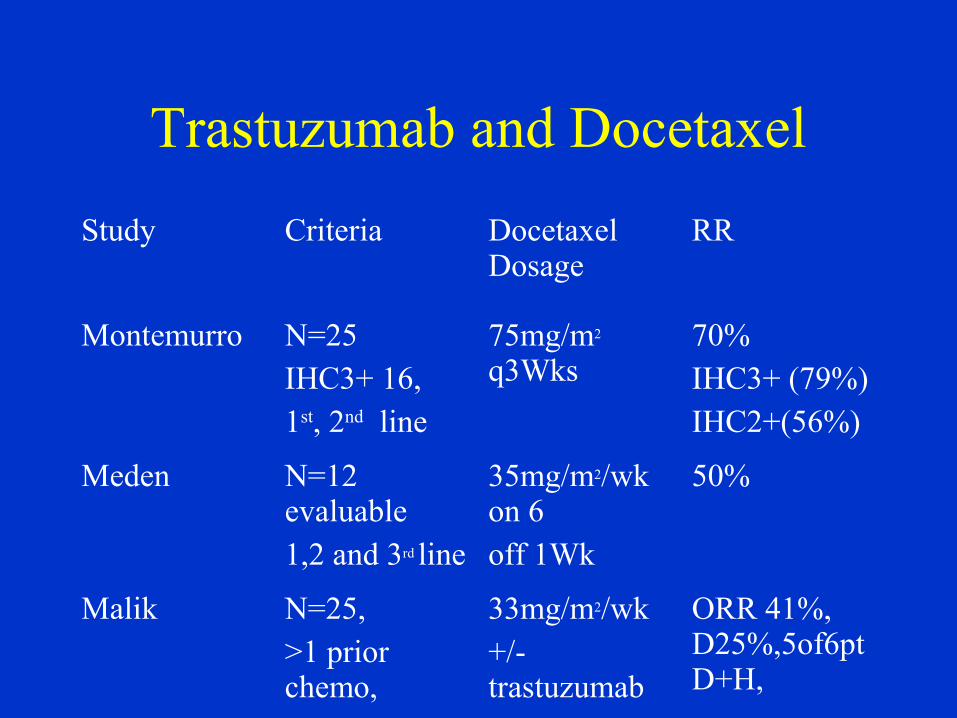
Trastuzumab and Docetaxel
Study Criteria Docetaxel Dosage
RR
Montemurro N=25 IHC3+ 16,1st, 2nd line
75mg/m2 q3Wks
70%IHC3+ (79%)IHC2+(56%)
Meden N=12 evaluable1,2 and 3rd line
35mg/m2/wk on 6 off 1Wk
50%
Malik N=25, >1 prior chemo,
33mg/m2/wk+/- trastuzumab
ORR 41%, D25%,5of6ptD+H,
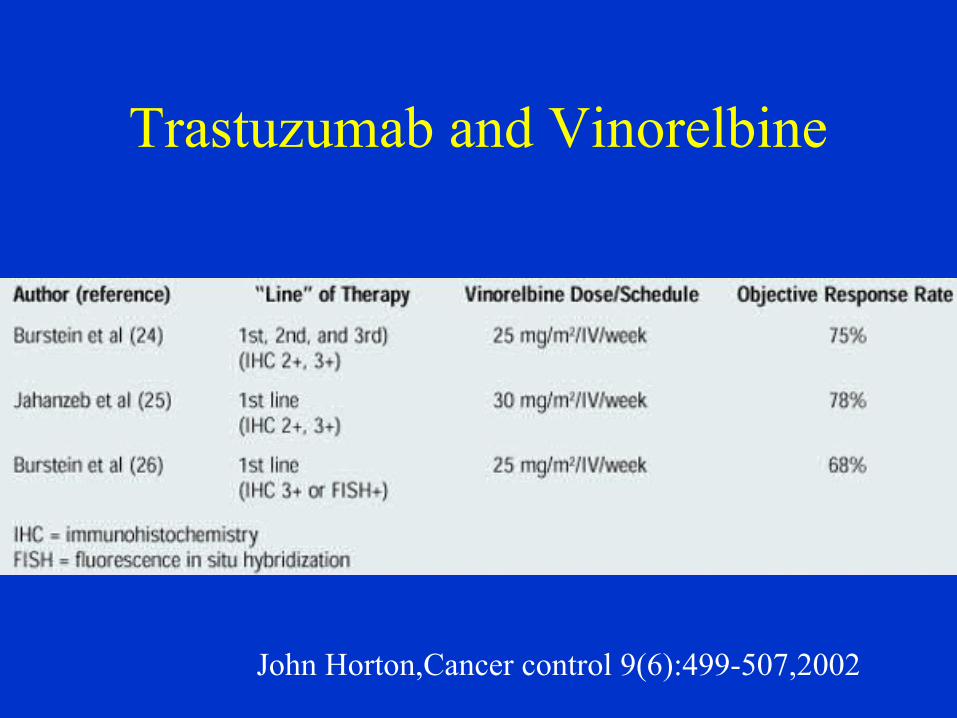
Trastuzumab and Vinorelbine
John Horton,Cancer control 9(6):499-507,2002
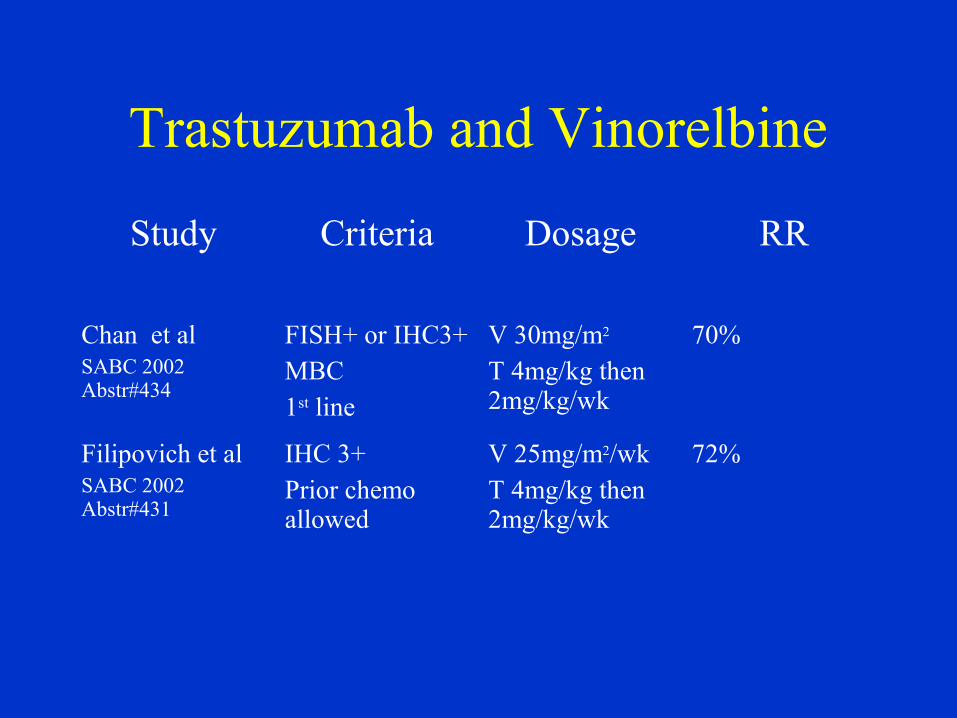
Trastuzumab and Vinorelbine
Study Criteria Dosage RR
Chan et alSABC 2002 Abstr#434
FISH+ or IHC3+MBC1st line
V 30mg/m2 T 4mg/kg then 2mg/kg/wk
70%
Filipovich et alSABC 2002 Abstr#431
IHC 3+Prior chemo allowed
V 25mg/m2/wkT 4mg/kg then 2mg/kg/wk
72%
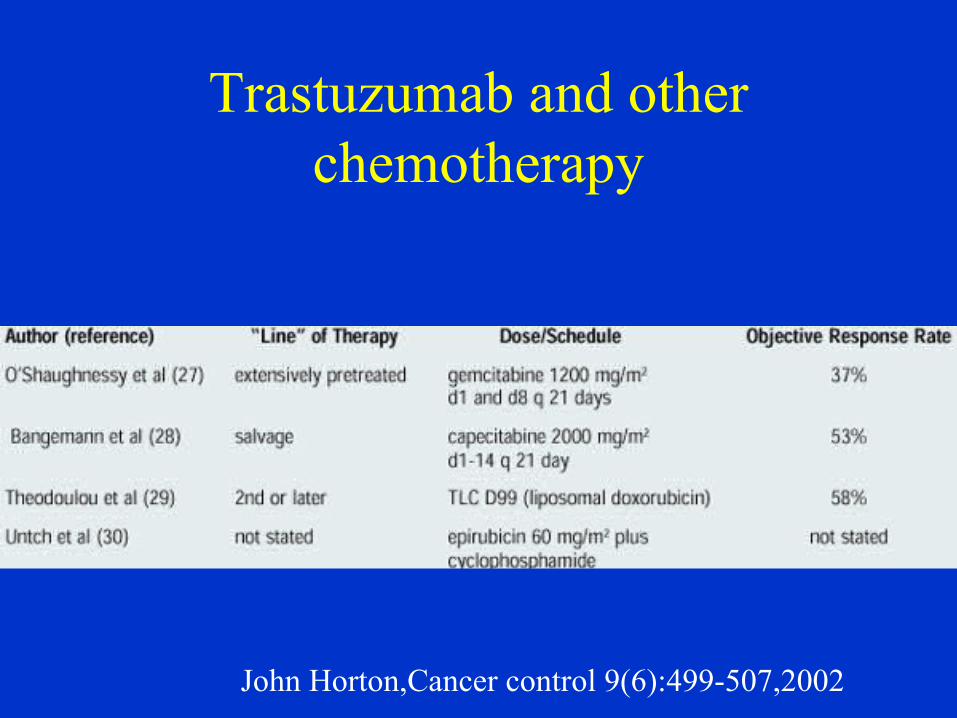
Trastuzumab and other chemotherapy
John Horton,Cancer control 9(6):499-507,2002
HET regimen
• Epirubicin 75 mg/m2 D1, Taxotere 75mg/m2 D1 Q21days• Trastuzumab as usual• 1st step 29pts presented • IHC2+/3+• 1 CHF • 2 decrease in LVEF (no CHF)• Gr 3/4 neutropenia 16% of cycles, 3 febrile neutropenia• Gr 1/2 nonhematological toxicity
(asthenia,N/V,mucositis,fever,bone pain)• 2nd step 30 additional pts being recruited
Bighin et al, ASCO 2002 Abstr#1973
Trastuzumab+Paclitaxel+Gemcitabine
• FISH+ or IHC 2-3+• T dosage as usual weekly • Paclitaxel 175mg/m2 on D1+• Gemcitabine 1200mg/m2 on days 1 and 8 q3wks+• Max 6 cycles. Responding and stable patients
continued on T till progression• 45pts • RR 62%, MTP 18M• Gr 4 neutropenia (20), Pulm toxicity (5), CHF(3)
Hoosier Oncology Group trial Miller et al, SABC 2002 Abstr#437
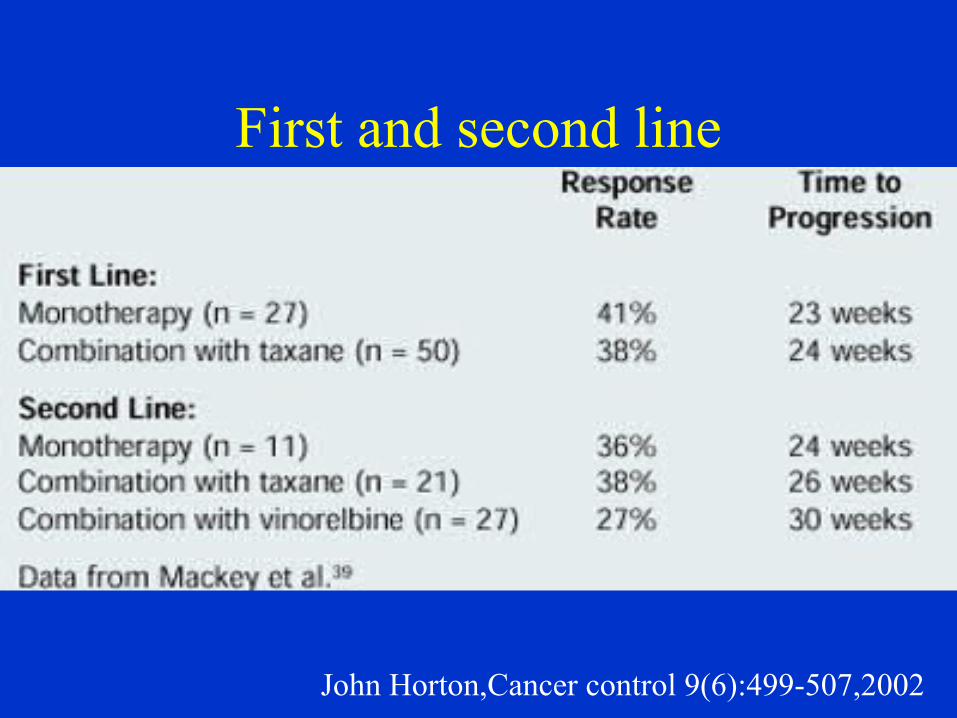
First and second line
John Horton,Cancer control 9(6):499-507,2002
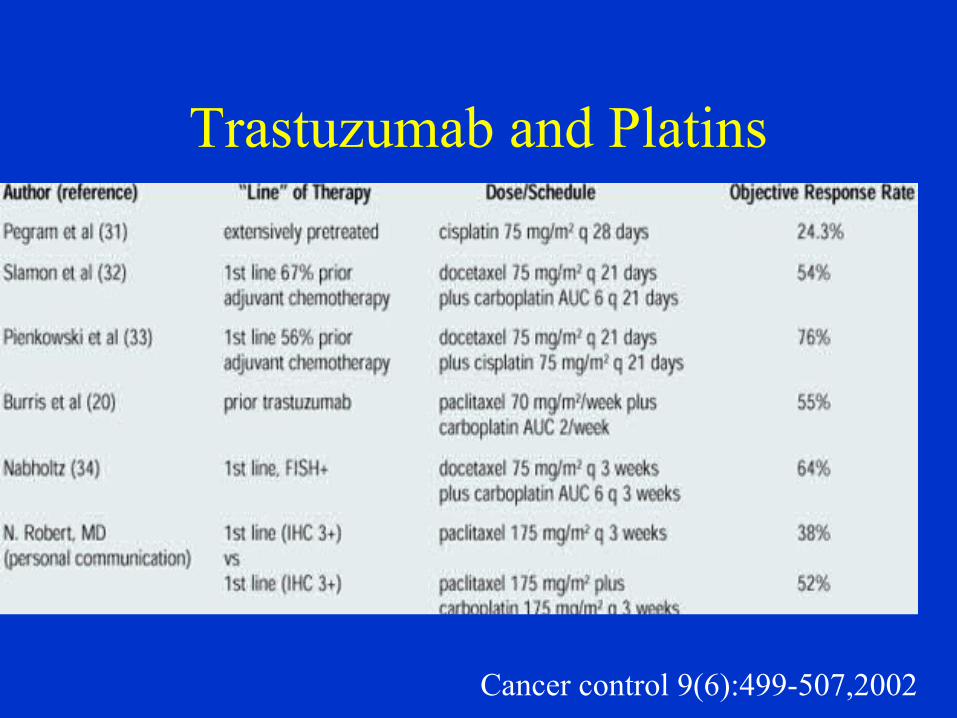
Trastuzumab and Platins
Cancer control 9(6):499-507,2002
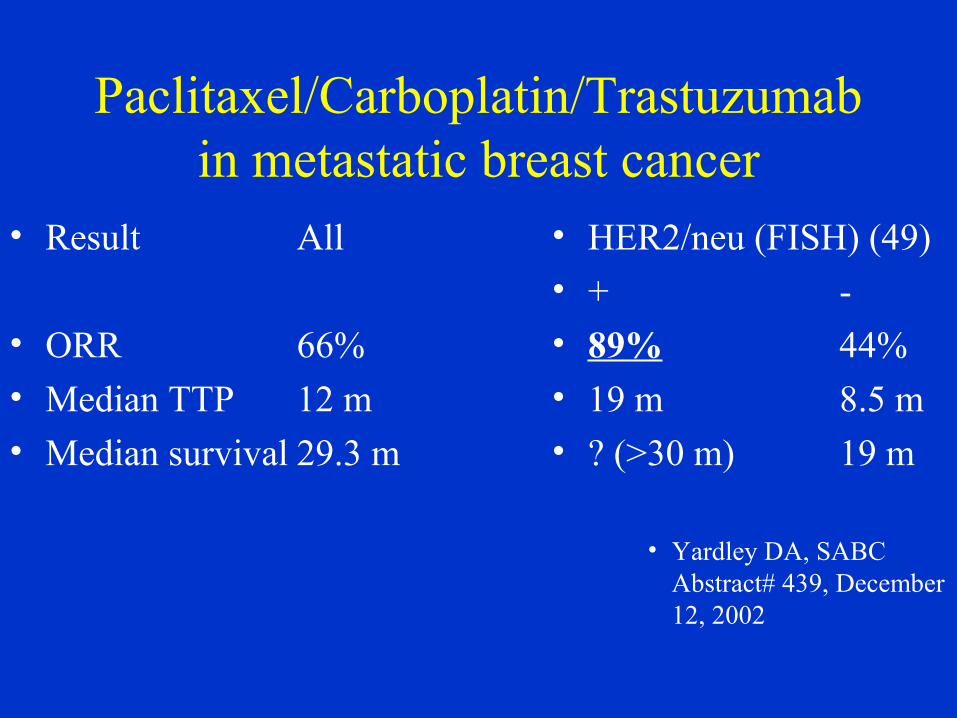
Paclitaxel/Carboplatin/Trastuzumabin metastatic breast cancer
• Result All
• ORR 66%• Median TTP 12 m• Median survival 29.3 m
• HER2/neu (FISH) (49)• + -
• 89% 44%• 19 m 8.5 m• ? (>30 m) 19 m
• Yardley DA, SABC Abstract# 439, December 12, 2002
Paclitaxel/Carboplatin/Trastuzumabin metastatic breast cancer
• Phase II multicenter pilot• 61 patients
– HER2 overexpression (IHC 2+ or 3+)– 52 years (median) – ECOG 0-1– 50% ER+ – >50% hepatic involvement
– Prior adjuvant therapy in 33– Newly diagnosed stage IV in 20
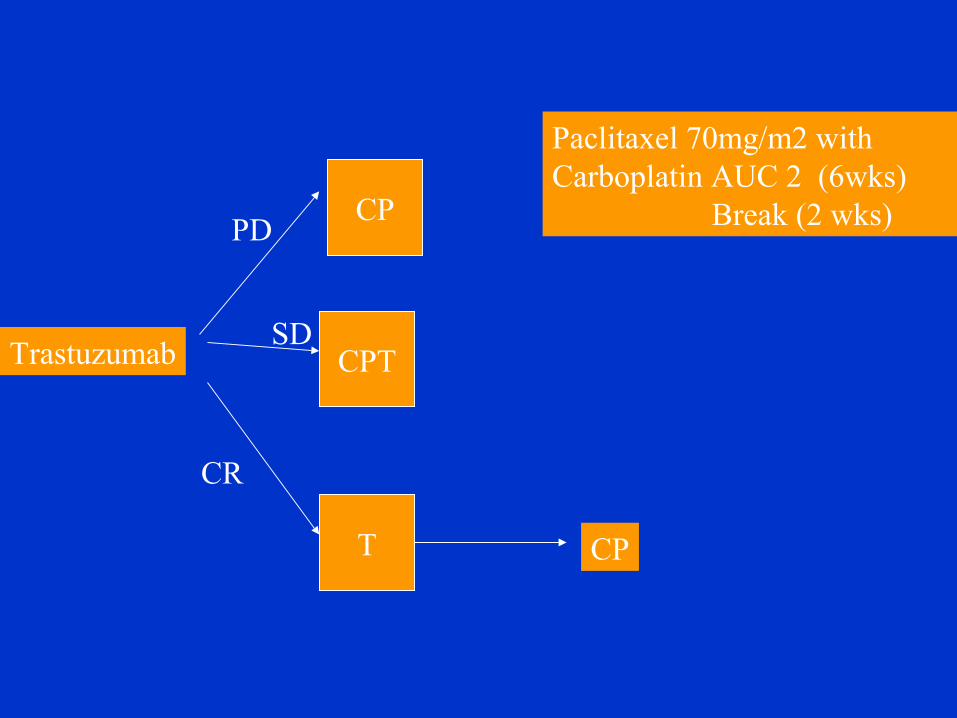
CP
Trastuzumab
PD
SD
CR
CP
Paclitaxel 70mg/m2 with Carboplatin AUC 2 (6wks)
Break (2 wks)
CPT
T
Toxicity
• 33% had Grade 3/4 leukopenia (no febrile neutropenia)
• Rare 3/4 non-hematological toxicity– 7% fatigue, 4% diarrhea, 4% neuropathy– 4% asymptomatic LVEF decline (recovered)

BCIRG
101 102
Cisplatin+Docetaxel q3W +Trastuzumab q1W
Carboplatin+Docetaxel q3W +Trastuzumab q1W
No prior chemo Prior taxane allowed
RR 79% RR 56%
Toxicity
• 1 pt Grade 3 infection • 3pts febrile neutropenia
• Grade 3/4 non-hematological side effect rare– Fatigue 11%– Stomatitis 11%– Nausea 7%
– Vomiting, diarrhea, myalgia, edema and skin disorder in 1 pt each
– 1pt with LVEF decline
Phase III comparitive study of Trastuzumab+Paclitaxel
+/-carboplatin• 194 patients• 83% Caucasian
• ECOG PS 0/1/2 were 60%/36%/4%• median age 55• No prior chemo for metastatic disease
• 40% had adj chemo• Cumulative anthracycline not >360mg/m2• 2/3 IHC 3+
US Oncology GroupRobert N, Leyland-Jones SABC Abstr # 35, Dec 2002
Dosage Schedule
• Trastuzumab 4mg/kg loading and 2mg/kg q week
• Paclitaxel 175mg/m2 q 3 wks
• Carboplatin AUC 6 q 3wks
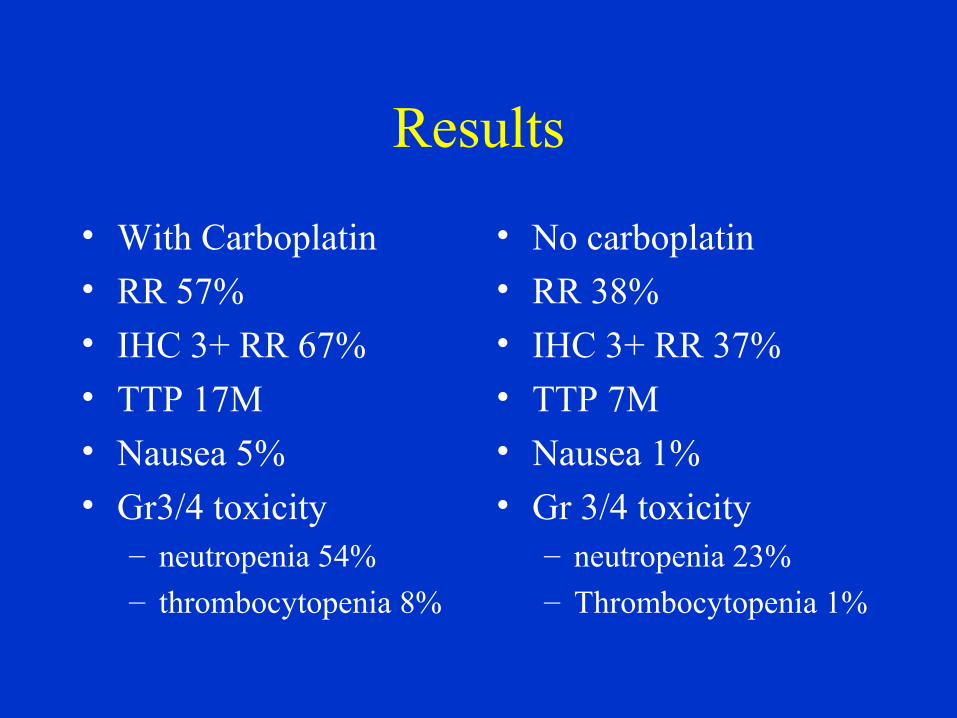
Results
• With Carboplatin• RR 57%
• IHC 3+ RR 67%• TTP 17M• Nausea 5%
• Gr3/4 toxicity– neutropenia 54%– thrombocytopenia 8%
• No carboplatin• RR 38%
• IHC 3+ RR 37%• TTP 7M• Nausea 1%
• Gr 3/4 toxicity– neutropenia 23%– Thrombocytopenia 1%
Proposed trial
• Carboplatin, Navelbine and Trastuzumab in Metastatic Breast Cancer