-
8/10/2019 PLD in Metastatic Breast Cancer
1/36
V1.0
Pegylated LiposomalDoxorubicin
and Breast Cancer
-
8/10/2019 PLD in Metastatic Breast Cancer
2/36
V1.0
Reduced Cardiotoxicity andComparable Efficacy in a Phase III
Trial
of Pegylated Liposomal Doxorubicin
Versus Conventional Doxorubicin forFirst-line Treatment of
Metastatic
Breast Cancer
OBrien M et al. Ann Oncol 2004; 15: 440-449
-
8/10/2019 PLD in Metastatic Breast Cancer
3/36
V1.0
OBrien Study Design
PLD 50 mg/m2
IV over 11.5 hours
Q4W
(n = 254)
Conventional
doxorubicin 60 mg/m2
IV over 1 hour Q3W
(n = 255)
1stline MBC, with
normal cardiac
function
Prior adjuvantanthracyclines
permitted
300 mg/m2
Randomized 1:1
N = 509
Progression-free survival and cardiotoxicityPrimary
endpoints:
Phase III, randomized, multicenter, international, open-label
trial
OBrien M et al. Ann Oncol 2004; 15: 440-449
TR
E
A
T
T
O
P
R
O
G
R
E
SS
I
O
N
-
8/10/2019 PLD in Metastatic Breast Cancer
4/36
V1.0
Baseline Patient Characteristics
*Cardiac risk factors: prior mediastinal irradiation, age >65
years, history of heart disease or had hypertension ordiabetes
requiring medical treatment. OBrien M et al. Ann Oncol 2004; 15:
440-449
PLD
(n=254)
Conventional doxorubicin
(n=255)
Median age (years) 58 (2882) 57 (2582)
Race
Caucasian 77.1% 75.6%
Hispanic 19.6% 19.6%
Other 3% 4.6%
Menopausal status at diagnosis
Premenopausal 30.7% 35.2%
Post menopausal 68.8% 62.3%
Unknown 0.3% 2.3%
WHO Performance Status
0 53.9% 49%
1 37% 39.6%
2 9% 10.9%
Missing 0 0.3%
Cardiac risk factors 48% 47.4%
-
8/10/2019 PLD in Metastatic Breast Cancer
5/36
V1.0
Cardiotoxicity
OBrien M et al. Ann Oncol 2004; 15: 440-449
PLD
(n=254)
Conventional
doxorubicin
(n=255)
Patients who developed
cardiotoxicity (LVEF decrease)
4% 19%
Cardiotoxicity with signs and
symptoms of CHF0 4%
Cardiotoxicity without signs
and symptoms of CHF4% 15%
Signs and symptoms of CHF
alone
-
8/10/2019 PLD in Metastatic Breast Cancer
6/36
V1.0
Efficacy Endpoints
*Overall response rate (n = 410); PLD n = 209; conventional
doxorubicin n = 201
OBrien M et al. Ann Oncol 2004; 15: 440-449
PLD
(n=254)
Conventional
doxorubicin
(n=255)
PFS 6.9 months 7.8 months
Overall Survival 21 months 22 months
Overall Response rate 33% 38%
-
8/10/2019 PLD in Metastatic Breast Cancer
7/36V1.0
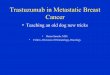
Cardiac Event Rates
100
90
80
70
60
50
40
30
20
10
0
0 50 100 150 200 300250 400 450 500 550 600350
Cumulative Anthracycline Dose (mg/m2)
Ka
plan-MeierEstimatesof
CardiacEvent
Rate
PLD
Conventionaldoxorubicin
Hazard ratio = 3.16 (95% CI: 1.58 - 6.31); P
-
8/10/2019 PLD in Metastatic Breast Cancer
8/36V1.0
Incidence of Cardiotoxicity/
High-risk Patients
OBrien M et al. Ann Oncol 2004; 15: 440-449
PLD Conventional
doxorubicin
HR
(95% CI)
Age 65 years 0 13.6% -
Cardiac risk factors 4.3% 21% 2.7(1.017.18)
Prior adjuvant
anthracycline
2.7% 38% 7.27
(0.9356.8)
-
8/10/2019 PLD in Metastatic Breast Cancer
9/36V1.0
Non-hematologic Toxicities
OBrien M et al. Ann Oncol 2004; 15: 440-449
PLD (n=254) Conventional doxorubicin (n=255)
All Grade 3-4 All Grade 3-4
Nausea 37% 3% 53% 5%
Alopecia 20% - 66% -
Vomiting 19%
-
8/10/2019 PLD in Metastatic Breast Cancer
10/36V1.0
Hematologic Toxicities
OBrien M et al. Ann Oncol 2004; 15: 440-449
PLD
(n=254)
Conventional
doxorubicin
(n=255)
All Grade 3-4 All Grade 3-4
Anemia 5% 1% 7% 2%
Leukopenia 2% 1% 11% 9%
Neutropenia 4% 2% 10% 8%
Thrombocytopenia 1% 0 1%
-
8/10/2019 PLD in Metastatic Breast Cancer
11/36V1.0
Conclusions
PLD and conventional doxorubicin have comparable
efficacy (OS, PFS, and response rates)
PLD treated patients had a significantly lower
incidence of cardiotoxicity EMA/FDA approved license of PLD in
metastatic breast
cancer based on these data
PLD treated patients had decreased alopecia,
myelosuppression, nausea, and vomiting, but morestomatitis,
hand-foot syndrome, and infusion
reactions
OBrien M et al. Ann Oncol 2004; 15: 440-449
-
8/10/2019 PLD in Metastatic Breast Cancer
12/36V1.0
Randomized Phase III Trial ofPegylated Liposomal Doxorubicin
(PLD) Versus Vinorelbine or
Mitomycin C Plus Vinblastine inWomen With Taxane-Refractory
Advanced Breast Cancer
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
13/36V1.0
Study Design
Pegylated Liposomal
Doxorubicin (PLD) 50 mg/m2
IV over 1 hour Q4W
(n = 150)
Vinorelbine 30 mg/m2
(n = 129)
or
Mitomycin C 10 mg/m2
Vinblastine 5 mg/m2
(n = 22)
Progression-Free SurvivalPrimary endpoint:
Taxane-refractory,
MBC with normal
cardiac function
< 2 prior
chemotherapies,excluding adjuvant
therapy
Prior adjuvant
anthracycline
permitted 450 mg/m2
N = 301
T
R
E
A
T
T
O
P
R
O
G
R
E
S
SI
O
N
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
14/36V1.0
Baseline Demographics
PLD (n=150) Comparator (n=151)
Median age (years) 56 (3387) 56 (3083)
Karnofsky performance score
60-70 19% 17%
>70 81% 83%
Menopausal status at diagnosis
Premenopausal 40% 35%
Perimenopausal 6% 8%
Post menopausal 54% 56%
Unknown 0
-
8/10/2019 PLD in Metastatic Breast Cancer
15/36V1.0
Response Rates
PLD (n=115) Comparator (n=117)
ORR (CR+PR) 10% 12%
CR 2% 2%
PR 8% 10%
SD 28% 28%
PD 32% 32%
Median DOR 5.7 months 6.0 months
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
16/36V1.0
PFS
Keller et al. J Clin Oncol 2004; 22: 3893-3901
PFS was similar for PLD vs. comparator (2.9 months vs.2.5
months; P=0.11)
-
8/10/2019 PLD in Metastatic Breast Cancer
17/36V1.0
OS
OS was comparable for PLD vs. comparatorAll randomised patients
- median OS, 10.4 months vs. 9.0
months (HR 1.07; 95% CI, 0.79 to 1.45; P=0.57).
Protocol-eligible patients - median OS was consistent with
the results of the analysis for the entire study population
(HR0.94; 95% CI, 0.68 to 1.33)
Updated survival analysis (October 2001) was
consistent with the original analysis
All randomized patients - median OS 11.0 vs. 9.0 months (HR1.05;
95% CI, 0.82 to 1.33; P=0.71)
Protocol-eligible patients - median OS 11.0 vs. 9.7 months
(HR 1.01; 95% CI, 0.77 to 1.33; P=0.93)
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
18/36
-
8/10/2019 PLD in Metastatic Breast Cancer
19/36V1.0
Overall Survival
PLD Comparator HR
(95% CI)
Prior Anthracycline Exposure
Any (n) 9.2 months
(92)
9.5 months
(96)
0.86
(0.58-1.26)
None (n) 10.4 months
(23)
10.4 months
(21)
1.51
(0.65-3.52)
Anthracycline Resistant (progression on or within 6 months)
Yes (n) 8 months(46)
6.1 months(34)
1.05(0.61-1.83)
No (n) 11.2 months
(69)
10.4 months
(80)
1.03
(0.65-1.60)
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
20/36V1.0
Selected AEs of Interest
PLD (n=150) Vinorelbine
(n=129)
Mitomycin C +
Vinblastine (n=22)
All Grade 3-4 All Grade 3-4 All Grade 3-4
Nausea 31% 3% 27% 7% 23% 5%
Fatigue 20% 4% 21% 2% 9% 5%
HFS 37% 19% 0.8% 0 0 0
Vomiting 20% 4% 17% 3% 18% 0
Asthenia 9% 1% 15% 4% 32% 0
Stomatitis 22% 5% 4% 0 0 0Neutropenia 3% 2% 14% 8% 5% 0
Mucositis NOS 14% 3% 0.8% 0 5% 0
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
21/36V1.0
Conclusions
PLD has comparable efficacy to standard salvage
regimens used in taxane-refractory patientsActivity seen with
PLD in anthracycline- and taxane-refractory
patients
PLD treated patients experienced more HFS and
stomatitis
Comparator-treated patients experienced more
neuropathy, constipation and neutropenia
PLD is a useful regimen in women with heavily pre-
treated, taxane-refractory advanced breast cancer
Keller et al. J Clin Oncol 2004; 22: 3893-3901
-
8/10/2019 PLD in Metastatic Breast Cancer
22/36V1.0
A randomized phase III studyevaluating pegylated liposomal
doxorubicin (PLD) versus capecitabine
as first-line therapy for metastaticbreast cancer (MBC): Results
of the
PELICAN study
Jger E et al. J Clin Oncol 2010; 28(15s): Abstract 1022
-
8/10/2019 PLD in Metastatic Breast Cancer
23/36
V1.0
Capecitabine
1,250 mg/m2BID x 14 days
Q21D
Pegylated Liposomal
Doxorubicin (PLD) 50 mg/m2
Q28D
Study Design
Time to disease progression (TTP)Primary endpoint:
Metastatic breast
cancer patients
N = 210
(randomized 1:1)
Stratified by age
and prior adjuvant
anthracycline
therapy
D
i
s
e
a
s
e
P
r
o
g
r
e
ss
i
o
n
Jger E et al. J Clin Oncol 2010; 28(15s): Abstract 1022.
-
8/10/2019 PLD in Metastatic Breast Cancer
24/36
V1.0
Efficacy Results
Prior adjuvant anthracycline treatment had a negative impact on
TTP
in the capecitabine group (4.8 months vs. 9.0 months
(p=0.0098)
PLD
(n=105)
Capecitabine
(n=105)
Median number of cycles 5 5
Median TTP 6.7 months 7.1 months
Prior anthracycline therapy 5.9 months 4.8 months
No prior anthracycline therapy 6.9 months 9.0 months
1-year overall survival 82% 75%
Overall response rate 24% 26%
Jger E et al. J Clin Oncol 2010; 28(15s): Abstract 1022.
-
8/10/2019 PLD in Metastatic Breast Cancer
25/36
V1.0
Adverse Events
PLD
(n=105)
Capecitabine
(n=105)
P Value
Diarrhoea (grade 3/4) 0 12% 0.0002
Thromboembolic events
(grade 3/4) 2% 10% 0.033
Hand-foot syndrome 36% 25% 0.1352
Cardiac events 9% 12% 0.4999
Jger E et al. J Clin Oncol 2010; 28(15s): Abstract 1022.
-
8/10/2019 PLD in Metastatic Breast Cancer
26/36
V1.0
Conclusions
PLD and capecitabine demonstrated similar
effectiveness with regard to TTP
PLD arm showed a better tolerability profile
compared to capecitabine
Jger E et al. J Clin Oncol 2010; 28(15s): Abstract 1022.
-
8/10/2019 PLD in Metastatic Breast Cancer
27/36
-
8/10/2019 PLD in Metastatic Breast Cancer
28/36
V1.0
Pegylated Liposomal
Doxorubicin (PLD) 50 mg/m2every 4 weeks
Study Design
Clinical benefit of PLD (CR+PR+SD 6 months duration)Primary
endpoint:
Metastatic breast
cancer patients
At least one prior
chemotherapy formetastatic disease
Previously treated
with anthracyclines
N = 79
Di
s
e
a
s
e
P
r
o
g
r
e
s
si
o
n
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
All patients received vitamin B6 (Pyridoxine) 300 mg orally once
daily to prevent PPE
-
8/10/2019 PLD in Metastatic Breast Cancer
29/36
V1.0
Patient Demographics
* n=3 by histochemistry or amplification by FISH
PLD (n=79)
Median age (years) 58
Karnofsky performance score
100 22.7%
90 34.1%
80 43.2%
Number of metastastic sites
1 32.9%
2 31.6%
3 35.4%
ER+ and PgR+ 86%
HER2+ 5.1%*
Site of disease
Bone only 6.3%
Non-visceral soft tissue only 11.1%
Visceral 82.6%
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
30/36
V1.0
Treatment History
PLD (n=79)
Previous chemotherapy for MBC
1 regimen 37.9%
2 regimens 29.1%
3regimens 32.9%Prior anthracycline-base therapy 100%
Adjuvant only 22.8%
Metastatic only 68.4%
Both settings 8.9%
Anthracycline free interval
0-12 months 41.8%
>12 months 58.2%
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
31/36
V1.0
PLD (n=79)
ORR (CR+PR) 12.7%
CR 1.3%
PR 11.4%
SD 27.8%
Median DOR 12 months
Median PFS 3.6 months
Stable disease (any) 9.5 months
Anthracycline resistant 2.8 months
Non-anthracycline resistant 3.7 monthsMedian OS 12.3 months
Anthracycline resistant 9.0 months
Non-anthracycline resistant 12.5 months
Efficacy Results
Anthracycline resistant defined as having disease progression on
anthracycline-
based therapy for MBC or within 6 months of adjuvant
anthracycline-based therapyAl-Batran S et al. Br J Cancer 2006;
94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
32/36
V1.0
OS and PFS
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
33/36
V1.0
Efficacy Results
Clinical Benefit 6 Months
All patients (N=79) 24%
1 regimen (n=30) 30%
2 regimens (n=23) 21.7%
3 regimens (n=26) 19.2%
Prior chemotherapy
Anthracycline resistant (n=31) 16.1%
Non-anthracycline resistant (n=48) 29.1%
Anthracycline Free Interval0-12 months (n=29) 24.1%
>12 months (n=32) 25%
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
34/36
V1.0
Safety Results
*20 Grade 1,22 grade 2; most events were considered not related
to PLD but to prior therapies by the investigator
Non-Hematological (n=79) All Grades Grade 1-2 Grade 3-4
Alopecia 53.8% 53.8%* 0
Nausea 47.4% 42.3% 5.1%
Diarrhoea 15.3% 15.3% 0
Vomiting 34.6% 32.0% 2.5%
Constipation 34.6% 30.7% 3.8%
Fever 19.2% 19.2% 0
Infection 28.2% 20.5% 7.6%
Neuropathy 32.0% 29.4% 2.5%
Hand-foot syndrome 46.1% 39.7% 6.4%
Mucositis 43.5% 33.3% 10.2%
Haematological (n=76) All Grades Grade 1-2 Grade 3-4
Neutropenia 50.0% 32.8% 17.1%
Leukopenia 72.3% 57.8% 14.4%
Anemia 88.1% 78.9% 9.2%
Thrombocytopenia 34.2% 30.2% 3.9%
Al-Batran S et al. Br J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
35/36
V1.0
Conclusions
Overall clinical benefit rate was 24% 16.1% in patients with
anthracycline resistance vs. 29% in
patients classified as having non-anthracycline-resistant
disease
Median PFS and OS were 3.6 and 12.3 months,respectively
PLD was generally well tolerated
No cardiac toxicities were seen and no significant
changes in electrocardiograms or echocardiograms
were observed during the study
PLD was associated with an clinical benefit in
anthracycline pre-treated patients with MBCAl-Batran S et al. Br
J Cancer 2006; 94(11): 1615-1620
-
8/10/2019 PLD in Metastatic Breast Cancer
36/36
PLD in MBC - Conclusion
PLD and conventional doxorubicin have similar
efficacy, however PLD has: significantly lower risk of cardiac
toxicity
improved convenience
differing tolerability profiles (less alopecia, nausea and
vomiting, myelosuppression but more HFS and stomatitis)
In general, no overlapping toxicity so readily able to
combine with other agents such as taxanes and
gemcitabine