Embed Size (px)
Citation preview

Eur. J. Clin. Pharmacol. 16, 149-153 (1979) European Journal of Clinical Pharmacology © by Springer-Verlag 1979
Long-Term Hemodynamic Effects of Penbutolol at Rest and During Exercise in Essential Hypertension
P. Lund-Johansen
Medical Department A, University of Bergen School of Medicine, Bergen, Norway
Summary. Thirteen men with previously untreated essential hypertension (WHO Stage I) were studied as out-patients. Oxygen consumption, heart rate, car- diac index and brachial arterial pressure were recorded at rest supine and whilst sitting position, and during steady state exercise at 50, 100 and 150 W. The subjects were then treated with penbutolol 20-80 mg/day. In 12 responding patients hemody- namic study after 1 year demonstrated that systolic, diastolic and mean arterial pressure were reduced by approximately 20% at rest and 18% during exercise. Heart rate was reduced about 24% at rest and 26% during exercise. The stroke index did not show any significant change during rest, but during exercise the post-treatment values were 8%, 13% and 18% higher than the pre-treatment values at the 50, 100 and 150 W exercise levels, the last two changes being significant. Thus, the reduction in cardiac index dur- ing exercise was less than the reduction in heart rate - about 15%, but 24% when sitting at rest. The total peripheral resistance index did not show any signifi- cant change at rest or during exercise. Dizziness or muscular fatigue occurred in 6 patients during the first two weeks of treatment. From then on no side- effects were noted. It is concluded that the hemody- namic effects of longterm treatment with penbutolol in mild to moderate hypertension largely resemble those after the majority of other beta-blockers.
Key words: beta-adrenergic blockade, penbutolol, haemodynamics; hypertension, prolonged treatment
Penbutolol is a relatively new, non-cardioselective beta-blocker without intrinsic sympathicomimetic activity [4]. Clinical studies have shown that the drug
reduces blood pressure in patients with hypertension [2, 3, 14]. No information is available about the long- term hemodynamic effects of this compound, either at rest and during exercise. The present work is a study of central hemodynamics at rest and during exercise in a relatively homogenous group of males with previously untreated essential hypertension, examined before and after one year of penbutolol therapy.
Material and Methods
The series comprised 13 males, aged 23-55 years (mean 42.6 years). All subjects had previously un- treated essential hypertension of WHO Stage I. Sec- ondary hypertension was excluded by conventional routine procedures. All patients were without symp- toms, the hypertension being discovered at routine health examination by a health officer or general practitioner, and confirmed by several visits to the out-patient clinic of Medical Department A, Hauke- land Hospital. The mean SD of body weight and body surface area before treatment were 75.6 + 9.6 kg and 1.92 _+ 0.14 m 2. After one year on therapy there was no significant change in body weight.
Methods
The subjects underwent hemodynamic study during strictly standardized conditions at rest supine and sit- ting, and when bicycling at steady state at 50, 100 and 150 W. Oxygen consumption (VO2), intra-arte- rial pressure (brachial artery), heart rate (HR) and cardiac output (CO; dye dilution, Cardiogreen) were measured in duplicate on each occasion. At rest VO 2 was measured only in the sitting position. The methods have previously been described in detail [5].
0031-6970/79/0016/0149/$01.00

150 P. Lund-Johansen: Hemodynamic Effects of Penbutolol
Table 1. Oxygen consumption (VO2), cardiac index (CI), stroke index (SI), heart rate (HR), systolic (SAP), diastolic (DA) and mean arterial pressure (MAP), and total peripheral resistance index (TPRI) before penbutotol therapy (1) and after one year of treatment (2). p = p value of paired sample test (n = 12)
Rest Work (W/min)
Supine Sitting 50 t00 150
1 2 1 2 1 2 1 2 1 2
VO 2 (ml rain -1 m -2) Mean SD P
CI (1 min -1 m -2) Mean SD P
SI (rnl stroke -1 m -2) Mean SD P
HR (beats min -1) Mean SD P
SAP (mmHg) Mean SD P
DAP (mmHg) Mean SD P
MAP (mm~g) Mean SD P
TPRI (dyn s -1 crn -5 m 2) Mean SD P
149 147 617 589 916 820 1300 1252 23 28 57 73 92 101 181 174
NS NS <0.05 NS
3.69 2.97 2.89 2.19 5.97 4.90 7.14 6.10 8.27 7.10 0.94 0.28 0.63 0,45 1.23 0.43 1.14 0.65 0.9 0.94
<0.05 <0.01 <0.01 <0.05 <0.01
49.4 52.2 37.4 36.2 51.9 56.1 51.7 58.6 51.8 60.0 7.6 6.3 8.0 4.7 9.0 3.0 7.1 5.0 9.1 9.6
NS NS NS <0.05 <0.01
74.8 57.7 78.9 59.9 116.3 87.5 139.8 104.3 164.4 119.1 14.0 6.6 15.2 8.3 21.5 8.5 23.0 10.1 19.6 9.9
<0.001 <0.001 <0.001 <0,001 <0.001
151.4 127.8 164.1 131.5 189.3 150.8 194.1 158.6 209.1 175.0 13.7 14.1 It .1 12.4 18.1 11.3 19.2 12.9 22.9 13.2
<0.001 <0.001 <0.001 <0.001 <0.001
93.8 74.7 105.3 83.8 107.6 86.8 108.9 88.8 114.0 95.9 10.1 8.7 9.7 9.0 16.2 6.8 18.7 9.3 17.5 11.8
<0.001 <0,001 <0.001 <0.001 <0.001
116.8 96.5 1.28.0 103.1 143.1 113.8 142.3 118.8 152.2 128.8 10.5 9.5 10.8 11.7 18.8 9.3 17.0 10.4 20.7 13.5
<0.001 <0.001 <0.001 <0.001 <0.001
2669 2606 3678 3888 1980 1865 1620 1573 1494 1472 640 283 718 661 408 139 239 201 291 261
NS NS NS NS NS
The subjects were in formed abou t the na ture and purpose of the s tudy and consent was obta ined f rom each of them.
The studies were m a d e on an out -pa t ien t basis. Af t e r a t r ea tment per iod of 1 1 - 1 2 mon ths the h e m o d y n a m i c s tudy was repeated. T he difference be tween the h e m o d y n a m i c results at the first and sec- ond study was tes ted by Student ' s t-test.
Treatment
The patients received penbutolo l as capsules, starting with 20 mg, at 7.00 a.m. T he aim of t rea tment was to p roduce a fall in casual b lood pressure to 140/ 90 m m H g or less wi thout side-effects. T w o pat ients had a marked b lood pressure decrease on 20 mg once daily and cont inued on this dose. In the remaining patients the dose was gradual ly increased to 40 mg
(4 patients) , 6 0 r a g (6 patients) and 8 0 m g (one patient). The pat ient receiving 80 mg did not r espond satisfactorily and hydrochloro th iaz ide was added to the reg imen after two mon ths with sat isfactory result. This subject (patient no. 13) has b e e n omi t t ed f r o m the statistical analyses. In the o the r 12 pat ients no o ther drugs or any diet any restriction was employed. O n the day of the second h e m o d y n a m i c study, the pat ient t ook the morn ing dose at 7 ,00 a.m. and the h e m o d y n a m i c s tudy was pe r fo rmed be tween 9.00 and 12.00 a.m.
Side- Effects
T w o pat ients compla ined of dizziness and 4 of mus- cular fatigue dur ing the first 2 weeks of t reatment . The muscular fat igue was most marked during sud- den and severe exercise, and was no t ed in pat ients
P. Lund-Johansen: Hemodynamic Effects of Penbutolol
- - Before CI I mm -~ m "2 . . . . . . After
10
i ~ 100 MAP mrnHg 1 iPRI dyn se¢ c < 5 m 2
0 0 0 ~ . . . . , . . . . . . . .
500 1OOO 500 1000
SI ml stroke -1 m -2
60 ,.x . . . . . . . . x x . - o
5 0 ~ j s S
4 0
3 0
500 1OOO
5OO 10OO VO 2 ml miD -1 m "2
HR beats mln 4
150
1OO .x'"
o S
5 0
. , , , , i , , , , i i i ,
50O 1OOO MO 2 mr r n m -1 m - 2
HR - MAP beats/mln -1. mmHg 28.10:
o
1 0
4
50(3 10OO
151
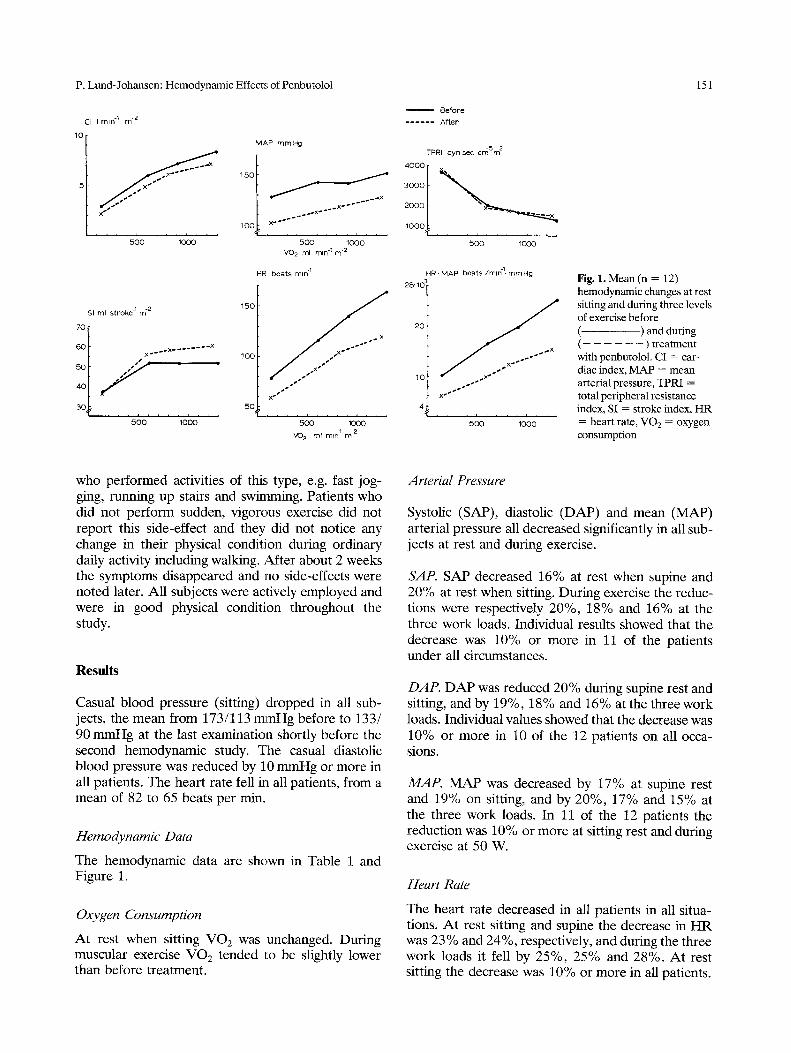
Fig. 1. Mean (n = 12) hemodynamic changes at rest sitting and during three levels of exercise before (- ) and during ( - ) treatment with penbutolol. CI = car- diac index, MAP = mean arterial pressure, TPRI = total peripheral resistance index, SI = stroke index, HR = heart rate, VO2 = oxygen consumption
who performed activities of this type, e.g. fast jog- ging, running up stairs and swimming. Patients who did not perform sudden, vigorous exercise did not report this side-effect and they did not notice any change in their physical condition during ordinary daily activity including walking. After about 2 weeks the symptoms disappeared and no side-effects were noted later. All subjects were actively employed and were in good physical condition throughout the study.
R e s u l t s
Casual blood pressure (sitting) dropped in all sub- jects, the mean from 173/113 mmHg before to 133/ 90 mmHg at the last examination shortly before the second hemodynamic study. The casual diastolic blood pressure was reduced by 10 mmHg or more in all patients. The heart rate fell in all patients, from a mean of 82 to 65 beats per min.
Hemodynamic Data
The hemodynamic data are shown in Table 1 and Figure 1.
Oxygen Consumption
At rest when sitting g o 2 w a s unchanged. During muscular exercise g o 2 tended 1:o be slightly lower than before treatment.
Arterial Pressure
Systolic (SAP), diastolic (DAP) and mean (MAP) arterial pressure all decreased significantly in all sub- jects at rest and during exercise.
SAP. SAP decreased 16% at rest when supine and 20% at rest when sitting. During exercise the reduc- tions were respectively 20%, 18% and 16% at the three work loads. Individual results showed that the decrease was 10% or more in 11 of the patients under all circumstances.
DAP. DAP was reduced 20% during supine rest and sitting, and by 19%, 18% and 16% at the three work loads. Individual values showed that the decrease was 10% or more in 10 of the 12 patients on all occa- sions.
MAP. MAP was decreased by 17% at supine rest and 19% on sitting, and by 20%, 17% and 15% at the three work loads. In 11 of the 12 patients the reduction was 10% or more at sitting rest and during exercise at 50 W.
Heart Rate
The heart rate decreased in all patients in all situa- tions. At rest sitting and supine the decrease in H R was 23% and 24%, respectively, and during the three work loads it fell by 25%, 25% and 28%. At rest sitting the decrease was 10% or more in all patients.

152 P. Lund-Johansen: Hemodynamic Effects of Penbutolot
The decrease was 15% or more in 10 of the when 12 sitting at rest and in 11 of the 12 during muscular exercise. Two patients had H R below 50 at rest supine (48 and 47), at rest sitting all had H R of 50 beats per min or more. During exercise at 150 W the H R averaged 45 beats per minute less than priore to treatment.
Stroke Index
At rest there was no significant change in stroke index (SI), a slight increase of 6% in the supine posi- tion and a small decrease of 3% in the sitting posi- tion. During exercise the post-treatment values were 8%, 13% and 17% higher than the pretreatment val- ues, the last two changes being significant. At rest supine and during exercise 6 patients demonstrated an increase in stroke volume of 10% or more.
Cardiac Index
With a few exceptions the post-treatment cardiac index (CI) was lower than the pretreatment value. The CI was 20% lower during supine rest and 24% on sitting at rest both changes being significant. Dur- ing exercise the reductions were 18%, 15 and 14%, respectively, all changes being significant. At rest sit- ting the CI was decreased 10% or more in 9 of 12 patients. Due to the compensatory increase in SI, the CI during exercise was reduced less than the HR.
Total Peripheral Resistance Index
Before treatment the total peripheral resistance index (TPRI) was increased in all but one patient at rest. During exercise the TPRI increased in all of them. The results after one year showed that there were only small changes in TPRI and none of the changes were significant. Four patients, however, demonstrated at least a 10% decrease in TPRI at rest sitting and during two of the work loads.
Discussion
ence of 62 similar patients, who participated in analogous studies of other beta-blockers [6-10].
The heart rate was reduced dramatically, and from the reduction in heart rate at rest and particu- larly during exercise it should be anticipated that beta-blockade was maximal in the patients at the time of the second hemodynamic study. As com- monly seen during use of other beta-blockers, there was considerable variation in the individual dose required to achieve a satisfactory reduction in blood pressure.
The decrease in blood pressure was associated with a reduction in cardiac index. Due to a compen- satory increase in stroke volume during exercise, par- ticularly at the two highest work levels, the reduction in cardiac index in those situations was less than at rest. Since oxygen consumption during exercise was almost unchanged, there was an increase in the arteriovenous oxygen difference, as is also commonly seen on use of other beta-blockers [6-10].
The total peripheral resistance did not decrease significantly de spite the marked decrease in blood pressure. Although there have been a few reports claiming significant reduction in total peripheral resistance during long-term treatment with a few beta-blockers, e.g. pindolol [1] and bunitrolol [12], we have not seen this response in groups of patients with mild hypertension treated with alprenolol [6], atenolol [8], metoprolol [9], timolol [7] or bunitrolol [10]. Only in 4 patients in the penbutolol group did the TPRI fall by 10% or more at rest and during two levels of exercise. None of these patients had any particular characteristics of pretreatment blood pressure or resistance.
It has been suggested that prolongation of beta- blocker therapy for a period longer than one year might cause a reduction in total peripheral resistance through some sort of readjustment response to the decrease in blood pressure [ 13]. However, in patients treated with alprenolol or atenolol and restudied after 1, 3 and 5 years, we were unable to find any support for this theory. The hemodynamic results after 3 and 5 years were not significantly different from those after 1 year [11].
From a clinical point of view, penbutolol induced a satisfactory reduction in blood pressure in 12 of the 13 patients studied. Patient 13 had an initial casual blood pressure of 195/110 mmHg and he had to be treated with hydrochlorothiazide after two months, when his blood pressure fell to 135/95 mmHg.
Apart from complaints of dizziness and muscular fatigue during the first weeks of treatment, no other side-effects were seen in this small patient group (all in WHO Stage I). This is accordance with our experi-
References
1. Atterh6g, J.-H., Dun6r, H., Pernow,B.: Haemodynamic effects of pindolol in hypertensive patients. Acta Med. Scand., Suppl. 606, 55 (1977)
2. Frick, M.H., Hartikainen, M., PSrsti, P.: Penbutolol, a new non-selective beta-adrenergic blocking compound in the treat- ment of hypertension. A comparison with propranotot. Ann. Clin. Res. 10, 105 (1978)
3. Hansson, B.-G., H6kfelt, B.: Long term treatment of moder- ate hypertension with penbutolol (Hoe 893 d). I. Effects on

P. Lund-Johansen: Hemodynamic Effects of Penbutolol 153
blood pressure, pulse rate, catecholamines in blood and urine, plasma renin activity and urinary aldosterone under basal con- ditions and following exercise. Eur. J Clin. Pharmacol. 9, 9 (1975)
4. H/irtfelder, G., Lessenich, H., Schmitt, K.: Penbutolol (Hoe 893d), ein neues, stark wirksames Beta-Sympathicolyticum mit langer Wirkungsdauer. Arzneim. Forsch. (Drug Res.) 22, 930 (1972)
5. Lund-Johansen, P.: Hemodynamics in early essential hyper- tension. Acta. Med. Scand. Suppl. 482, 1 (1967)
6. Lund-Johansen, P.: Hemodynamic changes at rest and during exercise in long-term beta-blocker therapy of essential hyper- tension. Acta. Med. Scand. 195, 117 (1974)
7. Lund-Johansen, P.: Hemodynamic long-term effects of timolol at rest and during exercise in essential hypertension. Acta Med. Scand. 199, 263 (1976)
8. Lund-Johansen, P.: Hemodynamic long-term effects of a new beta-adrenoceptor blocking drug, ate.nolol (ICI 66082), in essential hypertension. Br. J. Clin. Pharmacol. 3, 445 (1976)
9. Lund-Johansen, P., Ohm, O.-J.: Haemodynamic long-term effects of metoprolol at rest and during exercise in essential hypertension. Br. J. Clin. Pharmacol. 4, 147 (1977)
10. Lund-Johansen, P.: Long-term hemodynamic effects of buni- trolol at rest and during exercise in essential hypertension. J. Cardiovasc. Pharmacol. 1, 77 (1979)
1 i. Lund-Johansen, P.: Hemodynamic consequences of long-term beta-blocker therapy. A 5 year follow up study of atenolol. J. Cardiovasc. Pharmacol. (in Press)
12. Reybrouck, T., Amery, A., Fagard, R., Billiet, L.: Haemody- namic response to graded exercise during chronic beta- adrenergic blockade with bunitrolol, an agent with intrinsic sympathomimetic activity. Eur. J. Clin. Pharmacol. 12, 333 (1977)
13. Tarazi, R.C., Dustan, H.P.: Beta-adrenergic blockade in hypertension. Practical and theoretical implications of long- term hemodynamic variations. Am. J. Cardiol. 29, 633 (1973)
14. Yajnik, V.H., Nandi, J.S., Patel, S.C., Patel, S.H.: Pen- butolol in hypertension: a pilot study with single daily doses. J. Int. Med. Res. 5, 236 (1977)
Received: March 14, 1979 accepted in revised form: May 31, 1979
Prof. Dr. P. Lund-Johansen Medical Department A 5016 Haukeland Hospital Bergen, Norway











![Instructions for use - 北海道大学 · Chronological Change in Pulmonary Vascular Response to Hypoxia in Hepatopulmonary Syndrome ... hypertension [9]. The hemodynamic features](https://img.dokumen.tips/doc/110x75/5e1e414662e9cf6a9e7ba9d3/instructions-for-use-oee-chronological-change-in-pulmonary-vascular.jpg)

















