Embed Size (px)
Citation preview

Case Report
Ligneous Periodontitis and Ehlers-Danlos Syndrome
Viviane S.S. Pierro,* Ramon Vazquez-Sullca,† Aurea Simone Barroso Vieira,*Christina Maeda Takiya,‡ Gerson Carakushansky,§ and Eduardo J. Feres-Filho†
Background: Generalized membranous gingivalenlargement due to an accumulation of fibrin depositsassociated with severe alveolar bone loss (ligneousperiodontitis) is a rare condition, and plasminogende-ficiency seems to play a central role in its pathogene-sis. However, this condition has not been described inassociationwith syndromes. This article reports a caseof ligneous periodontitis in a boywith the classic typeof Ehlers-Danlos syndrome (EDS).
Methods: A 12-year-old white male presented withgeneralized gingival overgrowth and severe alveolarbone loss. A physical examination revealed clinicalsigns of EDS (velvety skin with mild hyperextensibil-ity, marked hypermobility of the limb joints, atrophicscars on his knees, and easybruising),which is associ-atedwith a positive family history for joint hypermobil-ity. A biopsy of gingival tissues was submitted forroutine histology, hematoxylin and eosin (H&E), anddirect immunofluorescence (antifibrinogen). An evalu-ation of plasminogen activity was also performed.
Results: Histopathology revealed chronic periodon-titis with fibrinoid material deposition, and direct im-munofluorescence proved to be positive for fibrin.Functional plasminogenwas reduced. A conclusive di-agnosis of ligneous periodontitis due to plasminogendeficiency associated with the classic type of EDSwas rendered.
Conclusions: Ehlers-Danlos syndrome can be asso-ciated with ligneous periodontitis. In the present case,the histologic examination represented an importanttool in the differential diagnosis, because it ruled outEDS type VIII as the associated systemic factor to peri-odontal breakdown. J Periodontol 2006;77:123-128.
KEY WORDS
Child; deficiency; Ehlers-Danlos syndrome; gingivalovergrowth; periodontitis; plasminogen.
The term ligneous periodontitis was first used byGunhan et al.1 to describe a destructive mem-branous periodontal disease characterized by
gingival enlargement and periodontal tissue destruc-tion due to the accumulation of amyloid-like material.Most of the pseudomembranous gingival lesions havebeen reported in association with ligneous conjuncti-vitis.1-10 Therefore, these findings suggest that bothclinical manifestations are related.11
Ligneous conjunctivitis is a rare form of chronicconjunctivitis that usually affects children, girls moreoften than boys (gender ratio of 3:1), but may occur atany age.11,12 This condition appears to be the ocularmanifestation of a systemic disease that might be ac-companied by formation of pseudomembranes on themucosa of the mouth (ligneous gingivitis or periodon-titis),1-10 the female genital tract (ligneous vulvovag-initis or cervicitis),3,13,14 the laryngotracheobronchialtree,3,14-17 the middle ear,14,17 and the mastoid sys-tem.17 Pseudomembranous inflammation simulta-neously involving the female genital tract, middleear, and oral mucosa, with no signs of ligneous con-junctivitis,18 also has been reported, as well as somecases in which pseudomembranes were present onlyin the gingival tissue.6-8,19
It has been suggested that ligneous conjunctivitismight be an autosomal recessive disorder.20 Its cen-tral feature is an impaired wound-healing capacitywith an arrest at the stage of granulation tissue forma-tion and excessive fibrin deposition.11 The prominentfibrinous component observed in histologic ex-aminations of eye lesions has also been reportedas the most notable histologic feature of affectedtissues from other mucosal sites.1,3,4,6-8,13,17-19
These descriptive findings have been related to amajor deficiency of (plasmin-mediated) extracellularfibrinolysis.11
The report of a case in which pseudomembranouslesions arose as a side effect of tranexamic acid, anantifibrinolytic drug used in the treatment of menor-rhagia, linked plasminogen deficiency to the patho-genesis of ligneous conjunctivitis and ligneousperiodontitis.4 After this report, many studies foundthat pseudomembranous lesions (regardless oftheir location) were indeed caused by plasminogen
* Department of Pediatric Dentistry and Orthodontics, School of Dentistry,Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
† Graduate Periodontics, School of Dentistry, Federal University of Riode Janeiro.
‡ Department of Histology and Embriology, Institute of Biomedical Sciences,Federal University of Rio de Janeiro.
§ Department of Pediatrics (Genetic Service), School of Medicine,Federal University of Rio de Janeiro.
J Periodontol • January 2006
123
deficiency.8-10,14-16,18,19,21-23 This condition is con-sidered rare, with a prevalence of about 0.4% in thegeneral population.24 The severity of the disease ap-pears to be inversely related to the level of functionalplasminogen activity.10 Gingival lesions due to plas-minogen deficiency may be progressive and resultin tooth loss despite treatment attempts with subgin-gival curettage, gingivectomy, and antibiotics.1,6,7
Gingival enlargement with or without severe peri-odontitis has also been described in association withEhlers-Danlos syndrome (EDS),25,26 especially typeVIII.27-29 EDS is a heterogeneous group of heritableconnective tissue disorders, characterized by articularhypermobility, skin hyperextensibility, and tissue fra-gility.30 The pattern of inheritance and the clinicalmanifestations vary with the type of EDS being exam-ined.31 The prevalence of EDS has been estimated tobe about one in 5,000 births,32 and diagnosis is basedprimarily on clinical findings.30
This case report describes a case of ligneous peri-odontitis in a boy with the classic type of Ehlers-Danlos syndrome.
CASE REPORT
A 12-year-old male of Italian descent presented to thepediatric dental clinic for special-needs patients atthe Federal University of Rio de Janeiro, Brazil, witha history of gingival overgrowth since the eruptionof primary molars. Previous medical history includeda 5-day hospital stay caused by a severe urinaryinfection episode at 2 weeks old, and a longer hospitalstay (15 days) as a result of an episode of acuteasthma at 2 years old. His parents also reported a de-lay in speech and walking that was associated withgeneralized muscle hypotonia. For this reason, thepatient had been taking speech therapy and physio-therapy sessions since he was 2 years old. Physiother-apy sessions were interrupted when he turned 6because the therapist noticed an uncommon hyper-mobility of his hip joint. On presentation, he wasotherwise healthy, and medications included dailymethylphenidatek prescribed by his neurologist forthe treatment of attention deficit disorder (ADD).
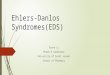
Intraoral examination revealed a permanentdentition presenting generalized gross plaque accu-mulation and a painless, massive, nodular fragilegingival enlargement involving both maxilla and man-dible. The enlargements were covered with white–yellowish membranes, with a tendency to bleed (Figs.1A and 1B). A panoramic radiograph revealed exten-sive bone loss (Fig. 2), and bitewings confirmed theabsence of carious lesions. The buccal aspect of gin-gival tissues from the left mandibular side was biop-sied. Half of the specimen was processed for lightmicroscopy, while the other half was frozen and pro-cessed for direct immunofluorescence using antibody
against fibrinogen conjugated with FITC¶ as describedelsewhere.33
Despite a negative family history for gingival over-growth, there was a positive history for joint hypermo-bility (the child’s uncle). For this reason, the patientwas referred to a geneticist. On referral, he presentedsmooth, velvety skin with mild hyperextensibility,marked hypermobility of the limb joints (e.g., thewrists and fingers), atrophic scars (having papy-raceous appearance) on his knees, and a positive his-tory for spontaneous ecchymoses (easy bruising)(Figs. 3A and 3B). Therefore, based on the patient’smedical and family histories, combined with clinicalfindings (especially his severe gingival overgrowthand aggressive periodontitis), his profile was consis-tent with Ehlers-Danlos syndrome type VIII.
Reevaluation of the biopsied site showed rapidregrowth of the excised tissue, and a histologic ex-amination revealed areas of ulceration, granulationtissue, subepithelial inflammatory infiltration, and
Figure 1.A) Extensive gingival overgrowth covered with white–yellowishmembranes (frontal view). B) Lateral view.
k Ritalina, Novartis Biociencias S/A, Sao Paulo, Brazil.¶ Dako, Carpinteria, CA.
Ehlers-Danlos Syndrome and Periodontitis Volume 77 • Number 1
124

amorphous nodular deposits of a homogeneous,eosinophilic substance beneath the gingival squa-mous epithelium (Fig. 4A). The microscopic diagno-sis was chronic hyperplasic gingivitis with ulcerationand fibrinoid deposits. Congo red staining for amy-loidosis was negative. Periodic acid-Schiff reactionand Sudan black staining proved to be negative aswell, thereby excluding the possibilities of infantilesystemic hyalinosis and lipid proteinosis, respec-tively. Direct immunofluorescence of the gingivalspecimen showed a positive staining for fibrinogen(Fig. 4B). Therefore, a recommendation was madeto evaluate plasminogen activity, and the functionalplasminogen and plasminogen antigen assays wererequested. The patient presented a low functionalplasminogen level of 13% (reference range, 70% to143%). His parents were asked about similar pseudo-membranous lesions in the patient’s conjunctivae.They reported that the lesions appeared when thepatient was about 6 months old, and that they weretreated by the age of 4 with a rigorous cleaning of sa-line solution, topical antibiotics, and corticosteroids.Since then, the parents continue to clean the child’sconjunctivae every day to control the growth of pseu-domembranes. Recently, an ophthalmologist con-firmed the absence of conjunctivae lesions. Despitea thorough otorhinolaryngological examination, noother membranes were found.
Upon physical examination, the clinical findings ledto a diagnosis of Ehlers-Danlos syndrome that couldnot be type VIII. According to Beighton et al.,30 the pa-tient presented with the classic type of Ehlers-Danlos(which include types I and II for their similarity) asso-ciated with ligneous periodontitis due to plasminogendeficiency.
The patient is being followed by a pedodontist,periodontist, ophthalmologist, otorhinolaryngologist,hematologist, psychologist, and speech therapist.The use of topical plasminogen to control the gingival
overgrowth during his teenage years is being dis-cussed with the hematologist. Exodontia of most per-manent teeth appears to be inevitable due toadvanced alveolar bone loss and poor prognosis ofthis ligneous disease. It is expected, however, thattopical plasminogen, together with periodontal ther-apy, can postpone it until adulthood.
DISCUSSION
The original classification of EDS was divided into 11phenotype subgroups.34 Since 1997, however, a pro-posed revised classification for EDS included the useof major and minor criteria to define six types: 1) clas-sic (I and II), 2) hypermobility (III), 3) vascular (IV), 4)kyphoscoliosis (VI), 5) arthrochalasia (VIIA and VIIB),and 6) dermatosparaxis (VIIC). Former types V, VIII,IX, X, and XI were classified as other forms becausethey were found to be rare.30 From these rare types,EDS type VIII is of special interest from a dental point
Figure 3.A) Hypermobility of the forefinger presenting dorsiflexion beyond 90�.B) Atrophic scar on the patient’s knee.
Figure 2.Panoramic radiograph showing generalized alveolar bone loss.
J Periodontol • January 2006 Pierro, Vazquez-Sullca, Vieira, Takiya, Carakushansky, Feres-Filho
125

of view because, except for the presence of aggres-sive periodontitis, this type is similar to the classictype.28,30 Because EDS types I, II, III, V, and VIII haveneither biochemical nor molecular markers, a diagno-sis must be based on patient symptoms and familyhistory alone.29 Therefore, tests to diagnose the pres-ent case were not performed.
Children or young adults presenting with gingivalinflammation and/or periodontal disease associatedwith a history of skin or joint symptoms (skin hyper-extensibility, fragility, and scarring; a tendency tobruise upon mild trauma; and small-joint hypermobil-ity) should be considered possible candidates for EDStype VIII.28 Such symptoms led us to tentatively diag-nose the present case with EDS type VIII, but the diag-nosis was ruled out after a histologic examinationobserved fibrin deposits, which are indicative of ligne-ous disease.
Although the histology is not pathognomonic, themost notable feature is the finding of a prominentfibrinous component to the pseudomembranous le-sions.22 This stromal accumulation of fibrin is dueto impaired fibrin degradation by plasmin, which isthe active enzyme responsible for fibrin degradationafter conversion of plasminogen (the inactive proen-zyme).35
Inherited plasminogen deficiency has been classi-fied into two types: hypoplasminogenemia (type I)and dysplasminogenemia (type II). In type I, boththe functional plasminogen level and plasminogenantigen are reduced, whereas in type II, only func-tional activity is reduced markedly.15 Interestingly,only hypoplasminogenemia (type I) has been re-ported to be associated with ligneous dis-ease.8,9,11,14-16,18,21,23 Because of this association,this case most likely presented plasminogen defi-ciency type I, whereas this could not be confirmed be-cause plasminogen antigen assay was not performed.It has been hypothesized that, in the case of dysplas-minogenemia, normal amounts of plasminogen anti-gen with decreased specific activity may be sufficientfor the process of normal wound healing.11
To date, the association of ligneous disease withplasminogen deficiency type I has been studied in11 patients presenting gingival lesions. In those pa-tients, plasminogen functional activities ranged from6% to 66%.8,9,18,19 Furthermore, certain homozygousor compound-heterozygous mutations in the plas-minogen gene have been identified in patients with hy-poplasminogenemia.9,14,15 It seems that the severityof clinical symptoms depends mainly on the amountof plasminogen functional residual activity. Indeed,patients who show undetectable plasminogen func-tional activity (<5%, where normal range is 70% to143%) usually exhibit severe multisystem disease.9,15
The patient described here presented a low, but notundetectable, plasminogen functional activity thatprobably prevented multisystemic disorder.
It is mainly the extravascular plasmin-mediatedfibrinolytic pathway that is impaired in affected sub-jects and that leads to deficient wound healing inmucous membranes. In predisposed children, evenminor trauma or local inflammation of mucous mem-branes (conjunctiva, trachea, mouth, nasopharynx,and female genital tract) may initiate the formationof ligneous pseudomembranes.9 The ligneous gingi-vitis presented in this case began at the time of theeruption of primary molars, and it seems that the in-flammatory process associated with the eruption ofthese larger teeth triggered the formation of gingivalpseudomembranes.
Once excised, these gingival pseudomembranespresent rapid regrowth and patients usually endup losing several teeth, if not all, at early ages.1,6
Figure 4.A) Histologic section of gingival biopsy showing acellular, eosinophilic,homogeneous, amorphous accumulation beneath the epithelium(H&E staining; bar = 100 mm). B) Subepithelial accumulation of fibrindepicted by direct immunofluorescence technique (bar = 20 mm).
Ehlers-Danlos Syndrome and Periodontitis Volume 77 • Number 1
126

Administration of topical plasminogen has showngood results for the treatment of ligneous conjunctivi-tis,10,16 whereas its efficacy for the treatment of orallesions remains to be elucidated. In the present case,the topical application of plasminogen is being con-sidered as a possible therapy to control pseudomem-brane growth, at least until adulthood, when a moreaggressive approach can be considered.
The association of ligneous disease with EDS hasnot been found in a review of the literature. Neverthe-less, an interesting case reported by Slootweg andBeemer in 198727 demonstrated that fibrinoid depos-its in the histologic examination of a 7-year-old girlwith recurrent recalcitrant hyperplastic gingivaltissue associated with alveolar bone loss who also pre-sented clinical findings compatible with EDS (skinhyperextensibility, joint hypermobility). At that time,histologic features of ligneous disease were not welldocumented, and the authors were uncertain whetherthe gingival fibrinoid deposits were a typical feature ofEDS type VIII. Therefore, based on clinical and histo-logic descriptions, it seems reasonable to speculatethat Slootweg and Beemer’s case could be consideredthe first evidence of ligneous periodontitis associatedwith EDS.
CONCLUSIONS
This case report provides further documentation onthe concomitant existence of ligneous disease dueto plasminogen deficiency and Ehlers-Danlos syn-drome. Histologic examination of gingival tissue isstrongly recommended for patients presenting withgingival overgrowth and alveolar bone loss associatedwith clinical findings that suggest Ehlers-Danlos syn-drome, especially to determine its most probable type.
REFERENCES1. Gunhan O, Gunhan M, Berker E, Gurgan CA, Yildirim
H. Destructive membranous periodontal disease (lig-neous periodontitis). J Periodontol 1999;70:919-925.
2. Frimodt-Møller J. Conjunctivitis ligneosa combinedwith a dental affection. Report of a case. Acta Oph-thalmol (Copenh) 1973;51:34-8.
3. Hidayat AA, Riddle PJ. Ligneous conjunctivitis. Aclinicopathologic study of 17 cases. Ophthalmology1987;94:949-959.
4. Diamond JP, Chandna A, Williams C, et al. Tranexa-mic acid-associated ligneous conjunctivitis with gingi-val and peritoneal lesions. Br J Ophthalmol 1991;75:753-754.
5. Nussgens Z, Roggenkamper P. Ligneous conjunctivi-tis. Ten years follow-up. Ophthalmic Paediatr Genet1993;14:137-140.
6. Gunhan O, Celasun B, Perrini B, et al. Generalizedgingival enlargement due to accumulation of amyloid-like material. J Oral Pathol Med 1994;23:423-428.
7. Gokbuget AY, Mutlu S, Scully C, et al. Amyloidaceousulcerated gingival hyperplasia: A newly described
entity related to ligneous conjunctivitis. J Oral PatholMed 1997;26:100-104.
8. Scully C, Gokbuget AY, Allen C, et al. Oral lesionsindicative of plasminogen deficiency (hypoplasmino-genemia). Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2001;91:334-337.
9. Schuster V, Mingers AM, Seidenspinner S, Nussgens Z,Pukrop T, Kreth HW. Homozygous mutations in theplasminogen gene of two unrelated girls with ligneousconjunctivitis. Blood 1997;90:958-966.
10. Watts P, Suresh P, Mezer E, et al. Effective treatmentof ligneous conjunctivitis with topical plasminogen.Am J Ophthalmol 2002;133:451-455.
11. Schuster V, Seregard S. Ligneous conjunctivitis. SurvOphthalmol 2003;48:369-388.
12. Shimabukuro M, Iwasaki N, Nagae Y, et al. Ligneousconjunctivitis: A case report. Jpn J Ophthalmol 2001;45:375-377.
13. Chakravarti S, Pickrell MD, Dunn PJ, Rollason TP.Ligneous conjunctivitis and the cervix. BJOG 2003;110:1032-1033.
14. Schuster V, Zeitler P, Seregard S, et al. Homozygousand compound-heterozygous type I plasminogen de-ficiency is a common cause of ligneous conjunctivitis.Thromb Haemost 2001;85:1004-1010.
15. Schuster V, Seidenspinner S, Zeitler P, et al. Com-pound-heterozygous mutations in the plasminogengene predispose to the development of ligneous con-junctivitis. Blood 1999;93:3457-3466.
16. Heidemann DG, Williams GA, Hartzer M, Ohanian A,Citron ME. Treatment of ligneous conjunctivitis withtopical plasmin and topical plasminogen. Cornea 2003;22:760-762.
17. Chai F, Coates H. Otolaryngological manifestations ofligneous conjunctivitis. Int J Pediatr Otorhinolaryngol2003;67:189-194.
18. Pantanowitz L, Bauer K, Tefs K, et al. Ligneous(pseudomembranous) inflammation involving the fe-male genital tract associated with type-1 plasminogendeficiency. Int J Gynecol Pathol 2004;23:292-295.
19. Suresh L, Aguirre A, Kumar V, Solomon LW, SielskiEA, Neiders ME. Recurrent recalcitrant gingival hy-perplasia and plasminogen deficiency: A case report.J Periodontol 2003;74:1508-1513.
20. Bateman JB, Pettit TH, Isenberg SJ, Simons KB.Ligneous conjunctivitis. An autosomal recessivedisorder. J Pediatr Ophthalmol Strabismus 1986;23:137-140.
21. Mingers AM, Heimburger N, Zeitler P, Kreth HW,Schuster V. Homozygous type I plasminogen de-ficiency. Semin Thromb Hemost 1997;23:259-269.
22. Chen S, Wishart M, Hiscott P. Ligneous conjunctivitis:A local manifestation of a systemic disorder? J AAPOS2000;4:313-315.
23. Kraft J, Lieb W, Zeitler P, Schuster V. Ligneousconjunctivitis in a girl with severe type I plasminogendeficiency. Graefes Arch Clin Exp Ophthalmol 2000;238:797-800.
24. Demarmels Biasiutti F, Sulzer I, Stucki B, WuilleminWA, Furlan M, Lammle B. Is plasminogen deficiencya thrombotic risk factor? A study on 23 thrombophilicpatients and their family members. Thromb Haemost1998;80:167-170.
25. De Coster PJ, Malfait F, Martens LC, De Paepe A.Unusual oral findings in dermatosparaxis (Ehlers-Danlos syndrome type VIIC). J Oral Pathol Med 2003;32:568-570.
J Periodontol • January 2006 Pierro, Vazquez-Sullca, Vieira, Takiya, Carakushansky, Feres-Filho
127

26. Pope FM, Komorowska A, Lee KW, et al. Ehlers-Danlos syndrome type I with novel dental features.J Oral Pathol Med 1992;21:418-421.
27. Slootweg PJ, Beemer FA. Gingival fibrinoid depositsin Ehlers-Danlos syndrome. J Oral Pathol 1987;16:150-152.
28. Karrer S, Landthaler M, Schmatz G. Ehlers-Danlostype VIII. Review of the literature. Clin Oral Investig.2000;4:66-69.
29. Perez LA, Al-Shammari KF, Giannobile WV, Wang HL.Treatment of periodontal disease in a patient withEhlers-Danlos syndrome. A case report and literaturereview. J Periodontol 2002;73:564-570.
30. Beighton P, De Paepe A, Steinmann B, Tsipouras P,Wenstrup RJ. Ehlers-Danlos syndromes: Revised no-sology, Villefranche, 1997. Am J Med Genet 1998;77:31-37.
31. Neville BW, Damm DD, Allen CM, Bouquot JE.Dermatologic diseases. In: Neville BW, Damm DD,Allen CM, Bouquot JE, eds. Oral & Maxillofacial
Pathology, Philadelphia: W.B. Saunders; 1995:552-553.
32. Prockop DJ, Kuivaniemi H, Tromp G, Ala-Kokko L.Inherited disorders of connective tissue. In: BraunwaldE, Fauci A, Hauser S, Longo D, Jameson JL, eds.Harrison’s Principles of Internal Medicine, vol. 2. NewYork: McGraw-Hill; 2001:2295-2297.
33. Coons AH. Histochemistry with labeled antibody. IntRev Cytol 1956;5:1-23.
34. Burrows NP. The molecular genetics of Ehlers-Danlossyndrome. Clin Exp Dermatol 1999;24:99-106.
35. Lijnen HR. Pathophysiology of the plasminogen/plasmin system. Int J Clin Lab Res 1996;26:1-6.
Correspondence: Dr. Viviane Santos da Silva Pierro, RuaPresidente Joao Pessoa, 263/904 Niteroi, Rio de Janeiro,Brazil. Fax: 55-21-2710-2171; e-mail: [email protected].
Accepted for publication May 13, 2005.
Ehlers-Danlos Syndrome and Periodontitis Volume 77 • Number 1
128